Autism Spectrum Differences: Diagnosis and Management Neurodiversity day 2019 Andrew Marshall - Werry Workforce
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below

Autism Spectrum Differences:
Diagnosis and Management
Neurodiversity day 2019
Andrew Marshall
Clinical Leader – Child Health
Developmental Paediatrician / General and Community
Paediatrician
Puketiro Child Development Team / Wellington Hospital
Overview • NZ context • Diagnostic Categories • Epidemiology • Conceptual Framework for Neuromaturational Differences • Early Identification and diagnosis of ASD • Assessment process • Behavioural, Educational and Pharmacological Management
NZ ASD Guideline •Full Guideline •Summary Guideline •Māori Summary
ASD Living Guideline Reports Supplementary Papers on: • Applied Behaviour Analysis 2010 • Three Pharmacological Interventions aripiprazole, citalopram, and melatonin) 2011 • Supported Employment Services 2012 • Gastrointestinal Problems 2013 • Changes to the Diagnosis of ASD in the DSM-5 2014 • Social Skills Groups for Children and Young People with ASD 2015 • Cognitive Behaviour Therapy for Adults with ASD 2016 • The impact of ethnicity on recognition, diagnosis, education, treatment and support for people on the autism spectrum 2018 • The effectiveness of sexuality education for young people on the autism spectrum 2018 • The effectiveness of strategies for supporting school transitions for young people on the autism spectrum. 2019
ASD Guideline Definition
All display impairment in ability to:
– understand and use verbal and non-verbal
communication
– understand social behaviour, which affects
their ability to interact with other people
– think and behave flexibly which may be
shown in restricted, obsessional or repetitive
activities
• All-encompassing features, intensity may vary
depending on context and emotional state
(adapted from NZASD Guideline, 2008, p17)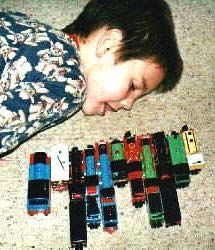
Diagnostic Categories

Diagnostic Categories ASD
Epidemiology
• Previously quoted: Autism = 5 per 10 000
• Recent studies 1 per 1000*
• Autistic Spectrum Disorders 3-4 per 1000 (some
estimates go up to 1:100 for ASD traits)
• Male:female 4:1
• Prevalence stable ? (apparent or real increase?)
* 21800 Japanese children prospective to 3 years 1.3 Autism + 0.7 Autistic Traits
Questionnaire all children 6-14 Nova Scotia (20800) 1 per 1000
Sweden 3-17yr olds 1-2 per1000 Autism, 3 per 1000 Aspergers
Why the increase ?
• Changes in diagnostic criteria over time
• Differences in methods used in studies
• Increasing awareness amongst professionals
and the wider community
• Recognition that ASD:
– occurs in association with other conditions (eg. ID,
physical disability, syndromes, psychiatric
conditions)
– could occur in people with high IQ
– presentation can be subtle.
• The question as to whether there has been a
genuine increase remains open
• Evidence for higher rates in older fathersDSM 5 Autism Spectrum Disorder
• “The proposal asserts that symptoms of these four
disorders represent a continuum from mild to
severe, rather than a simple yes or no diagnosis to
a specific disorder.
• The proposed diagnostic criteria for Autism
Spectrum Disorder specify:
1) a range of severity
2) a description of the individual’s overall developmental
status (in social communication and other relevant
cognitive and motor behaviors). News release, January 20 2012, APADSM 5 Autism Spectrum Disorder
Must meet criteria 1, 2, and 3:
1. Clinically significant, persistent deficits in social communication and
interactions, as manifest by the following:
a. Marked deficits in nonverbal and verbal communication and
interaction
b. Marked deficits in social-emotional reciprocity
c. Failure to develop and maintain peer relationships appropriate to
developmental level
2. Restricted, repetitive patterns of behavior, interests, and activities, as
manifested by at least TWO of the following:
a. Stereotyped or repetitive speech, motor movements, or use of
objects;
b. Excessive adherence to routines, ritualized patterns of verbal or
nonverbal behaviour, or excessive resistance to change;
c. Highly restricted, fixated interests that are abnormal in intensity or
focus;
d. Hyper-or hypo-reactivity to sensory input or unusual interest in
sensory aspects of environmentDSM 5 Autism Spectrum Disorder 3. Symptoms must be present in early childhood (but may not become fully manifest until social demands exceed limited capacities) 4. Symptoms together limit and impair everyday functioning • Further distinctions will be made according to severity levels. • The severity levels are based on the amount of support needed, due to challenges with social communication and restricted interests and repetitive behaviours. For example, a person might be diagnosed with ASD, Level 1, 2, or 3.
ASD 1 Mild 2 Moderate 3 Severe
Social Communication Domain
Without supports in Marked deficits in Severe deficits in
place, deficits in social verbal and verbal and
communication cause
noticeable impairments.
nonverbal social nonverbal social
Has difficulty initiating communication communication
social interactions and skills; social skills cause
demonstrates clear impairments severe
examples of atypical / apparent even with impairments in
unsuccessful responses
to social overtures of
supports in place; functioning; very
others. May appear to limited initiation of limited initiation
have decreased interest social interactions of social
in social and reduced or interactions and
interaction abnormal response minimal response
to social overtures to social
from others overtures from
others.ASD 1 Mild 2 Moderate 3 Severe
ASD Behaviour domain
Rituals and RRBs and/or Preoccupations, fixated
repetitive preoccupations or fixated rituals and/or repetitive
behaviours interests appear frequently behaviours markedly
(RRB’s) cause enough to be obvious to interfere with
significant the casual observer and functioning in all
interference with interfere with functioning spheres. Marked
functioning in one in a variety of contexts. distress when rituals or
or more contexts. Distress or frustration is routines are
Resists attempts by apparent when RRB’s are interrupted; very
others to interrupt interrupted; difficult to difficult to redirect
RRB’s or to be redirect from fixated from fixated interest or
redirected from interest. returns to it quickly.
fixated interest.Social Communication Disorder
• For those with a current diagnosis of PDD-NOS,
or who no longer fit the criteria for an Autism
Spectrum Disorder (e.g., they do not have the
RRBs), it is envisaged that their diagnosis should
move to that of the new diagnosis of SCD.
• Some research indicates that of those currently
diagnosed with Asperger’s; under the new
criteria...
– between 16 -75% will no longer fit this diagnosis, but
SCD instead.Common Features of Autism (not part of DSM 5 diagnostic criteria) • Motor Clumsiness • Anxiety • Behaviour difficulties including aggression • Sleeping and Eating issues • Auditory Processing Disorder • Attentional problems
Conceptual Framework for Neuro-
Maturational Differences
Concept 1:
Deficits are in a continuum with the normal range
Medical model diagnoses “disorder” for those outside
typical range (2 SD) – better viewed as differences
Cognition
BehaviourConceptual Framework for
Concept 2: Neuro-Maturational Differences
Neuromaturational Difficulties Overlap
Clumsiness, attention
deficits, hyperactivity,
social difficulties,
anxiety and learning
disabilities often
cluster together
Always consider the
Environment (Abuse /
Neglect / Parental
Mental Health) as
potent contributors or
causes of all these
symptomsConceptual Framework for Neuro-
Maturational Differences
Concept 3: Cause is largely polygenic
Genes
ANXIETY
ODD/CD
ADHD DAMP DCD ASPERGER SPEC LEARN
DISABILITYConceptual Framework for Neuro-
Maturational Differences
• In 2001, 4.7 % of the workforce
Concept 3: Cause is and 3.65 % of the male NZ
largely polygenic European workforce was
employed in the IT industry
• In children with Autism, 8/26 =
31% Dads worked in IT and
• All these conditions share genetic telecommunications (in 2 yr local
predisposition cohort in 2003-04 of 68)
• Autism twin studies 70-80% • Evidence that engineering, science
genetic and accountancy are over-
• 50% monozygotic concordance, represented in fathers of children
5% dyzygotic concordance with Autism
• Siblings 50-fold risk compared to • Evidence of a ‘peak and trough”
population risk
cognitive profile in Autism
• Multiple interacting genes relatives (better rote-learned and
• Family history invariably present spatial abilities and difficulties
with executive function)
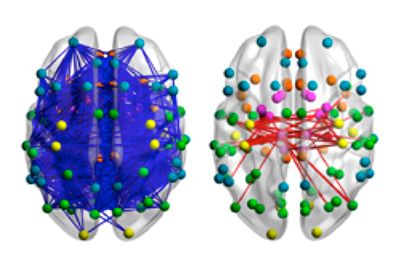
*Brain Formation
• Different parts of the brain
are activated differently in
people with autism
– Social “nodes”
– Reward activation
– Language processing
– Connectivity
• Long-distance
underconnectivity e.g.
between lobes of the brain
• Local hyperconnectivityEnvironment/Gene Interaction
Concept 4: Environment plays a significant part in the
manifestations of the
disorders
NO PROBLEM
PROBLEM Social Model of
Disability:
An impairment is only disabling if the environment is
not adapted to it (WHO)Environmental Predictors of
Triggers? Outcome
– Not MMR • Non-verbal Cognitive
Level
– Leaky gut → dietary
peptides acting as • Level of social interaction
neurotransmitters? • Level of communication
– Viral infections • Early Intervention
– In utero infections provision
– Maternal distress in
pregnancy
– Congenital
Measles/Rubella
– Metabolic conditions:
untreated PKUOverlap ASD and Transgender –
goes both ways
• Start with ASD: CBCL self-report item “wishes to be
opposite sex”:
–4-5% of ASD adolescents will answer yes vs controls* 0.7% (compare
with NZ/Netherlands rates of 1-1.5% gender diversity and 1 in 3000
transgender) *referred to clinic with non- ASD neurodevelopmental issues
• or
start with Gender diverse population and screen for
ASD:
–40-60% in clinical range in social responsiveness scale
–Amsterdam clinic diagnostic interviews 8% vs population 1%
–Birth assigned males higher rates
–RCH Melbourne transgender service 15% clients dx ASD prior, 8.3%
suspected ASDEarly Diagnosis – Why is it important? • A child’s developmental course is determined genetically, in combination with their environment • Children are “wired” to learn, and will do so unless in a deprived environment • Evidence that Early Educational Intervention improves long-term outcome
Early Diagnosis - Why is it important? • Parental concerns about their child’s development need recognition/validation • Early intervention does not require a diagnosis • However, a diagnosis serves as a “short-hand” to direct the most appropriate action at the best time • A correct diagnosis empowers by enabling understanding of needs and what the future may hold. It defines both strengths and difficulties • Beware the dangers of a diagnosis – restricting future possibilities, reinforcing society perception of normal versus abnormal, discrimination of those with differences • Accurate diagnosis must be timely, high quality and collaborative
Referral indications
What are the major
problems at home and
at preschool/school? • ADHD
• Concentration / focus • Specific Learning
• Hyperactivity Difficulty (SLD)
• Slow development • Generalised Learning
• Tearful / no friends Difficulty (ID)
• Aggressive / no friends • Autism Spectrum
• Clumsy • Anxiety
• DCD/DyspraxiaFlowchart of identification and assessment process for children
(agedCDT Wellington MDT
AssessmentAims of Assessment
Comprehensive diagnostic assessment should:
– Identify health needs (includes differential
diagnosis, aetiology and provision of genetic
advice)
– Promote understanding and agreement about
potential developmental implications, so that
effective strategies can be put in place
– Address needs of individual and family, give
confidence to provide for needs and look after own
needs.Components of Assessment • Developmental and family history • Observations across more than one setting • Cognitive / formal developmental assessment • Communication assessment • Mental health • Behaviour. • Needs and strengths of all family members • Physical examination
Investigation and Management
• Formal Audiology • Behaviour Management
• CGH microarray, Fragile X, Service (Explore)
TFTs, urine metabolic screen – Behaviour management
assessment, support and advice for
– FBC and iron studies if restricted children and adults with
diet, lead if Pica, full metabolic intellectual disability or autism
workup if regression (except for – Parent training / education
isolated language regression) (ASD+, TIPS, Teenlife etc)
• Child Development Team • WINZ
– VNDT and/or SLT and/or – Child Disability Allowance
Psychologist and/or OT – Disability Allowance (means tested)
• Special Education Early • Paediatric Follow-up
Intervention Team – Advocacy, anticipatory
– Speech Language Therapist, Guidance, medications where
Early intervention teacher, required
Psychologist
• Service organisations
• NASC (Autism NZ, Altogether
– Home Help and Respite Care Autism etc)
– Parent support
– Information sourcesTreatment and Management of
ASD
• What is “Good” treatment of ASD?
– Encourages functional development and skills
for independent living
– Minimises stress on person with ASD and
family
– But first step is comprehensive assessmentTreatments - The Advice • Treatment programmes should be individually designed • Structured educational/daily living programmes should be considered; e.g. visual cues, adapting environment increases understanding, reduces distress • Interventions should take account of the core difficulties of autism (eg, communication, social skills and stereotyped and ritualistic behaviour) • Co-morbid conditions should be treated • Effective communication strategies are often the most successful means of reducing difficult or disruptive behaviours • Family-centred treatment approaches result in greater generalisation and maintenance of skills.
Behavioural management • Consistent routine • Visual prompts to aid understanding of expectations, transitions and sequences • Modification of environment to compensate for sensory overload / overstimulation
Difficult behaviour in Autism:
Causes: Consequences:
• Anxiety – often social
anxiety • Obsessive repetitive
behaviour
• Communication
• Aggression and self
• Sensory harm
(seeking/avoiding/
• Irritability
overload)
• Hyperactivity
• “Hard-wired” /
intrinsic • Social withdrawal or
phobias
Medication trials can only be planned and managed
effectively if the cause of the target behaviour is knownPrinciples and Practice of
Pharmacotherapy in ASD
• There is no medication to treat autism, only medications to
manage some symptoms/associated behaviours
• Environmental manipulation and behavioural / educational
management always the first step and always used in
partnership with medications
• Start low, go slow, one change at a time, monitor response
• Medication trials with behavioural targets have high placebo
response
• Plan to withdraw medication in future to assess continued
benefits and side effects.
• Everything with benefits has risk
• These medications are evidence-based, but used ‘off label”
• Use the internet cautiouslyMedications
• Stimulants • Hyperactive, impulsive
– Methylphenidate behaviour and short
• (Ritalin/Rubifen) attention span
– Dexamphetamine
• Clonidine/Atomoxetine • Mixed profile
• Atypical Antipsychotics • Aggressive, disturbed,
– Risperidone anxious behaviour
• SSRI antidepressants
– Fluoxetine (Prozac) • Obsessive compulsive,
anxious behaviour
– Citalopram (Cipramil)Medications • Melatonin • Sleep • Omega 3 • General brain enhancement? • Anticonvulsants • Epilepsy (occasionally • Nutritional support behaviour) – Vitamins – Minerals – Restrictions
Summary
• ASD often presents as a social communication
and behavioural difficulty in young children,
but can be recognised throughout life
• Awareness of the genetic and environmental
contributors allows earlier recognition of risk
factors
• The earlier the diagnosis is made and
appropriate interventions are put in place the
better the outcome
Questions?You can also read