BENIGN PAROXYSMAL POSITIONAL VERTIGO (BPPV) - Tim Frith
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
BENIGN PAROXYSMAL
POSITIONAL VERTIGO (BPPV)
Tim Frith
WHAT IS BPPV? ■ inner ear disorder caused by otoconia displacement into the SCCs, which causes the acute onset of vertigo and nystagmus ■ benign – not malignant ■ paroxysmal – has sudden onset of a symptom or disease ■ positional – denotes head position as the provoking stimulus ■ rapid change of head position, resulting in vertigo and nystagmus, will subside in less than 60secs, even if the provoking head position is sustained ■ True vertigo – illusion of motion (sensation of spinning), most common symptom – is only caused by a CNS disorder 5% of the time, peripheral causes of vertigo are much more common
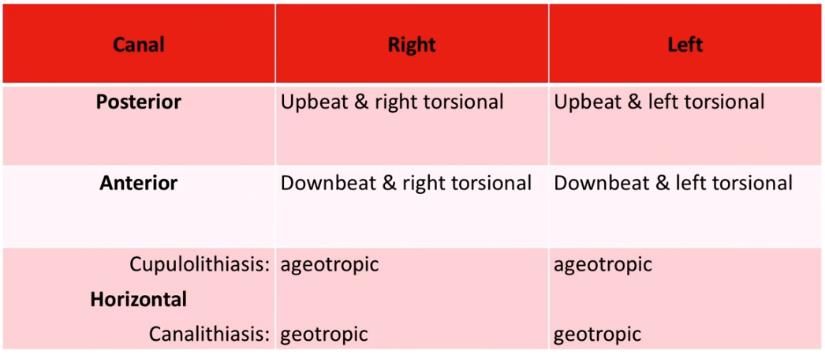
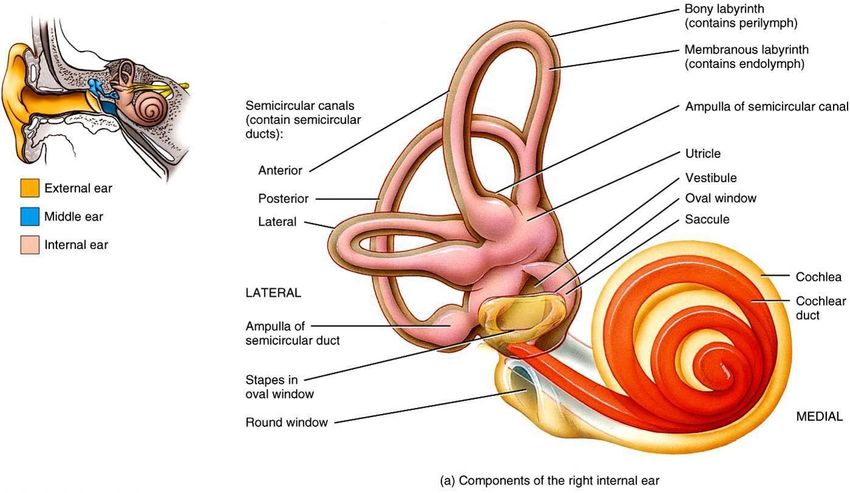
ANATOMY OF INNER EAR ■ Calcium crystals known as otoconia or otoliths usually sit within the utricle of the inner ear, in people with BPPV, the otoconia are dislodged and migrate to one of the semicircular canals ■ 3 Semi-Circular Canals – Anterior, Posterior, Lateral ➢ The posterior semicircular canal is the most commonly affected due to its anatomical position (90%)
SUBJECTIVE EXAM
SUBJECTIVE EXAM
Current History functional loss, mechanical loss?
Senses – vision (difficulties), samotosensory – proprioception, sensation loss
Recent TBI
Recent Concussion
Common (DOPP) – dizziness, Ocular (gaze instability) – oscillipsia, Postural instability,
Symptoms Perceptual dysfunction, Nystagmus, Nausea
Type of dizziness
-True vertigo (external environment moving)
-Disequilibrium (off balance, tilting sensation)
-Pre-syncope or light-headedness
Behaviour of Sudden vs gradual?
Symptoms Any associated trauma?
Aggs/eases dizziness? Change in head position, bending over look under
bed, reaching up high to shelf, turning over in bed
time course:
acute 3days
- Comes and goes – mins, secs, hours, days – continuous?
- Seconds to mins – could be - Does it fluctuate (BPPV)- positional change
- Hours to days – could be acute vestibular neuritis or stroke (check Mx hx)
- Mins to hours – TIA (HT, DM, smoking) or Meniere’s disease (fluctuating
hearing loss, episodic vertigo), migrainesSUBJECTIVE EXAM
SHx Any recent traumatic event
Older age (esp. 40-50’s) (Guar et al. 2015)
PMHx Recent concussion/TBI (17-30% of these have vestibular component (Haripriya
et al. 2018)
Previous BPPV (recurrence rate 27% esp.Symptom Likelihood
Peripheral Central
True Vertigo forOBJECTIVE EXAM
OBJECTIVE EXAM
Exam What the test is What’s a positive result What a positive
result means
Dix Hallpike Rotate patients head latency of 2-15secs before vertigo and Posterior Canal BPPV
45deg, move patient nystagmus, characteristic up or down ~90% BPPV
swiftly to supine + nystagmus, reduction of vertigo and (Guar et al. 2015)
30deg neck extension nystagmusBPPV Interpretation of Ax Findings
OBJECTIVE EXAM – IF THINKING CENTRAL!
HINTS EXAM – (Head Impulse, Nystagmus, Test of Skew)
Perform on patients with hours/days of continuous, ongoing vertigo and spontaneous nystagmus
Occulomotor Exam What the test is What’s a positive result What a positive
result means
Spontaneous/Gaze Look straight ahead Unidirectional Nystagmus Vestibular Neuritis
Holding Nystagmus Look to left only to 30deg (Reassuring) likely?
Bidirectional Nystagmus
(worse) Stroke?
Test of Skew Cover one eye, move to other Abnormal vertical skew Central (brain)
(eye gaze vertically dysfunction
deviates)
VOR function (Head Moving head, keeping eyes still Eyes dragged off target by Deficient VOR on
Impulse Test) turning the head, same side of
corrective saccade back to head turn,
target after turning head peripheral
vestibular lesion
Reassuring – Unidirectional Nystagmus, No Vertical Skew, Abnormal Head Impulse Test
Worrisome – Bidirectional Nystagmus, Vertical Skew, Normal Head Impulse Test
HINTS = better than an MRI in urgently ruling out strokeDIAGNOSIS OF BPPV ■ Sx: Nystagmus, nausea, true vertigo
PHYSIOTHERAPY MANAGEMENT OF BPPV Posterior Canal ■ Modified Epley Manoeuvre - 1-3 sessions 70-90% response -Dix Hallpike + contralateral head turn 90deg (30-60deg), turn onto contralateral side maintaining head turn (head should be facing down at 45deg from horizontal), sit up and stay an upright position for at least 10mins No postural restriction necessary (523 patients - collar for 2 days, head elevation for >1day, avoiding effected side) (Devaiah & Andreoli, 2010) https://www.youtube.com/watch?v=9SLm76jQg3g -90% patients cured after single session (Guar et al. 2015) Horizontal canal ■ Lempert (BBQ) Manoeuvre - canalithiasis (latent onset, fatigable, most provocative side) - Supine, turn head 90deg (hold 30-60secs), turn 90deg ipsilateral (face down - 30-60secs), turn 90deg (lay on side – 30-60secs), turn supine 90deg (starting position – 30-60sec), sit back up stay upright at least 10mins https://www.youtube.com/watch?v=mwTmM6uF5yA ■ Casani liberatory manoeuvre – cupulolithiasis - Lay onto side of capulolithiasis (hold 1-2mins), turn head ipsilateral (towards floor 1-2mins), sit up https://www.youtube.com/watch?v=OudVoS5UY0c
PHYSIOTHERAPY MANAGEMENT OF BPPV ■ Short term goals Assess patients with BPPV for factors that modify management, including impaired mobility or balance, central nervous system disorders, a lack of home support, and/or increased risk for falling. (Bhattacharyya et a;. 2017) Retrain gaze stability and dynamic ocular control, decrease dizziness, challenge balance in condition of visual/proprioceptive conflict, restore conditioning and endurance Educate patients regarding the impact of BPPV on their safety, the potential for disease recurrence, and the importance of follow-up (Bhattacharyya et a;. 2017) Recurrence rate 27% esp.
SUMMARY ■ BPPV can be a debilitating disorder ■ Diagnosis key! Nystagmus, nausea, true vertigo
THANK YOU
REFERENCES
■ Bhattacharyya, N., Gubbels. S., Schwarts, S., Edlow, J., Kashlan, H., Fife, T., Holmberg, J. (2017) Clinical Practice Guidelines: BPPV
(Update). Otolaryngol Head Neck Surg. S1-47
■ Cohen H. S., Kimball K. T., Stewart M. G. Benign paroxysmal positional vertigo and comorbid conditions. ORL. 2004;66(1):11–15.
■ Devaiah, A., Andreoli, S. (2010) Postmaneuver Restrictions in BPPPV: An individual patient data meta-analysis. Otolaryngology –
Head and Neck Surgery. 142(2) 155-9
■ Guar, S., Kumar, S., Saxena, R., Pathak, V., Bisht, M. (2015). Efficacy of Epley’s Maneuver in Treating BPPV Patients: A Prospective
Observational Study. Int J Otolaryngol.
■ Haripriya, G., Mary, P, Mathew, D., Goyal, R, Sahadevan, A. (2018). Incidence and Treatment Outcomes of Post Traumatic BPPV in
Traumatic Brain Injury Patients. Indian J Otolaryngol Head Neck Surg. 70(3): 337-341.
■ Korres, S., et al. (2010). "Canalithiasis of the anterior semicircular canal (ASC): treatment options based on the possible
underlying pathogenetic mechanisms." Int J Audiol 49(8): 606-612.
■ Perez, P., Franco, V., Cuesta, P., Aldama, P., Jesus Alvarez, M., Carlos, J. (2012) Recurrence Rate of Benign Paroxysmal Positional
Vertigo. 33 (3):437-43
■ Thompson, T., Amedee, R. (2009) Vertigo: A Review of Common Peripheral and Central Vestibular Disorders
■ Saberi, A., Nemati, S., Sabnan, S., Mollahoseini, F., Kazemnejad, E. (2016). A safe-repositioning maneuver for the management of
benign paroxysmal positional vertigo: Gans vs. Epley maneuver; a randomized comparative clinical trial. European Archives of Oto-
Rhino-Layngology. 274- 2973-2979.You can also read