Revelation microMAX Surgical Technique
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below

TM Revelation® microMAX Surgical Technique
DJO Surgical Table of Contents
9800 Metric Boulevard
Austin, TX Design Rationale 2
(800) 456-8696 Indications 4
www.djosurgical.com
Contraindications 4
Preoperative Planning 5
Surgical Approach 6
Femoral Neck Resection 6
Femoral Preparation 6
Femoral Canal Reaming 7
Broaching 8
Implant Seating 9
Final Head Selection 10
Closure 10
Postoperative Rehabilitation 11
This brochure is presented to demonstrate
a surgical technique. DJO Surgical, as the
manufacturer of this device, does not
practice medicine and cannot recommend
this or any other surgical technique for
use on a specific patient. The choice of
the appropriate surgical technique is the
responsibility of the surgeon performing
the operation.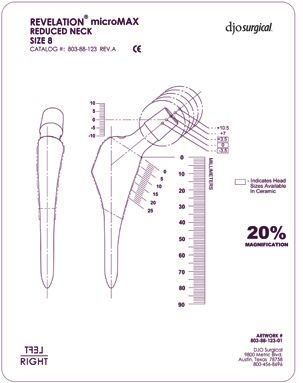
Surgical Technique
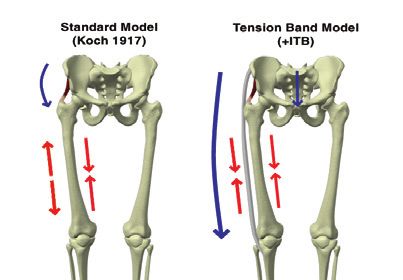
Revelation® microMAX The Ilio-Tibial Model
In the 1980s, Dr. Fetto’s work with above and below the knee amputees
reinforced the discovery of the importance of the ilio-tibial band and its
possible implications on hip replacement design. The ilio-tibial model, as
presented by Dr. Fetto, et al extends Koch’s model by adding the ilio-
Introduction tibial band as a lateral tension band.3,4
The Revelation Hip System represents a fundamental departure from the As a result, the lateral femur is shown to be under compression rather
traditional way in which femoral stems have been designed. Unlike other than tension during the unilateral stance phase of gait. The lateral femur
hip systems created to address a specific clinical issue, the Revelation stems thus becomes a potential base of support for femoral components.
represent the result of a multidisciplinary investigation into the basic science
of joint biomechanics and bone morphology. The system was developed
through an international cooperative effort that included New York Proximal Femur Load Transfer
University, the University of London, the University of Rome, Johns Hopkins
University, and Nagoya University of Japan. By loading the lateral femur, the Revelation stem is designed to
reproduce normal physiologic loading patterns, reduces potential
Revelation Hip Stems are applicable to both primary and revision surgery for subsidence, and avoids diaphyseal overloading, which can cause
with a unique shape designed to physiologically load the proximal femur. The thigh pain. The point of lateral engagement is at, or proximal to, the
Revelation design has been shown to permit immediate full weight bearing intersection of the midneck axis and the lateral cortex. The Revelation
following primary hip replacement, facilitate recovery of function, and shorten femoral component provides secure primary stability which is a
length of hospitalization. More importantly, it has been shown to preserve prerequisite for long-term biological fixation. Compared to a straight
95 percent bone stock and, in the case of prior bone loss, to encourage bone stem, the lateral flare stem has been shown to be significantly less likely
regeneration.1 to migrate.5
Revelation microMAX is a new offering within the Revelation family. It
features the same time-tested Lateral Flare® geometry of the original Stability and Short Stems
Revelation stem to provide multi-plane stability. Because the Revelation
Increased interest in shorter-than-conventional length stems has
proximal geometry inherently limits distal load transfer, Revelation stems
emerged as tissue-sparing approaches and bone conservation concepts
are less reliant on distal length for stability. Thus, the Revelation design’s
have been popularized. Shorter stems relieve some of the challenges
proximally-concentrated stability makes the stem an appropriate candidate
associated with implant placement trajectory in limited-access
for adaptation as a short stem.
approaches. They also reduce intra-operative bone removal which may
make less drastic options available to patients when and if the need
Design Rationale for revision surgery arises. Stability becomes of critical concern when
considering the shortening of a hip stem. Stem designs vary in the
Long-term success of a cementless femoral stem is determined by its ability degree of stability they derive from their distal portions. A stem that
to achieve stable fixation in the bone. The requirements include inherent is more reliant on distal fixation would intuitively be considered a poor
primary stability; physiologic load transfer to avoid stress shielding and candidate for shortening. Conversely, a stem designed for proximal load
resulting bone resorption; and prevention of micromotion between the stem transfer would be regarded as a more appropriate short stem candidate.
and the bone which may lead to loosening of the prosthesis and thigh pain. A Designed specifically for proximal load transfer, the Revelation is seen as
design based on a more complete understanding of hip biomechanics allows the right stem design to address the demand for short stems in today’s
the Revelation and Revelation microMAX stems to meet these requirements market.
by maximizing engagement of the inter-trochanteric cortex.
Conclusion
Hip Biomechanics
By conserving and preserving bone, the Revelation microMAX stem
In 1917, John C. Koch, M.D., of John Hopkins University, defined the traditional holds great promise for long-term success of total hip arthroplasty,
model of hip loading.2 He believed that a downward force applied to the particularly in younger, more active patients.
femoral head during unilateral stance would create a compressive load in the
medial aspect of the femur and tensile loading in most of the lateral cortex.
References
Koch’s work became the standard by which hip biomechanics was analyzed.
Due to limitations of its time, it did not, however, include soft tissues, and 1. Alex Leali and Jospeh F. Fetto. Preservation of Femoral
thus contains several inconsistencies with regard to bone morphology and Bone Mass after Total Hip Replacements with a Lateral
Flare Stem. 2004; 10.1007/s00264-004-0554-1.
energy expenditure. The most obvious question concerns the presence
of cortical bone in both the lateral and the medial femur. According to 2. Koch, J.C. The Laws of Bone Architecture. Am J
Wolff’s law, bone is formed in response to the loading it experiences. The Anatomy.1917; 21:177.
tension in the lateral femur as stated by Koch would theoretically result in 3. Fetto, J.F., Austin, K.S. A Missing Link in the Evolution of
poorly calcified or uncalcified material in that area. This, of course, does not THR: “Discovery” of the Lateral Femur. Orthopedics.
correspond to femoral features observed in clinical practice. 1994; 17:347-350.
2 4. Fetto, J.F., Bettinger P., Austin K. Reexamination of Hip
Surgical Technique 3
Biomechanics During Unilateral Stance. Am J Orthop.
August 1995:605-612. Revelation microMAX
®
5. Culligan, S., Walker P.S., Fetto J.F. The Effect of the
Surgical Technique
Revelation® microMAX Preoperative Planning
Preoperative templates are provided for determining
Standard Neck optimal component size, femoral neck resection
Stem Size Offset level, appropriate neck length and offset (Figure 1).
Radiographs should include a full A/P (anterioposterior)
The Revelation microMAX Hip System features porous coated view of the pelvis including the proximal one-half of both
8.0 37.5mm
titanium short stems designed to reconstruct proximal femurs and an A/P and lateral view of the proximal half
femoral anatomy and proximally load the femur. The 9.0 39.5mm
of the affected femur. As with any surgical procedure,
Revelation microMAX Hip System features state-of-the-art 10.5 42.5mm
proper radiographs are required for accurate templating.
instrumentation that is adaptable to any surgical approach. 12.0 44.5mm Ideally, the A/P radiograph should demonstrate a full
13.5 47.5mm profile of the femoral neck. This is usually best obtained
• Revelation Lateral Flare for lateral cortical loading
15.0 49.5mm by internally rotating the affected limb 15°. Optimally, this
• Flat posterior surface for transfer of flexion/extension should be individualized to each patient’s anatomy. If the
stresses 16.5 51.5mm femur is not rotated or is incorrectly rotated, the neck
• Trapezoidal proximal cross-section for rotational stability 18.0 51.5mm length and offset could be misjudged pre-operatively.
A standard method of templating is used by aligning
• Eight stem sizes available in both left and right the center line of the femoral stem to the center of the
configurations: 8, 9, 10.5, 12, 13.5, 15, 16.5 and 18mm femoral shaft and moving the template up or down to
• Intertrochanteric circumferential porous coating align the flare of the prosthesis silhouette with the flare
Reduced Neck of the bone on the medial/lateral endosteal surface.
• Highly polished in non-porous proximal region
Stem Size Offset Note the diaphyseal fill, the neck resection level, and Figure 1
• Highly polished distal stem to prevent bone on-growth the modular neck length estimation. Careful attention
• 130 degree neck angle 8.0 36.0mm should be made to note the proposed neck resection
9.0 38.5mm level by measuring the distance between the templated
• Choice of 12 degrees (standard neck) or 5 degrees (reduced
neck resection level and the superior aspect of the
neck) anteversion with origin at stem center line 10.5 41.5mm
lesser trochanter. This measurement will be utilized in
• All stems 80mm in length from the medial-proximal coating 12.0 43.0mm conjunction with the osteotomy guide to translate the
boundary to the tip of the stem 13.5 46.5mm pre-operative plan accurately into the operative field.
• Accepts modular CoCr and ceramic femoral heads 158.0 48.5mm Finally, the lateral radiograph should be used for checking
diaphyseal fill with the stem size selected on the A/P.
16.5 50.5mm
18.0 50.5mm
Indications Contraindications
Joint replacement is indicated for patients suffering from Joint replacement is contraindicated where there is:
disability due to: - Infection;
- Noninflammatory degenerative joint disesase including - sepsis;
osteoarthritis and avascular necrosis; - osteomyelitis;
- Rheumatoid arthritis; - rapid joint destruction or bone absorption apparent
- Correction of functional deformity; on roentgenogram;
- Femoral fracture; - skeletally immature patients and cases where there
- Revision procedures where other devices have failed; is a loss of abductor musculature, poor bone stock,
- Treatment of nonunion, femoral neck and trochanteric poor skin coverage around hip joint which would make
fractures of the proximal femur with head involvement, the procedure unjustifiable.
which is unmanageable using other techniques.
Instrumentation
Template
[803-88-123]
4 Surgical Technique 5
Revelation microMAX
®
Surgical Technique
Revelation® microMAX
Femoral Preparation
It is important that the relationship of the femoral
canal with the greater trochanter be appreciated. The
Surgical Approach thin, sharp starter reamer/canal finder may be used to
open the canal (Figure 5). It should encounter minimal
The Revelation microMAX stem’s size enables its use resistance. For enlarging the initial femoral opening, a
with any surgical approach for THR including tissue tapered reamer is included in the set. It can be operated
sparing methods. With limited access approaches, manually with a detachable t-handle or attached to
particular care should be taken in properly locating the power. Lateralizing with the tapered reamer helps
femoral neck resection per the following section. ensure proper positioning (Figure 6).
Femoral Neck Resection
The femoral neck osteotomy should be located by using
the osteotomy guide corresponding to the templated
stem size (Figure 2). The femoral neck resection should
be measured proximally from the lesser trochanter
based on the preoperatively templated measurement Figure 2 Figure 5
(Figure 3). This will allow restoration of the proper
relationship between the tip of the greater trochanter
and the center of the femoral head and avoidance
of post-operative leg length discrepancy. Use of the
osteotomy guide also helps avoid an overly proximal
cut which may interfere with accurate alignment and
seating of the component. The box osteotome further
assists implantation of the device by removing residual
cortical bone in the postero-lateral region of the
piriformis fossa. (Figure 4).
Figure 3
Instrumentation
Figure 6
Osteotomy Guide
[803-04-015/016/017/
018/019/020]
Box Osteotome
[803-04-030] Instrumentation T-handle
[803-05-257]
Reamers
[803-04-022/023/024/025 Starter Awl/Reamer
/026/027] [803-04-021]
Figure 4
6 Surgical Technique 7
Revelation microMAX
®
Surgical Technique
Revelation® microMAX An optional modular slaphammer is available
for broach impaction or extraction. In surgeries
involving removal of fixated devices or compromised
femoral bone, it is strongly advised that prophylactic
wiring prior to broaching be employed in
anticipation of possible intraoperative fracture of
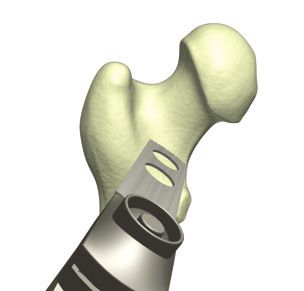
Broaching the femur.
A bone curette is included for preparing the Removal of the broach and examination of the
lateral portion of the intertrochanteric space. It surface of the medullary canal should confirm
is recommended for use prior to broaching but correct seating of the lateral flare broach. The
may also be interspersed with broaching passes calcar planer may be used to level the osteotomy
for avoiding and correcting for varus positioning. to match the broach and corresponding implant
The curette should be focused at the internal level (Figure 11). Correct positioning will demonstrate
corresponding with the trochanteric ridge. broach tooth marks around the perimeter within
the medullary canal. Particular attention should be
Always begin broaching with the smallest available given to observing the presence of these markings
broach size. It is imperative that the femoral broach on the lateral surface of the femur in the region of
be properly aligned with the medullary canal the greater trochanter flare. An alternate method
with special attention to avoiding varus and/or Figure 11
of assessing correct seating of the lateral flare
flexion mal-alignment (Figure 7 and 8). An external broach is by the use of intraoperative radiographs.
alignment guide attaches to holes in the broach A trial reduction can be performed with the broach,
Figure 7 Figure 8
handles and provides visual confirmation of proper corresponding head/neck adapter and modular
broach alignment in the femur. Its tip should be femoral head trial to ensure adequate/optimal joint
pointed toward the medial femoral condyle. (Figure stability (Figure 12).
9). Misalignment of the broach relative to the axis
of the femoral canal is corrected by more valgus
(lateral) and/or extended (posterior) placement of Implant Seating
the broach in the metaphyseal portion of the femur.
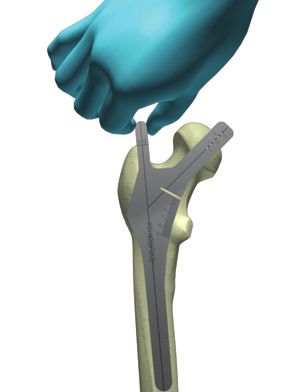
After initial broaching, the proximal lateral aspect After confirming the restoration of alignment,
of the medullary canal should be visually inspected. stability, and uninhibited range of motion, the
To avoid lateral compaction, it may be necessary broach is removed. It is replaced by the final femoral
to further remove the lateral cancellous bone with implant. The femoral component is gently seated
the curette (Figure 10). This will facilitate broaching into its final position with only light impaction.
and proper seating of the final lateral-flare Heavy impaction forces customary with other stem
broach which will remain in place as a provisional designs are not necessary with the Revelation’s
component for trial reduction of the hip. proximal geometry and are discouraged (Figure 13). Figure 12
Figure 9
Instrumentation Instrumentation
Bone Curette Broach Handle Slap Hammer Calcar Planer
[803-00-022] [803-04-028] [803-00-032/033]
Figure 10 Figure 13
Broaches Stem Inserter
[803-04-001/002/003/004/ [803-04-029]
005/006/007/008/009/
8 010/011/012]
Surgical Technique 9
Revelation microMAX
®
Surgical Technique
Revelation® microMAX Postoperative Rehabilitation
Patients, unless constrained by bone defects, are
permitted immediate full weight bearing as tolerated.
Range-of-motion restrictions are only in flexion (0-90
degrees), adduction (0 degrees), and internal rotation (0
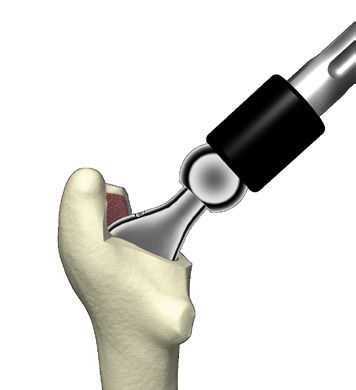
Final Head Selection degrees) during the initial six weeks post-surgery, so as
not to compromise soft-tissue healing. Stationary bicycle
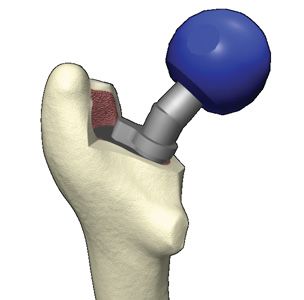
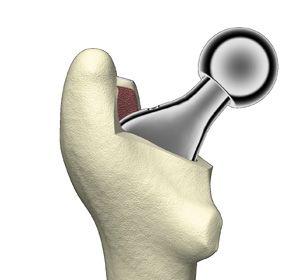
Once the stem has been fully seated, a trial head is
and light progressive resistance exercise are begun when
fitted to the prosthesis (Figure 14). The hip is reduced,
tolerable, usually by three to four weeks post-surgery.
leg length is checked, and range of motion is confirmed
Stimulation of the proximal femur is a specific intention
before final head size and neck length are selected
of the design concept. Therefore, moderate activity
(Figure 15 and 16).
consistent with the material limitations of the prosthesis
component parts is encouraged.
Closure Figure 14
The joint is inspected for any osteophytes or debris
that could have access to the articulating surface. The
hip is reduced and closure initiated while giving careful
attention to an anatomic reconstruction of the capsular
and muscular tissues of the hip, so as to improve joint
stability during postoperative activity.
Figure 15
Head Impactor
[800-01-018/
803-00-041] Figure 16
10 Surgical Technique 11
Revelation microMAX
®
TM
CAUTION: Federal Law (USA)
restricts this device to sale by
DJO Surgical I A DJO Global Company or on the order of a physician.
T 800.456.8696 D 512.832.9500 F 512.834.6300
9800 Metric Blvd. I Austin, TX 78758 I U.S.A. See package insert
djosurgical.com for a complete listing of
indications, contraindications,
warnings, and precautions.
©2011 Encore Medical, L.P. 0020325-001 Rev A 12/11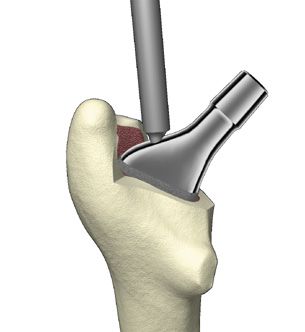
You can also read