Tramadol - interaction with SSRIs and with Morphine - September 2008 Prof E Shipton Christchurch School of Medicine Clinical Director: Pain ...
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below

Tramadol – interaction with
SSRIs and with Morphine
September 2008
Prof E Shipton
Christchurch School of Medicine
Clinical Director: Pain Management Centre
Serotonin Syndrome (SS) • all drugs that directly/indirectly central serotonin neurotransmission at postsynaptic 5-HT(2A) receptors in nervous system, on platelet surfaces, on vascular endothelium, can SS • spectrum serotonergic adverse effects to intra- synaptic serotonin concentration-related toxidrome • When serotonergic drugs with different mechanisms of action are mixed together intra-synaptic serotonin • low incidence • dose-related; rapid onset and progression (hours) • no formal test for the diagnosis of SS

Diagnosis of SS • diagnostic criteria are confusing • vague, non-specific clinical features • combination of altered mental status, neuromuscular hyperactivity, and autonomic hyperactivity • exclude common mental status adverse effects from centrally acting pharmaceuticals • Differential - neuroleptic malignant syndrome; anticholinergic delirium; malignant hyperthermia

Neuromuscular hyperactivity
Clonus,
Autonomic hyperactivity
myoclonus,
diaphoresis, fever
hyper-reflexia,
tachycardia
shivering,
tachypnoea
hypertonia,
flushing,
rigidity
hyperthermia
Altered mental status Whytes
Agitation, anxiety Distinguishing
hypomania Features
confusion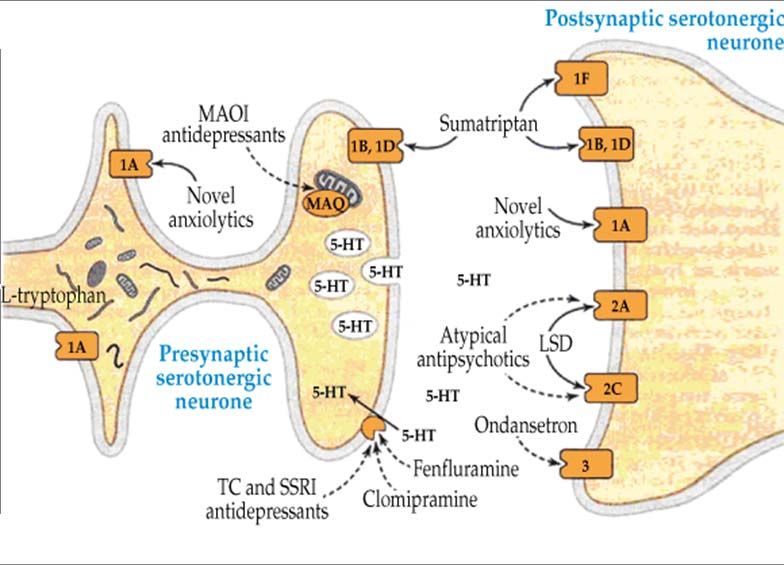
Hunter Serotonin Toxicity Criteria
Serotonergic
S
agent ingestion or E
overdose R
O
T
Spontaneous Yes O
N
clonus I
No
Agitation or N
diaphoresis or
Inducible or Plus hypertonia Yes
T
and pyrexia O
ocular clonus X
(> 38 C)
I
Plus Yes C
Tremor Hyperreflexia I
No No T
Y
Not clinically significant serotonin toxicityDrugs associated with SerotoninToxicity • SSRIs - fluoxetine, fluvoxamine, paroxetine, citalopram, sertraline, escitalopram • SNRIs - venlafaxine, duloxitine, milnacipran, sibutramine • TCAs - clomipramine, imipramine • Opioids - pethidine, fentanyl, methadone, dextromethorphan, dextropropoxyphene, tramadol • Anti-histamines - chlorpheniramine, brompheniramine • Serotonin releasers - fenfluramine, amphetamine, MDMA (ectasy) • Monoamine oxidase inhibitors – moclobemide (reversible), linzolid; tranylcypromine, phenelzine • Others - lithium, tryptophan
Pathways by which serotonin acts within the central nervous system (MJA 2007;187:361-5)
Cyproheptadine (5-HT2A antag)
12 mg orally Chlorpromazine (5-HT2A antag)
or crushed via 12.5–25 mg i.v
nasogastric after fluid
tube, then load, then 25
4–8 mg mg orally or
every 6 h iv every 6 h
Benzodiazepines
Supportive
to reduce
passive + active cooling
pyrexia,
sedation, intubation,
agitation,
muscle paralysis + ventilation
seizuresTramadol
Tramadol and SSRIs • Tramadol - atypical opioid analgesic with partial µ agonism; central re-uptake inhibition of 5HT and noradrenaline; serotonin release (induced at high doses) • Tramadol partial inhibition of serotonin uptake (especially in drug combinations) cerebral serotonin activity • SSRIs can inhibit the CYP2D6 iso-enzyme metabolising tramadol therapeutic overdose of tramadol idiosyncratic induction of SS (in susceptible individuals)
Tramadol and SSRIs • SS - rare with tramadol (less than 20 cases in PUBMED); used over 30 years with > 5 billion treatment days • Most frequent (and almost the only) fatal combination is: - MAOIs with SSRIs • Safety Practice Points - use no more than two SRI drugs; use low doses of combinations - e.g. fluoxetine 20 mg plus tramadol SR 100 mg bd - if fluoxetine dose to 40 mg, reduce and stop tramadol
Tramadol
and Morphine
• Multimodal (or balanced analgesia) is a validated
concept in the postoperative period
- combination of analgesic drugs with different
pharmacological properties
- supra-additive effects of paracetamol/tramadol on
analgesia (anti-hyperalgesia)
• Synergy between opioids reported in animal studies
• Remifentanil (0.2 ug kg-1) to tramadol (0.2 mg kg-1), with
10-min lockout times, for PCA postop analgesia +
patient comfort after abdominal surgery, without sedation or
respiratory depression (Unlugenc H. Eur J Anaesthesiol 2008; June 05:1)Tramadol and
Paracetamol
(Filitz J et al, Pain 2008;136:262-70)
Double-blind and placebo-controlled study with a
cross-over in 17 volunteers using high current
intensity TENS
(a) Pain ratings and (b) Areas
of pinprick-hyperalgesia were
significantly reduced after
combination of paracetamol
and tramadol (means ± SE).Tramadol 2500-4000 x less mu
opioid receptor
CYP2D6
(sparteine affinity vs morphine
oxidase)
O-desmethyl tramadol
inhibits 9-450 x less mu
neuronal opioid receptor
reuptake of affinity vs morphine
serotonin and
activates descending
noradrenaline
mono-aminergic inhibitory pathsTramadol
Morphine
Tramadol Morphine
Enantiomer - weak mu opioid mu opioid agonist - Activates
effect descending analgesic paths
Enantiomer – inhibits Inhibits sub P release at spinal
noradrenaline/serotonin uptake cord synapse
+ activates descending mono- Hyperpolarises post-synaptic
aminergic inhibitory paths inter-neurones
Potency (weight for weight)
intravenous 1 10
epidural 1 13Tramadol
Morphine
• Does combination increase efficacy with less
adverse effects?
Yes! No!
• Evidence from studies on post-operative pain for
tramadol/morphine combination is mixedRCT - addition of tramadol to morphine via PCA after
total knee arthroplasty
(Stiller CO et al, Acta Anaesthesiol Scand 2007;51:322-30)
Spinal anaesthesia
63 patients randomised
VAS = 40/100
Tramadol 100
VAS = 40/100
mg over 20 min PCA Saline iv every
iv every 6 h for 24h morphine B1 6 h for 24 h
(total 400 mg/24 h) mg; LO 6 min
(Max 35mg/6h)
VAS of pain, nausea, sedation - every hour for 6 h; prior
to infusion of study drugs and 1 h after infusion; final
assessment at 24 hMedian (and interquartile range) of Average VAS after
administration of tramadol 100mg 6 hourly for ‘intention to treat’
population (Mo – morphine)
(Stiller CO et al, Acta Anaesthesiol Scand 2007;51:322-30)
no significant difference in pain intensity (sedation, nausea)
Median Effective Dose of Tramadol and Morphine for
Postoperative Patients: a double-blind, randomised, two-stage
prospective study in 90 postoperative patients after slightly or
moderately painful surgery
(Marcou TA et al. Anesth Analg 2005;100:469-74)
Identical anaesthetic; Three Groups (n = 30) using an up down
allocation technique; NPS (0–10) at T0 min; at T 20 min if NPS > 3,
dose for next patient; at T 20 min if NPS < 3 dose for next patient
Tramadol group Morphine group Combined Group
initial doses 100 initial doses 5 40 (6.67) mg: 3 (0.5) mg
mg (increments mg (increments tramadol:morphine
10 mg) 1 mg dosing ratio;
isobolographic analysisPain Intensity in Three groups by NPS on arrival in Recovery (T0)
(Box plot with median, 25th–75th, and 10th–90th percentiles)
(Marcou TA et al. Anesth Analg 2005;100:469-74)
NPS was similar in the three groups with median of 5Sequence of dosing in groups
morphine, tramadol, and tramadol
+ morphine with up-and-down
allocation technique
ED50 is represented by dashed lines
no significant in adverse effects
except for dry mouth in combination
stars are failures (ineffective analgesia)
and open circles are success (effective
analgesia)Median Effective Dose of Tramadol and Morphine for
Postoperative Patients: a double-blind, randomised, two-stage
prospective study in 90 postoperative patients after slightly or
moderately painful surgery
(Marcou TA et al. Anesth Analg 2005;100:469-74)
ED50 values (95% CI) of ED50 values (95% CI) of
Tramadol = 86 mg Morphine = 5.7 mg
(57–115 mg) (4.2–7.2 mg)
ED50 of combination
was Tramadol 72 mg
(62–82 mg) and
Morphine 5.4 mg (4–
6.2 mg)
= infra-additive
?A Double-blind, RCT - addition of a Tramadol Infusion to Morphine
PCA in 69 patients after Abdominal Surgery:
(Webb AR et al. Anesth Analg 2002;95:1713-8)
end surgery initial end surgery initial
loading dose of loading dose of
Tramadol (1 mg/kg) Saline
postoperative infusion postoperative infusion
of Tramadol at 0.2 mg of Saline
kg-1 · h-1
morphine B 1
mg; LO 5 min
via PCAMean (95% CI) Values for analgesic Efficacy four hourly (1 =
excellent, 2 = good, 3 = satisfactory, 4 = poor, and 5 = very poor)
and PCA Morphine Consumption 48 h after Surgery
(Webb AR et al. Anesth Analg 2002;95:1713-8)
no evidence of increased adverse effects in patients receiving tramadol
RCT- Effects of a single dose of tramadol prior to extubation on
post-operative pain and morphine consumption after coronary
artery bypass surgery
(But AK et al, Acta Anaesthesiol Scand 2007;51:601-6)
Similar anaesthesia (fentanyl 5 ug/kg;
maintenance 30 ug/kg); propofol 1mg/kg/h to
pre-extubation)
60 Patients randomised
into two groups
Group T - Tramadol 1 Group P - 2 ml of
mg/kg 1 h before Saline 0.9% 1 h
extubation before extubation
PCA (for 24h)
morphine B1
mg; LO 7 min
Max 20mg/4hMean Post-operative Pain Scores (± SD), group P (Saline) vs.T
(Tramadol) († p < 0.01 * p < 0.05) (plus morphine PCA)
(But AK et al, Acta Anaesthesiol Scand 2007;51:601)
pain scores significantly higher 1-4 h in group P
[total morphine consumption reduced in group T over 24h (p < 0.01)]
Evidence for tramadol/morphine combination
from studies on post-operative pain
is mixed
Need more prospective double-blind randomised
controlled studies in a cross-over design or where
variables are minimisedYou can also read

















































