Building on our successes: Pushing the CV envelope - B. R. Berridge 15 May 2018 Boston, MA
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
Building on our successes:
Pushing the CV envelope
B. R. Berridge
15 May 2018
Boston, MA
Outline • Motive • Opportunity • Mission • Challenges • Inspiration
There are good reasons for us to be interested in novel ways of working!

A concerning bit of denial Usual table of ’Key Facts’ not included.
Safety liabilities are
important
contributors to
pharma attrition!
Nat Rev Drug Disc 14: 475, 2015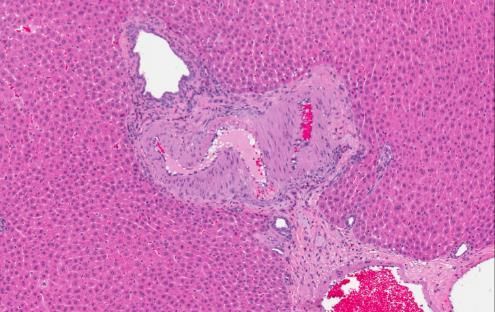
Cardiovascular liabilities are an important contributor to safety-
related attrition- i.e. we have motive!
Attrition of Small Molecules during Pre-Clinical Development
Late Discovery:
➢ Primary toxicity was associated with
the following target organs:
• Liver, kidney, GI, cardiovascular, CNS
➢ Cardiovascular toxicity (18%) was
most prominent reason for
termination
• Includes both
electrophysiology/hemodynamic, and
histological findings
➢ Liver (16%), GI (12%), and CNS (13%) also
major reasons for attrition
IND-enabling phase:
➢ Primary toxicity associated with similar
target organs as in late Discovery
• Liver, kidney, cardiovascular, CNS, testis
➢ Cardiovascular toxicity (27%) continues to
be the most prominent reason for
attrition
➢ Majority of compounds with liver or GI
liabilities are eliminated in late discovery
➢ Testicular toxicity becomes major reason
for attrition (11%)
IQ Consortium Confidential
We have opportunity!
Capabilities
Phenotypic
Bioinformatics assays Activity assays
Animal studies
Binding assays Patient studies
Human tissue -omics
Target ID & Hit/lead Lead Candidate Preclinical Clinical
validation discovery optimisation selection safety assessment
#compounds 1000’s 100’s 10’s 1-3
Design compounds by first intent that engage disease-
modifying targets at appropriate concentrations
without inducing unmanageable liabilities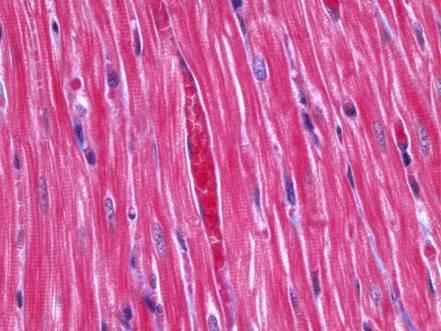
We know what the CV system looks like and how it
works! It’s plumbing, electromechanics and energetics!
Despite a fair bit of evolutionary
conservation, there are important
differences across species!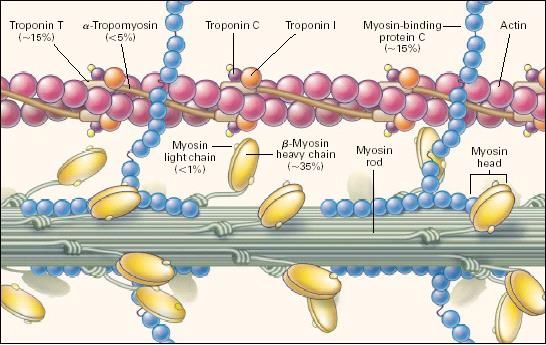
We understand many control systems!
• β-adrenergic agonist
Frank-Starling
•non-selective for β1, β2
Law
•β1 = cardiac inotropy,
chronotropy
Natriuretic •β2 = vasodilation
peptides
•Heart rate (chronotropy) determined by rate of spontaneous SA nodal
discharge
•Spontaneous SA nodal discharge determined by balance of autonomic
control
Sympathetic- norepinephrine discharge
Parasympathetic- acetylcholine discharge Renin-
angiotensin
system
NO,
Endothelin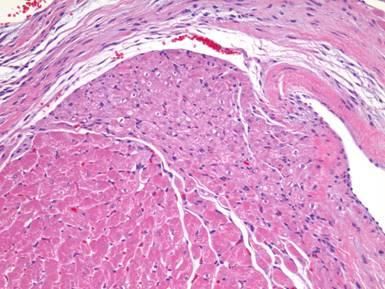
We know what cardiovascular toxicity looks like!
Structural injuries Functional changes
cardiomyocyte injury vascular injury
Arrhythmia
valvulopathy organellar injury ∆ BP ∆ HR
∆ contractility
∆cardiac mass Changes in disease
Ischemic events
Coronary artery dz
Heart failure
Cerebrovascular events
Hypertension
Neoplasia Metabolic diseaseMechanistic, Human-relevant
Cardiovascular Safety Assessment: A HESI
Cardiac Safety Technical Committee
Initiative
2015?
April, 2018Mission Statement Contemporary pharmaceutical cardiovascular safety assessment would benefit from an approach that is more efficient in cost and time, mechanistically informative and human relevant. Such an approach would enable earlier recognition of development-limiting liabilities, fewer false positives leading to premature development termination, more relevant biomarkers and decreased late-stage attrition. The HESI Cardiac Safety Technical Committee will work across its working groups and with other stakeholders to design, test and implement such an approach.
Value Aim Mission Statement proposition Contemporary pharmaceutical cardiovascular safety assessment would benefit from an approach that is more efficient in cost and time, mechanistically informative and human relevant. Such an approach would enable earlier recognition of development-limiting liabilities, fewer false positives leading to premature development termination, more relevant biomarkers and decreased late-stage attrition. The HESI Cardiac Safety Technical Committee will work across its working groups and with other stakeholders to design, test and implement such an approach.
Salient features of the framework
• Knowledge-based
– aligned to what we know about the mechanisms, pathogeneses and
phenotypes of CV toxicity
• Human-relevant
– systems that reflect human biology at the subcellular, cellular or tissue
level
– testing at in vivo concentrations/exposures
• Mechanisms
– goes beyond phenotypic outcomes and probes underlying cellular
mechanisms
• Ability to be applied earlier in development than traditional animal
studies (e.g. at molecular design rather than candidate profiling)Mechanisms CV failure modes- Mechanisms to phenotypes
Drug actions on human receptors, ion channels, cellular processes
βAR, PDE Na+, K+ Ca2+ ATP generation 5HT2B Cytotoxicity Etc.
Potency + Exposure (dose, time)
Valvular
1o Failure
Δ Vasoactivity Δ Inotropy
modes
injury/proliferation
Δ Action Cardiomyocyte/
myocardial Endothelial
potential
injury injury/coagulation
Phenotypes
Nonclinical
Δ BP Hemorrhage,
Δ EF Cardiac fibrosis
thrombosis
Arrhythmia Myocardial Regurgitant flow
necrosis
Phenotypes
Clinical
Δ BP, ΔHR, ↑cTn, Δ EF, HF, Arrhythmia , ↑MACEMechanisms CV failure modes- Mechanisms to phenotypes
Drug actions on human receptors, ion channels, cellular processes
βAR, PDE Na+, K+ Ca2+ ATP generation 5HT2B Cytotoxicity Etc.
Potency + Exposure (dose, time)
Valvular
1o Failure
Δ Vasoactivity Δ Inotropy
modes
injury/proliferation
Aim = shift our testing from
Cardiomyocyte/my
phenotypic to mechanistic,
Δ Action
potential ocardial injury Endothelial
injury/coagulation
observational to predictive
Phenotypes
Nonclinical
Δ BP Hemorrhage,
Δ EF Cardiac fibrosis
thrombosis
Arrhythmia Myocardial Regurgitant flow
necrosis
Phenotypes
Clinical
Δ BP, ΔHR, ↑cTn, Δ EF, HF, Arrhythmia , ↑MACEKey Assumptions
• There are a finite number of primary responses to CV toxicity- i.e. failure modes
(n= 6 in the graphic)
• Behind those failure modes, there are a finite number of key cellular and or
molecular ‘mechanistic’ events (modes of action) that initiate and drive their
pathogenesis which are ‘screenable’
• The likelihood of a xenobiotic inducing a failure mode is a product of it’s potency
for functionally perturbing a cellular event and the likely in vivo exposure in dose
and time
– our confidence in a phenotypic outcome for a mechanistic activity relates to our experience
with it- i.e. some activity at a mechanistic level can be directly related to a phenotypic
outcome (e.g. 5HT2b agonism)
– other activities will require phenotypic confirmatory testing (i.e. Tier 2) in more complex
biological systems to build confidence in the phenotypic outcome
• A relevant mechanistic testing strategy should enable clinical risk assessment,
progression decisions and the development of clinical monitoring strategiesDesigning and executing the framework
Mobilize experts in CV toxicology and safety assessment
Map phenotypic outcomes of CV toxicity (i.e. failure
modes) linked to cellular targets and known mechanistic
pathogeneses
Define a portfolio of potential testing platforms-
e.g. binding assays vs. cellular function assays vs.
3D tissues
Crowd source the development of the needed assays
Validate the assays and qualify the paradigm
Socialize and launchBridge from innovation to application
Progression in confidence
Validate the analytical Qualify the solution's
Develop a decision
Identify and articulate Build a capability to performance and translational
framework that
a gap or problem address the problem reproducibility of that relevance to the
enables application
capability species/context of use
Recognize the
Engage end- Recognize Align to Enable the
ultimate
users and technical performance application of
application of
decision- constraints needs the data
the data
makers
These processes defined by the ultimate ‘context-of-use’The stuff that scares us: Pathogenesis of toxicity can be complex!
28d repeat-dose study in HW rats with a novel compound
Males Males Males
Heart Female
Liver Female Thymus Female
0.500 4.000 0.250
0.450 ** ** 3.500 **
**
Percentage to body weight
Percentage to body weight
Percentage to body weight
0.400
0.350
* ** 3.000 ** * ** ** 0.200
0.300 Dose-progressive
2.500 *
0.150
0.250 2.000 * **
0.200 increase
1.500
in heart weight 0.100 **
0.150
1.000
0.100 0.050
0.050 0.500
0.000 0.000
Treated
0.000
Control 15mg/kg 45mg/kg 100mg/kg Control 15mg/kg 45mg/kg 100mg/kg Control 15mg/kg 45mg/kg 100mg/kg
Males Males
Kidneys Female Brain Female
0.900 1.200
0.800
**
Percentage to body weight
Percentage to body weight
1.000
0.700
0.600 0.800
*
0.500
0.600
0.400
0.300 Grossly visible 0.400
0.200
0.100
enlargement of 0.200
Treated
0.000
Control
the heart
15mg/kg 45mg/kg 100mg/kg
0.000
Control 15mg/kg 45mg/kg 100mg/kg
Control Treated
Treated
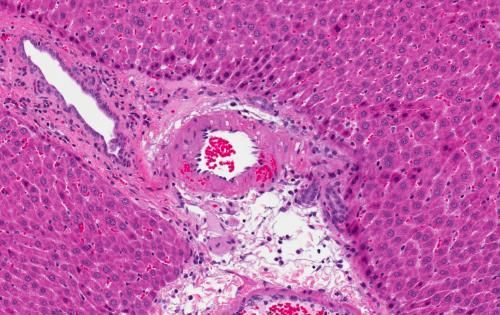
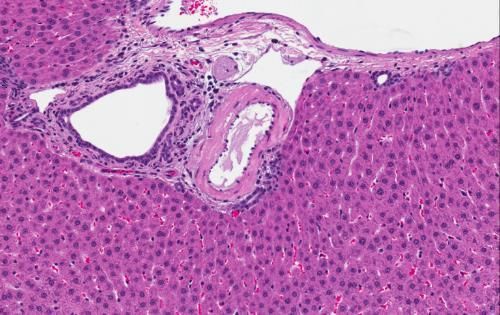
Multifocal arterial injury
Treated Treated
Focal to multifocal myocardial necrosis Is there a pathogenic connection between
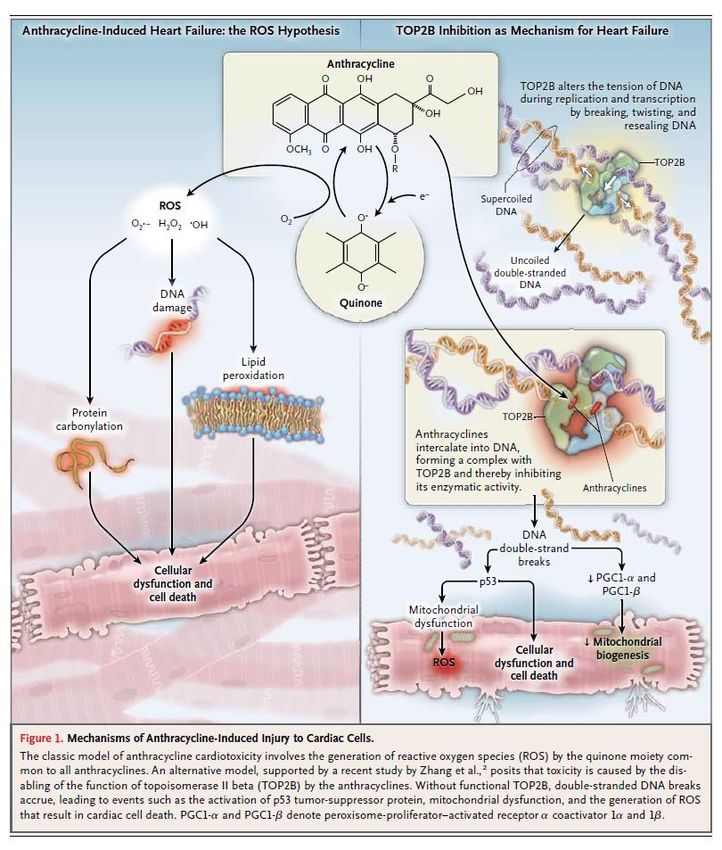
(tendency for subendocardial location?) these changes?The stuff that scares us: How many ‘mechanisms’ do we truly understand? Doxorubicin cardiotoxicity- two (of many?) mechanisms: •Oxidative stress •Top2B inhibition But, that’s okay because we know a lot about ‘modes’!
The stuff that scares us: Pathobiology is a
continuum, it’s adaptive and it’s integrated
Magnitude and Duration
Quantitative Biological Measures
Normal Adaptive Maladaptive Pathology
physiology physiology physiology
•Transition from normal to abnormal is generally not
binomial.
•Thresholds of biological perturbation that represent
‘toxicity’ are difficult to define and not generally well
understood mechanistically.
•Contextualizing those perturbations in a myriad of possible
individual susceptibilities is even more difficult.
•We’re still struggling to extrapolate from simple systems to
complex in vivo outcomes.The stuff that scares us: Pathobiology is a
Military words of inspiration
continuum, it’s adaptive and it’s integrated
Magnitude and Duration
Suck itQuantitative
up, Buttercup.
Biological Measures
We can beat this!
Normal
physiology
Adaptive Maladaptive Pathology
physiology physiology
•Transition from normal to abnormal is generally not
binomial.
•Thresholds of biological perturbation that represent
‘toxicity’ are difficult to define and not generally well
understood mechanistically.
•Contextualizing those perturbations in a myriad of possible
individual susceptibilities is even more difficult.
•We’re still struggling to extrapolate from simple systems to
complex in vivo outcomes.The stuff that scares us: Pathobiology is a
Military words of inspiration
continuum, it’s adaptive and it’s integrated
Magnitude and Duration
Suck itQuantitative
up, Buttercup.
Biological Measures
We can beat this!
Normal
physiology
Adaptive Maladaptive Pathology
physiology physiology
•Transition from normal to abnormal is generally not
binomial.
•Thresholds of biological perturbation that represent
Lead, follow, or get the
‘toxicity’ are difficult to define and not generally well
understood mechanistically.
hell out of the way!
•Contextualizing those perturbations in a myriad of possible
individual susceptibilities is even more difficult.
•We’re still struggling to extrapolate3701 USAFsystems
from simple BMTS
to
complex in vivo outcomes.You can also read

















































