Antifungal Susceptibility testing of Candida Species Isolates at a Tertiary Care Hospital in Central India
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
Int. J. Adv. Res. Biol. Sci. (2021). 8(3): 103-111
International Journal of Advanced Research in Biological Sciences
ISSN: 2348-8069
www.ijarbs.com
DOI: 10.22192/ijarbs Coden: IJARQG (USA) Volume 8, Issue 3 -2021
Research Article
DOI: http://dx.doi.org/10.22192/ijarbs.2021.08.03.012
Antifungal Susceptibility testing of Candida Species Isolates at
a Tertiary Care Hospital in Central India
Sanjo Gupta*, Dr Hemant B. Gadekar1
1
Department of Microbiology, RKDF Medical College & Research Centre, Bhopal
*Corresponding author: Sanjo Gupta
E-mail: sanjnagupta289@gmail.com
Abstract
Introduction: Vaginitis or Vulvovaginal candidiasis (VVC) is a most common fungal infection that affects the all-age groups of
women. Vulvovaginal candidiasis is the second most common cause of vaginitis after bacterial vaginosis and is diagnosed in 40
% women with vaginal discharge. Candida is a fungal pathogen and the common opportunistic fungi in human. Methodology:
Samples were processed using standard methods for Candida isolation. Candida speciation were performed by germ tube test and
Candida CHROM agar medium. Antifungal sensitivity pattern was performed on Mueller Hinton Agar (MHA) supplemented
with 2% glucose and 0.5 μg/ ml methylene blue dye by disc diffusion method. Result & Conclusion: Out of 350 Candida
isolated 42 (36.3%) were Candida albicans, 28 (24.1%) were Candida glabrata, 25 (22.5%) were Candida tropicalis, 12(10.3%)
Candida krusei and 9 (7.7%) Candida parapsilosis. Antifungal sensitivity pattern reveals Amphotericin Bis the most active agent
106/116 (91.3%) against Candida isolates. Conversely, the highest resistance was recorded in Ketoconazole 24 (20.6%). The
present study has shown that specie level identification of Candida isolates should be encouraged in view of the rising spate of
antimicrobial resistance to fungal agents.
Keywords: VVC, Candida, Antifungal sensitivity pattern, Candida albicans.
Introduction
Vulvovaginal candidiasis (VVC) or vaginitis is a most parapsilosis, Candida dubliniensis, Candida
common fungal infection that affects the all age guillermondii, and Candida kyfe 3,4,5,6. Candida species
groups of women. Vulvovaginal candidiasis is the are the normal floras in mucosal surfaces of the human
second most common cause of vaginitis after bacterial gastrointestinal tract, genitourinary tract, and mouth. It
vaginosis and is diagnosed in 40 % women with causes different types of diseases ranging from
vaginal discharge. Candida is a fungal pathogen and superficial infection to life threatening invasive and
the common opportunistic fungi in human1. The haematogenic infections7. Vaginal candidiasis is the
genus Candida has over 350 heterogeneous species, most common fungal disease all over the world which
but only a few of them have been known to cause an affects the female genital tract 8, 9. They are the main
opportunistic human disease2. Among the cause of vaginitis next to bacteria and is characterized
various Candida species that cause disease in human by vaginal pruritis, thick white vaginal discharge,
includes Candida albicans, Candida glabrata, itching, inflammation of vulva and dyspareunia 10.
Candida tropicalis, Candida krusei, Candida Based on the clinical presentation and antifungal
103Int. J. Adv. Res. Biol. Sci. (2021). 8(3): 103-111
response, vaginal candidiasis can be classified as at 37°C. Direct smear examination was done by 10 %
either uncomplicated or complicated. Uncomplicated KOH preparation and Gram staining.
vaginal Candidiasis, mostly caused by C.
albicans causes mild to moderate symptoms. Whereas Identification: The Candida growth on Sabouraud’s
complicated vaginal candidiasis is mostly caused by dextrose agar was confirmed by Gram staining in
non-albicans Candida species and are common among which gram positive budding fungal yeast cells were
immuno-compromised individuals and pregnant observed. The growth of Candida on SDA was
women 10.The principal agent of VVC is Candida confirmed based on colony morphology and gram
albicans, but other species known generally as stain examination. After growth species of Candida
Candida non-albicans (C. glabrata, C. tropicalis, C. were identified.
krusei, C. parapsilosis, C. gullermondii) are also
isolated. C. glabrata is the second most common Species identification: Species identification of
yeast, and its treatment is considered a serious clinical Candida isolates was done by following standard
challenge11. Candida albicans and non-albicans mycological methods including germ tube test, sugar
species are closely related but differ from each other fermentation and sugar assimilation, color of colony
with respect to epidemiology, virulence on Hi Chrome Candida agar and chlamydospores
characteristics, and fungal susceptibility, therefore formation on Corn meal agar.
Candida species identification is important for
successful management12. Prolonged therapy and Antifungal susceptibility testing: Antifungal
increased use of antifungal for recurrent candidiasis susceptibility testing was performed by disk diffusion
are the most common risk factors for azoles resistance method using Mueller-Hinton Agar, 2% Glucose with
among Candida isolates from vulvovaginitis Methylene Blue Dye Medium as per CLSI guidelines
candidiasis patients13. women with vaginal candidiasis (C.L.S.I. document M44-A2, 2009.). The Inoculum
are more susceptibility to HIV 14. Multiple studies was prepared by taking five distinct colonies of
explained a strong association of candida and diabetes approximately 1 mm in diameter from at least 24 h old
15,16,17
and preterm 18. Risk factors for VC are culture of Candida species. Colonies were suspended
pregnancy, uncontrolled diabetes, use of antibiotics, in 5 ml of sterile saline and its turbidity was adjusted
oral contraceptive, immune suppression status, over visually with the transmittance to that produced by a
use of perfume, use of contraceptive 19. Treatment for 0.5McFarland standard was used to standardize the
VC is very mild, short course. When it is left inoculums density.
untreated, it is a potent risk factor for other sexually
transmitted disease 20. Treatment for proven case of Antifungal susceptibility testing was undertaken by
VC with a short course of azolebased antifungal is the disk diffusion method. Using disk dispenser
effective, safe and affordable 21 (Oxoid™), fluconazole disk (10 μg), itraconazole (10
μg), voriconazole (10 μg), clotrimazole (10 μg) and
Materials and Methods nystatin (100 IU) antifungal discs (Thermo
Scientific™ Oxoid™) were applied on MHA (Thermo
This is a cross-sectional study was conducted during Scientific™ Oxoid™) as recommended by the Clinical
January 2018to February2020 in the Department of Laboratory Standard Institute (CLSI) M44A
Microbiology, tertiary care hospital, central India. A document.
total number of 350 patients with complain of vaginal
discharge attending department of Obstetrics & The plates were incubated in ambient air at 37°C and
Gynaecology are included in the study. read at 24 hours. The diameters of zones of inhibition
were measured in millimetres using a ruler for each
Specimen collection: antifungal disk. Interpretation of all antifungal
susceptibility (susceptible S, susceptible dose
Specimens were collected with sterile cotton swab dependent [SDD], and resistant R) was done according
from the vagina or cervix avoiding the contamination to CLSI standards (Table 1). Quality control was
of other organisms. The two swabs were collected for undertaken by using quality control strains, American
each specimen. Out of two one was used for direct Type Culture Collection (ATCC) 90028.
smear examination and another was inoculated on
Sabouraud’s dextrose agar and aerobically incubated
104Int. J. Adv. Res. Biol. Sci. (2021). 8(3): 103-111
Table 1 Interpretative breakpoints of antifungal agents
Resistant
Sensitive Intermediate/SDD
Amphotericin B
≥15 10-14 ˂10
(20 µg)
Fluconazole (10 µg) ≥19 15-18 ≤14
Clotrimazole (10 µg) ≥20 12-19 ≤11
Voriconazole (10 µg) ≥17 14-16 ≤13
Nystatin (100 U) ≥15 10-14 ˂10
C.albicans ATCC 90028 and C. parapsilosis ATCC parapsilosis and 10/112(8%) were C. krusei as shown
22019 were used as quality control. All the culture in figure1. The speciation of Candida species done by
media, Antifungal disk, and control strains were Candida HiChrom agar color of the colony and Germ
obtained from Himedia Laboratories, India. tube test presented in Table1. Candida albicans was
showing green color colonies & germ tube positive,
Results Candida glabrata shows purple color colonies and
germ tube negative, Candida krusei shows Pink color
Totally 116 Candida species were isolated from 350 colonies & germ tube negative, Candida tropicalis
high vaginal swabs. Out of 116 Candida isolates, shows Blue color colonies & germ tube negative and
74/116(63.7%) were Non-albicans Candida (NAC) Candida parapsilosis shows cream color colonies and
and 42/116(36.2%) were C.albicans. Among germ tube negative.
NAC, 26/116(22.4%) were C. glabrata, followed by
24/116(20.6%) C. tropicalis, 16/116(13.7%) C.
Table 1: Characterization of vaginal Candida isolates.
Colony on chrome
Candida species Germ tube test
agar
Candida albicans Light green +
Candida glabrata Purple -
Candida tropicalis Dark blue Later produced
Candida krusei Pink -
Candida parapsilosis Cream -
Table 2. Shows the sensitivity pattern of different Voriconazole, (86 isolate, 74.1%) was sensitive to
antifungal agents used for the 116 Candida isolates Ketoconazole, (94 isolates 81%) was sensitive to
tested (73 isolates, 62.9%) were sensitive to Nystatin and (106 isolates 99.2%) was sensitive to
fluconazole, (104 isolates, 89.6%) were sensitive to Amphotericin B.
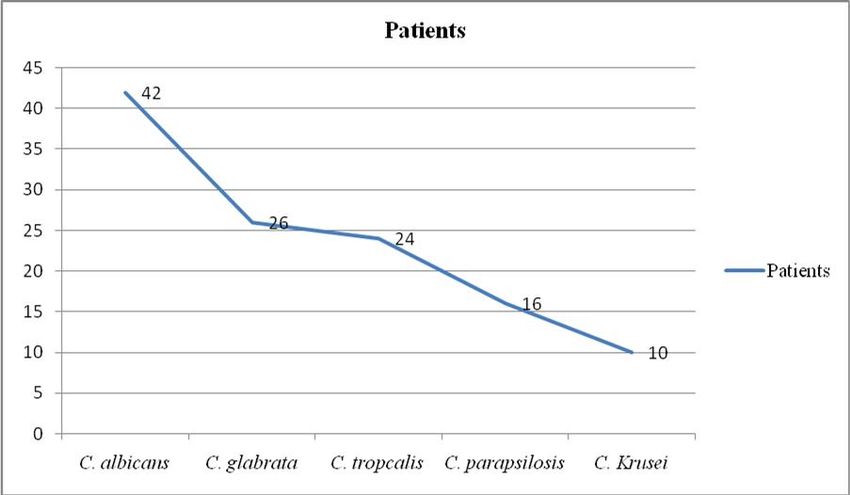
Table 2: Frequency distribution of Candida species in positive culture
Candida species No of patients (n=116) Percentage (%)
C. albicans 42 (36.2%)
C. glabrata 26 (22.4%)
C. tropcalis 24 (20.6%)
C. parapsilosis 16 (13.7%)
C. krusei 10 (8.6%)
105Int. J. Adv. Res. Biol. Sci. (2021). 8(3): 103-111
Figure 1: Frequency distribution of Candida species
Regarding Candida albicans (n=42) (35 isolates, 70.8%) susceptible to Ketoconazole, (18 isolate 75%)
83.3%) were susceptible to Fluconazole, (34 isolates, was susceptible to Nystatin and (23 isolates 95.8%)
80.9 %) were susceptible to Voriconazole, (32 was susceptible to Amphotericin B.
isolates, 76.1%) susceptible to Ketoconazole, (38
isolate 90.4%) was susceptible to Nystatin and (40 Of the 16 isolates of Candida Parapsilosis, (13
isolates 95.2%) was susceptible to Amphotericin B. isolates, 81.2%) were susceptible to Fluconazole, (16
isolates, 100%) were susceptible to Voriconazole, (13
For 76 isolates of Non albicans candida the 26 isolates isolates, 81.2%) susceptible to Ketoconazole, (11
of Candida glabrata, (21 isolates, 80.7%) were isolate 68.7%) was susceptible to Nystatin and (14
susceptible to Fluconazole, (24 isolates, 92.3%) were isolates 87.5%) was susceptible to Amphotericin B.
susceptible to Voriconazole, (19 isolates, 73.0%)
susceptible to Ketoconazole, (22 isolate 84.6%) was Of the 8 isolates of Candida krusei, (4 isolates, 50%)
susceptible to Nystatin and (24isolates 92.3%) was were susceptible to Fluconazole, (7 isolates, 87.5%)
susceptible to Amphotericin B. were susceptible to Voriconazole, (5 isolates, 62.5%)
susceptible to Ketoconazole, (6 isolate 75%) was
Of the 24 isolates of Candida Tropicalis, (18 isolates, susceptible to Nystatin and (6 isolates 75%) was
75%) were susceptible to Fluconazole, (23 isolates, susceptible to Amphotericin B.
95.8%) were susceptible to Voriconazole, (17 isolates,
106Int. J. Adv. Res. Biol. Sci. (2021). 8(3): 103-111
Table 3: Antifungal susceptibility pattern of various species of Candida
Antifungal
Amphotericin B (20 g) Fluconazole (10 g) Voriconazole (10 g) Ketoconazole(30 g) Nystatin (100 U)
Candida R
species DDS DDS DDS
R 19 17 R 15 S >15 DDS R≤10
n(%) n (%) n n (%) (%)
(%) n (%) n (%)
(%)
C. albicans 40 0 2 35 4 3 34 3 5 32 3 7 38 0 4
(n=42) (95.2) (0.0) (4.7) (83.3) (9.5) (7.1) (80.9) (8.8) (19.5) (80.9) (8.8) (16.6) (90.4) (0.0) (9.5)
C. glabrata 26 2 23 2 3 26 0 2 21 2 5 24 1 3
0
(n=28) (92.8) (7.1) (82.1) (7.6) (11.5) (92.8) (0.0) (7.1) (75) (7.6) (17.85) (85.7) (3.5) (11.5)
(0.0)
C. tropicalis 24 0 1 19 0 6 24 0 1 18 2 5 19 1 5
(n=25) (96) (0.0) (4.0) (76) (0.0) (25) (96) (0.0) (4) (72) (8) (20) (75) (4.1) (20.8)
C. parapsilosis 10 0 2 10 0 2 12 0 0 9 2 5 9 0 3
(n=12) (83.3) (0.0) (16.6) (83.3) (0.0) (12.5) (100) (0.0) (0.0) (83.3) (8) (20) (75) (0.0) (25)
C. krusei 6 0 3 5 0 4 8 0 1 1 2 7 0 3
6 (66.6)
(n=9) (66.6%) (0.0) (33.3) (55.5) (0.0) (44.4) (88.8) (0.0) (11.1) (11.1) (22.2) (77.7) (0.0) (33.3)
18
106 0 10 92 6 18 104 3 9 86 10 24 97 2
Total (15.5)
(91.37) (0.0) (8.6) (79.3) (5.1) (15.5) (89.6) (2.5) (7.7) (74.1) (8.6) (20.6) (83.6) (1.7)
S - Sensitive. DDS - Dose dependent Susceptible, R – Resistant
107Int. J. Adv. Res. Biol. Sci. (2021). 8(3): 103-111
Discussion The level of resistance to Ketoconazole found in this
study was higher (20.6%) than that to voriconazole
In our study the rate of isolation of NAC was higher (9.1%), possibly because Ketoconazole is more
63.7% than that of C. albicans 36.2%. Higher isolation frequently used than voriconazole. The resistance to
of NAC over C.albicans has also been reported by Ketoconazole is a matter of concern, not only because
Kikani B et a122(55.6% vs 44.4%), Deepa Babin et it is cost effective but also the most common azole
a123 (64.5% vs 35.5%) and Namrata et a124 (53% vs used for the treatment of candidiasis. Hence, caution
47%). needs to be practiced when prescribing and/or using
Ketoconazole. Voriconazole, on the other hand seems
However, there have been reports of higher isolation to be a better choice not only because of lower
of the commonest species, C. albicans over NAC from resistance observed against this antifungal but also
Tehran25 (65.1% vs 34.9%), Sudan 26 (92 % Vs 8%), because of more effective binding of voriconazole to
Egypt27 (60.3% vs 39.7%), Turkey 28 (59.9% vs cytochrome P-450 isoenzyme of Candida species 52
40.1%) and India29 (66% vs 34%).
In the present study, resistance to Amphotericin B was
In the present study, C. glabrata (24.1 %) was the seen in 8.6% Candida species, it being reported as
second most commonest isolate after C. albicans. It 1.37% by Kashid et a153 and zero percent by Negri
has been reported to be the second most common et54, and Dota et a1 55. Amphotericin B resistance was
isolate in cases of VVC from Saudi Arabia30 (31%), found to be 4.7% in C. albicans of our study, which is
Turkey31 (34.5%), Australia32 (20%), Egypt33 (12.7%) close to that reported by Capoor et a156and Badiee et
and India 34 (11%). a157 (4.3% and 7% respectively).
In the present study C.tropicalis was the third References
commonest isolates after C. albicans and C. glabrata.
have reported the rates of C. tropicalis isolation in
1. Kumar A, Thakur VC, Thakur S, Kumar A, Patil
cases VVC ranging between 4% to 26.4%. 34,35,36
S. Phenotypic characterization and in vitro
examination of potential virulence factors
In our study, (15.5%) Candida isolates were resistant
of Candida species isolated from a bloodstream
to fluconazole by disk diffusion method. This finding
infection. W J Sci Techno. 2011;1(10):38–42.
is close to the reports of resistance by Lee et al37
2. Williams DW, Koriyama T, Silva S, Malic S,
(17.1%) and Kustimur et a138 (16%). However, Ooga
Lewis MAO. Candida biofilms and oral
et a139, (25%) and Negri et a140 (27%), reported a
candidosis: treatment and prevention.
higher rate of resistance while, Zomorodian et
Periodontology2000. 2011; 55:250–65.
a141(3.4%), Colombo et a142 (6%), Kikani et al43
3. Oyewole OA, Okoliegbe IN, Alkhalil S, Isah P.
(8.2%) and Pfaller et a1 44 (9.9%). a lower rate as
Prevalence of vaginal candidiasis among pregnant
compared to our study.
women attending the Federal University of
Technology, Minna, Nigeria, Bosso clinic.
Resistance to fluconazole among C. albicans in our
RJPBCS. 2013;4(1):113–20.
study was 7.1%. Our findings are close to that reported
4. Deorukhkar SC, Saini S. Vulvovaginal
by Capoor et al45 (21.8%). Doddaiah V et a146however
candidiasis due to non albicans Candida: its
reported it to be in 8.6% of their C.albicans isolates.
species distribution and antifungal susceptibility
profile. Int J CurrMicrobiol App Sci. 2013;
Resistance to fluconazole has been reported in
2(12):323–8.
C. tropicalis (10-11%) and C. glabrata(31-33%) by
5. Kumar A, Sharma PC, Kumar A, Negi V. A study
several workers 147, 48, 49 though none of our isolates
on phenotypic traits of Candida species isolated
were resistant.
from bloodstream infections and in vitro
susceptibility to fluconazole. Al Ameen J Med
Resistance to voriconazole was seen in 7.7% of our
Sci. 2014; 7(1):83–91.
isolates. This is close to the findings by Das P P et a150
6. Babic M, Hukic M. Candida albicans and
(6.45%), Dalia Saad El Feky et a1 (7.9%) and Babin et
nonalbicans species as the etiological agent of
al51 (14%). Voriconazole resistance among C. albicans
vaginitis in pregnant and non-pregnant women.
of our study was seen in 21.1% isolates and in 50%
BJBMS. 2010; 10(1):89–97.
among C. parapsilosis.
108Int. J. Adv. Res. Biol. Sci. (2021). 8(3): 103-111
7. Coutinho HDM. Factors influencing the virulence Practice of Infectious diseases. 5th Ed. New
of Candida spp. West Indian Med J. 2009; York: Churchill Livingstone, 2000, 2291.
58(2):160. 20. Abebe EA, Olumide M, Oke O. A manual for
8. Kamath P, Pais M, Nayak MG. Risk of vaginal Health workers on Syndromic Management of
candidiasis among pregnant women. Int J Current STI. National AIDS and STD control program;
Microbiol App Sci. 2013; 2(9):141–6. Federal Ministry of Health Abuja, 2001, 3-7.
9. Esmaeilzadeh S, Omran S, Rahmani M. 21. JD Sobel. Vulvovaginal candidosis, Lancet.
Frequency and etiology of vulvovaginal 2007; 369(9577):1961-1971.
candidiasis in women referred to a gynaecological 22. Kikani B, Kikani K, Pathak S. Effects of
Center in Babol, Iran. Int J of Fertility and chemically synthesized azole compounds on
Sterility. 2009;3(2):74–7. clinical isolates of vaginal candidiasis, in
10. Hainer BL, Gibson MV. Vaginitis: diagnosis and comparison with commercially available drugs,
treatment. American FamPhysi. 2011; 83(7):808– Internet J Micro- biol 2008; 4:2.
15. 23. Babin D, Kotigadde, Rao Sunil P and Rao TV.
11. Kelen F. D. Dota, Alessandra R. Freitas, Marcia Clinico-mycological profile of vaginal candidiasis
E. L. Consolaro, Terezinha I. E. Svidzinski. A in a tertiary care hospital in Kerala. International
Challenge for Clinical Laboratories: Detection of Journal of Research in Biological Sciences, 2013;
Antifungal Resistance in Candida Species 3(1):55-59.
Causing Vulvovaginal Candidiasis. Journal of 24. Kalia N., Singh J., Sharma S., Kamoj S., Arora
Labmedicine February 2011 Volume 42 Number H., et al. Prevalence of Vulvovaginal Infections
2. and species specific distribution of vulvovaginal
12. Dr.Ajitha Reddy, Dr.Maimoona Mustafa. candidiasis in married women of north India. Int.
Phenotypic identification of candida species and J.of Current Microbiology and Applied Sciences
their susceptibility profile in patients with 2015; 4(8): 253-266.
genitourinary candidiasis International Journal of 25. Mahnaz Mahmoudi Rad, Ameneh Sh
Advanced Research (2014), Volume 2, Issue 12, Zafarghandi, Maryam Amel Zabihi, Mahkam
76-84 Tavallaee, and Yasaman Mirdamadi.
13. Chander J. Candidiasis. In: A textbook of Identification of Candida Species Associated with
Medical Mycology, 3rd ed. Mehta Publishers, Vulvovaginal Candidiasis by Multiplex PCR.
New Delhi, 2009; 266-90. Infectious Diseases in Obstetrics and Gynecology
14. Kamya Ramesh 7. JA Røttingen, WD Cameron, 2012.
GP Garnett. A system- atic review of the 26. Ibrahim Ali Altayyarl, AlliwaShihaAlsanosil and
epidemiologic interactions between classic NazarAbdalazeem Osman : Prevalence of vaginal
sexually transmitted diseases and HIV: how much candidiasis among pregnant women attending
really is known? Sexually Transmitted Diseases. different gynecological clinic at South Libya;
2001; 28(10):579- 597. European Journal of Experimental Biology, 2016,
15. Bohannon NJV. Treatment of vulvovaginal 6(3):25-29)
candidiasis in patients with diabetes. Diabetes 27.Dalia Saad El Feky, Noha Mahmoud Gohar, Eman
Care. 1998; 21:451-456. Ahmad El-Seidi, Mona Mahmoud Ezzat, Somaia
16. McCormack WM, Starko KM, Zinner SH. Hassan Abo Elew . Species identification and
Symptoms associated with vaginal colonization antifungal susceptibility pattern of Candida
with yeast. Am J Obstet Gynecol. 1988; 158:31- isolates in cases of vulvovaginal candidiasis.
33. Alexandria J of Med. (2016), 52, 269-277.
17. 10. Reed BD. Risk factors for Candida 28. Ayse Kalkana, Ahmet Bads Ouzel, Israa Ibrahim
vulvovaginitis. ObstetGynecolSurv. 1992; Jabban Khalil et al. Yeast vaginitis during
47:551-560. pregnancy: L Susceptibility testing of 13
18. CL Roberts, JM Morris, KR Rickard et al. antifungal drugs and boric acid and detection of
Protocol for a randomised controlled trial of four virulence factors: Medical Mycology: 2012
treatment of asymp- tomatic candidiasis for the (50); 585-593.
prevention of preterm birth 29. Chander J., Singla N., Kaur S., Sidhu S.,
[ACTRN12610000607077], BMC Pregnancy and Epidemiology of Candida blood stream
Childbirth, 2011; (11). infections; experience of a tertiary care centre in
19. John EE. Mycosis. In: Mandell G L, Bennett J E, North India: J Inject DevCtries2013; 7(9):670-
Dollin R., (editors) Textbook of Principles and 675,
109Int. J. Adv. Res. Biol. Sci. (2021). 8(3): 103-111
30. Ribeiro MA, Dietze R, Paula CR, Da Matta DA, Species from Infection and Colonization. J. Clin
Colombo AL. Susceptibility profile of vaginal Lab Anal. 2009; 25 (5):324-30.
yeast isolates from Brazil, Mycopathologia 2000; 41. Zomorodian K, Rahimi MJ, Pakshir K,
151:5-10. MotamediM, Ghiasi MR, Rezashah H.
31. Otero L, Fleites A, Mendez FJ, Palacio V, determination of antifungal susceptibility patterns
Vazquez F. Susceptibility of candida species among the clinical isolates of Candida species. J
isolated from female prostitutes with global infect Dis. 2011; 3(4): 357-60.
vulvovaginitis to antifungal agents and boric acid. 42. Colombo AL, Da matta D, De Almeida LP, Rosas
European Journal of Clinical Microbiol Infect R. Fluconazole Susceptibility of Brazilian
Disease 1999; 18: 59-61. Candida Isolates Assessed by a Disk Diffusion
32. Pfaller M., Diekema D., eta/.Stability of Mueller- 43. Kikani B, Kikani K, Pathak S. Effects of
Hinton agar Supplemented with Glucose and chemically synthesized azole compounds on
Methylene Blue for Disk Diffusion Testing of clinical isolates of vaginal candidiasis, in
Fluconazole and Voriconazole. J. Clin. Microbiol. comparison with commercially available drugs,
March 2004; (42)3: 128889. Internet J Micro- biol 2008; 4:2.
33. Galan A., Veronica V., Murgui A., et al. Rapid 44. Pfaller MA, Diekema DJ, Rinaldi MG, Barnes R,
PCR-based test for identifying Candida albicans Hu B, Veselove AV et al. Results from the
by using primers derived from the pH-regulated ARTEMIS DISK Global Antifungal Surveillance
KERI gene .FEMS Yeast research November Study: a 6.5 year analysis of Susceptibilities of
2006: vol(6) :Pages 1094-1100. Candida and Other Yeast Speciesto Fluconazole
34. Galan A., Veronica V., Murgui A., et al. Rapid and Voriconazole by Standardized Disk Diffusion
PCR-based test for identifying Candida albicans testing. J ClinMicrobiol. 2005; 43 (12): 5848-59.
by using primers derived from the pH-regulated 45. Capoor MR, Nair D, Deb M, VermaP K,
KERI gene .FEMS Yeast research November Srivastava L, Aggarwal P, Emergence of non-
2006: vol(6) :Pages 1094-1100. albicans Candida Species and Antifung.al
35. Pfaller M., Diekema D., eta/.Stability of Mueller- Resistance in a Tertiary Care Hospital. Jpn J
Hinton agar Supplemented with Glucose and Infect Dis.2005; 58(6):344-8.
Methylene Blue for Disk Diffusion Testing of 46. Doddaiah V., Dhanalakshmi T., Kulkami S.,
Fluconazole and Voriconazole. J. Clin. Microbiol. Changing trends of ulvovaginal Candidiasis.
March 2004;(42)3: 128889. Journal of Laboratory Physicians 2014; 6(1): 28-
36. Kalpana. A study on speciation and antifungal 30.
susceptibility pattern of Candida isolates from 47. Whiteway M., Bachewich C., Signal transduction
HIV patients with Oropharyngeal Candidiasis and in the interactions of fungal pathogens and
correlation with CD4 count.Madras Medical mammalian hosts. In Molecular principles of
College the Tamil nadu DR.M.G.R Medical fungal pathogenesis. Heitman J, Filler SG,
University Chennai, India march 2010. Edwards JE Jr, Mitchell AP, eds.2006; 143-161
37.Lee SC, Fung CP, Lee N, See LC, Huang JS, Tsai ASM Press, Washington DC.
CJ et al. Fluconazole Disk Diffusion Test with 48. Pfaller MA, Diekema DJ, Gibbs DL, Newell VA,
Methylene Blue- and Glucose- Enriched Muller- Meis JF, Gould IM et al. Results from the
to Fluconazole and Voriconazole by Standardized ARTEMIS DISK Global Antifungal
Disk Diffusion Testing. J ClinMicrobiol. 2005; SurveillanceStudy, 1997 to 2005: an 8.5-Year
43 (12): 5848-59 Analysis of Susceptibilities of Candida Species
38. Kustimur S, Kalkanci A, Mansuroglu H, Senel K. and Other Yeast Species to Fluconazole and
evaluation of the disc diffusion method with a Voriconazole Determined by CLSI Standardized
comparison study for fluconazole susceptibility of Disk Diffusion Testing. J Clin Microbio1.2007;
candida strains. Chin Med J.2003; 116 (4): 633-6. 45 (6): 1735-45.
39. Ooga VB, Gikunju JK, Bii CC. Characterization 49. Pfaller MA, Diekema DJ, Gibbs DL, Newell V A,
and antifungal drug susceptibility of clinical Ellis D, Tullio V et al. Results from the
isolates of candida species. Afr J Health Sci.2011; ARTEMIS DISK Global Antifungal Surveillance
19:80-7. Study, 1997 to 2007: a 10.5-Year Analysis of
40. Negri M. Henriques M, Svidzinski TI, Paula CR, Susceptibilities of Candida Species to
Oliveira R. Correlation Between Etest, Disk Fluconazole and Voriconazole as Determined by
Diffusion, and Microdilution Methods for CLSI Standardized Disk Diffusion. J Clin
Antifungal Susceptibility testing of candida Microbiol. 2010; 48 (4):1366-77.
110Int. J. Adv. Res. Biol. Sci. (2021). 8(3): 103-111
50. Das PP, SaikiaLahari, Nath R and PhukanSanjib 54. Negri M. Henriques M, Svidzinski TI, Paula CR,
Kumar. Species distribution and antifungal Oliveira R. Correlation Between Etest, Disk
susceptibility pattern of oropharyngeal Candida Diffusion, and Microdilution Methods for
isolates from human immunodeficiency virus Antifungal Susceptibility testing of candida
infected individuals. Indian Journal of Medical Species from Infection and Colonization. J. Clin
Research 2016; 143(4):495-501. Lab Anal. 2009; 25 (5):324-30.
51. Dalia Saad ElFeky, Noha Mahmoud Gohar, Eman 55. Dota KFD, Freitas AR, Consolaro MEL,
Ahmad El-Seidi, Mona Mahmoud Ezzat, Somaia Svidzinski TIE. A Challenge for Clinical
Hassan Abo Elew. Species identification and Laboratories: Detection of Antifungal Resistance
antifungal susceptibility pattern of Candida in Candida Species Causing Vulvovaginal
isolates in cases of vulvovaginal candidiasis. Candidiasis. 2011, February, Lab Medicine; 42
Alexandria J of Med. (2016), 52, 269-277. (2):87-93.
52. Regha IR. Invitro susceptibilities of Candida 56. Capoor MR, Nair D, Deb M, Verma PK,
isolates to Fluconazole and Voriconazole Srivastava L, Aggarwal P, Emergence of non-
determined by disc diffusion in a tertiary care albicans Candida Species and Antifung.al
centre. South India. Int J Res Heal Sci 2014; Resistance in a Tertiary Care Hospital.Jpn J Infect
2(3):783-6. Dis.2005;58(6):344-8.
53. Kashid RA, Belawadi S, Devi G, Indumati. 57. Badiee P, Alborzi A. Susceptibility of clinical
Characterisation and antifungal susceptibilty Candida species isolates to antifungal agents by
testing for Candida species in a tertiary care E-test, Southern Iran: A five year study. Iran J
hospital. Journal of Health Sciences and Microbio1.201 I; 3 (4): 183.
Research. 2011; 2(2):1-7.
Access this Article in Online
Website:
www.ijarbs.com
Subject:
Medical Mycology
Quick Response Code
DOI:10.22192/ijarbs.2021.08.03.012
How to cite this article:
Sanjo Gupta, Dr Hemant B. Gadekar. (2021). Antifungal Susceptibility testing of Candida Species Isolates
at a Tertiary Care Hospital in Central India. Int. J. Adv. Res. Biol. Sci. 8(3): 103-111.
DOI: http://dx.doi.org/10.22192/ijarbs.2021.08.03.012
111You can also read