BIOSIMILARS Biosimilars for Hematologic Malignancies
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
Biosimilars for Hematologic Malignancies:
Dissecting Real-World Evidence and Barriers to Utilization
BIOSIMILARS
Biosimilars for Hematologic Malignancies:
Dissecting Real-World Evidence and Barriers to Utilization
Thank you for joining us, I am Dr. Charles Bennett. I'm an MD, PhD, hematologist-
oncologist, and I'm what's called a SmartState Chair and Director at the SmartState Center
at the University of South Carolina. It's one of 47 endowed chairs in the state of South
Carolina and my program focuses on medication safety and efficacy.
With me for presentation are Dr. Marc Fishman, founder, and chairman of the Board of
Directors of Oncology Analytics Incorporated, it's in Atlanta, Georgia, and Dr. Kevin Knopf,
the Chief in the Section of Hematology/Oncology at Alameda Health Systems and Highland
Hospital, which is Oakland, California.
©2021 MediCom Worldwide, Inc. 1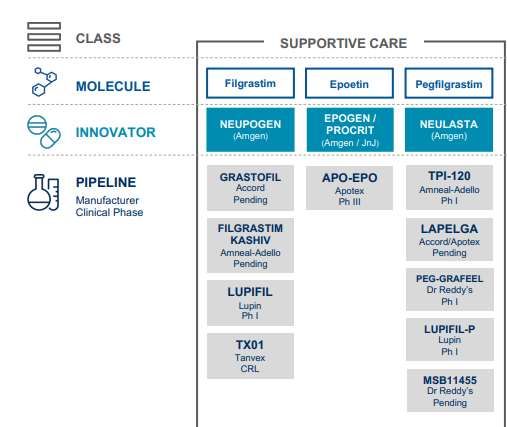
Biosimilars for Hematologic Malignancies:
Dissecting Real-World Evidence and Barriers to Utilization
Disclosures
• Dr. Charles Bennett has disclosed no relevant financial relationships.
• Dr. Marc Fishman has disclosed no relevant financial relationships.
• Dr. Kevin Knopf has disclosed no relevant financial relationships.
©2021 MediCom Worldwide, Inc. 2Biosimilars for Hematologic Malignancies:
Dissecting Real-World Evidence and Barriers to Utilization
Learning Objectives
At the conclusion of this activity, participants will be able to:
• Identify key scientific factors surrounding biosimilarity and drug
interchangeability of biosimilar agents
• Distinguish potential clinical and regulatory challenges to uptake of
biosimilars for supportive care in patients with hematologic cancer
• Outline and overcome barriers and care disparities related to uptake and
adoption of biosimilars in comparison to their biologic originator drug
In today's presentation, we're going to provide information on key scientific factors that are
around biosimilarity and also address drug interchangeability, which is one of the most
confusing terms we have today in biosimilars. We're going to talk about potential clinical
and regulatory challenges to the uptake of biosimilars for supportive care in cancer patients
in the United States, particularly those with hematologic malignancies, and we'll discuss
the challenges and opportunities to overcome barriers and the care disparities related to
the uptake and adoption of biosimilars in comparison to original biologics. We'll have that
as the third part of the presentation today.
©2021 MediCom Worldwide, Inc. 3Biosimilars for Hematologic Malignancies:
Dissecting Real-World Evidence and Barriers to Utilization
Global Cancer Biologics Market
Current and Anticipated Growth of Global Cancer Biologics Market
100 CGAR 7.2%
90
Global Market ($billion)
$93
80 CGAR 6.9%
70
$71
60 $66
50
40
30
20
10
0
2020 2021 2025
Cancer Biologics Global Market Report 2021. Global Cancer Biologics Market Data And Industry Growth Analysis (thebusinessresearchcompany.com)
Let's talk about the global cancer biologics market. Very simple slide here, showing that the
growth of the cancer market is about 7.2% to $93 billion in 2025 estimated and it was 6.9%
in 2021. In 2020, it was about $66 billion. If you look overall, you've gone from a left bar of
$66 billion to the right bar of $93 billion, a huge anticipated growth of the cancer global
market. This is the entire world at the same time.
©2021 MediCom Worldwide, Inc. 4Biosimilars for Hematologic Malignancies:
Dissecting Real-World Evidence and Barriers to Utilization
Biologic Drug Therapies
• Biologic oncology products are integral to the treatment of cancer patients
– Cell therapies, cytokine or growth factors, monoclonal antibodies, and monoclonal
antibody-drug toxin combinations
• Median annual cost of biological therapy for oncology/hematology per
person: $142,833
• Patents for therapeutic originator biologic supportive and therapeutic
oncology drugs have expired in most countries, giving way to improved
healthcare costs, access, and outcomes for a large number of cancer patients
internationally with off-patent biosimilar molecules
World Health Organization. Technical Report: Pricing of cancer medicines and its impacts. 2018.
https://www.rdmag.com/article/2016/12/new-rules-engagement-challenges-associated-commercializing-biosimilars
Biologic drug therapies are integral to treat cancer patients. These include cell therapies,
cytokines, growth factors, monoclonal antibodies, and monoclonal antibody-drug toxin
combinations, and they're all produced, and we'll go into that a little bit later, in a living
system, which makes them complex to produce. Given their complexity, they're expensive.
The median annual costs of biologic therapy for oncology hematology biologics today are
about $142,000 per patient. Really difficult to think of that number.
©2021 MediCom Worldwide, Inc. 5Biosimilars for Hematologic Malignancies:
Dissecting Real-World Evidence and Barriers to Utilization
What Are Biosimilars?
• The U.S. Food and Drug Administration: A biosimilar is a biological
product that is highly similar to and has no clinically meaningful
differences from an existing FDA-approved reference product.
(Biosimilars formally established by FDA in 2015)
Highly similar: No clinically meaningful differences:
• Extensively analyzed structure and • In terms of:
function of reference product and ‒ Safety
biosimilar ‒ Purity
• Compared characteristics (purity, chemical ‒ Potency
identity, etc.) • Demonstrated through human PK/PD
• Minor differences in clinically inactive studies and assessment of clinical
components are acceptable immunogenicity
U.S. Food and Drug Administration. https://www.fda.gov/drugs/biosimilars/biosimilar-and-interchangeable-
products#:~:text=A%20biosimilar%20is%20a%20biological,existing%20FDA%2Dapproved%20reference%20product.
The US Food and Drug Administration, our regulatory agency, they have defined a
biosimilar. It's a biological product that is highly similar, highly similar to, and has no
clinically meaningful differences from the existing FDA-approved reference biologic. These
were formally established by the FDA in 2015, a full decade after they were established in
Europe. On the left, you can see in the shaded region, highly similar, they're extensively
analyzed, they have comparative characteristics, and they have minor differences that are
acceptable. On the right, we show that they have no clinically meaningful differences in
terms of safety, purity, and potency, and they're demonstrated through human studies,
pharmacokinetics, pharmacodynamics, and immunogenicity to be about the same as the
parent drug.
At this point, I'd like to turn it over to Kevin, Dr. Knopf, to continue the discussion on a few
of the clinical considerations we do and use in demonstrating biosimilarity.
©2021 MediCom Worldwide, Inc. 6Biosimilars for Hematologic Malignancies:
Dissecting Real-World Evidence and Barriers to Utilization
Fundamental Principles for Establishing
Clinical Biosimilarity
• Goal of biosimilar clinical trial is to demonstrate similar efficacy and safety compared with
reference product ‒ not to reestablish benefit
• The clinical trial program for a potential biosimilar includes assessments of PK, if feasible,
PD, efficacy, and safety
– Short-term surrogate endpoints (ORR, pCR). Can be 1-arm or 2-arm study. In some settings, no clinical trials
with cancer patients are needed for FDA approval of oncology biosimilar. Hence, preclinical data constitute
90% of the dossier
Degree of analytical and
functional similarity
REFERENCE
BIOSIMILAR
BIOLOGIC Comparative Clinical
Assessment
PK/PD Safety
Efficacy
Stebbing J, et al. J Clin Oncol. 2020;38:1070-1080.
Dr. Kevin Knopf: Thank you. The goal of biosimilars is to lower the cost of care in cancer
and other areas where they're used, in clinical trials to establish similar efficacy and safety
compared with a reference project, not to re-establish benefit. The way I think about it is
the way I think about a generic drug that the biosimilar drug works as well as the reference
product. The clinical trial program includes the assessments of pharmacokinetics, if
possible, pharmacodynamics, efficacy, and safety, and the use of short-term surrogate
endpoints with one arm or two-arm studies. In some settings, no clinical trials of cancer
patients are needed for FDA approval of the oncology biosimilar and preclinical data can
constitute 90% of the dossier.
©2021 MediCom Worldwide, Inc. 7Biosimilars for Hematologic Malignancies:
Dissecting Real-World Evidence and Barriers to Utilization
Clinical Considerations in Demonstrating Biosimilarity
Patient Population • Most sensitive population to show clinically meaningful differences
• Based on dose-response curve
Dose
• Chosen to sensitively detect any differences
• Chosen to enable precise and meaningful comparison to the
End Points reference biologic
• Non-inferiority or equivalence margins
Design
• Parallel or crossover (depending on half-life)
FDA Guidance for Industry. Scientific Considerations in Demonstrating Biosimilarity to a Reference Product, 2015.
Clinical considerations in demonstrating biosimilarity, the patient population that is of
interest for the reference drug and the biosimilar drugs should show clinically meaningful
benefit or differences. The dose including the pharmacokinetics, the dose-response curve
can be chosen to sensitively detect any differences between the biosimilar and the
reference drug, the endpoints to enable precise and meaningful comparisons to reference
biologic and the design of the trial, typically non-inferiority or equivalents, parallel or cross
over depending on the half-life of the agent.
©2021 MediCom Worldwide, Inc. 8Biosimilars for Hematologic Malignancies:
Dissecting Real-World Evidence and Barriers to Utilization
Biosimilars vs Generics: Brief Comparison
Biosimilars Generics
Originated from Biologic medicines Conventional medicines
Development paradigm Highly similar and not identical to the originator (comparative studies) Bioequivalent and identical to the
originator (bioequivalence studies)
Approval procedure Usually approved from central regulatory authorities EMA or FDA Usually approved from national
regulatory authorities of EU or FDA
Immunogenicity Yes No
Nomenclature Trade names or the use of distinguishable names with distinct suffixes INN names
Interchangeability Not yet assessed, established or approved Yes
Substitution Not yet assessed, established or approved Yes
ADR Report the INN name manufacturer and batch number Report the INN name
Risk management plan Yes No
Price discount 20%-30% discount over originator 80%-90% discount over originator
Timeline development 8-10 years 3-5 years
Development cost $100–$200 M $1–$5 M
Halimi V, et al. Int J Environ Res Public Health. 2020;17(6):5800.
Dr. Charles Bennett: As you can see in there, on those kinds of issues, when we talk about
biosimilars and generics, these should look very different, even though they sound like they
should be the same. Biosimilars are biologic medicines. Generics, these identical twins are
conventional medicines. They developed biosimilars, they're shown- as Dr. Knopf just
mentioned, they both should be highly similar and not identical to the originator. Then you
see in generics, the second row on this slide, they're supposed to be identical , just like
identical twins to originator, bioequivalence studies, this is really a key distinction. The
approval in the third row of the biosimilars, they get EMA or the FDA will approve these
products, whereas the generics, they get approved by the countries rather than in Europe,
each individual country or the FDA. In the fourth row, you can see that biosimilars have
really a potential to be immunogenic, generics have none. The nomenclature in the fifth
row, they use the tradenames or they use the usual names with different suffixes. Those of
you who are starting to use some generics right now, you might get into some names that
sound so foreign because they may not be similar to the names that you would have used
with the reference drug, whereas the generics, they used the basic generic drug name.
Interchangeability, the next row, is an important concept. It means what it says,
interchangeable, you can change one out for the other, but the FDA has not yet assessed,
established, or approved a single interchangeable biologic yet. Generics, they all are
interchangeable, which means if you get the prescription for generic A today and generic B
next month, you're good to go. On the other hand, with interchangeable, biosimilar A, this
©2021 MediCom Worldwide, Inc. 9month, you're not good to go to biosimilar B next month, they're not interchangeable yet.
Substitution, next row, is not yet assessed again or established, or approved. Substitution is
when rather than you decide which one you might want, the substitution would be the
pharmacist might say, "Let's give you biosimilar A today." Generics, always, you go in and the
pharmacist has the ability to substitute the generic for the primary drug unless the physician
says not to do so. If you get an adverse drug reaction, they want you to report both the name
of the drug and the batch number because the batch number could be faulty. On the other
end, in generics, you put just the name of the drug. The risk management plan is by the FDA,
and that is where they're carefully looking to see if there are any risk management issues,
and this is done on all biosimilars, not done on generic. Price discounting, we're looking at
about 20% to 30% price discount over the originator is what we try to see in the US,
whereas, in the generics, it's a good 80% to 90% discount. How long does it take to develop
these things? Biosimilar is about 9 to 10 years, generic 3 to 5 years. How much does it cost to
develop these drugs? It costs $100 million to $200 million for development costs for
biosimilars and a million to $5 million for generic, and that explains to you very quickly why
certain companies have to be well-capitalized, well-financed to do biosimilar production,
whereas the generics have a plethora of generic manufacturers.
9Biosimilars for Hematologic Malignancies:
Dissecting Real-World Evidence and Barriers to Utilization
Biosimilars: EU Experience
• Biosimilar adoption has been greater in the European Union (EU)
compared to the US, in part due to differences in lower rates of
regulatory disapproval of initial dossiers and fewer patent lawsuits
brought against the biosimilar sponsor
• Biologics in the EU are often procured through government
contracts to reduce expenditures
• While biosimilar use in the US is rising, currently they comprise an
estimated 2.3% of all biologics in the country compared to 90% in
the EU
Generics and Biosimilars Initiative (GaBI). Approval and launch dates for US biosimilars. Accessed at https://www.gabionline.net/Reports/Approval-
and-launch-dates-for-US-biosimilars, April 16, 2021.
Bennett CL, et al. Lancet Oncol. 2020;21(12):e575-e588.
As I mentioned in the beginning, biosimilars have been in place in Europe since 2005, 2006,
10 years before us.
In the United States, it's rising, biosimilars, but they compromise only 2.3% of all biologics
in the country compared to 90% in the EU.
Marc, Dr. Fishman, why don't you talk to us now about the US experience with biosimilars?
©2021 MediCom Worldwide, Inc. 10Biosimilars for Hematologic Malignancies:
Dissecting Real-World Evidence and Barriers to Utilization
29 FDA-Approved Biosimilars
Reference Biosimilar Approval date Reference Biosimilar Approval date
product product
(Renflexis) Infliximab-abda April 2017
(Hyrimoz) Adalimumab-adaz October 2018
Infliximab (Avsola) Infliximab-axxq December 2019
(Amjevita) Adalimumab-adbm August 2017
(Remicade) (Inflectra) Infliximab-dyyb April 2016
Adalimumab (Abrilada) Adalimumab-afzb November 2019
(Ixifi) Infliximab-qbtx December 2017
(Humira) (Amjevita) Adalimumab-atto September 2016 (Fulphila) Pegfilgrastim-jmdb* June 2018
(Hadlima) Adalimumab-bwwd July 2019 Pegfilgrastim (Udenyca) Pegfilgrastim-cbqv* November 2018
(Hulio) Adalimumab-fkjp July 2020 (Neulasta) (Ziextenzo) Pegfilgrastim-bmez* November 2019
(Mvasi) Bevacizumab-awwb* September 2017 (Nyvepria) Pegfilgrastim-apgf June 2020
Bevacizumab
(Avastin) (Truxima) Rituximab-abbs* November 2018
(Zirabev) Bevacizumab-bvzr June 2019 Rituximab
(Ruxience) Rituximab-pvvr July 2019
Epoetin alfa (Retacrit) Epoetin alfa-epbx May 2018 (Rituxan)
(Riabni) Rituximab-arrx December 2020
(Epogen/Procrit)
(Ogivri) Trastuzumab-dkst* December 2017
Etanercept (Evelzi) Etanercept-szzs August 2016
(Herzuma) Trastuzumab-pkrb December 2018
(Enbrel) (Eticovo) Etanercept-ykro April 2019 Trastuzumab
(Ontruzant) Trastuzumab-dttb January 2019
(Herceptin)
Filgrastim (Zarxio) Filgrastim-sndz* March 2015 (Trazimera) Trastuzumab-qyyp March 2019
(Neupogen) (Nivestym) Filgrastim-aafi* July 2018 (Kanjinti) Trastuzumab-anns* June 2019
*Commercially marketed biosimilar.
Dr. Marc Fishman: This is a list of the 29 FDA approved biosimilars currently available. As
you can see, there's two for bevacizumab or Avastin. There's a number of them for
pegfilgrastim and rituximab and trastuzumab.
©2021 MediCom Worldwide, Inc. 11Biosimilars for Hematologic Malignancies:
Dissecting Real-World Evidence and Barriers to Utilization
G-CSF Biosimilars Currently Approved in the US
Product Description Approval Date
Filgrastim
Tbo-filgrastima (Granix®) Short-acting 2012
Filgrastim-sndz (Zarxio®) Short-acting 2015
Filgrastim-aafi (Nivestym®) Short-acting 2018
Pegfilgrastim
Pegfilgrastim-cbqv (Udenyca®) Long-acting 2018
Pegfilgrastim-jmdb (Fulphila™) Long-acting 2018
Pegfilgrastim-bmez (Ziextenzo®) Long-acting 2019
Pegfilgrastim-apgf (Nyvepria™) Long-acting 2020
aTbo-filgrastim is FDA approved as an original biologic in 2012 prior to establishment of FDA biosimilar process; approved for severe neutropenia
prophylaxis for cancer patients receiving chemotherapy with high risk of neutropenia.
This slide shows the currently approved granulocyte colony-stimulating factors. As you can
see, the first one, 2012, we had tbo-filgrastim, which is actually a cost-effective drug, but
it's not a biosimilar. Technically, it functions as a biosimilar in my mind, but it wasn't
approved as a biosimilar because there wasn't an approvable process.
Subsequently, Zarxio (filgrastim-sndz) and Nivestym (filgrastim-aafi), and I use the brand
names even though I don't like to because using the product names is confusing, and we
can see when those were approved. Pegfilgrastim is interesting. We have the four long-
acting pegfilgrastim products, but none of them have the facility that Neulasta
(pegfilgrastim), the original brand drug, has of being able to apply a device to the arm and
have it deliver the medication the next day. For all of these biosimilars, patients will have to
come to the office or have someone administer the biosimilar the day after or at least one
day after the chemotherapy is administered.
Now, Dr. Knopf will speak a little bit more about the approved indications for the originator
and biosimilar G-CSFs.
©2021 MediCom Worldwide, Inc. 12Biosimilars for Hematologic Malignancies:
Dissecting Real-World Evidence and Barriers to Utilization
Approved Indications for Originator and Biosimilar G-CSF
Filgrastim Filgrastim-sndz Filgrastim-aafi
Indications (Neupogen®) (Zarxio®) (Nivestym®)
Decrease incidence of infection (FN) in patients with nonmyeloid ✓ ✓ ✓
malignancies receiving myelosuppressive anticancer drugs
Reduce time to neutrophil recovery and duration of fever in AML ✓ ✓ ✓
Reduce duration of neutropenia while undergoing myeloablative ✓ ✓ ✓
chemotherapy followed by bone marrow transplantation
Mobilize autologous hematopoietic progenitor cells into peripheral blood ✓ ✓ ✓
for leukapheresis
Increase survival in hematopoietic syndrome of acute radiation syndrome ✓ ✓ ✓
Reduce incidence and duration of sequelae of severe neutropenia in ✓ ✓ ✓
neutropenic disorders
Q2 2021 MCA per MCG 0.950 .378 . 450
.
1. Zarxio (filgrastim-sndz). Prescribing Information. https://www.accessdata.fda.gov/drugsatfda_docs/label/2015/125553lbl.pdf. Accessed March 30, 2020.
2. Nivestym (filgrastim-aafi). Prescribing Information. http://labeling.pfizer.com/ShowLabeling.aspx?id=10899. Accessed March 30, 2020.
Dr. Kevin Knopf: Thank you. These are all agents that are used to decrease the drop in
white blood cell count when we give cytotoxic chemotherapy, the short-acting versions,
and then the long-acting versions. These are the short-acting versions. Their approvals are
basically the same as that for the originator G-CSF. As listed on this table here, decreased
incidence of infection in patients with non-myeloid malignancies receiving
myelosuppressive chemotherapy, given to reduce the time to neutrophil recovery in AML
patients, reduced duration of neutropenia while undergoing myeloablative therapy for a
bone marrow transplant, for leukapheresis purposes, for acute radiation syndrome, which
is an uncommon utilization, and to treat neutropenic disorders in patients who have those
rare disorders.
©2021 MediCom Worldwide, Inc. 13Biosimilars for Hematologic Malignancies:
Dissecting Real-World Evidence and Barriers to Utilization
Approved Indications for Pegylated G-CSF Originator and
Biosimilar Pegylated G-CSFs
PEG PEG-apgf PEG-bmez PEG-cbqv PEG-jmdb
Indications (Neulasta®) (Nyvepria™) (Ziextenzo®) (Udenyca®) (Fulphila™)
Decrease incidence of infection‚ as manifested by febrile
neutropenia‚ in patients with nonmyeloid malignancies
receiving myelosuppressive anti-cancer drugs associated ✓ ✓ ✓ ✓ ✓
with significant incidence of severe neutropenia with fever
Increase survival in patients acutely exposed to
myelosuppressive doses of radiation
✓ X* X* X* X*
*All of Neulasta’s biosimilars are approved for the same indications as Neulasta with the exception of increasing survival in patients acutely exposed
to myelosuppressive doses of radiation, which is protected by Orphan Drug Exclusivity until November 2022
1. Fulphila (pegfilgrastim-jmdb). Prescribing Information. https://www.accessdata.fda.gov/drugsatfda_docs/label/2018/761075s000lbl.pdf.
Accessed May 15, 2021.
2. Udenyca (pegfilgrastim-cbqv). Prescribing Information. https://udenyca.com/wp-content/pdfs/udenyca-pi.pdf. Accessed May 15, 2021.
3. Ziextenzo (pegfilgrastim-bmez). Prescribing Information. https://www.accessdata.fda.gov/drugsatfda_docs/label/2019/761045lbl.pdf.
Accessed May 15, 2021.
4. Nyvepria www.drugs.com/pro/nyvepria.html. Accessed May 15, 2021
The similar indications are for the long-acting G-CSF which are more convenient for the
patients than daily G-CSF for five to eight doses, to decrease the incidence of infections and
febrile neutropenia for patients receiving cytotoxic chemotherapy, and to increase in
survival of patients exposed to myelosuppressive doses of radiation, which hopefully does
not happen that often. We'll go back to Dr. Bennett now.
©2021 MediCom Worldwide, Inc. 14Biosimilars for Hematologic Malignancies:
Dissecting Real-World Evidence and Barriers to Utilization
Peg-filgrastim vs Biosimilar Peg-filgrastim
• Meta-analysis: no significant difference between G-CSF reference
biologics and biosimilars in terms of efficacy and safety
Biosimilar Reference
First author, PY Total Mean SD Total Mean SD Mean difference 95% CI Weight
Blackwell, 2016 155 1.36 1.13 153 1.19 0.96 0.17 [-0.07; 0.41] 20.2%
Blackwell, 2015 107 1.17 1.11 107 1.20 1.02 -0.03 [-0.32; 0.26] 14.2%
del Giglio, 2008 140 1.10 1.25 136 1.10 2.25 0.00 [-0.43; 0.43] 6.4%
Harbeck, 2016 155 0.75 0.88 155 0.83 0.90 -0.08 [-0.28; 0.12] 28.1%
Park, 2016 36 2.28 1.14 38 2.08 0.85 0.20 [-0.26; 0.66] 5.6%
Waller, 2010 165 1.60 1.20 85 1.30 1.08 0.30 [0.01; 0.59] 13.4%
Waller, 2016 127 1.20 0.93 67 1.20 1.10 0.00 [-0.31; 0.31] 12.2%
Pooled estimate 885 741 0.06 [-0.05; 0.17] 100.0%
Heterogeneity: I2 = 4%, P = 0.39
-1 -0.5 0 0.5 1
Favors Biosimilar Favors Reference
Mean difference of duration of severe neutropenia (DSN) in days. Numbers refer to the first cycle of chemotherapy.
Botteri E, et al. Eur J Cancer. 2018;89:45-99.
Dr. Charles Bennett: Thank you Kevin. We have started now to do meta-analyses. Meta-
analyses, as you can see in the slide, for G-CSF, PEG-G versus biosimilar PEG-G has shown
really that these drugs on a meta-analytic basis are very similar. By that, I mean when you
look at the middle figure, it has a long line down the middle around zero. The point, the
little square, the black line, touching zero, which says statistically and analytically, that
these products are biosimilar and they're very similar in efficacy between the biosimilar
drug and the reference drug. As you see in the individual clinical trials, people like Kim
Blackwell, early investigators, 2016-2015, did the work, so we have quite a bit of
knowledge. There's a lot of effort to put 7 studies together with a total of 800 patients to
allow us to say that the G-CSF and the PEG-G-CSF are biosimilar and analytically similar in
terms of safety and efficacy between that and the reference drugs. This is work that was
published in the European Journal of Cancer.
©2021 MediCom Worldwide, Inc. 15Biosimilars for Hematologic Malignancies:
Dissecting Real-World Evidence and Barriers to Utilization
Biosimilars: The US Filgrastim Experience
• Biosimilar filgrastim approved in 2016
• Fast uptake - 50% market share by 2017
• Influencing factors:
– Designation of large health insurers of biosimilar filgrastim as the preferred filgrastim
– Acceptance by oncologists of biosimilar filgrastim as having similar safety and efficacy as
reference filgrastim
– Settling of patient litigation between the manufacturers of reference and biosimilar filgrastim
– Lower pricing (after rebates) for biosimilar filgrastim vs reference filgrastim
Bennett CL, et al. Oncologist. 2021 Feb 14 [Epub ahead of print].
The US experience is a little bit clearly less mature because the Europeans started using
biosimilar G in 2007. This is my work that was published, we just got it ahead of print. It's in
The Oncologist and we may be able to find a way to get it to you later. The Oncologist has
done a nice job of keeping up with each of these biosimilars one by one, so I refer that to
you to get to look at if you can. Biosimilar filgrastim was approved in 2016, and by 2017,
one year, 50% market share, unbelievable, very great uptake. The factors that led to this
marked uptake was that large insurers designated the biosimilar filgrastim to be the
preferred drug over by reference filgrastim. Oncologists, in practice, have had no problem
accepting biosimilar filgrastim as having a similar safety and efficacy. There's always been a
big push to educating oncologists. Here it's worked.
We also had an important settling of patent litigation between the manufacturers, in the
reference biosimilar. Of course, in most cases, not all, most cases there's lower pricing after
rebates for biosimilar filgrastim. This is work, as I've mentioned, it's in The Oncologist.
©2021 MediCom Worldwide, Inc. 16Biosimilars for Hematologic Malignancies:
Dissecting Real-World Evidence and Barriers to Utilization
Biosimilars: The US Epoetin Experience
2018: Biosimilar epoetin 2019: UnitedHealthcare 2020: AETNA Medicare Advantage
launched; average wholesale requires all patients receiving and Humana designate biosimilar
price 57% lower than reference epoetin alfa to epoetin over reference epoetin in
comparator switch to biosimilar its preferred formulary list
Use of biosimilar Use of biosimilar Use of biosimilar
epoetin*: 0.4% epoetin*: 45.3% epoetin*: 82.1%
*Numbers not nationally representative. Numbers represent biosimilar epoetin reimbursement by one large insurer.
Bennett CL, et al. Oncologist. 2021 Feb 14 [Epub ahead of print].
The US epoetin experience is a little bit newer. Of course, we try to update ourselves with
that, so I refer to you at the bottom, we have- a similar paper just came out. Epub ahead of
print in The Oncologist on biosimilar EPO. In 2018, the biosimilar EPO was launched, wasn't
much different at that point. 5.7% lower and its use was not very big. Over time, people got
better discounts, UnitedHealthcare, other places became more supportive. The use of
biosimilar EPO went from 0.4% to 45%. Here we have in 2020 besides UnitedHealthcare,
Aetna, Humana picking up biosimilar as preferred. The final look that we have in this slide,
as well as in my manuscript, 82% utilization. It's gone from 0.4% in 2018 to 82% in 2020.
©2021 MediCom Worldwide, Inc. 17Biosimilars for Hematologic Malignancies:
Dissecting Real-World Evidence and Barriers to Utilization
US Biosimilar Pipeline Landscape
As of January 2021
McGowan S, Jesse M. AmerisourceBergen. https://www.amerisourcebergen.com/-/media/assets/amerisourcebergen/biosimilars-page/biosimilar-us-
market-landscape_010421.pdf?la=en&hash=C2727AB6635DA1A8804FB13BB7044214A38C5BF1
The biosimilar pipeline landscape as of three months ago, we have filgrastim, we have
EPOs, we have for pegfilgrastim. Dr. Fishman went over those, Dr. Knopf, and you can see
that this pipeline started to fill up tremendously. Pegfilgrastim that we saw Neulasta, and
then we have the size accepted, approved, and marketed biosimilar pegfilgrastim. You see
five more coming on the market, as soon as they get approved. Five more to get approved.
If they get through trials, and in filgrastim, we have four more. At the end of the day, we
will have nine biosimilar filgrastims if they all get approved and 10 biosimilar filgrastims.
This is going back to spaces we've never even imagined when we started talking about
these products.
©2021 MediCom Worldwide, Inc. 18Biosimilars for Hematologic Malignancies:
Dissecting Real-World Evidence and Barriers to Utilization
Biosimilar US Challenge: Safety
• FDA issued guidance which includes requirements for safety
• Biosimilar studies assess adverse events and ADAs
• FDA has not issued guidance on studies required for interchangeability
– US biosimilars are not designated as interchangeable
• Safety and immunogenicity profiles have been shown to be comparable
across treatment groups
– ADA development lower in some trials with biosimilars
ADAs, anti-drug antibodies
Braun J, et al. Expert Opin Drug Saf. 2017;16(3):289-302.
Safety. I'm like the safety maven around the world in terms of things that I think about in
oncology, but I have to say at the end of the day, I’ve spent a lot of time looking at
biosimilar safety, and I'm really impressed with the safety efforts that have been done. FDA
has made guidance. There are studies that assess adverse events and ADAs. The FDA has
not issued guidance for studies for interchangeability yet, so there's some concern of
interchangeability, of whether it'll be immunogenicity if you'd go from one back and forth
to the other. We've never seen it yet. We have not seen it with any of the other biosimilars,
even in the non-oncology space. There's not a lot of antibodies that are forming and
developing in these biosimilars yet at this point either.
©2021 MediCom Worldwide, Inc. 19Biosimilars for Hematologic Malignancies:
Dissecting Real-World Evidence and Barriers to Utilization
Biosimilar Challenge: Interchangeability
• The FDA requires interchangeability to be shown in clinical trials
– Patients must be switched from the reference drug to the biologic (or vice versa) without substantial loss of
efficacy or safety concerns
• 351(k) required conditions for interchangeability designation:
– Biosimilarity established
– Produces same clinical result in any given patient
– Risk in terms of safety or efficacy of alternating or switching is not greater than risk of using innovator
product without alternation or switch
• Currently there are no FDA-approved biologics in the United States that meet the criteria listed in the
Biologics Price Competition and Innovation Act (BPCIA) for an interchangeable biosimilar
– US pharmacists are unable to substitute biosimilars for reference biologics
– FDA is currently considering revising regulatory requirements for interchangeability
Bennett CL, et al. Lancet Oncol. 2020;21(12):e575-e588.
FDA. Considerations in Demonstrating Interchangeability with a Reference Product: DRAFT Guidance. Web. Accessed September 20, 2017.
Interchangeability. If you ever want to get in a fight at a party, just talk about
interchangeability. This is so difficult. The FDA says they want to be interchangeable to be
shown in clinical trials. Yet there's never been a study that shows interchangeability. There's
no assay that's shown in red. There are no FDA-approved biologics in the United States that
meet the criteria listed in the BPCI, Biologics Price Competition and Innovation Act, for
interchangeable biosimilars. At this point, your pharmacist is unable to substitute a
biosimilar for reference biologics, they are not interchangeable, and the FDA is getting so
many messages that they will have to come up with a much more manageable approach to
the interchangeability.
©2021 MediCom Worldwide, Inc. 20Biosimilars for Hematologic Malignancies:
Dissecting Real-World Evidence and Barriers to Utilization
Biosimilar Challenge: Extrapolation
• Extrapolation: Approval for use of a biosimilar to be used in a clinical setting that has
not been evaluated in pivotal clinical trials if the reference biologic has received
approval for use in that setting
– Not permitted if:
The reference biologic’s mechanism of action in the proposed extrapolated setting differs from its
MOA in the clinical setting that was evaluated for regulatory approval
The dose to be used in the proposed setting differs from the dose used in the setting approved by
the regulator
If the reference biologic is approved as a treatment in a designated orphan drug setting
• In the US, many biosimilars have not been granted extrapolation
• Full extrapolation for each clinical indication approved for the reference biologic is
necessary to better support market competition
Bennett CL, et al. Oncologist. 2021 Feb 14 [Epub ahead of print].
Extrapolation is another term that you won't get as much flak at a party about but you
should know about. I think we heard in the earlier slide presentations, we saw when some
of the look at the FDA-approved indications that Dr. Knopf went through for the filgrastim.
They didn't do a clinical trial in all those settings. What they did do is called it extrapolate.
The FDA has said, just like Europe, that if your products are approved in one setting, then
it's likely to be a similar mechanism in another setting, it can get regulatory approval in that
setting. In the United States, many biosimilars are granted extrapolation. Full extrapolation
for all clinical indications approved by the reference biologic would be helpful because if
they extrapolate and improve 6 out of 10 indications, sometimes people are going to say,
"Which one of the four is extrapolated that's not working out and which one of the six
that's worked out?" We think, and this is the work that we published, again, in The
Oncologist, we strongly think the extrapolation should be complete for each biologic.
©2021 MediCom Worldwide, Inc. 21Biosimilars for Hematologic Malignancies:
Dissecting Real-World Evidence and Barriers to Utilization
Other Barriers and Solutions
Barrier Result Proposed strategy
Regulatory policy
Approval process Prescribers are uncertain if clinical evidence is adequate Rigorous educational programs by manufacturers
Interchangeability and if products are interchangeable or if indications can and policy makers on FDA processes for approving
Extrapolation be extrapolated. biosimilars and how pharmacovigilance programs
are implemented.
Economics
Reimbursement models Complex and dynamic CMS reimbursement rules for Simplify coding and reimbursement processes and
Pricing biosimilars create confusion for billing offices. work with payers on demonstrating the value that
Payers Economic impact on patients and providers is difficult biosimilars bring to market, such as lowering costs
to evaluate. and improving access.
Providers may not be able to adopt biosimilars if payers
prefer innovator products.
Perception
Treatment goals Prescribers may be more willing to accept biosimilars More educational programs that focus on
Patient acceptance when treating for palliative intent rather than acknowledging behavioral economics as a concept
curative intent. that affects prescribing.
Patients may be reluctant to accept what they view as Incentivizing prescribers to use biosimilars using
“generic” products. various payer-based vehicles.
CMS, Centers for Medicare and Medicaid Services; FDA, U.S. Food and Drug Administration
Nabhan C, et al. Oncologist. 2018;23(11):1261-1265.
We have other solutions, we talked about the barriers. The regulatory policy, the approval
process, interchangeability, extrapolation needs to be fixed. We don't need to have
problems and fights at parties about interchangeability and extrapolation. The economics
of these non-transparent rebates make it almost impossible to compare prices. The
perceptions have to be fixed. We need to continue to educate providers to talk about the
similarities in efficacy and safety. One of the guys' papers and this is written by Chadi
Nabhan, one of my collaborators with my SONAR program in 2018 in The Oncologist, and it
gives you a nice overview as well. I'll turn it over to Marc now to provide us information on
the economics of biosimilars.
©2021 MediCom Worldwide, Inc. 22Biosimilars for Hematologic Malignancies:
Dissecting Real-World Evidence and Barriers to Utilization
Biosimilars and Economics
• The typical list price for a biosimilar
marketed in the US is 15% to 35% lower
than the reference product
• Economic effect of biosimilars hinges on:
– Pharmacovigilance and safety
– Endorsement by the medical community
– Patient acceptance
– Price
– Competition
– Insurers
– Reimbursement programs
Merten J. Pharmacy Times [CE Activity]. Released July 15, 2020.; Mulcahy AW, et al. Rand Health Q. 2018;7(4):3.
Dr. Marc Fishman: Thank you, Charlie. This slide shows that the typical price for a
biosimilar in the United States is only about 15%, sometimes up to 35% lower than the
reference product. Not dramatic reductions, but significant. The economic effect of
biosimilars hinges on the pharmacovigilance and safety of the agents, the endorsement by
the medical community. I don't really think that's of particular concern nor patient
acceptance. There haven't been things, stated or written, that patients don't want
biosimilars. We have not found that to be the case. Then there's the price. When you look
at price, that's a pretty broad word. The price to whom? Is it the cost to the health plan,
the cost to the patient? By inference, there's also profitability that's related to price. Then
there's competition amongst the various agents. We haven't really seen that in the
biosimilars as a major factor in which drug a physician might prefer or choose.
Starting with endorsement by the medical community I would like to separate this into
both the treatment of the cancer, whether talking about cure or overall survival and then
the supportive agents. Personally, I look at them very differently. I don't think physicians in
the community look at them very differently though because we do not get demands for
the originator pharmaceutical when there's a request for a treatment drug like, say,
rituximab or bevacizumab, and if a patient fails and progresses on one of the treatment
drugs, we don't have people saying, "Well, that patient failed on the biosimilar
bevacizumab. I want to try the originator drug." We don't really see that.
©2021 MediCom Worldwide, Inc. 23Although logically, I would think that might make more sense than requests for the originator
drug in the supportive care environment because, with supportive care, whether it's a white
cell or a red cell growth factor, you can see the results. If you give a white cell growth factor,
the neutrophils will either increase or they won't. We don't see people saying, "It didn't
increase with the biosimilar, I want to use the originator." We just don't see that. Nor do we
see resistance where if a health plan prefers through the CMS Medicare-approved step
therapy programs, if the step therapy program requires stepping through, say, Zarxio before
you get Neupogen, we don't see people saying, "I won't use Zarxio. I don't think it works."
We don't see that. We do see people saying, "It's not on our formulary. We don't have it, so
we can't use it because the patient needs it today and it is not on our formulary.“ There's
been talk about patient acceptance. We've never heard about a patient saying, "I want the
brand drug." It's theoretically possible, but I think that patients now, specifically referring to
supportive care, the treating physician will say something like, "Your white cell count or your
hemoglobin is low and we're going to give you something to increase it." That's the end of it.
The patient doesn't say, "I don't want a biosimilar." The patient will be interested in the price.
We know that because there's a lot of financial stress placed on cancer patients and they
have co-pays. Patients will generally prefer a lower co-pay.
23Biosimilars for Hematologic Malignancies:
Dissecting Real-World Evidence and Barriers to Utilization
Economics
• Large insurers are beginning to identify biosimilars as preferred therapy over reference biologics1
– In 2019, US health plans covered biosimilars as preferred in 14% of decisions2
UnitedHealthcare – biosimilars for bevacizumab and trastuzumab1
Aetna – short- and long-acting G-CSF1
• Rebates are key to inclusion of biosimilars on formularies2,3:
– Manufacturers negotiate rebate agreements with pharmacy benefit managers to ensure their drug remains
on the formulary or on a preferred formulary tier
– Rebates for some high-cost biologics can reach or exceed 50% of the list price
– “Rebate traps” result when there is a financial incentive to favor a higher-priced, higher-rebated reference
product versus a lower-priced, lower-rebated biosimilar
– Medicare Part D is financially incentivized to keep biosimilars off their formulary due to inability to offer
competitive rebates
– Rebate agreements are not publicly disclosed
1. Whalen J. Am J Manag Care. 2020;26(2 Suppl):S23-S31. 2. Chambers JD, et al. JAMA. 2020;323(19):1972-1973. 3. Carioto J, Mirchandani H. Millman
White Paper. November 2018.
In 2019, US health plans covered biosimilars as preferred in 14% of decisions. That seems
to be going up quite significantly. Then there's a question of rebates, as I alluded to, that
manufacturers provide rebates, we don't know how much, we don't know precisely to
whom, co-pays are based often on the cost of the drug, the list price of the drug, not the
price after rebate. I think a key thing and something that we would think all like to see
change would be more clarity, more transparency on rebates.
I'd like to turn this over to Dr. Knopf again to give us a view of how all of this comes
together from his clinical experience.
©2021 MediCom Worldwide, Inc. 24Biosimilars for Hematologic Malignancies:
Dissecting Real-World Evidence and Barriers to Utilization
Biosimilars and Disparities
• The high cost of biologics translates into access challenges, care disparities, and
inequities in use1
• Biosimilars represent cost-effective alternatives to their reference product, providing
an opportunity to expand patient access to biologic therapy1
– May result in improved clinical outcomes
• To increase uptake:
– Awareness must be increased1,2
70% of Americans have never heard of biosimilars2
– Negative perceptions of patients and/or physicians will need to be addressed1,2
1. Baumgart DC, et al. Front Pharmacol. 2019;10:279.
2. Brill A. https://www.boehringer-ingelheim.us/sites/us/files/files/barrierstobiosimilars_september2018.pdf.
Dr. Kevin Knopf: Thank you. I'm interested in healthcare disparities, and health economics,
and a lot of healthcare disparities has to do with how assets are allocated among different
patient populations. The high cost of biologic therapies, I think, exacerbates some
healthcare disparities and leads to inequities in the use of these agents and probably
affects cancer outcomes worse for certain patient populations in America. The biosimilars
represent a cost-effective alternative to the reference product. They provide the same
quality and efficacy of care at a lower cost. From the greater healthcare system, they're a
win situation in that they may enhance health equity. To increase uptake of these agents,
awareness must be increased by providers and patients. Most Americans have never heard
of biosimilars, although the majority of them are aware of generic drugs. The negative
perceptions of any patients or physicians around biosimilars must also be addressed.
©2021 MediCom Worldwide, Inc. 25Biosimilars for Hematologic Malignancies:
Dissecting Real-World Evidence and Barriers to Utilization
Alameda Health Systems (AHS) Perspective
• AHS is the only public/safety net hospital serving East Bay (California) Alameda County
(including Alameda and Oakland)
• Payer mix is only public insurance or uninsured
• Collaboration with local Medicaid HMO to align financial incentives
• As biosimilars become available, we have quickly moved to 100% adoption in
hematology/oncology and >70% in other fields of medicine
• System requires biosimilar be “on market” for 6 months; once available, biosimilar
submitted to monthly P&T Committee – 100% have been approved as they are available
• Chief of Hematology/Oncology mandates 100% biosimilar use in infusion center unless
there is a strong (and valid) objection
• Neurology, rheumatology, and gastroenterology are not yet at 100% but are increasing to
>70% within 6 months of introduction
My healthcare system is a public hospital. We care for the underserved, those with public
insurance, either Medicare or Medicaid, or uninsured. Actually, California as a whole, more
than half of California's healthcare is delivered to patients who have public insurance,
whether it's a county hospital like ours or a private hospital elsewhere in California. We
collaborated with a local Medicaid HMO, who was also interested in cost-effective care, to
look at our utilization of biosimilar medicines. We had a plan definitively, as soon as a
biosimilar became available, we put it on our formulary and quickly moved to 100%
adoption in the hematology-oncology space. We're a little bit slower in GI and
rheumatology, and neurology, but we're getting closer to 100% in those other fields. These
are all patients who receive treatment at our institutions in the infusion center. Our system
requires that the product be on market for six months go through our pharmaceutics and
therapeutics committee. To date, 100% of medicines that have come on the market have
been approved by our P&T committee as soon as they're available. Then I have mandated
for all our oncologists that everybody use 100% biosimilars unless there's a strong invalid
objection, in which case exceptions can be made. Our other specialties are not yet at 100%,
but they are getting closer and closer and I anticipate that they will be at 100% within the
next 6 to 12 months.
©2021 MediCom Worldwide, Inc. 26Biosimilars for Hematologic Malignancies:
Dissecting Real-World Evidence and Barriers to Utilization
Closing Remarks
• Overall viewpoints: Have oncology biosimilars been the large economic
change agents that the US has hoped for? Short answer: Clearly, billions
of dollars in savings have yet to be realized
• What is the path forward? Strong – particularly with formulary decisions
favoring biosimilar oncology drugs as preferred options
• What are the key barriers? Education, acceptance, FDA regulatory
decisions, patent litigation
Dr. Charlie Bennett: Let's get through some quick questions we want to cover. Overall, we
want to ask the question, have oncology biosimilars been the large economic change agent
that the United States as hoped for? I put it down as a short answer, billions of dollars of
savings have yet to be realized. We heard from Kevin's presentation, 100% utilization in his
hospital. Marc said there's been a pretty large uptake, especially amongst the different
insurers. I practice in the VA, and there has been a big uptake in the VA. Clearly, we've been
looking for $25 billion, $30 billion in savings. We have not seen that savings yet. We're still
looking and this still has room to go. How do we get there? The path forward. I think it's
strong. The fact that the formulary decisions are favoring oncology drugs as preferred
options is really opening the door. One of the key barriers I think we should discuss and
we've talked about is the fact that I think Marc made a point that education has been
pretty proactive. You have had a lot of education on what biosimilars are amongst
oncologists. On the other hand, Kevin made a strong point, that when you ask somebody in
the street, what is a biosimilar, they'll look at you like you have two heads. Acceptance is
also an important issue. I went through the data in my presentation. The fact is the data
strongly support that there's been statistical analytics, studies to show that these
biosimilars are about the same safety and efficacy as the reference drug. The FDA has to
improve its clarity. We have to be able to identify what it means to be interchangeable,
what it means to be extrapolation, and just be complete.
©2021 MediCom Worldwide, Inc. 27I want to thank you. I want to thank Kevin and Marc and the audience for participating and
hopefully participating in our studies. Thank you very much.
27You can also read

















































