Magenta Therapeutics ASH 2018 - Investor Relations - Magenta Therapeutics
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below

Magenta
Therapeutics
ASH 2018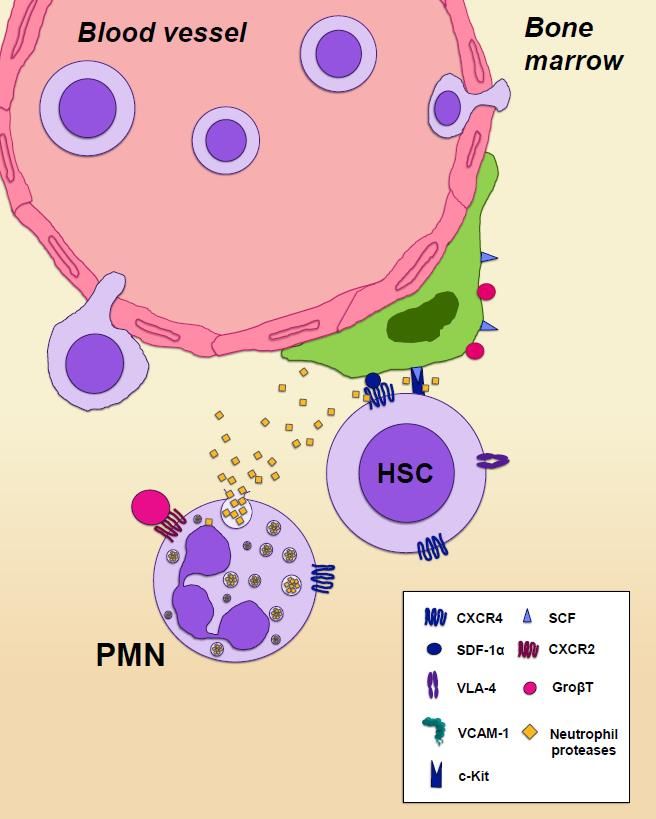
Agenda
Topic Presenter
Welcome and Introduction Manisha Pai, Vice President, Investor Relations and
Communications
Magenta Vision and Overview Jason Gardner, President and Chief Executive Officer
Targeted Conditioning Programs Michael Cooke, Chief Scientific Officer
Stem Cell Mobilization and Stem Cell Expansion Programs John Davis, Chief Medical Officer
Concluding Remarks Jason Gardner
Q&A • Jason Gardner
• Michael Cooke
• John Davis
• David Scadden, Chair of Magenta Scientific Advisory Board
and Co-Founder
2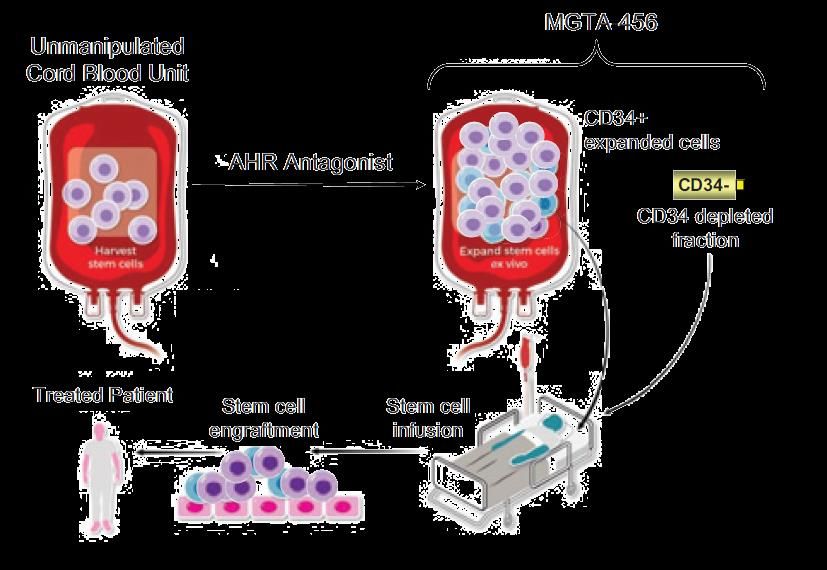
Forward-Looking Statement
This presentation contains forward-looking statements, including express or implied statements regarding
Magenta’s future expectations, plans and prospects, including projections regarding future revenues and
financing performance, our long-term growth, the anticipated timing of our clinical trials and regulatory filings,
the development of our product candidates and advancement of our preclinical programs, as well as other
statements containing the words “anticipate,” “believe,” “continue,” “could,” “estimate,” “expect,” “intend,”
“may,” might,” “plan,” “potential,” “project,” “should,” target,” “will” or “would” and similar expressions that
constitute forward-looking statements under the Private Securities Litigation Reform Act of 1995.
Although Magenta's forward-looking statements reflect the good faith judgment of its management, these
statements are based only on facts and factors currently known by Magenta. As a result, you are cautioned not
to rely on these forward-looking statements. These and other risks concerning Magenta's programs and
operations are described in additional detail in its registration statement on Form S-1, its Quarterly Report on
Form 10-Q and its other filings made with the Securities and Exchange Commission from time to time. Any
forward-looking statement made in this presentation speaks only as of the date on which it is made. Magenta
undertakes no obligation to publicly update or revise any forward-looking statement, whether as a result of new
information, future developments or otherwise.
3
Transplant Success Stories
4
Transformative Drugs to Broaden the Reach of One-Time Curative
Therapies
Uniquely positioned to lead a new era in curative therapies, from bone marrow
transplant to gene therapy and genome editing
◉Multiple modalities
First-in-class
◉Large market opportunity, potential for significant growth
portfolio
◉100% of commercial rights
Clinical-stage ◉ Clinical proof of concept in 41 patients for first product candidate
company ◉Second product candidate entering the clinic in 1H19
◉Three clinical trials to be initiated in late 2018/early 2019:
◉Phase 2 in SCD (MGTA-456)
Multiple catalysts
◉Phase 2 IIT in blood cancers (MGTA-456)
2018–2020
◉Phase 1 in healthy subjects (MGTA-145)
◉Lead ADC for targeted conditioning in IND-enabling studies
Well-positioned ◉$159M in cash as of September 30, 2018
for future growth ◉Seasoned executive team and board of directors
5
Bone Marrow Transplant: The Patient Journey to a Cure
CONDITIONING
Antibody
Drug
Conjugates
Post-Transplant
Complications
Novel
Therapeutics
MOBILIZATION EXPANSION
Biologic Small Molecule
Combo Drugs Ex Vivo
Expansion
6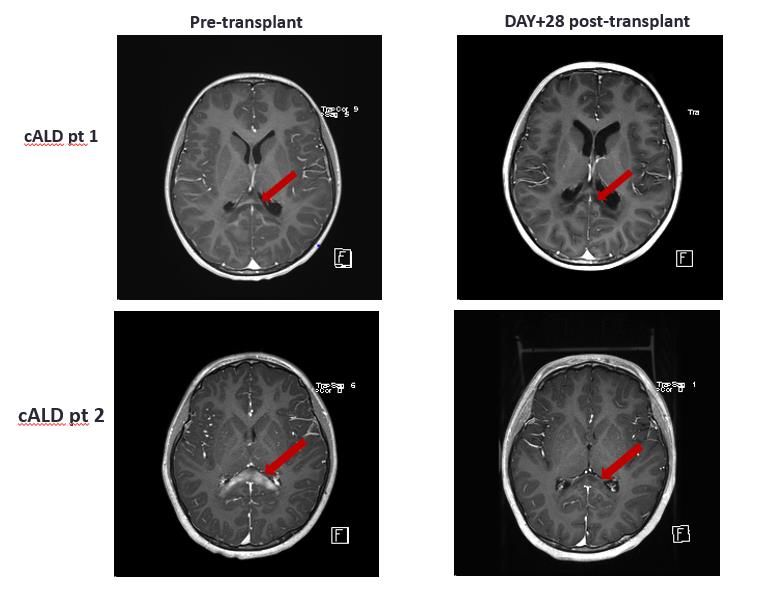
Magenta Portfolio Provides Value Across Transplant Journey
Unmet Needs Magenta Program Magenta Value Proposition
CONDITIONING
Minimize transplant-related
Genotoxic patient Antibody mortality and morbidities
Drug
Patient conditioning with Conjugates
Reduce toxicity
Conditioning significant side effects
Reduce relapse rates
Minimal graft rejection
Low stem cell engraftment EXPANSION
and poor outcomes Small Molecule Faster time to engraftment and
Ex Vivo
Expansion
immune reconstitution
Stem Cell Source
Limited access to well Broadens access to transplant
matched grafts with well matched cord blood
cells
MOBILIZATION Safely mobilize without severe
Non-robust stem cell Biologic side effects
Combo Drugs
Stem Cell mobilization with side- Same-day dosing and
Collection effects apheresis to maximize
operations efficiency
Post-Transplant
Complications
Novel
Post-Transplant High risk of Graft vs. Host Therapeutics
Complications Prevent acute GvHD
disease
7
Magenta Engine Drives Innovative Programs
IND-
Program Preclinical Phase I Phase II
Enabling CONDITIONING
Antibody
C100 Blood cancers, Autoimmune diseases Drug
Conjugates
Targeted
C200 Blood Cancers, Genetic Diseases, HSC Gene Therapy
Stem Cell
Discovery Conditioning
Biology
Biology C300 Blood Cancers, Autoimmune Disease, CAR T
MOBILIZATION
Biologic
Combo Drugs
Mobilization Autologous transplant, Allogeneic donors, Sickle
MGTA-145
Cell Disease
EXPANSION
Blood cancers,
Biotherapeutics Small Molecule
Inherited Metabolic Ex Vivo
MGTA-456
Discovery Diseases, Sickle Cell Expansion
Expansion Disease
E478* Gene therapy/Genome editing
Post-Transplant
Complications
Novel
Post- Therapeutics
Transplant G100 Acute Graft vs Host Disease
Complications
* To be developed in partnership for E478-expanded gene therapies
8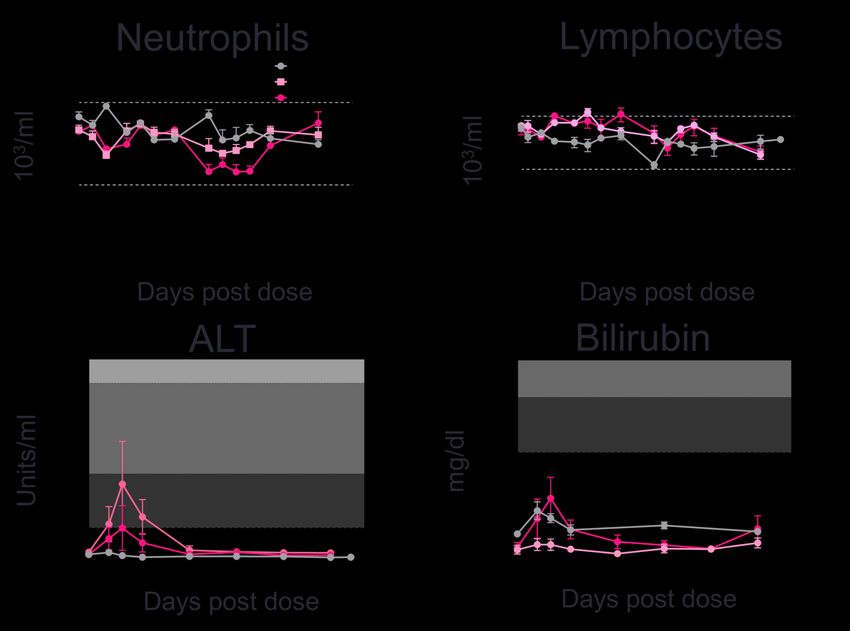
Nine Abstracts Accepted at ASH
IND-
Program Preclinical Phase I Phase II
Enabling CONDITIONING
Antibody
C100 Drug
Conjugates
Targeted
5 abstracts
C200
Stem Cell
Discovery Conditioning
Biology
Biology
MOBILIZATION
Biologic
Combo Drugs
Mobilization MGTA-145 1 abstract
EXPANSION
Biotherapeutics Small Molecule
Discovery
MGTA-456 3 abstracts Ex Vivo
Expansion
Expansion
9
Magenta Targeted
ConditioningMagenta: Transforming the Paradigm of Conditioning
CONDITIONING
Current Agents
Deplete ◉Make space for incoming
◉Discovered 50+ years ago stem cells donor stem cells
◉Toxic chemotherapy
◉Highly toxic, total body irradiation
Deplete ◉Prevent rejection by host
immune cells immune cells
Severe Side Effects
◉Organ toxicity
◉Prevent relapse in blood
◉Cancers Deplete cancers
disease-causing
◉Infertility cells ◉Remove pathogenic immune
cells in autoimmune disease
◉Death
Confidential and Proprietary 11Innovative Targeted Approach to Transplant Patient Conditioning
CONDITIONING
Antibody Drug Conjugate (ADC)
• Receptor-specific ADCs to replace current systemic
chemotherapy agents and radiation
• ADCs are clinically validated and already used to treat
Payload
some cancers
• Magenta will build ADCs designed for transplant
12C100: CD45-ADC for Myelo- and Lymphodepletion
CONDITIONING
C100 Hematopoietic Stem
Cell
HSC Depletion and Immune
Goal
Depletion
Common Myeloid Progenitor Common Lymphoid Progenitor
Lead target CD45
Mast Small Lymphocyte
Payload Amanitin Erythrocyte
Erythrocyte
Cell Myeloblast
Natural killer cell
T cell B cell
Stem and immune cells
Cells removed Megakaryocyte
Disease-causing cells Basophil Eosinophil
Monocyte
Neutrophil
Plasma cell
Autoimmune diseases Platelet
Platelet
Diseases
Blood cancers
Macrophage
13C100: Anti-CD45-ADC Effectively Kills Human Cells In Vitro
CONDITIONING
Human PBMC
Luminescence (AU)
80000
CD45-ADC Isotype
60000
IC50 = 614 pM
40000
20000
0
-1 2 -1 1 -1 0 -9 -8 -7 -6 -5
10 10 10 10 10 10 10 10
Payload depletes non- ADC concentration (M)
Payload
dividing cells for efficient
killing of HSC and Immune
cells Human HSC
CD34+CD90+ number
3 0 0 0
Isotype
2 0 0 0
Engineered for short half-life so
antibody is gone at time of transplant
IC50 = 68 pM
1 0 0 0
0
-1 3 -1 2 -1 1 -1 0 -9 -8 -7
1 0 1 0 1 0 1 0 1 0 1 0 1 0
14
ADC concentration (M)C100: Single Dose Anti-CD45 Amanitin ADC Demonstrates Potent
Killing of Human HSC and Immune Cells in vivo
CONDITIONING
Humanized NSG mice Day 0 Day 7 Day 14 Day 22
CD45-ADC
(single dose, i.v.) PBMC PBMC Assess HSC depletion
in bone marrow
Immune Cells in Blood Stem Cells in Bone Marrow
Data in cynomolgus monkeys to be presented tomorrow evening: Poster #4526
10 15C200: CD117-ADC for Hematopoietic Stem and Progenitor Cell
Depletion
CONDITIONING
C200 Hematopoietic stem and
progenitor cell depletion Hematopoietic Stem
Cell
Goal Selective HSC Depletion
Lead target CD117 Common Myeloid Progenitor Common Lymphoid Progenitor
Payload Amanitin Erythrocyte Mast Small Lymphocyte
Cell Natural killer cell
Myeloblast
Stem cells T cell B cell
Cells removed
Disease-causing cells Megakaryocyte
Basophil Eosinophil
Monocyte
Blood cancers Neutrophil
Plasma cell
Platelet
Diseases Genetic diseases (gene Neutrophil Lymphocyte
therapy) preservation preservation
Macrophage
16C200: Single Dose CD117- Amanitin Depletes HSCs
in Non-Human Primates (NHPs)
CONDITIONING
HSC depletion in Bone Marrow
1 0 0
HSC x 103 / mL
5 0
2 0
1 5
1 0
5
* ** **
0
P B S 0 .1 0 .3 0 .6 1 0 .6 1 0 .6
Anti-CD117-AM IgG1-AM Anti-CD117
• Dose dependent decrease in hematopoietic stem and progenitor cells in bone marrow on day 7
• No depletion observed with the isotype-amanitin conjugate or unconjugated antibody
• Depletion is maintained at 20 days post dosing Poster #3314
17C200: Fast Half-Life CD117- Amanitin ADC Effectively Depletes HSC and
CFU in NHPs
CONDITIONING
HSC number CFU number
A single dose of fast-half life anti-CD117–Amanitin shows greater than 95% depletion of HSC
and CFU in the bone marrow of NHPs 7 days after treatment
Poster #3314
18C200: Fast Half-Life CD117- Amanitin ADC Is Safe and Well-
Tolerated in Non-Human Primates
CONDITIONING
Neutrophils Lymphocytes
• Delayed mild neutropenia (on target)
• No impact on lymphocytes
• Transient dose-dependent reversible
liver enzyme elevation
• No change in liver function (PT,
albumin)
ALT Bilirubin
• No change in food consumption,
weight change or observations
19
Poster #3314Single Doses of CD117-Amanitin and CD45-Amanitin ADCs Show Potent
Anti-Leukemia Activity in Patient-Derived AML Models
CONDITIONING
Target Percent of AML Patients Percent of MDS Patients
CD117 80% 65%
CD45 90-100% 90-100%
Experiment:
• Evaluated 3 AML CD117+ PDX models (n=5 mice/group)
• Treated with 1 mg/kg of indicated ADC when tumor levels reach 2-5 % in peripheral blood
AML #1 AML #2 AML #3
Previously treated with: Allogeneic HSCT, Sorafenib, No previous treatment reported Previously treated with: Allogenic HSCT, Induction
Hydroxyurea, Decitabine FLT3+, NPM1+ chemotherapy, consolidation HiDAC,
FLT3+, NPM1+, DNMT3A+, IDH1+ FLT3 ITD+, TKD+, NPM1+ PBS
100
C D 4 5 - A M ( 1 m g /k g )
100 100 100
Percent survival
C D 1 1 7 - A M (1 m g /k g )
Is o ty p e - A M (1 m g /k g )
43 days 50
50 50 50 > 150 days
106 days 81 days > 150 days
30 days
0
0
0 0
0 75 150 225 0 75 150 225
0 0 7 57 5 1 51 05 0 222255
Days post implantation Days post implantation Days post implantation
20
Poster #3316Next Steps for Targeted Conditioning Programs
CONDITIONING
Indications:
2018 2019 2020 • Relapsed/refractory
AML
• Elderly AML/MDS
C200 Development IND-enabling • Hemoglobinopathies
First clinical study
(CD117) Candidate studies (gene therapy)
2018 2019 2020 Indications:
• Relapsed/refractory
AML
C100 Finalize Development IND-enabling • Elderly AML/MDS
(CD45) antibody Candidate studies • Autoimmune disease
21Magenta Mobilization:
MGTA-145MGTA-145 + Plerixafor Enables Rapid and Robust Mobilization of
HSCs
MOBILIZATION
G-CSF Induced Mobilization Magenta Mobilization
65,000 transplants annually
70% use mobilized peripheral blood
Mobilization
Mobilization
Time to
Time to
Days Minutes
Limitations to current Standard of Care
• Requires 4-6 days
Stem Cells • Unpredictable yields Stem Cells
• Associated adverse events
• Contraindicated for certain diseases
Benefits of novel mobilization regimen
• Mobilize more HSCs
• Shorten time required for mobilization
• Fewer adverse events
Significant opportunity for a predictable and reliable first-
line mobilization agent that enables same-day apheresis
23MGTA-145 and Plerixafor Work Synergistically to Rapidly Mobilize HSCs
MOBILIZATION
Novel regimen:
MGTA-145 (GroβT) + plerixafor (AMD3100)
CXCR2 agonist CXCR4 antagonist
Key features:
• Rapid & robust mobilization of HSCs in mice
plerixafor
• Well-tolerated
• Mimics physiological response
MGTA-
145
November 2017
24A Single Injection of MGTA-145 + Plerixafor Rapidly Mobilizes Large
Numbers of HSCs into Peripheral Blood in Nonhuman Primates
MOBILIZATION
CD34+ CELLS CD34+CD90+CD45RA- CELLS
C D 34+ C D90+ C D 45R A - per m L
1 0 0 ,0 0 0 4 0 ,0 0 0
8 0 ,0 0 0
* 3 0 ,0 0 0
C D34+ per m L
6 0 ,0 0 0
2 0 ,0 0 0
4 0 ,0 0 0
1 0 ,0 0 0
2 0 ,0 0 0
0 0
0 6h 12h 1d 2d 3d 4d 5d 0 6h 12h 1d 2d 3d 4d 5d
T im e P o s t A d m in is t r a t io n T im e P o s t A d m in is t r a t io n
Abstract #116
25A Single Injection of MGTA-145 + Plerixafor Rapidly Mobilizes
Sufficient CD34+ Cells for Transplant in Four Hours
MOBILIZATION
EXPERIMENTAL DESIGN MOBILIZATION & COLLECTION
In collaboration with Dr. Hans-Peter Kiem APHERESIS PRODUCT POST ENRICHMENT Cells Harvested
MOBILIZATION & LEUKAPHERESIS
CD34+ CD34+ Cell Type Dose
0.12% 47%
CD34+ 2.3x106 / kg
MGTA-145 CD34+CD90+CD45RA- 0.9x106 / kg
+ plerixafor
CD34
CD34
CD45 CD45 Cells Infused
CD34+ SELECTION Cell Type Dose
CD34+ 1.8x106 / kg
CD90+CD45RA-
CD90+CD45RA- CD34+CD90+CD45RA- 0.8x106 / kg
CD90
AUTOLOGOUS TRANSPLANTATION
CD90
53% 45%
CD45RA
CD45RA
4 Hour Collection
1080 cGy Abstract #116
26MGTA-145 + Plerixafor Mobilized CD34+ Cells Rapidly Engraft
Following Autologous Transplantation in Nonhuman Primate
MOBILIZATION
AUTOLOGOUS TRANSPLANT
N e u t r o p h il E n g r a f t m e n t P la t e le t E n g r a f t m e n t
20 500
450
N e u tr o p h ils (x 1 0 / L )
10
P la te le ts (x 1 0 /µ L )
400
3
5
350
3
4 300 p la t e le t
n e u t r o p h il 250 re c o v e ry
3 re c o v e ry
200 b lo o d
2 GCSF 150 t r a n s f u s io n
100
1
50
0 0
0 5 10 15 20 25 30 35 40 45 50
0 5 10 15 20 25 30 35 40 45 50
D a y s p o s t t r a n s p la n t D a y s p o s t t r a n s p la n t
Abstract #116
27MGTA-145 + Plerixafor Leads to a 10-fold Increase in Monocytes
MOBILIZATION
REPRESENTATIVE MOBILIZATION OF CD34dim CELLS ENUMERATION OF CD34dim CELLS
Unmobilized MGTA-145 + plerixafor
HSPC HSPC
0.02% 0.09%
CD34dim CD34dim
3.6% 12.4%
3-fold
p < 0 .0 1
8 .0
CD90
CD90
C e l l s p e r m L (x 1 0 )
6
CD34 CD34
6 .0
4 .0
2 .0
0
d im
C D 34 c e lls
28
Abstract #116MGTA-145 + Plerixafor Mobilizes an Immunosuppressive Graft
MOBILIZATION
EXPERIMENTAL DESIGN XENO TRANSPLANTATION
MOBILIZATION
* p < 0 .0 0 0 1
Unmobilized #
100 p < 0 .0 5
MGTA-145 + plerixafor
P e r c e n t s u r v iv a l
plerixafor
G-CSF (QDx5) 75
n=3-5 per regimen
50
ISOLATE PBMCs U n m o b iliz e d (n = 1 3 )
M G T A -1 4 5 + p le rix a fo r (n = 1 6 )
25 p le rix a fo r (n = 1 6 )
XENO TRANSPLANTATION IN NSG MICE
G -C S F (n = 1 6 )
6x106 PBMCs 0
per mouse 0 20 40 60
NSG mice D a y s p o s t t r a n s p la n t
200 cGy
* Compared to Unmobilized
n = 13-16 per regimen # Compared to plerixafor
29
Abstract #116A Single Injection of MGTA-145 + Plerixafor Mobilizes Large
Numbers of Engraftable HSCs and Immunosuppressive Monocytes
MOBILIZATION
Magenta Mobilization BENEFITS OF MGTA-145 + PLERIXAFOR
Rapid and robust
Minutes
mobilization of HSCs
Single injection of Rapid engraftment in large
Stem Cells
MGTA-145 + plerixafor
animal transplant model
Mobilization of CD34dim monocytes
capable of suppressing GvHD
MGTA-145
+ plerixafor
MGTA-145 + plerixafor is moving into the clinic
in the first half of 2019
30Next Steps for MGTA-145
MOBILIZATION
Endpoints:
• Number of CD34+
cells mobilized
2018 2019 2020
• Engraftment
Initiate Phase 1 in Initiate Phase 2 in
Complete IND-enabling
healthy subjects multiple myeloma and
studies
non-Hodgkin lymphoma
(1H19)
Confidential and Proprietary 31Magenta Stem Cell Expansion: MGTA-456
MGTA-456: First-in-class Allogeneic Stem Cell Therapy
EXPANSION
• Increases number of stem
cells in a single cord blood
unit to yield a higher stem
cell dose
• Goal is to allow more
patients to have successful
transplants
36 Patients Treated in Phase I/II Hem/Onc Study
5 Patients Treated in Phase II IMD Study
33Next Steps for MGTA-456
EXPANSION
2018 2019 2020
Endpoints:
Continue enrolling patients with
IMDs • Engraftment
leukodystrophies in Phase 2 study
• Time to immune
recovery
• Days in hospital
• Biomarkers
• Disease-specific
Initiate Phase 2 study endpoints
SCD (1H19)
36 patients Phase 2 (IIT) to begin
Hem/Onc
treated to date
34Unmet Need in Inherited Metabolic Disorders
EXPANSION
Inherited Metabolic Diseases:
MGTA-456 Benefits:
• Rapidly progressive, fatal
diseases ✓ Increased stem cell dose
• Characterized by defective ✓ 100% patient engraftment to date
enzyme function in the brains of
patients
✓ Rapid immune recovery
• Transplant only treatment
option ✓ Preclinical data demonstrate improved
microglial engraftment in brain
35Phase 2 Study of MGTA-456 in Inherited Metabolic Disorders
EXPANSION
• Phase 2, open-label, single arm • Primary endpoint: Successful
engraftment of MGTA-456 as measured
by rate of neutrophil recovery
• Enrolling 12 patients between 2 and 16
years of age with:
• Cerebral adrenoleukodystrophy (cALD) • Key secondary endpoints:
• Globoid cell leukodystrophy (GLD) • Safety
• Metachromatic leukodystrophy (MLD) • Engraftment characteristics: chimerism,
• Hurler’s syndrome (MPS1) neutrophil and platelet recovery
• Disease-specific indicators: Brain MRI
enhancement and Loes score in cALD; enzyme
activity and metabolite levels in Hurler’s
syndrome
• Neurodevelopment and resource utilization
Poster #3467 36Patients Treated Per Protocol on IMD-001
EXPANSION
• As of November 2, 2018 data cutoff, 5 patients treated and evaluable
• Safety consistent with myeloablative conditioning
• Two product-related adverse events: one grade 1 vomiting, one grade 3 nausea
• Two patients < 2 years of age with Hurler’s syndrome (MPS1) developed autoimmune cytopenia, a known and
frequent complication of transplant in younger patients and patients with MPS1
• This was not related to MGTA-456
Days in
HLA Allele TNC dose x106/kg CD34+ dose x106/kg Hospital Post-
Patient Age (y) Disease Match (expanded fraction) (expanded fraction) Transplant
cALD-1 7.1 cALD 8/8 131 58 12
cALD-2 6.7 cALD 7/8 257 110 19
MPS1-1 1.7 MPS1 7/8 164 60 17
MPS1-2 1.3 MPS1 7/8 274 109 22
MPS1-3 0.3 MPS1 7/8 270 111 25
One patient had a protocol deviation at time of conditioning and was a priori deemed non-evaluable for analysis. Reported results are for per protocol patients
37
Poster #3467Five of Five Evaluable Patients Had Rapid Immune System
Recovery, Median of 1 Day of Neutropenia
EXPANSION
Endpoint SOC MGTA-456
Engraftment 68% 100%
Time to Immune Recovery 8 days 1 day
10
1
ANC
0.5
MGTA-456
0.1 mean UCB
0.01
SOC
0 1 2 3 4 5 6 7 8 9 10 11 12 13 14 15
Days Post-transplant
38
Confidential and Proprietary Poster #3467100% Primary engraftment and Early Platelet Recovery with
MGTA-456
EXPANSION
Myeloid
Cells
Patient
Poster #3467 39Rapid Resolution of Brain Inflammation in Patients with cALD
EXPANSION
Loes score = 3 Loes score = 2
cALD Patient 1
Loes score = 2 Loes score = 2
cALD Patient 2
Poster #3467
Contrast enhancement in brain MRI images from cALD patients at screening and at day +28 post-transplant showing resolution.
40
Red arrows indicate areas of inflammation on screening and resolution of contrast-enhancement by day +28.Next Steps for MGTA-456
EXPANSION
2018 2019 2020
Endpoints:
Continue enrolling patients with
IMDs • Engraftment
leukodystrophies in Phase 2 study
• Time to immune
recovery
• Days in hospital
• Biomarkers
• Disease-specific
Initiate Phase 2 study endpoints
SCD (1H19)
36 patients Phase 2 (IIT) to begin
Hem/Onc
treated to date
41Concluding Remarks
Magenta Pipeline Anticipated Progress: Year-End 2019
IND-
Program Preclinical Phase I Phase II
Enabling CONDITIONING
C100 Targeted, non-genotoxic patient Antibody
Drug
Conjugates
preparation for transplant and
Conditioning C200
Stem Cell
Discovery
Biology
gene therapy
Biology
MOBILIZATION
Biologic
First-line standard of care Combo Drugs
Mobilization MGTA-145 for robust mobilization of
stem cells
EXPANSION
Biotherapeutics IMDs Cell therapy with Small Molecule
MGTA-456 Ex Vivo
Discovery
Expansion
SCD high dose of well- Expansion
Hem-Onc IIT matched CD34+
cells
43Magenta Vision: Integrated Company for Total Patient Care and Cures
Third Horizon
• Total patient care
Second Horizon
• Outpatient setting for
• Multiple first-in-class all transplants
products across
First Horizon programs
• First global product
launched
44Transplant Success Stories
45Q&A
You can also read

















































