Case Discussion on 'Return-to-Play' for the Athlete Following COVID-19 Infection
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
EXT RA
C A SE REP ORT/ D ISCUSSIO N
Case Discussion on ‘Return-to-Play’ for
the Athlete Following COVID-19 Infection
NATHANIEL MOULSON, MD; MEAGAN WASFY, MD, MPH
K E YWORDS: COVID-19, SARS-CoV-2, myocarditis, of his quarantine, he attempted a short distance run. During
athletes, return-to-play this run, he experienced shortness of breath with minimal
exertion forcing him to cease exercise. He was referred by
his school for outpatient cardiology evaluation prior to being
permitted to return to organized team training.
INTRO D U C T I O N
Myocarditis, or inflammatory disease of the myocardium,
is a well described etiology of sports-related sudden cardiac ‘RETURN-TO-PLAY’ ASSESSMENT POST-COVID-19
death.1 Viral illness is amongst the most common causes Among patients hospitalized with severe COVID-19, a high
for myocarditis.2 Shortly after the emergence of coronavi- prevalence of ‘cardiac injury,’ defined as a cardiac specific
rus disease 2019 (COVID-19) as a global pandemic, reports troponin level exceeding the 99th percentile, was observed
of associated myocarditis led to concern regarding how to early in the pandemic.4 In the critically ill population, this
appropriately evaluate athletes who had COVID-19 prior to cardiac injury may be due to several different mechanisms,
return to their sport. This concern arose given the potential one of which is inflammatory heart disease (myocarditis,
risk of arrhythmia and cardiac arrest, potentiated by exercise, pericarditis) secondary to a systemic inflammatory response
in those who have had recent myocarditis. Resultant expert and/or direct viral invasion.5 The concern that COVID-19
consensus guidelines have addressed the clinical dilemma viral myocarditis may occur in young athletes suffering
of athlete evaluation prior to returning to sport following from non-severe infection resulted in a series of clinical
COVID-19 infection and have evolved over the past year in practice recommendations aimed at identifying those at
order to address new data. Herein we describe an illustrative risk prior to return to sport and exercise.6,7 The first set of
case of a young (35 years of age) lete-specific research data and growing clinical experience.
populations consisting of both competitive and recreational The guidelines recommend that all athletes should avoid
athletes as outlined by the American College of Cardiology’s exercise during the acute infectious period. After quaran-
(ACC) Sports and Exercise Cardiology Section guidelines.3 tine, the recommended approach to post-COVID-19 cardiac
screening is symptom-driven and stepwise. On the basis of
experience suggesting the risk of COVID-19 related inflam-
CA SE P RES EN TAT I O N: PART 1 matory heart disease is very low in this group, athletes with
A 21-year-old Caucasian male college student contracted asymptomatic or mildly symptomatic initial infection do
COVID-19 upon return to campus to resume in person not need to undergo cardiac investigations prior to return to
classes and training. He is a member of his school’s lacrosse sport. In those suffering from moderate or greater severity
team and immediately self-quarantined upon diagnosis. He infection, or those who develop cardiopulmonary symptoms
has no relevant medical history, is on no regular medica- on return to sport, cardiac diagnostic testing is warranted as
tions, and has not previously undergone cardiac screening or detailed further below. Moderate symptoms are defined as
evaluation. His initial symptoms included profound fatigue, persistent fever, chills, myalgias, lethargy, or any cardiopul-
subjective fever, headache, loss of taste and smell, and short- monary symptoms, which include chest pain or tightness,
ness of breath occurring with minimal exertion. He did not dyspnea, syncope, or palpitations. The presence of a ‘multi-
require medical assessment or hospitalization. While many system inflammatory syndrome’ in pediatric populations
of his symptoms resolved over the course of 72 hours, the should also be considered in those with moderate or greater
fatigue and shortness of breath persisted for the remainder of disease severity. This symptom-driven stepwise approach is
his 14-day quarantine period. He felt back to normal by the supported by recent large cohort studies of both collegiate
conclusion of his quarantine, though had not completed any and professional athletes.8, 9
exercise over this span. About 10 days after the conclusion
RIMJ ARCHIVES | AUGUST ISSUE WEBPAGE | RIMS AUGUST 2021 RHODE ISL AND MEDICAL JOURNAL 8C A SE REP ORT/ D ISCUSSIO N
CA SE P RES EN TAT I O N: PART 2 remains for COVID-19 cardiac involvement on the basis of
The patient’s initial symptom burden would most appropri- the clinical history despite normal triad testing. Contem-
ately be classified as ‘moderate.’ Additionally, he experienced porary CMR diagnostic criteria for myocarditis include the
the cardiopulmonary symptom of dyspnea on attempted combination of myocardial edema, as determined by abnor-
return to exercise after initial symptoms had resolved. The mal T2-weighted images or T2 parametric mapping, and a
presence of both a moderate initial symptom burden and non-ischemic myocardial injury, as determined by abnormal
cardiopulmonary symptoms on return to exercise warranted T1 mapping or late gadolinium enhancement (LGE).10
further testing to both rule out cardiac involvement second- Several specific sports leagues11 have utilized screening
ary to COVID-19 and assess for other clinically important algorithms that stipulate all athletes who have had COVID-
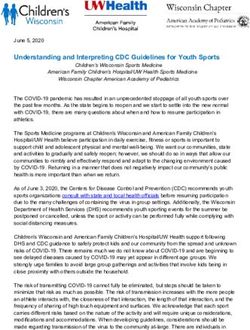
causative etiologies. He underwent initial testing, with 19 should undergo a screening CMR regardless of presenting
a 12-lead electrocardiogram (ECG), high-sensitivity car- symptoms and triad testing results. This practice is driven
diac troponin level, and a transthoracic echocardiogram, by several small observational studies in both non-athletic
as recommended by the expert consensus statement.3 His and athletic populations with COVID-19 that demonstrated
high-sensitivity cardiac troponin-T level was found to be a high prevalence of CMR abnormalities. In non-athletes,
mildly elevated at 18 ng/L (0-14 ng/L) and his 12-lead elec- cardiac abnormalities were seen in up to 78%, while abnor-
trocardiogram demonstrated abnormal T-wave inversions in malities in athletes suggestive of either myocarditis or
the inferolateral leads (Figure 1). Notably, no exercise was pericarditis ranged from 1.4–40%, often without abnor-
performed within 24-hours of his blood draw and no prior mal triad testing results.12-14 These studies were limited by
12-lead ECG existed. His echocardiogram demonstrated the absence of standardized disease definitions and lack of
biventricular size at the upper limit of normal, and mild adequate control group comparators. Many of the athletes
biatrial dilatation. His biventricular function was normal, with CMR abnormalities lacked the other clinical features
and there was no evidence of wall motion abnormalities, of inflammatory heart disease that would usually be paired
pericardial effusion, or valvular disease. with the CMR imaging findings to make the diagnosis,
which makes the significance of these results
Figure 1. 12-lead Electrocardiogram unclear. Subsequent multi-center studies of
Sinus bradycardia with RSR’ pattern in V1 (QRSC A SE REP ORT/ D ISCUSSIO N
Table 1. Normal or Non-specific Cardiac Testing Findings in Athletes* versus Abnormalities Possibly Related to COVID-19 Infection
Cardiac Testing Modality Normal or Non-specific findings in Athletes Abnormalities Possibly Related to COVID-19 infection
Cardiac Troponin 1) Below the 99th percentile for specific 1) Troponin elevation >99th percentile with no other
assay (either conventional or high readily explainable cause
sensitivity)
2) Isolated troponin elevation within 24–48
hr of moderate-to-vigorous exercise and
resolved on repeat testing
12-lead ECG Normal Athlete ECG findings 1) Abnormal TWI
1) Increased QRS voltage for LVH or RVH 2) Pathologic Q waves
[Adapted from the International Criteria for 2) Incomplete RBBB 3) Abnormal ST-depressions
Electrocardiographic Interpretation in Athletes17]
3) Early Repolarization 4) ≥2 PVCs
4) ST elevation followed by TWI V1-V4 in 5) Complete LBBB
black athletes 6) QRS≥140ms
5) TWI V1-V3 < age 16 years old 7) 3rd degree AV block
6) Sinus bradycardia or arrhythmia 8) Atrial tachyarrhythmias
7) 1st degree AV block 9) Ventricular tachyarrhythmias
8) Mobitz Type 1 2nd AV block 10) Complete RBBB combined with axis deviation
or atrial enlargement
Borderline ECG findings^ 11) Diffuse ST elevations or PR depressions
1) Left axis deviation
2) Left atrial enlargement
3) Right axis deviation
4) Right atrial enlargement
5) Complete RBBB
Transthoracic Echocardiogram 1) Mild symmetric increased LV wall 1) LVEFC A SE REP ORT/ D ISCUSSIO N
CA SE P RES EN TAT I O N: PART 3 not involve the myocardium, there is potential for a small
The combination of clinical symptoms, troponin elevation, degree of disease overlap in the form of myopericarditis. As
and abnormal T-wave inversions in the inferolateral leads such, the diagnosis of pericarditis results in similar exercise
elevated the pre-test probability of COVID-19 related myo- restriction recommendations as for myocarditis but for a
carditis, and a CMR was performed. The CMR demonstrated shorter duration.19 In pericarditis, if no evidence of myocar-
normal biventricular size and function with no evidence of dial inflammation is demonstrated and there is complete
wall motion abnormalities or pericardial effusion. There resolution of disease including symptoms, pericardial effu-
was late gadolinium enhancement (LGE) within the sub- sion, and serum markers of inflammation (i.e., CRP, ESR)
epicardial to mid-wall involving multiple left ventricular with appropriate treatment, patients may resume exercise
segments, and increased native T2 in a small focal area of after two weeks. In contrast, the expert consensus recom-
the basal inferolateral septum (Figure 2). These imaging find- mendations for acute myocarditis suggest a period of 3–6
ings were consistent with a small area of myocardial edema months of exercise avoidance to allow for resolution of myo-
(increased native T2) and corresponding injury (LGE) con- cardial inflammation19 with the exact duration to be deter-
sistent with myocarditis.10 His high-sensitivity troponin-T mined by disease severity and trajectory. This timeframe is
was undetectable on repeat testing 10 days later. Given based on expert opinion rather than any prospective data
the clinical presentation and diagnostic testing consistent examining the appropriate duration of sports restriction.
with a diagnosis of myocarditis secondary to COVID-19, Return to sport may occur after this timeframe assuming
the patient was provided with the recommendation to avoid symptoms have resolved, left ventricular systolic function
moderate to vigorous intensity physical activity for at least has remained/returned to the normal range, serum markers
a 3-month period.19 This recommendation is consistent with of myocardial injury and inflammation have normalized
sports participation expert consensus guidelines for athletes (i.e. troponin), and there is no evidence of clinically relevant
with cardiovascular disease that pre-dated COVID-19 as dis- arrhythmia on exercise and ambulatory ECG monitoring.
cussed further below. In the absence of LV dysfunction or This case represents a relatively straightforward clinical
any high-risk arrhythmias on ambulatory ECG monitoring, scenario in that the criteria for a clinical diagnosis of myo-
no medical therapy was indicated. carditis were fulfilled, including the presence of suggestive
symptoms, and cardiac testing was performed based on
Figure 2. Cardiac MRI with Gadolinium Contrast appropriate pre-test probability of disease. The clinical sce-
Subepicardial to mid-wall late gadolinium enhancement involving the nario becomes more challenging when cardiac testing abnor-
inferolateral wall of the left ventricular (Yellow arrow) with associated malities are present but do not formally fulfill diagnostic
small area of increased native T2 (not shown). criteria for inflammatory heart disease, or testing is abnor-
mal but there are no clinical symptoms. Examples of these
scenarios include: 1) isolated troponin elevation and/or ECG
abnormalities with a normal CMR, 2) isolated abnormal
CMR findings (LGE, T1 or T2 mapping) that do not fulfill
CMR criteria for myocarditis, 3) small pericardial effusions
in the absence of symptoms. Expert consultation with a
clinician, such as a sports cardiologist, is recommended in
these situations to balance the need to identify clinically
relevant disease with the importance of avoiding over-
diagnosis and unwarranted restriction from sport.
This case also serves to highlight the uncertainty of cur-
rent return-to-play recommendations regarding duration of
sports restriction for mild presentations of myocarditis (i.e.,
cases in which there is no ventricular dysfunction or arrhyth-
mia and a relatively small area of involvement on CMR). In
athletes for whom restriction has been recommended, but
where return to sport may be more pressing, such as in pro-
M A N A GE M EN T C O NS I D E R AT I ONS fessional or high-level amateur athletics, re-imaging with
Patients with acute cardiac inflammation, either myocar- CMR at the 3-month mark or potentially earlier, may be
dial (myocarditis) or pericardial (pericarditis), should refrain considered pending resource availability. If complete resolu-
from moderate-to-vigorous intensity physical activity until tion of acute inflammation is demonstrated by biomarkers
acute inflammation has resolved.19 This acute inflamma- and imaging, and other appropriate risk stratification mea-
tory period represents one of increased arrhythmic risk par- sures including exercise and ambulatory ECG monitoring
ticularly if placed under the physiologic stress of intensive are normal, an earlier return-to-sport may be considered in
exercise. In pericarditis, although the inflammation does consultation with an experienced clinician.
RIMJ ARCHIVES | AUGUST ISSUE WEBPAGE | RIMS AUGUST 2021 RHODE ISL AND MEDICAL JOURNAL 11C A SE REP ORT/ D ISCUSSIO N
CON C L U S I O N 13. Puntmann VO, Carerj ML, Wieters I, Fahim M, Arendt C, Hoff-
mann J, Shchendrygina A, Escher F, Vasa-Nicotera M, Zeiher
The use of cardiac diagnostic testing to screen for cardiac AM, Vehreschild M, Nagel E. Outcomes of Cardiovascular
involvement in athletes following COVID-19 infection Magnetic Resonance Imaging in Patients Recently Recovered
should be performed by a symptom-guided and stepwise From Coronavirus Disease 2019 (COVID-19). JAMA Cardiol.
2020;5:1265-1273.
strategy. The interpretation of testing abnormalities should
14. Rajpal S, Tong MS, Borchers J, Zareba KM, Obarski TP, Simonet-
be considered within the context of exercise-induced cardiac ti OP, Daniels CJ. Cardiovascular Magnetic Resonance Findings
remodeling and the pre-test probability of disease. Expert in Competitive Athletes Recovering From COVID-19 Infection.
referral should be considered for challenging cases. JAMA Cardiol. 2021 Jan 1;6(1):116-118.
15. Shave R, Baggish A, George K, Wood M, Scharhag J, Whyte G,
Gaze D, Thompson PD. Exercise-induced cardiac troponin el-
evation: evidence, mechanisms, and implications. J Am Coll
Cardiol. 2010;56:169-76.
References
16. Baggish AL, Battle RW, Beaver TA, Border WL, Douglas PS,
1. Eckart RE, Scoville SL, Campbell CL, Shry EA, Stajduhar KC, Kramer CM, Martinez MW, Mercandetti JH, Phelan D, Singh
Potter RN, Pearse LA, Virmani R. Sudden death in young adults: TK, Weiner RB, Williamson E. Recommendations on the Use
a 25-year review of autopsies in military recruits. Ann Intern of Multimodality Cardiovascular Imaging in Young Adult Com-
Med. 2004;141:829-34. petitive Athletes: A Report from the American Society of Echo-
2. Tschope C, Ammirati E, Bozkurt B, Caforio ALP, Cooper LT, cardiography in Collaboration with the Society of Cardiovascu-
Felix SB, Hare JM, Heidecker B, Heymans S, Hubner N, Kelle lar Computed Tomography and the Society for Cardiovascular
S, Klingel K, Maatz H, Parwani AS, Spillmann F, Starling RC, Magnetic Resonance. J Am Soc Echocardiogr. 2020;33:523-549.
Tsutsui H, Seferovic P, Van Linthout S. Myocarditis and inflam- 17. Drezner JA, Sharma S, Baggish A, Papadakis M, Wilson MG,
matory cardiomyopathy: current evidence and future directions. Prutkin JM, Gerche A, Ackerman MJ, Borjesson M, Salerno
Nat Rev Cardiol. 2021;18:169-193. JC, Asif IM, Owens DS, Chung EH, Emery MS, Froelicher VF,
3. Kim JH, Levine BD, Phelan D, Emery MS, Martinez MW, Chung Heidbuchel H, Adamuz C, Asplund CA, Cohen G, Harmon KG,
EH, Thompson PD, Baggish AL. Coronavirus Disease 2019 and Marek JC, Molossi S, Niebauer J, Pelto HF, Perez MV, Riding
the Athletic Heart: Emerging Perspectives on Pathology, Risks, NR, Saarel T, Schmied CM, Shipon DM, Stein R, Vetter VL,
and Return to Play. JAMA Cardiol. 2021;6(2):219-227. Pelliccia A, Corrado D. International criteria for electrocardio-
4. Clerkin KJ, Fried JA, Raikhelkar J, Sayer G, Griffin JM, Masoumi graphic interpretation in athletes: Consensus statement. Br J
A, Jain SS, Burkhoff D, Kumaraiah D, Rabbani L, et al. COVID-19 Sports Med. 2017;51:704-731.
and Cardiovascular Disease. Circulation. 2020;141:1648-1655. 18. Phelan D, Kim JH, Elliott MD, Wasfy MM, Cremer P, Johri AM,
5. Basso C, Leone O, Rizzo S, De Gaspari M, van der Wal AC, Emery MS, Sengupta PP, Sharma S, Martinez MW, La Gerche
Aubry MC, Bois MC, Lin PT, Maleszewski JJ, Stone JR. Patho- A. Screening of Potential Cardiac Involvement in Competitive
logical features of COVID-19-associated myocardial injury: Athletes Recovering From COVID-19: An Expert Consensus
a multicentre cardiovascular pathology study. Eur Heart J. Statement. JACC Cardiovasc Imaging. 2020;13:2635-2652.
2020;41:3827-3835. 19. Maron BJ, Udelson JE, Bonow RO, Nishimura RA, Ackerman
6. American Medical Society for Sports Medicine and the Ameri- MJ, Estes NAM, 3rd, Cooper LT, Jr., Link MS, Maron MS. Eligi-
can College of Cardiology. Cardiac Considerations for College bility and Disqualification Recommendations for Competitive
Student-Athletes during the COVID-19 Pandemic. 2020. Athletes With Cardiovascular Abnormalities: Task Force 3: Hy-
7. Baggish A, Drezner JA, Kim J, Martinez M, Prutkin JM. Resur- pertrophic Cardiomyopathy, Arrhythmogenic Right Ventricular
gence of sport in the wake of COVID-19: cardiac considerations Cardiomyopathy and Other Cardiomyopathies, and Myocardi-
in competitive athletes. Br J Sports Med. 2020;54:1130-1131. tis: A Scientific Statement From the American Heart Associa-
tion and American College of Cardiology. J Am Coll Cardiol.
8. Martinez MW, Tucker AM, Bloom OJ, Green G, DiFiori JP, Sol-
2015;66:2362-2371.
omon G, Phelan D, Kim JH, Meeuwisse W, Sills AK, Rowe D,
Bogoch, II, Smith PT, Baggish AL, Putukian M, Engel DJ. Preva-
Acknowledgments
lence of Inflammatory Heart Disease Among Professional Ath-
letes With Prior COVID-19 Infection Who Received Systematic Dr. Moulson is supported by the University of British Columbia
Return-to-Play Cardiac Screening. JAMA Cardiol. Published Clinician Investigator Program.
online March 4, 2021.
9. Moulson N, Petek BJ, Drezner JA, Harmon KG, Kliethermes Authors
SA, Patel MR, Baggish AL. SARS-CoV-2 Cardiac Involvement Nathaniel Moulson, MD, Massachusetts General Hospital,
in Young Competitive Athletes. Circulation. 2021 Apr 17. doi: Division of Cardiology, Cardiovascular Performance Program.
10.1161/CIRCULATIONAHA.121.054824. Online ahead of print.
Meagan Wasfy, MD, MPH, Massachusetts General Hospital,
10. Ferreira VM, Schulz-Menger J, Holmvang G, Kramer CM, Car-
Division of Cardiology, Cardiovascular Performance Program.
bone I, Sechtem U, Kindermann I, Gutberlet M, Cooper LT, Liu
P, Friedrich MG. Cardiovascular Magnetic Resonance in Non-
Correspondence
ischemic Myocardial Inflammation: Expert Recommendations.
J Am Coll Cardiol. 2018;72:3158-3176. Meagan Wasfy, MD, MPH
11. Rink LD, Daniels CJ, Boersma D, Borchers J, Busch J, Kovan J, Massachusetts General Hospital
Kratochvil CJ, Rifat S, Rosenthal G, Chung EH. Competitive 55 Fruit St, Yawkey 5E
Sports, the Coronavirus Disease 2019 Pandemic, and Big Ten Boston, MA 02114
Athletics. Circ Cardiovasc Qual Outcomes. 2020;13:e007608. 617-643-7117
12. Brito D, Meester S, Yanamala N, Patel HB, Balcik BJ, Casa- mwasfy@partners.org
clang-Verzosa G, Seetharam K, Riveros D, Beto RJ, Balla S, Mon-
seau AJ, Sengupta PP. High Prevalence of Pericardial Involve-
ment in College Student-Athletes Recovering From COVID-19.
JACC: Cardiovascular Imaging. 2021 Mar;14(3):541-555.
RIMJ ARCHIVES | AUGUST ISSUE WEBPAGE | RIMS AUGUST 2021 RHODE ISL AND MEDICAL JOURNAL 12You can also read