An Epidemiological Analysis of Dengue in Argentina
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below

An Epidemiological Analysis of Dengue in Argentina
Cecilia Radkiewicz
12 credits, 11th semester
Supervisors:
Åke Lundkvist, professor, Institutionen för Mikrobiologi, Tumör och Cellbiologi, (MTC)
Karolinska Institutet
María Cristina Diumenjo, MD, Departemento de Bioestatística, Ministerio de Salud,
Universidad Nacional de Cuyo
1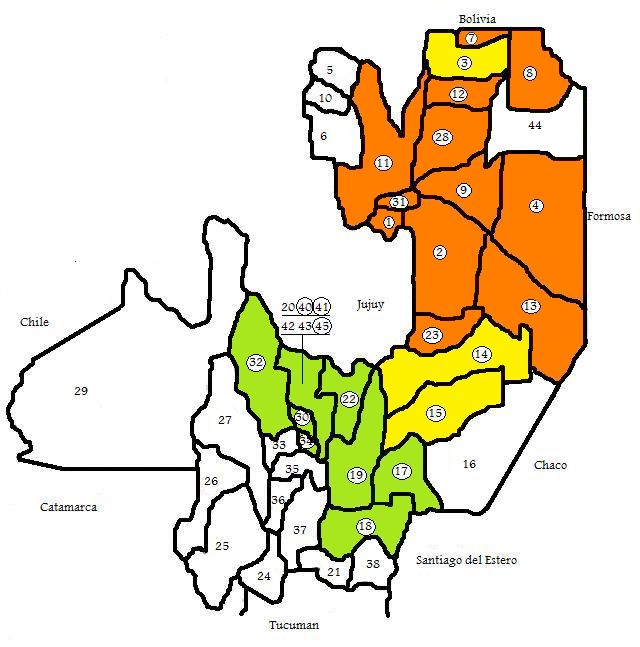
Abstract 3
Introduction 4
Aetiology, the dengue virus 4
Clinical features 5
Treatment 6
The vector, Aedes aegypti 6
History and Geographic Distribution 8
Material and Methods 10
The site of the study 10
The surveillance system 13
Dengue surveillance 13
Case classification 14
Laboratory investigations 14
Prevention 15
Out-break plan 15
The low-risk province, Mendoza 15
The high-risk province, Salta 16
Results 19
The Salta province 19
Seasonal variation 19
Sex distribution 21
Age distribution 21
Geographical distribution 22
Argentina 23
Discussion 24
References 26
2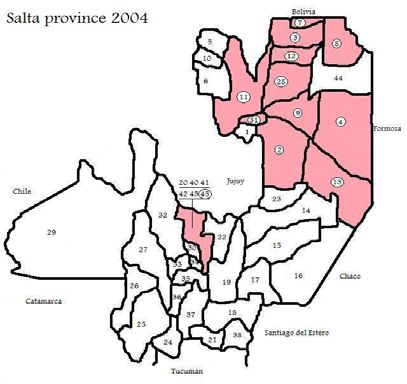
An Epidemiological Analysis of Dengue in Argentina
Cecilia Radkiewicz
12 credits, 11th semester
Supervisors: Åke Lundkvist, prof, institutionen för mikrobiologi, tumör och cellbiologi, Maria
Cristina Diumenjo, MD, departemento de estatistica, universidad nacional de cuyo
Abstract
Objective To make an epidemiological analysis of dengue (2002-2007), in the Salta province
in detail, and Argentina in general.
Background The emergence of dengue has been dramatic in South America, the cause is
complex and not well understood.1 A. aegypti, the main vector, was eradicated in Argentina in
1963 but has partly re-infested the country. In 1997 the first cases of dengue in Argentina
since 1916 were detected in Salta.2,3
Methods The intranet of the national surveillance system in Argentina coordinates and
presents epidemiological dengue data collection.4 The intranet was employed to gather the
necessary statistical material.
Results 613 laboratory confirmed cases of dengue fever (DF) and three cases of dengue
haemorrhagic fever (DHF) were reported. All DHF cases were reported in Salta in 2007. The
seasonal distribution showed a peak in the summer. Both sex and all age groups were
affected. In Salta 13 operative areas were affected, the majority identified as high risk areas.
Conclusions This analysis suggests that dengue is on the way of becoming endemic in
northern Argentina. If governmental organizations do not take immediate actions to prevent
the ongoing development there is an impending risk that dengue in Argentina in general and
the in Salta province in particular is on the way to becoming a major health problem.
3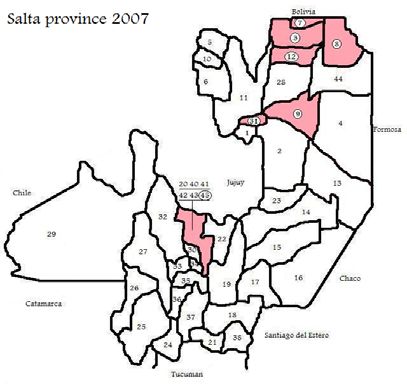
Introduction
The global incidence of dengue has increased dramatically during the last decades and dengue
is currently classified as an emerging or re-emerging infectious disease by the WHO. Dengue
fever (DF) and dengue haemorrhagic fever (DHF) occur in over 100 countries, with more than
2.5 billion people at risk and an estimated 50-100 million cases per year. The major disease
burden is found in south-east Asia and the western Pacific, with increased reporting of
DF/DHF especially in the Americas.5
Aetiology, the dengue virus
DF and DHF are caused by a flavivirus, an enveloped virus, with an icosahedral capsid and a
single-stranded, linear, non-segmented, positive polarity RNA. The flaviviruses include
dengue, hepatitis C, yellow fever, West Nile, and St. Louis and Japanese encephalitis viruses.
Dengue virus circulates as four immunologically distinct serotypes with large genetic
diversity (DEN-1, DEN-2, DEN-3, and DEN-4). Despite this diversity dengue fever normally
displays a typical clinical picture. Infection with one serotype provides lifelong immunity to
that specific serotype, but only transient immunity to the other serotypes.6 The dengue
genome encodes a single large open reading frame that is translated to form a viral
polyprotein. The polyprotein is subsequently cleaved in the cytoplasm by viral and host
proteases to produce three structural and seven non-structural (NS) proteins. The structural
proteins are named C (capsid), PrM/M (pre-membrane/ membrane), and E (envelope).7
Two electron images of mature DEN-2 particles replicating in five-day-old tissue culture cells. The original magnification is 123,000 times.8
Adaptive immunity (antibodies and cytotoxic T cells) is very important in the prevention of
viral diseases. The first exposure to a virus, symptomatic or asymptomatic, stimulates
production of antibodies and activation of cytotoxic T cells. Adaptive immunity plays an
essential role in protecting against disease when exposed to the same virus in the future. The
duration of protection varies. Lifelong protection against systemic viral infections is a
function of the secondary IgG response. The role of adaptive immunity in recovery from an
acute viral infection is often uncertain, since recovery usually precedes the appearance of
detectable humoral antibodies. An important phenomenon is original antigenic sin. This
means that when a person is exposed to a virus that cross-reacts with another virus to which
that individual was previously exposed, more antibody may be produced against the original
virus than against the current one. This may yield misleading antibody titres but is also one of
the underlying causes of severe dengue hemorrhagic shock. The pathogenesis is as follows:
The patient recovers from classic dengue fever caused by one of the four serotypes, and
antibody against that serotype is produced. When the patient is infected with another serotype,
a heterotypic response occurs, and large amounts of cross-reacting antibodies to the first
4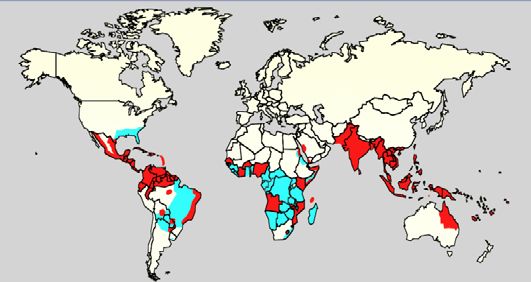
serotype are produced. There are two major hypotheses about what happens next. One is that
immune complexes, composed of virus and antibodies, are formed and activate complement,
causing increased vascular permeability and thrombocytopenia. The second one is that the
antibodies increase the entry of virus into monocytes and macrophages with the consequent
liberation of a large amount of cytokines. In either scenario, shock and haemorrhage is the
result.6
The dengue virus is an arbovirus mainly transmitted by the Aedes aegypti mosquito, which
is also the vector of yellow fever virus. Humans are the major reservoir, but a jungle cycle
involving monkeys as reservoir and other Aedes species as vectors are suspected. The life
cycle of arboviruses is based on the ability to multiply in both the vertebrate host and the
bloodsucking vector. For effective transmission, the virus must be present in the bloodstream
of the vertebrate host (viremia) sufficiently to be taken up in the small volume of blood
ingested during an insect bite. After ingestion, the virus replicates in the gut of the arthropod
and then spreads to other organs, including the salivary glands. An obligatory length of time,
called the extrinsic incubation period (the intrinsic incubation period refers to the interval
between the time of the bite and the appearance of symptoms in the human host) must pass
before the saliva of the vector is infectious. Usually humans are dead-end hosts, because the
concentration of virus in human blood is too low and the duration of viremia too short for the
next bite to transmit the virus. However, in some diseases, e.g. yellow fever and dengue,
humans have a high-level viremia and thereby act as reservoirs of the virus. The diagnosis
(see following chapters) can be made in the laboratory either by isolation of the virus in cell
culture, by serologic tests that demonstrate the presence of virus specific IgM antibodies or a
4-fold or greater rise in antibody titres between the acute and the convalescent sera, or by
molecular biology test (PCR).6
Clinical features
Dengue infection can produce a spectrum of clinical illness, from a non-specific viral
syndrome to severe and fatal hemorrhagic disease and shock. Symptoms appear 3-14 days
(average 6 days) after the bite of an infected mosquito. Risk factors for developing severe
disease include the strain and serotype of the virus, chronic diseases, age, immune status and
genetic predisposition of the patient, but also prior infection with another serotype.9 DF is a
severe, flu-like illness that affects infants, young children and adults, but seldom causes death.
Infants and young children may have a non-specific febrile illness with rash. Older children
and adults may have either a mild febrile syndrome or the classic “break bone fever” with
abrupt onset of high fever, severe headache, infraorbital pain, myalgia, arthralgia and rash.
DHF is a potentially fatal complication that is characterized by high fever, haemorrhagic
phenomena (such as petechiae, microscopic haematuria, epistaxis, bleeding gums,
haematemesis or melaena), liver enlargement and circulatory failure (mainly due to capillary
plasma leakage). It begins with a sudden rise in temperature and other non-specific
constitutional DF symptoms. The fever (sometimes biphasic) may reach 40-41°C and usually
continues for two to seven days. In moderate DF cases symptoms subside after temperature is
normalized. In severe cases the temperature drops after a few days of fever and the patient
may rapidly go into a critical state of circulatory failure and shock, dengue shock syndrome
(DSS), and die within 24 hours.8 Important differential diagnoses are chikungunya fever and
other viral fevers transmitted by arthropods, but also influenza, measles, rubella, malaria,
leptospirosis, typhoid, and systemic viral fevers, especially those associated with coetaneous
manifestations.10
5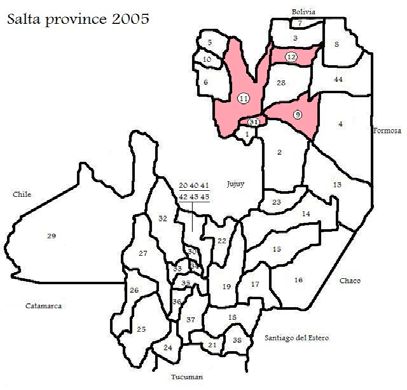
Treatment
There is still no DF vaccine available, although there are several tetravalent live-attenuated
dengue vaccines in clinical phase I or II trials. Neither does any DF specific treatment exist,
the only therapy available is symptomatic. Therapeutic-based processes are being investigated
and the development of new potential drugs with molecular viral targets is emerging.11
DHF patients should be monitored concerning platelet count (falling), haematocrit (rising)
and signs of shock (deterioration, lethargy, restlessness, acute abdominal pain, cold
extremities, skin congestion or oliguria), since about one-third develop DSS. The critical
period usually occurs after the third day of fever when the temperature starts to normalize.
The major pathologic process is increased vascular permeability leading to loss off fluid from
the vascular compartment. If uncorrected this may lead to shock, tissue anoxia, metabolic
acidosis and death. Apart from the vascular changes mentioned, DHF also exhibit
thrombocytopenia and disorders of coagulation. This may lead to disseminated intravascular
coagulation (DIC) which can cause bleeding (mainly from the gastrointestinal tract) and play
a major role in the development of a refractory lethal shock. Early and effective replacement
with plasma expander or fluid and electrolyte solution in combination with adequate
correction of metabolic and electrolytic disturbances rapidly reverses DHF/ DSS.12 High
fever, anorexia and vomiting may result in dehydration, oral fluid intake is usually sufficient.
During the acute febrile phase there is a risk of convulsions, antipyretics (for example
paracetamol) can be used for high risk patients (positive history). Salicylates must be avoided
since they can enhance bleeding and cause acidosis, but also trigger Reye syndrome.11 There
are data suggesting that administration of dipyrone (NSAID) in patients with DF is associated
with decreasing platelet counts and an increased risk of developing DHF.13 Blood grouping
and matching should be carried out for every patient in shock, though blood transfusion
(preferably fresh full blood) is only indicated when significant clinical bleeding. Fresh frozen
plasma or platelets may be indicated in DIC cases or where coagulopathy causes bleeding.
Essential laboratory tests are; haematocrite, serum electrolytes, blood gas analysis, platelet
count, prothrombin time, partial thromboplastin time, thrombin time and liver function tests.11
Some DHF cases develop acute hepatic failure with elevated aminotransferases and
neurological symptoms. This is a bad prognostic sign and causes therapeutic problems since
these patients must be given intravenous fluid with extreme caution to avoid brain oedema
and encephalopathy.11
The vector, Aedes aegypti
Dengue virus is transmitted to humans through the bites of an infective female Aedes
mosquito (especially A. aegypti, but also A. albopictus). A. aegypti is also the principle vector
transmitting yellow fever and chikungunya virus. Worldwide, this species has a range
extending from 40°N - 40°S latitude and is found throughout most tropical to subtropical
regions. Survival is poor in hot, dry climates. The mosquito acquires the virus from feeding
on blood from an infected person in the febrile phase of the disease when the virus is
circulating in the blood. Infected female mosquito may also transmit the virus to their
offspring via their eggs, though the role of this has not yet been thoroughly investigated. After
virus incubation for 8-10 days, an infected mosquito is capable of transmitting the virus for
the rest of its life (4-30 days). Humans are the main amplifying host of the virus, although
studies have shown that monkeys may also serve as a viral source.14, 15 A. aegypti is a day
biting mosquito (highest activity early morning and late afternoon), that preferably resides in
urban and semi-urban areas. Adult mosquito feed on flower nectar and juices of fruits for
flight energy. The female requires a blood meal for egg development. Human blood is
preferred and the ankle area is a favoured feeding site. A. aegypti only flies a few hundred
6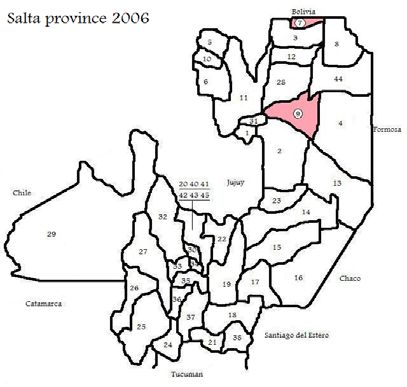
yards from the breeding site. The life cycle consists of four separate stages: ovum, larva,
pupa, and adult. Aedes species do not make egg rafts, like other mosquito species. The female
mosquito deposits the eggs separately on damp surfaces, next to stagnant water. Preferred
breeding areas are flower vases, uncovered barrels, buckets and discarded tires. The ovum
may survive up to one year when dry and hatch within 48 hours when flooded with water,
typically after rainfall. The ovum takes 5 days to develop into larvae, the larvae stage
generally last for 5-14 days. The larvae feed on micro-organisms and organic matter in the
water and come to the surface to breathe. Larvae die at temperatures below 10°C or above
44°C. On the fourth molt the larva changes into a pupa, a resting, non-feeding stage. This is
when the mosquito turns into an adult. Adults are killed by temperatures below freezing and
do not survive well at temperatures below 5°C. The length of the different stages depends on
the surrounding environment conditions (nutrition, temperature and humidity). On average,
females live up to a month and males die sooner.13, 14
A. aegypti is a medium-sized (approx. 0.5 cm) blackish mosquito easily recognized by a white pattern of scales on its scutum and white rings
on segment 1-4. The coloration of both sexes is similar.
Monitoring
Several indices have been used to measure larval densities, such as the number of water
receptacles containing larvae (container index), or the total number of receptacles with A.
aegypti larvae per 100 houses (Breteau index). Often a container index greater than 20, or a
Breteau index above 5 indicate that the vector population has reached a level which presents a
threat of urban transmission of yellow fever.16
History
In the eighteenth century slave ships from West Africa to the Americas carrying casks of
drinking water, providing breeding places for A. aegypti, aided the spread of the mosquito into
the New World. The extended global spread of the mosquito is facilitated by a rapid
urbanization accompanied by an unreliable water supply and domestic water containers
providing a perfect habitat for A. aegypti.15
A. albopictus is a native of South-East Asia where it commonly breeds in discarded tyres.
Like other Aedes species eggs can tolerate months of desiccation and then hatch when soaked
by rainwater. In 1979 A. albopictus suddenly appeared in Albania and in 1985 in Texas, USA.
It has also been introduced into Mexico, South America, Fiji, Italy, Nigeria and a few other
countries. It was brought to these countries as dry viable eggs mainly in used exported tyres.15
In the1940s and 1950s an A. aegypti eradication programme in Latin America freed 19
countries. But the mosquito was not eradicated from all countries and in the 1970’s the
programme deteriorated. In 1995 the distribution of A. aegypti in Latin America was almost
identical to that of the 1940s.15 In Argentina the mosquito has been detected in 332
municipalities, from Buenos Aires and the Pampas in the south stretching all the way to the
northern border.9
7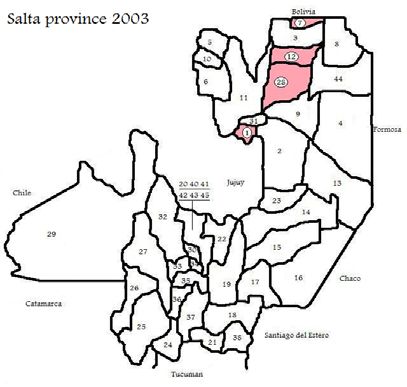
Problems and difficulties
Water-storage containers cannot be discarded since they provide essential domestic water.
Covering with plastic mosquito screening counteract ovi-positioning but still allow the
containers to be filled with rainwater. However, in practice it is notoriously difficult to get
communities to cover such potential breeding places. In Puerto Rico, in the 1980s, after
comprehensive educational propaganda, more than 70% of the people considered dengue an
important disease and about 70% also believed that dengue could be prevented. Nevertheless,
it proved impossible to get the community to change their habits. There are many more
examples illustrating the difficulties to get full and sustained community cooperation.
Though, in Cuba, when Fidel Castro declared A. aegypti “The Public Enemy Number One”
the entire community cleaned up the environment, removing discarded bottles, tin cans, and
other mosquito breeding places. Similarly, in Singapore, people helped to eliminate A. aegypti
breeding places around their houses, because householders could otherwise be fined or
imprisoned. Consequently Singapore and Cuba have the most efficient A. aegypti control
programmes in the world. Despite many disappointments and failures, most national and
international health agencies believe that the only long-term solution to controlling dengue in
Asia and the Americas is through community participation.15
Environmental measures, such as physically preventing A. aegypti from breeding in
domestic water containers, are preferable. But, if a dengue epidemic is threatening the lives of
people, the only rapid response is insecticidal spraying to kill infected adult mosquitoes. Once
the epidemic is under control there can be a return to a more integrated approach to vector
control. However, the situation has to be constantly monitored for detection of any re-
introduction.15
History and geographic distribution
The first reported dengue epidemics occurred in 1779-1780 in Asia, Africa, and North
America. Until the mid-twentieth century DF only occurred infrequently as major epidemics
in tropical regions. Nowadays dengue is endemic in the majority of the tropical countries.17
The global spread started in Southeast Asia following World War II. The epidemiology
changed because of ecological transformations (domestic water storage, transport of war
equipment and soldiers, left over war material) which increased larval habitat for A. aegypti
and enabled transport of mosquitoes and their eggs to new geographical areas but also human
transport of virus strains to susceptible populations. This resulted in high densities of A.
aegypti and hyperendimicity (co-circulation of multiple strains of dengue virus) which
facilitated the first real emergence of DF and DHF in Southeast Asia. An unsurpassed
urbanization and population growth, involving inadequate housing, water, sewer and waste
management in this region contributed. In every Southeast Asian country the emergence of
DHF evolved in a similar way, at first sporadic cases for several years, then culminating into
outbreaks. From the mid 1950s to the 1970s epidemic DHF was localized to a few Southeast
Asian countries. In the 1980s and 1970s a dramatic geographic expansion west into India,
Pakistan, Sri Lanka, the Maldives and east into China took place. Even in Singapore, with an
outstanding prevention and control program, there was a resurgence of DHF, mainly because
of a low herd immunity and virus import via migrant workers. Today Asia suffers from cyclic
DF and DHF outbreaks every 2nd - 5th year.16
The dengue surveillance in Africa has been poor and still is, when epidemics occur they are
often reported as malaria outbreaks. In spite of this, laboratory confirmed dengue-epidemics
have increased dramatically since 1980. Limited outbreaks have occurred in West Africa, but
also in East Africa and in the Middle East. All four virus serotypes have been involved, but
only sporadic cases of clinical DHF have been reported.16
8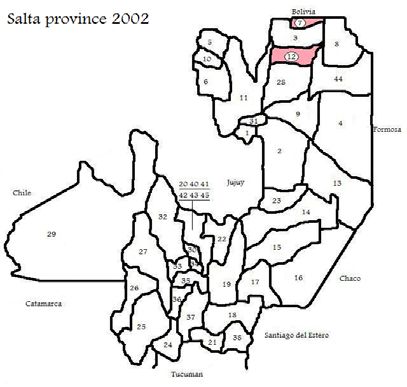
Map: Dengue distribution in the world, 2006. Blue areas: Aedes aegypti infestation. Red areas: Aedes aegypti and recent dengue epidemics.18
Epidemic dengue re-emerged in the Americas in the late 1970s. Before this there was no
epidemic activity due to a successful A. aegypti eradication programme initiated by the Pan
American Health Organization (PAHO) in 1946 to prevent yellow fever. In the early 1970s
the programme was discontinued and by the end of the 1980s the countries that achieved
eradication were re-infested.16
Map: Aedes aegypti re-infestation in the Americas, 1970 and 2002. PAHO/WHO, 2002
This coincided with movement of dengue virus both into and within the region. From the
1950s to early 1980s there was non-endimicity (no virus) or hypo-endimicity (only one
serotype) in most American countries. In 1977 DEN-1 was introduced to the region via
Jamaica and Cuba, and subsequently spread into the Caribbean islands, Mexico, Texas,
Central America and Northern South America, causing major or minor epidemics over the
next four years. In 1981 DEN-4 was introduced and spread rapidly in a similar way. Some of
the outbreaks were associated with the first documented cases of DHF in the Americas. In
1981 a new strain of DEN-2 was introduced in Cuba, most probably from Southeast Asia.
This caused the first major DHF epidemic in Cuba and was associated with thousands of cases
of severe DHF. Epidemic DHF of variable intensity caused by the same strain of DEN-2 has
subsequently occurred in numerous American countries, but none with the same severity. In
1994 a new strain of DEN-3, also from Asia, caused a major DF/DHF epidemic in Nicaragua
and subsequently spread throughout Central America and Mexico causing major outbreaks.
The changing epidemiology of dengue in the Americas in the 1970s to the 1990s is almost
identical to the development in Southeast Asia in the 1950s to the 1970s. The re-invasion of
Aedes aegypti in combination with increased urbanization and movement of people has
resulted in an increased epidemic activity and the emergence of DHF. Cuba, Venezuela,
9Brazil, Colombia and Nicaragua have had major DHF epidemics, but only small DHF
numbers have emerged in the rest of the American countries.16 Today dengue is endemic and
cause cyclic outbreaks in almost the hole of the Caribbean and Latin America, including
Bolivia, Brazil, Colombia, Ecuador, French Guyana, Guyana, Mexico, Paraguay, Peru,
Suriname, Venezuela and Central America.9
In northern Argentina several cases of dengue were reported in 1905-1911 and in 1916 an
outbreak of 15,000 cases were reported. In 1955 A. aegypti covered a large part of Argentina,
reaching Buenos Aires, but by 1963 the mosquito was considered eradicated. In 1997 the first
dengue cases since 1916 were confirmed.19 The mosquito has been detected in 332
municipalities from Buenos Aires and the Pampas in the south stretching all the way to the
northern border.9 In 1998 a dengue outbreak occurred in the province of Salta, in total 644
cases of dengue was laboratory confirmed. This was the first time dengue was laboratory
diagnosed and the virus isolated (DEN-2) in Argentina.20
Material and Methods
The site of the study
Geography and Climate
Argentina is situated in southern South America, between the Andes in the west and the
Atlantic Ocean in the east. It is bordered by Paraguay and Bolivia in the north, Brazil and
Uruguay in the northeast, and Chile in the west. Its total area is approximately 2.7 million
km². Consequently, Argentina is the second largest country in South America (after Brazil)
and the 8th largest country in the world. Argentina is nearly 3,700 km long from north to
south, and 1,400 km from east to west (maximum values). The geographic coordinates are
34°00’S, 64°00’W. The terrain can roughly be divided into four parts: the fertile agricultural
plains of the Pampas in the centre, the flat to rolling and oil-rich plateau of Patagonia in the
southern half down to Tierra del Fuego, the subtropical flats of the Gran Chaco in the north,
and the rugged Andes mountain range along the western border. Argentina displays a variety
of climates, but is predominantly temperate with extremes ranging from sub-tropical in the
north to sub-Antarctic in the south. The north of the country is characterized by very hot,
humid summers with mild drier winters, and suffers from periodic droughts. Central
Argentina has hot summers with thunderstorms and cool winters. The southern regions have
warm summers and cold winters with heavy snowfall, especially in the mountains. Higher
elevations at all latitudes experience cooler conditions.21
The province of Salta is situated in north-east Argentina. It is bordered by Bolivia and the
province of Jujuy in the north, Paraguay and the provinces of Formosa and Chaco in the east,
the provinces of Santiago del Estero, Tucumán and Catamarca in the south, and Chile and the
province of Jujuy in the west. Its total area is approximately 155 488 km². The geographic
coordinates are 22°00’N, 26°23’S, 62°21’E, 68°33’W. The climate is tropical but displays
distinct variations between the different regions. The mountain chain has an important
influence on the precipitation. The eastern part is semi-dry, annual precipitation 500 mm, the
temperature ranging from -5°C up to 47°C (average 20°C). The mountain plateau is
characterized by brusque changes in temperature (average 10°C) and sparse rainfall, annual
precipitation 200 mm. The fertile valleys are densely populated and have a humid climate
suitable for agriculture, annual precipitation reaching 1000 mm, average temperature in
summer 20°C and 14°C in winter. The A. aegypti infestation is abundant, with a peak during
summer months (December to March). The population is approximately one million
inhabitants. Almost half of the population live in Salta capital, Orán or Tartagal, which are the
10most densely populated municipalities. The Salta province is a communication node between
the north of Chile, the north-east of Argentina, Bolivia and Paraguay. There is a constant and
intense movement of people and merchandise across the border to the neighbouring countries.
Bolivia and Paraguay have both suffered from several severe dengue outbreaks in the last
years.22
Map: Climate Map of Argentina. Gobierno Electrónico Argentina. Available from: http://www.surdelsur.com/argentinamap/climatemap.htm
Population (in thousands) total 38747 (2005)
Total fertility rate (per woman) 2.3 (2005)
Population annual growth rate (%) 1.1 (2005)
Population in urban areas (%) 90.0 (2005)
Population living below the poverty line (% living on < US$1 per day) 7.0 (2003)
Gross national income per capita (PPP international $) 13920 (2005)
Total expenditure on health as percentage of gross domestic product 9.6 (2004)
Adult literacy rate (%) 97.2 (2004)
Life expectancy at birth (years) men 72.0 (2005)
women 78.0 (2005)
Population with sustainable access to improved drinking water (%) urban 98 (2004)
rural 80 (2004)
Population with sustainable access to improved sanitation (%) urban 92 (2004)
rural 83 (2004)
Table 1. Core Health and Socioeconomic Indicators23
Inequities in Health24
Argentina is not only extremely diversified when it comes to geography and climate. It is also
a country with a severe disparity between rich and poor, urban areas and countryside, and
displays major differences in development between the central provinces and the remote
northern parts. The figures in Table 1 are all correct but do not give a fair picture. The
northern, subtropical provinces; Chaco, Corrientes, Formosa, Misiones, Jujuy and Salta are in
high risk of future dengue epidemics. These provinces also have the smallest margin and lack
sufficient financial resources to combat a feasible epidemic. They fall behind development in
several important areas. This is neatly illustrated by the statistics in Table 2-3. Table 2
11displays socio-economic indicators, comparing the situation in the whole country, Buenos
Aires city (BA) and the Northern provinces. The Human Development Index (HDI) measures
the average achievements in a country in three basic dimensions of human development; a
long and healthy life (life expectancy), knowledge (literacy and education) and a decent
standard of living, for countries worldwide. It is used by the United Nations Development
Programme in its annual Human Development Report to determine whether a country is
developed, developing, or underdeveloped.25 The mean HDI for Argentina and BA is high
(0,800-1) while the northern provinces only reach a medium (0,500-0,799). Another
multidimensional measure of poverty is Unsatisfied Basic Needs (Necesidades Básicas
Insatisfechas NBI). The Argentine government uses the following strategy to characterize
households with unsatisfied basic needs:26
1. Overcrowded homes is households with more than three persons per room.
2. Unsuitable housing. Housing is considered unsuitable if it is a tenement or some other
poorly built house, apartment, or shack.
3. Houses without toilets.
4. Households with children aged 6-12 years not attending school.
5. Survival capacity. Households which have 4 or more working members as well as
those households whose head of household has not completed third year of primary
education.
Only 7.8% of the households in BA, but almost a third of the households in the poorest
provinces does not have one or more of the basic needs satisfied.
1. 2. 3. 4. 5.
Argentina 0,826 17,7 2,6 77 42,5
Buenos Aires city 0,892 7,8 0,5 99,9 96,6
Corrientes 0,772 28,5 6,5 81 42,4
Chaco 0,755 33 8 61,6 18,6
Formosa 0,764 33,6 6 64,7 21,7
Jujuy 0,772 28,8 4,7 92,6 48
Misiones 0,772 27,1 6,2 57,2 11,3
Salta 0,792 31,6 4,7 89,9 51,1
Table 2. Socioeconomic Indicators 2003.23 1. Human Development Index (HDI) 1996. 2. Households with at least one NBI (%) 2001. 3.
Adult illiteracy rate (%) 2001. 4. Population with sustainable access to improved drinking water sources (%). 5. Population with sustainable
access to improved sanitation (%).
A. B. C. D.
1
Argentina 4,4 16,5 10,5 0,7
2
The central region 2,6 15,2 9,4 0,5
3
The north-west region 7,6 19,1 12,6 0,8
4
The north-east region 8,2 23,2 15,7 1,3
Table 3. Maternal and Child Health 2003. 23 A. Maternal mortality rate (per 10.000 live births). B. Infant mortality rate (per 1000 live births).
C. Neonatal mortality rate (per 1000 live births). D. Under-5 mortality rate (per 1000 live births). 1The whole country. 2Buenos Aires city and
province, Cordoba, Entre Rios, Santa Fe. 3Catamarca, Jujuy, Santiago del Estero, Salta, Tucuman. 4Corrientes, Chaco, Formosa, Misiones.
Table 3 compare indicators concerning maternal and child health. Development, i.e. public
health, is falling behind in the northern provinces. The actual dengue prevention programme
is based on vector population control. The cornerstones of this programme are public health
education and communication, and improvement of the sanitary environment (see following
chapters). Subsequently, a region falling behind in development will face major difficulties
combating a feasible dengue outbreak.
The living standards in the Salta province are poor when comparing to the central provinces,
as well as the general level of education. A significant part of the population lack sustainable
access to improved drinking water and sanitation. Also a large proportion of the population
12are descendants to indigenous people. These people commonly live segregated from the rest
of the population in so-called Misiónes. The litteracy rate is low and malnutrition is common.
The grave poverty as well as cultural differences in these neighbourhoods, contribute to the
difficulties the public health care system meet.
The surveillance system (Sistema Nacional de Vigilancia Epidemiologica SiNaVE)
Dengue surveillance in Argentina is organized as a collaboration of the National Department
of Epidemiology, National Ministry of Health, Provincial Departments of Epidemiology,
National and Provincial Departments of Vector control, and the DENV laboratory network.27
A compulsory report program, a disease specific form and laboratory procedures for several
diseases, among them dengue, are essential components of the surveillance system. (See
attached form Notificación Médica Obligatoria C2)
SiNaVE is organized into four levels;
1. Population; all inhabitants of Argentina.
2. Local health care professionals in direct contact with the population.
3. Provincial Departments of Epidemiology collect, compile and forward the information
reported by the local physicians.
4. The National Department of Epidemiology summarize, draw up national guidelines,
and forward epidemiological data to international organizations (WHO and PAHO).28
Dengue surveillance
Information and instructions on the surveillance, prevention, and control of dengue are
distributed to health care professional at all health care establishments (public as well as
private). Case classification and information about the procedures and investigations that must
be performed on suspected cases are disseminated to physicians at all levels. When
identifying a suspected case, every physician is obliged to;
1. Immediately contact the provincial epidemiological department by telephone or fax.
2. Obtain the laboratory tests needed.
3. Complete the specific designed form containing personal information, clinical signs,
laboratory tests performed, and epidemiological data on the suspected case.29 (See
attached form Vigilancia de Sindrome Febril B1-3).
DengueNet is an international surveillance system created by the WHO to improve global
dengue surveillance. It is a central data management system made to collect and analyse
standardized epidemiological and viral data, and present epidemiological trends. The
American region was the first to participate. The objective is to provide public health
authorities and the general public with immediate real time data on dengue morbidity and
mortality as well as circulating virus serotypes.30
Due to the major dengue outbreak in the neighbouring country Paraguay in January 2007,
the Argentine National Ministry of Health declared an alert epidemic situation. The Northern
provinces (Formosa, Misiones, Corrientes, Chaco and Salta) bordering Paraguay and Bolivia
and A. aegypti infested are at especially high risk. High risk provinces must monitor all febrile
cases and the following measurements and recommendations were reinforced;31
- Intensified surveillance of all febrile conditions.
- Registration and epidemiologic investigation of all suspected, probable and confirmed
dengue cases.
- Focal control and/or block of viral transmission.
- Evaluation of the efficiency of the intervention programme.
- Intensified vector control at a provincial level.
13Case classification28
Classical dengue fever (DF), ICD-10: A90
A suspected DF case is defined as an acute febrile illness no longer than seven days,
characterized by frontal headache, and showing at least two of the following symptoms; retro-
ocular pain, muscle and joint pain, coetaneous rash, minor bleeding phenomena
immobilisation, nausea or vomiting, in combination with residence or movement into an area
with confirmed dengue transmission.
A Probable DF case is a clinically compatible case with supportive serologic findings such as
single acute or convalescent-phase serum positive for Immunoglobulin (Ig) M antibody or a
dengue virus IgG antibody titre ≥1280.
A confirmed case is a clinically compatible case that is laboratory confirmed either by virus
isolation, IgM seroconversion or a four-fold increase in IgG titres for paired serum, or
molecular biology test (PCR).
Dengue haemorrhagic fever (DHF), ICD-10: A91
A clinically compatible DF case presenting one or more of the following haemorrhagic
manifestations;
1. Positive Tourniquet (capillary fragility test)
2. Petechiae, ecchymoses or purpura
3. Gastrointestinal or mucosal haemorrhage (gingival bleeding, haematemesis, melaena)
4. Thrombocytopenia (≤100x109/l)
5. Plasma leakage, due to increased capillary permeability, causing one or more of the
following characteristics;
- 20% increase of haematocrit (adjusted for age).
- 20% decrease of haematocrit after rehydration therapy, (compared to basal level).
- Pleural effusion, ascites or hypoproteinaemia.
Dengue haemorrhagic shock syndrome (DSS)
A DHF case presenting symptoms or signs of circulatory failure; fast and weak pulse, reduced
pulse pressure, hypotension (age adjusted), cold extremities, restlessness or agitation.
Laboratory investigations28
1. Isolation of dengue virus from serum and/or or autopsy tissue samples (confirmed).
2. Demonstration of a four-fold or greater rise or fall in reciprocal IgG or IgM antibody
titres (MAC-ELISA) to one or more dengue virus antigens in paired serum samples
(confirmed).
3. Detection of dengue virus antigen in autopsy tissue by immunohistochemistry or by
viral nucleic acid detection (confirmed).
4. Detection of dengue virus genomic sequences in autopsy tissue, serum samples, or
cephalo-rachidial liquid using polymerase chain reaction (PCR) techniques (probable).
Serum samples (≥ 5 ml, if possible 10 ml) should preferably be collected from suspected
cases 5 days (late acute) and 10-20 days after onset of symptoms (convalescent). When using
serological methods for diagnosis it is important that the corresponding epidemiological
history accompany the sample to the laboratory. The usage of anti-coagulants must be
avoided, as well as deep freezing, unless the sample can not be sent to the national reference
laboratory within 4 days. The laboratory result for specific antibodies is ready within 72
hours, PCR within 48 hours, and virus cultivation takes about 15 days.32
The DENV laboratory network is coordinated by the national institute for human viral
diseases (Instituto Nacional de Enfermedades Virales Humanas, INEVH), the national
14reference centre of DENV diagnosis in Argentina.26 To guarantee true verification of
suspected cases additional support was distributed to the DENV laboratory network
(laboratorios de la Red), including equipment and instructions on how to collect, handle and
process dengue diagnostic samples. Standardized protocols were designed to secure sufficient
diagnostic quality and a reliable sample referral chain.33
Prevention34
1. Public health education and communication on methods how to eliminate, destroy and
control the vector mosquito (i.e. A. aegypti) larvae habitat, that is to say artificial water
containers inside or close to housing (water receptacles, vases, old tyres, and groceries).
2. Community studies to assess vector density and recognise major larvae habitats, with the
objective to speed up programs on how to eliminate, control and combat the mosquito.
3. Personal protection against mosquito bites; repellents, mosquito nets, and adequate
clothing.
Out-break plan35
Four different epidemiologic situations and four corresponding contra-actions can be outlined.
In the first scenario a probable case is identified in an area with no vector infestation, this
demands for an epidemiological investigation. In the second scenario A. aegypti is present but
indigenous dengue is not (Mendoza), a probable dengue case then causes an alert
epidemiologic situation and calls for active measures at community level. In scenario number
three there are several probable cases in a mosquito endemic area, an epidemic (Salta). This
requires active measurements as well as serologic surveillance to detect new serotypes. The
fourth situation is “worst case scenario” where hyperendimicity (more than one serotype
circulating) is present and dengue is endemic.34
Active measures at the individual level involve.33
- Epidemiological (activities last 15 days before debut) and laboratory investigation.
- Report to local health authorities.
- Avoid patient-mosquito contact until the fever has subsided.
- Active look-out for unreported or undiagnosed cases.
- If DF appears in Yellow Fever (YF) endemic areas, YF-vaccination is recommended.
In case of an epidemic, the local government must act to locate and kill adult mosquito near
housing, and to protect people exposed to mosquito bites;
- Information, education and communication to the general public, concerning mosquito
biology, virus transmission and prevention.
- Intensified surveillance of febrile cases in high risk areas.
- Intensified control of mosquito breeding ground.
- Elimination of mosquito breeding ground through destruction or inversion of water
containers, larvae repellents, or elimination of adults.
- Campaigns to eliminate crocks and improve municipal waste management.27
The low-risk province, Mendoza
The following section is based on an oral presentation and a personal interview with Dr.
Horacio Falconi (e-mail: zoonosismendoza@yahoo.com.ar phone: +54 261 5091772) the
responsible veterinary at the Division for Zoonosis, Reservoirs and Vectors (División de
Zoonosis, Reservoires y Vectores) in the Mendoza province.
15Several approaches to improve the sanitary environment to combat the mosquito vector and
inhibit viral transmission exist. Environmental modifications involve improvement of public
access to drinking water and sanitation, as well as elimination of natural vector reservoirs.
Manipulative methods include covering reservoirs with mosquito net and improving
community consciousness to prevent human vector contact (physical barriers, repellents).
Another aspect when discussing preventive measurements is to subdivide methods into
natural or chemical. Natural methods are preferable;
- Sustainable access to improved drinking water (water supply and storage).
- Sustainable access to improved sanitation.
- Improved garbage management, including; yards, houses, lots, streets, dustbins, etc.
- Modification of other man-made breeding ground, such as; farm basins, enclosures,
posts, tarpaulins, wash basins, etc.
- Personal protection, e.g. adequate clothing, mosquito nets, etc.
A chemical approach must be rational and strategic to avoid mosquito resistance to
insecticides, ecologic changes affecting other species, and unwanted human effects;
- Focal control is limited to larvae habitat and consists of organic phosphor insecticide
granules placed in artificial water containers.
- General control methods aim at adult mosquito and involve spatial spraying of ultra
low volume (ULV) of a pyrethroid insecticide 400 meters around case location blocks.
- Sub-focal control is aiming at larvae habitat as well as adult mosquito. ULV indoor
spraying is limited to mosquito infested households of suspected cases.
Biological control methods, yet not applied in large-scale, are fresh-water fish feeding on
larvae (Gambusia and Poecilia species), competitive larvae, hormones, water fleas, and
bacteria (Bacillus species). In Mendoza preventive actions are based on public education. An
impressive educational material on how to eliminate larvae habitat, vector biology and
lifecycle, and dengue symptoms, has been prepared. Pedagogical material, including a CD
ROM computer game, is handed out to teachers at primary schools. Written information is
distributed to primary health care professionals performing home visits. Due to economic
limitations, the use of other mediums (newspapers, radio and television) does not exist.
Entomologic surveillance in Mendoza is only implemented during summer months (e.g.
January till May). These investigations are basic and the objective is to determine A. aegypti
presence in the province. Water-filled tyres are placed in appropriate surroundings and
checked for mosquito egg, larvae or pupae every week.
If a suspected dengue case appear in Mendoza the patient is highly recommended to accept
hospital admission where patient-mosquito contact can be strictly under control. If this is not
possible, the Division for Zoonosis, Reservoirs and Vectors will investigate if the affected
household and block must be subject for a general chemical control programme.
The high-risk province, Salta
The following chapter is based on a study visit at the municipal Department of Epidemiology,
Hospital Juan D. Peron in Tartagal, the Salta province and circulating letters of directions
(Circular Normativa) provided by Dr. Josefina Aguierre, chief at the local Department of
Epidemiology in Tartagal, published by the Ministry of Public Health in the Province of Salta;
EPI 5 Sitios centinela para la vigilancia epidemiologica de dengue
EPI 7 Vigilancia entomológica de Aedes Aegypti
EPI 8 Uso de repelente en pacientes y convivientes de casos sospechosos de dengue
EPI 12 Dispositivo para recipientes no descacharrables
EPI 19 Guia para la utilización del Spinosad y Glifosato para el manejo de Aedes Aegypti
EPI 20 Uso del hipoclorito de sodio contra huevos de Aedes Aegypti
16The objectives of the surveillance system are intensified epidemiological surveillance of all
cases of acute febrile illness and early detection of any cases compatible with dengue (see
previous chapters) as well as early identification of circulating serotypes. The Salta province
is divided into operative areas;
1. Operative areas in high risk of DF and DHF. (orange)
2. Operative areas in high risk of DF. (yellow)
3. Operative areas in moderate risk of DF. (green)
Map: The Salta province, operative areas. Orange: operative areas in high risk of DF and DHF. Yellow: operative areas in high risk of DF.
Green: operative areas in moderate risk of DF. (EPI 5)
1 Colonia Santa Rosa O 13 Rivadavia Banda Sud O 25 San carlos 37 Guachipas
2 Pichanal O 14 Las Lajitas Y 26 Molinos 38 El Potrero
3 Aguaray Y 15 J.V. Gonzalez Y 27 Cachi 39 Urundel O
4 Morillo O 16 El Quebrachal 28 General Mosconi O 40 Hospital San Bernardo G
5 Santa Victoria Oeste 17 El Galpón G 29 Los Andes 41 Hospital del Milagro G
6 Inya 18 Rosario de la Frontera G 30 Cerrillos G 42 Hospital Christofredo
7 Salvador Mazza O 19 Metán G 31 Hipólito Yrigoyen O Jackob
8 Santa Victoria Este O 20 Hospital Materno Infantil 32 Rosario de Lerma G 43 Hospital Endocrinologia
9 Embarcación O 21 La Candelaria 33 Chicoana y Metabolismo
10 Nazareno 22 General Güemes G 34 El Carril G 44 Alto La Sierra
11 Orán O 23 Apolinario Saravia O 35 Coronel Cornejo 45 PNA- Area Capital G
12 Tartagal O 24 Cafayate 36 La viña 46 Hospital “El Milagro” G
Salta Province, Operative Areas. (EPI 5)
Anticipatory surveillance phase
Serum samples for viral isolation should be collected from suspected cases 3 days after onset
of symptoms, and sent to the National Reference Laboratory (INEVH in Pergamino) within
72 hours, accompanied by the dengue specific form. In case of an outbreak and when the
circulating serotype has been identified, confirmation of suspected cases should be carried out
by testing for IgM antibodies instead of viral isolation. Serologic samples are sent to the
17provincial laboratory (Laboratorio de Virologia del Hospital Milagro) (see previous chapters).
Local pharmacists are instructed to report increasing consumption of the most commonly used
antipyretics.
Surveillance during the high risk period (Nov-May)
- Daily notification of suspected cases tested negative.
- Weekly epidemiological report in case of an outbreak.
- Weekly report of housing and Breteau index (A. aegypti infestation), the objective is to
keep the housing index < 1%. A fixed number of households are selected and larvae
presence is controlled weekly (Nov-May) or monthly (Jun-Oct). (EPI 7)
Once an outbreak is officially announced, IgM samples are collected from one out of five of
the suspected DF cases and from every single suspected case of DHF.
Communication
All probable DF cases detected during the anticipatory surveillance phase must be reported
immediately to the chief of the Epidemiologic Surveillance Programme: Dr. Griselda
Rangeón or her subordinate Dr. Alberto Gentile. Daily notification, by fax or telephone, of
suspected cases tested negative starts on the first of November every year. In case of an
outbreak in an operative area the weekly epidemiological report is sent by e-mail or fax to the
Epidemiologic Coordination Committee (Dirección de Coordinación Epidemiológica).
Control actions
All suspected cases and co-inhabitants must be informed on how to use mosquito repellent by
their physician. Individuals ≥ 2 years are advised to use a 23.8% DEET (N,N-diethyl-m-
toluamide) spray, individuals ≤ 2 use a special customized alcohol free essence. Suspected
cases must use repellent up to and including day four and co-inhabitants up to and including
day 12 after symptom onset (EPI 8). Detection of probable and confirmed cases leads to
immediate and urgent actions to find compatible cases in the same household and
neighbourhood. Simultaneously, actions to verify the entomologic situation in every single
household in the neighbourhood are made (EPI 7). This is also an opportunity to inform the
neighbours to seek medical advice and to avoid aspirin in case of acute febrile illness. The
problem how to discard water-storage containers which serve as mosquito breeding places has
been subject to many discussions. But it has proved difficult to change human behaviour. In
the Salta province, sanitary agents work preventive by visiting people in their homes, handing
out information and showing potential risks in the surrounding environment. Despite many
disappointments community participation is the only long-term solution to control A. aegypti
(EPI 12). Spinosad insect spray (a mixture of two naturally occurring metabolites, spinosyns
A and D, produced by S. spinosathe) is used to control adult A. aegypti. Glyphosate (N-
(phosphonomethyl) glycine), is an herbicide used to constrain mosquito preferred mating
areas (EPI 19). Sodium hypochlorite (NaOCl), commonly known as bleach, is placed in dry
containers before watering to prevent A. aegypti ovipositioning (EPI 20).
Responsibility
- Management of diagnostic laboratory samples; provincial (Laboratorio de Virologia
del Hospital Milagro) and national (INEVH, Pergamino).
- Vector Index Reports: The Department of Zoonosis and Environment.
- Daily reports of negative cases and weekly reports; The Epidemiologic Surveillance
Programme.
18Results
Salta
From January 2002, when SiNaVE first introduced the electronically surveillance system, to
December 2007 the Provincial Department of Epidemiology in Salta reported 378 DF and 3
DHF laboratory confirmed cases to the National Department of Epidemiology. The incidence
rate ranges from 0.28 to 15.6 cases per 100,000. All DHF cases were registered in 2007. Two
outbreaks, in 2004 and 2007, occurred during the period studied (see Table 1).
Year 2002 2003 2004 2005 2006 2007 Total
1
N 21 52 168 11 3 126 381
2
IR 1,946155 4,819049 15,56924 1,019414 0,278022 11,67693 35,3088
Table 1. 1Number of laboratory confirmed DF and DHF cases reported to SiNaVE. 2Incidence rate (per 100 000 population). Salta 2002-
2007.
Seasonal variation
There is a marked seasonal correlation between the number of registered DF cases and the
temperature and precipitation (see Diagram 1-7). Most cases were reported between January
and June with a slight peak in March. From epidemiological week 17 onwards the weekly
report dropped, showing a probable halt in transmission. Effective transmission probably only
occur over the first four months of the year (see Diagram 8).
Diagram 1, weekly DF surveillance Salta 2002 Diagram 2, weekly DF surveillance Salta 2003
DF Salta 2002 (N=21) DF Salta 2003 (N=52)
9 20
8 18
16
7
14
6
12
5
Cases
Cases
10
4
8
3
6
2
4
1 2
0 0
1 3 5 7 9 11 13 15 17 19 21 23 25 27 29 31 33 35 37 39 41 43 45 47 49 51 53 1 3 5 7 9 11 13 15 17 19 21 23 25 27 29 31 33 35 37 39 41 43 45 47 49 51 53
Epidemiological week Epidemiological week
Diagram 3, weekly DF surveillance Salta 2004 Dagram 4, weekly DF surveillance Salta 2005
DF Salta 2004 (N=168) DF Salta 2005 (N=11)
18 4,5
16 4
14 3,5
12 3
10 2,5
Cases
Cases
8 2
6 1,5
4 1
2 0,5
0 0
1 3 5 7 9 11 13 15 17 19 21 23 25 27 29 31 33 35 37 39 41 43 45 47 49 51 53 1 3 5 7 9 11 13 15 17 19 21 23 25 27 29 31 33 35 37 39 41 43 45 47 49 51 53
Epidemiological week Epidemiological week
19Diagram 5, weekly DF surveillance Salta 2006 Diagram 6, weekly DF surveillance Salta 2007
DF Salta 2006 (N=3) DF Salta 2007 (N=123)
2 30
25
20
Cases
Cases
1 15
10
5
0 0
1 3 5 7 9 11 13 15 17 19 21 23 25 27 29 31 33 35 37 39 41 43 45 47 49 51 53 1 3 5 7 9 11 13 15 17 19 21 23 25 27 29 31 33 35 37 39 41 43 45 47 49 51 53
Epidemiological week Epidemiological week
Diagram 7, weekly DF surveillance Salta 2002- 2007
DF Salta 2002-2007 (N=378)
45
40
35
30
25
Cases
20
15
10
5
0
1 3 5 7 9 11 13 15 17 19 21 23 25 27 29 31 33 35 37 39 41 43 45 47 49 51 53
Epidemiological week
Sex distribution
The distribution by sex did not show any predominance though the attack rate was slightly
higher in females. The mean male:female ratio between 2002 and 2007 was 1:1,1. A great
variation different years is observed, the ratio ranging from 1:3,2 in 2002 to 2:1 in 2006 (see
Table 2).
Year Male (%) Female (%) Total (%) M:F ratio
Table 2. Number of DF cases per sex.
2002 5 (23,8) 16 (76,2) 21 (100) 1:3,2 Salta 2002- 2007
2003 24 (46,2) 28 (53,8) 52 (100) 1:1,2
2004 76 (45,2) 92 (54,8) 168 (100) 1:1,2
2005 6 (54,5) 5 (45,5) 11 (100) 1,2:1
2006 2 (66,7) 1 (33,3) 3 (100) 2:1
2007 69 (54,8) 57 (45,2) 126 (100) 1,2:1
Total 182 (47,8) 199 (52,2) 381 (100) 1:1,1
Age distribution
The age distribution displays an extreme dispersion going fromAge group
The majority of the operative areas reporting laboratory confirmed DF cases between 2002
and 2007 were affected in one or both of the 2004- and 2007-outbreaks (see Table 4).
Salvador Mazza (7) and Tartagal (12) reported the highest number of DF cases and are also
affected almost every year (see Map 1- 6).
Map 1, affected operative areas, Salta province 2002 Map 2, affected operative areas, Salta province 2003
Map 3, affected operative areas, Salta province 2004 Map 4, affected operative areas, Salta province 2005
Map 5, affected operative areas, Salta province 2006 Map 6, affected operative areas, Salta province 2007
22Argentina
From January 2002, when SiNaVE first introduced the electronically surveillance system, to
December 2007, 616 laboratory confirmed DF and DHF cases were reported to the National
Department of Epidemiology. Overall, 3 cases of DHF cases were registered, all in 2007 in
the Salta province. The incidence rate ranges from 0,022 (in 2006) to 0,71 (in 2007) cases per
100 000 population (see Table 5).
Year 2002 2003 2004 2005 2006 2007 Total
1
N 21 58 255 11 8 259 616
2
IR 0,057915 0,159955 0,703252 0,030336 0,022063 0,714283 1,698836
Table 5. Overall DF cases Argentina 2002- 2007. 1 Number of laboratory confirmed DF and DHF cases reported to SiNaVE. 2 Incidence rate
(per 100 000 population).
Seasonal variation
The seasonal pattern in Argentina was similar to the Salta province. Most cases were reported
in the first months of the year with a slight peak in the end of February and the beginning of
March. From epidemiological week 17 onwards the weekly report dropped, showing a
probable halt in transmission. A few cases were also reported in epidemiological week 39 to
49 (see Diagram 11).
Diagram 11, weekly DF surveillance Argentina 2002- 2007
DF Argentina 2002-2007 (N=613)
70
60
50
40
Cases
30
20
10
0
1 3 5 7 9 11 13 15 17 19 21 23 25 27 29 31 33 35 37 39 41 43 45 47 49 51 53
Epidemiological week
23Discussion
In 2007, 259 DF and DHF cases were registered in Argentina, this is the highest annual
number recorded since SiNaVE first introduced the electronically surveillance system. The
same year the first DHF cases were registered. Close to half (N=126) of the DF cases and all
(N=3) of the DHF cases in 2007 were registered by the Provincial Department of
Epidemiology in Salta. Even though the numbers are small this indicates that dengue is
increasing in Argentina and that the Salta province is in particularly high risk of dengue
epidemics in the near future.
The number of DF cases reported to SiNaVE demonstrates laboratory confirmed cases only.
The actual number can therefore be considered to be higher. Another reason to believe that
dengue incidence is underestimated is the fact that an unknown percentage of the dengue
fever infections are asymptomatic or present atypical or light symptoms. Patients who do not
seek medical advice are obviously not included in the statistics. In Salta a significant part of
the population is indigenous people living under very poor conditions which contribute to a
low report frequency (patient bias). Dengue fever can also be mistaken for other febrile
conditions such as; malaria, yellow fever, leptospirosis, hantavirus infections, among others
(doctor bias). The above mentioned biases are of unknown magnitude. In 1997 the first cases
of dengue in Argentina since 1916 were detected in the Salta province. The time span
between 1916 and 1997 (81 years) eliminates the suspicion that herd immunity could cause
over- or under-diagnosis of dengue.
The surveillance system is not optimal for analyzing incidence rates. When an outbreak is
recognized and the circulating serotype identified, case confirmation is carried out testing for
IgM antibodies instead of viral isolation. Once an outbreak is officially announced, IgM
samples are only collected from one out of five suspected DF cases. It is simple to identify an
outbreak and analyze the epidemiological pattern retrospectively but impossible to calculate
the quantity.
A dengue epidemic requires the presence of the vector mosquito (until today mainly A.
Aegypti), the dengue virus (DEN-1, -2, -3, -4) and a large number of susceptible human hosts.
Outbreaks may be explosive or progressive, depending on the density and efficiency by which
the vector can be infected, the serotype and strain of dengue virus, the number of susceptible
humans in the population, and the amount of vector-human contact.1 In the Salta province all
these variables coincide creating a surrounding in high risk of severe outbreaks in the future.
A. aegypti infestation is abundant. The vicinity to Bolivia and the concurrent movement of
people across the boarder result in introduction of new dengue virus serotypes into a highly
susceptible and previously unexposed population, a combiantion of low herd immunity and
virus import via migrant workers. A significant share of the population lives under poor
conditions in shantytowns without systems for running water or sewage. Gathering rainwater
in receptacles is an essential part of everyday life. Together with the low educational level this
give rise to great difficulties for governmental sanitary agents working preventive against
dengue.
A male predominance was expected since that has been shown in other studies36,37 and since
men are more exposed to mosquito bites, a higher proportion working outdoors in the
agricultural sector. When comparing farming to other occupations, a strong association with
DENV prevalence has been shown in other studies.38 But the distribution by sex (male:female
ratio 1:1,1) did not show any significant predominance. In contrary, the incidence rate was
slightly higher in females. Other studies have shown that the dengue case fatality rate is
higher in females.35 A hypothesis is that if women have a severe clinical picture and
subsequently seek medical advice more often. This could explain the slight female
predomination. The considerable variation observed between the different years, the ratio
24You can also read