Treatment of prosthetic joint infection - Alex Soriano Department of Infectious Diseases Hospital Clínic of Barcelona - Infektion.net
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below

Treatment of prosthetic joint infection Alex Soriano Department of Infectious Diseases Hospital Clínic of Barcelona

Barret L, et al. The clinical presentation of prosthetic joint
infection. J Antimicrob Chemother 2014; 69: suppl 1: i25-i27
debridement, antibiotic
treatment and implant
retention (DAIR)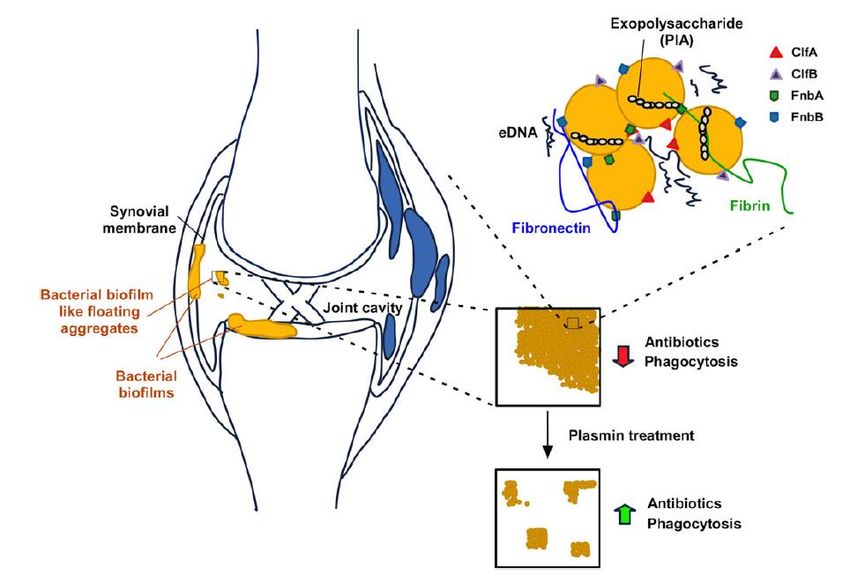
“planktonic” bacteria
bactericidal antibiotic (5-10 d)
“adapted” bacteria
anti-biofilm antibiotic (2-6 m)
“persistent” bacteria
“suppresive” antibiotic (???)
Lora-Tamayo J, et al. A Large Multicenter Study of MS and MR
Staphylococcus aureus Prosthetic Joint Infections Managed
With Implant Retention. Clin Infect Dis 2013; 56: 182–94
retrospective & multi-centric study including
345 episodes of acute PJI
MSSA: i.v. cloxacillin
MRSA: i.v. vancomycin
1m
Tornero E, et al. KLIC-score for predicting early failure in
acute prsothetic joint infections treated with DAIR
Clin Microbiol Infect 2015; 21: 786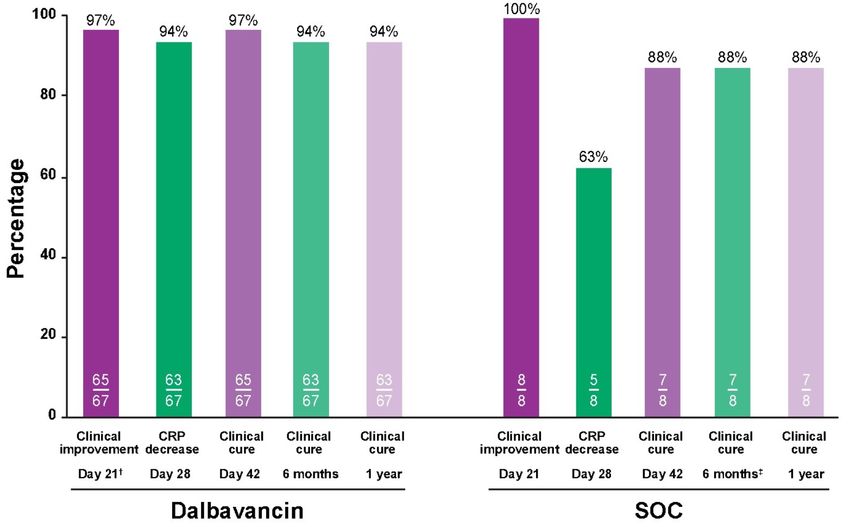
Tornero E, et al. KLIC-score for predicting early failure in
acute prsothetic joint infections treated with DAIR
Clin Microbiol Infect 2015; 21: 786
5%
Tornero E, et al. KLIC-score for predicting early failure in
acute prsothetic joint infections treated with DAIR
Clin Microbiol Infect 2015; 21: 786
N=114 N=54 N=36
% remission / failure
(56%) (26%) (18%)
C-reactive protein before debridement (mg/dL)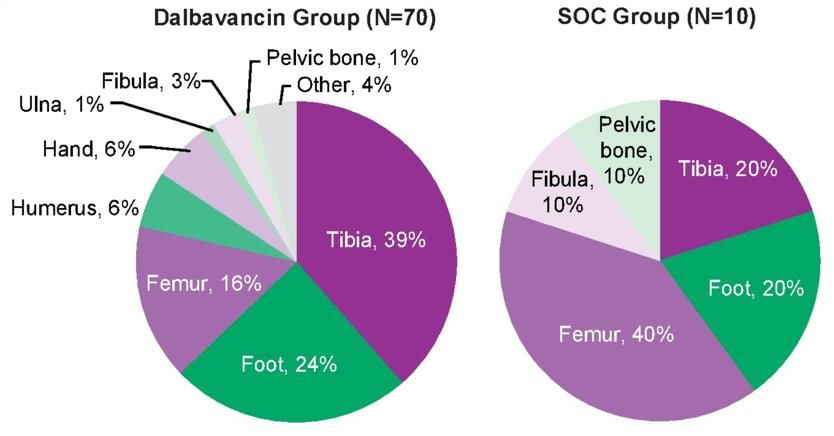
Tornero E, et al. KLIC-score for predicting early failure in
acute prsothetic joint infections treated with DAIR
Clin Microbiol Infect 2015; 21: 786
high planktonic
bacterial load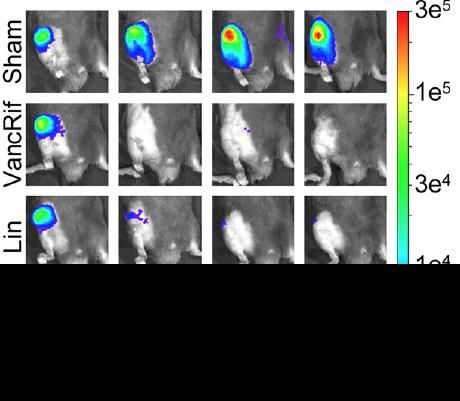
Dastgheyb S, et al. Staphylococcal Persistence Due to Biofilm
Formation in Synovial Fluid Containing Prophylactic Cefazolin.
Antimicrob Agents Chemother 2015; 59:2122–2128
Staphylococcus aureus
x10 PIA/PNAG 3D- confocal
staining laser microscopy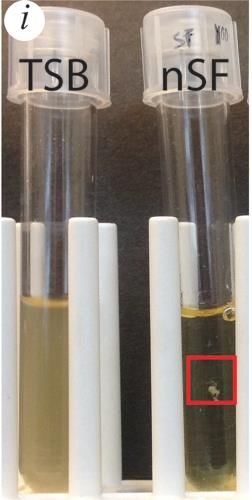
Dastgheyb S, et al. Effect of Biofilms on Recalcitrance of
Staphylococcal Joint Infection to Antibiotic Treatment.
J Infect Dis 2015; 211: 641-50Dastgheyb S, et al. Effect of Biofilms on Recalcitrance of
Staphylococcal Joint Infection to Antibiotic Treatment.
J Infect Dis 2015; 211: 641-50Thompson JM, et al. Oral-Only Linezolid-Rifampin Is Highly Effective
Compared with Other Antibiotics for Periprosthetic Joint Infection
J Bone Joint Surg (Am) 2017; 99:656-65
1. inoculum 103 CFU of bioluminiscent MRSA
2. After a 2-week incubation period to allow biofilm
formation on the Kirschner
3. Antibiotic treatment (or sham treatment with saline
solution) was initiated for 6 weeks with doses that
approximate human-exposure doses according to the
AUC and differences in serum drug protein binding
between mice and humansThompson JM, et al. Oral-Only Linezolid-Rifampin Is Highly Effective
Compared with Other Antibiotics for Periprosthetic Joint Infection
J Bone Joint Surg (Am) 2017; 99:656-65
1. inoculum 103 CFU of bioluminiscent MRSA
2. After a 2-week incubation period to allow biofilm formation on the
Kirschner
3. Antibiotic treatment (or sham treatment with saline solution) was
initiated for 6 weeks with doses that approximate human-exposure
doses according to the AUC and differences in serum drug protein
binding between mice and humansThompson JM, et al. Oral-Only Linezolid-Rifampin Is Highly Effective
Compared with Other Antibiotics for Periprosthetic Joint Infection
J Bone Joint Surg (Am) 2017; 99:656-65
culture results after 6 weeks of treatmentAchermann Y, et al. Factors associated with rifampin
resistance in staphylococcal periprosthetic joint infections
(PJI): a matched case–control study.
Infection 2013; 41: 431-7
variable P-value
male 0.02
≥3 prior revision surgeries 0.006
rifampin treatment“planktonic” bacteria
bactericidal antibiotic (5-10 d)
• debridement + PE exchange
• C-RP < 10 mg/dL: cloxacillin / linezolid / daptomycin /ceftaroline
• C-RP ≥ 10 mg/dL: association of ≥2 atb (fosfomycin)
• Local antibiotics ?: gentamicin beads have been associated
with a worse outcome (Lowik C, et al. J Arthroplasty 2018)
“adapted” bacteria
anti-biofilm antibiotic (2-6 m)Otero LH, et al. How allosteric control of Staphylococcus aureus penicillin
binding protein 2a enables methicillin resistance and physiological
function. PNAS 2013; 110: 16808-16813
PBP2A (MRSA)
ß-lactams bind in a
distal site
(alosteric site)
Mahasenan KV, et al. JACS 2017; 139; 2102-2110Saravolatz LD, et al. Ceftaroline: A Novel Cephalosporin with
Activity against Methicillin-resistant Staphylococcus aureus
Clinical Infectious Diseases 2011;52(9):1156–1163
MIC90 (µg/mL)
MIC90 (µg/mL). For GNB, has an activity similar to ceftriaxoneRemission rates with different oral antibiotic regimens in
staphylococcal prosthetic joint infections
Senneville CID Tornero IJAO
2011 N=98 (%) 2012 N=106 (%)
Surgical treatment: DAIR or Ex DAIR
Microorganims: S. aureus S. aureus & CoNS
Oral options*:
FQ+Rif 37/39 (94.8) 44/50 (88)
LNZ (+/-Rif) 9/11 (81.8) 26/32 (81)
others 31/48 (64.5) 22/28 (78.5)
v
* after 1 week of intravenous antibiotic with vancomycin and a ß-lactamViale P, et al. Treatment of pyogenic (non-tuberculous)
spondylodiscitis with tailored high-dose levofloxacin plus
rifampicin
Int J Antimicrob Agents 2009; 33: 379-82
Levo (750 mg/24h) + rifa 600 mg/24hZeller V, et al. Continuous Clindamycin Infusion, an
Innovative Approach to Treating Bone and Joint Infections
Antimicrob Agents Chemother 2010; 54: 88-92
Continuous infusion 30-40 mg/kg/24h (2-3 g/24h for 70 kg)
30-40%Ribera E, et al. Rifampin Reduces Concentrations of Trimethoprim
and Sulfamethoxazole in Serum in HIV-Infected Patients.
Antimicrob Agents Chemother 2001; 45: 3238-41
Serum concentration of trimethroprim
decreased 47% and sulfametoxazol 23%Gandelman K, et al. Unexpected Effect of Rifampin on the
Pharmacokinetics of Linezolid: In Silico and In Vitro
Approaches to Explain Its Mechanism.
J Clin Pharm 2011; 52: 229-236
Linezolid 600 mg Linezolid 600 mg +
Rifampicina 600 mgTornero E, et al. Importance of selection and duration of
antibiotic regimen in prosthetic joint infections treated with
debridement and implant retention
J Antimicrob Chemother 2016; 71:1395-1401
grampositives
Lev+Rif Lin+Rif LinPushkin R, et al. A Randomized Study Evaluating Oral Fusidic Acid (CEM-102)
in Combination with Oral Rifampin Compared with Standard of Care
Antibiotics for Treatment of Prosthetic Joint Infections: A Newly Identified
Drug-Drug Interaction. Clin Infect Dis 2016; 63: 1599-1604.
FA (1200-1500 mg/24) +
RIF (450 mg/12h) n= 7
Stopped RIF
2 failures
1 MRSA – RIF-R“planktonic” bacteria
bactericidal antibiotic (5-10 d)
• debridement + PE exchange
• C-RP < 10 mg/dL: cloxacillin / linezolid / daptomycin /ceftaroline
• C-RP ≥ 10 mg/dL: association of ≥2 atb (fosfomycin)
• Local antibiotics ?: gentamicin beads have been associated
with a worse outcome (Lowik C, et al. J Arthroplasty 2018)
“adapted” bacteria
anti-biofilm antibiotic (2-6 m)
• levofloxacin (500 mg/24h) + rifampin (600 mg/24h)
• cotrimoxazol, clindamycin, linezolid, minocycline? +/- rifampinCheng M, et al. Anti-cooperative ligand binding and dimerisation
in the glycopeptide antibiotic dalbavancin.
Org. Biomol. Chem 2014; 12: 2568
dalbavancin (derivative of teicoplanin)Mature PG
Trans-
peptidation
Trans-
GP (dalbavancin) glycosilation
Nascent PG
C55 PBP
MIC90 (mg/L) for MIC90 (mg/L) for
Antibiotic Staphylococcus spp Enterococcus spp
dalbavancin 0.06 0.06-0.12
vancomycin 2 2
daptomycin 0.5 2Dorr MB et al. Human pharmacokinetics and rationale for once-
weekly dosing of dalbavancin, a semi-synthetic glycopeptide
J Antimicrob Chemother 2005;55 (Suppl2):25-30
Renal adjustment:
300
- GF20 mg/L, PBS frente a SARM*
0
0 8 14 days
1000 mg (30’) 500 mg (30’)
1500 mg (30’) * Leighton, et al. AACh 2004Dunne MW, et al. Extended duration dosing and distribution
of dalbavancin into bone and articular tissue.
Antimicrob Agents Chemother 2015; 59:1849 –1855
1000 mg DLBRappo U, et al. Long-term outcomes of dalbavancin for the
treatment of osteomyelitis in adult patients.
28th ECCMID 2018, Madrid, Spain. Abst 697
* implant-associated infections were excludedRappo U, et al. Long-term outcomes of dalbavancin for the
treatment of osteomyelitis in adult patients.
28th ECCMID 2018, Madrid, Spain. Abst 697
1500 mg day 1
1500 mg day 7Rappo U, et al. Long-term outcomes of dalbavancin for the
treatment of osteomyelitis in adult patients.
28th ECCMID 2018, Madrid, Spain. Abst 697Barret L, et al. The clinical presentation of prosthetic joint
infection. J Antimicrob Chemother 2014; 69: suppl 1: i25-i27
debridement, antibiotic treatment and implant retention
(DAIR)Wouthuyzen-Bakker, M et al. Late acute prosthetic joint infections
treated with DAIR; outcome and risk factors for failure (ESGIAI).
340 patients (27 centers) Definition:
< 3 weeks of symptoms
> 3 months after the index surgery
a prior history of normal function
60%
% survival
45%
27%
Failure:
related death
Prosthesis removal
Suppressive therapyWouthuyzen-Bakker, M et al. Late acute prosthetic joint infections
treated with DAIR; outcome and risk factors for failure (ESGIAI).
Variables OR P-value
Fracture as indication for prosthesis 5.4 0.01
Rheumatoid arthritis 5.1 0.04
Chronic obstructive pulmonary disease 2.9 0.05
Age above 80 years 2.6 0.02
Male Gender 2.0 0.04
C-reactive protein > 150 mg/L 2.0 0.04
Exchange of mobile components 0.35 0.002
340 patients (27 centers)Wouthuyzen-Bakker, M et al. Late acute prosthetic joint infections
treated with DAIR; outcome and risk factors for failure (ESGIAI).
19
% failure
56
124
68 340 patients
18 (27 centers)Wouthuyzen-Bakker, M et al. Late acute prosthetic joint infections;
should the imlant be removed? (ESGIAI).
Implant removal (n=105)
75%
% survival
55%
Implant retention (n=340)
A propensity-matching score analysis (81:81)
confirm these results (48% vs. 74%, P=0.001) 445 patients
(27 centers)Wouthuyzen-Bakker, M et al. Late acute prosthetic joint infections;
should the imlant be removed? (ESGIAI).
Late acute PJI (n=395) % of FAILURE
CRIME80 ≥ 3 n=107 CRIME80 < 3 n=288
(retention 83% vs. removal 31%)
S. aureus (n=125) other (n=163)
(retention 45% (retention 29%
vs. removal 25%) vs. removal 23%)
No RA
PE exchange
CRPKunutsor SK, et al. One- and two-stage surgical revision of peri-
prosthetic joint infection of the hip: a pooled individual participant
data analysis of 44 cohort studies.
Eur J Epidemiol 2018; 97: 1368
Reinfection rates per 1000 person-years of
follow-up were 16.8 (95% CI 13.6–20.7) and
32.3 (95% CI 27.3–38.3) for 1-stage and 2-
stage strategies respectively.EUROPEAN BONE AND JOINT INFECTION SOCIETY 6-8 SEPTEMBER 2018 - HELSINKI, FINLAND The conference will be held in the white marble and granite faced Finlandia Hall. The congress venue is situated beautifully in a park near the sea in the centre of Helsinki, in the vicinity of several hotels- DEADLINES ABSTRACT SUBMISSION: 20 APRIL 2018 EARLY REGISTRATION: 1 JULY 2018 We look forward to welcoming you to Helsinki!
You can also read

















































