Choice t My - People's Experiences of Self-directed Support and Social Care in Glasgow
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below

My o r t
s u p py
m
choice
My Support My Choice:
People’s Experiences
of Self-directed
Support and Social
Care in Glasgow
August 2021
Table of Contents Acknowledgements and Dedication...............................................................................4 About this Report............................................................................................................4 COVID-19.........................................................................................................................4 Executive Summary.......................................................................................................5 Recommendations.........................................................................................................9 National and Local Context for SDS/ Social Care..........................................................13 Research Participants...................................................................................................14 Overall Experiences of SDS and Social Care.................................................................21 Information About SDS.................................................................................................23 Informed Choice and Control.......................................................................................32 Communication and Relationships with Social Work...................................................40 Care Staff Recruitment, Training and Quality...............................................................45 Independent Advocacy and Support............................................................................49 Response from Glasgow City Council.........................................................................52 Endnotes.......................................................................................................................54 Glossary.........................................................................................................................57 About the Project Partners...........................................................................................60 My Support My Choice: Glasgow - August 2021 2

List of Charts Chart 1: Respondents’ gender......................................................................................15 Chart 2: Respondents’ age............................................................................................15 Chart 3: Client group/Disability/Long Term Condition (Survey)..................................16 Chart 4: Survey respondents’ religion..........................................................................17 Chart 5: Survey respondents’ sexual orientation.........................................................17 Chart 6: Survey respondents’ housing arrangements.................................................18 Chart 7: Survey respondents’ annual household income............................................19 Chart 8: “SDS has improved my social care experience” (Survey)...............................21 Chart 9: How did survey respondents first hear about SDS?.......................................23 Chart 10: Information received before discussing support (Survey)...........................26 Chart 11: “I felt prepared for my needs assessment” (Survey)...................................26 Chart 12: Discussing SDS options with professionals (Survey)....................................27 Chart 13: “The person I met explained things clearly to me” (Survey).......................28 Chart 14: “All my questions were answered” (Survey)................................................28 Chart 15: “Have you been told the amount of money you can spend on your support?” (Survey)........................................................................................................29 Chart 16: Enough time to choose SDS option (Survey)................................................32 Chart 17: “Waiting times, or waiting for responses, makes SDS more difficult for me” (Survey).........................................................................................................................33 Chart 18: “I am fully involved in all decisions about my care and support” (Survey).34 Chart 19: “I had a say in how my help, care or support was arranged” (Survey)........35 Chart 20: Who chose support arrangements? (Survey)..............................................36 Chart 21: Did you choose who manages your personal budget? (Survey)..................37 Chart 22: “Enough budget to meet my outcomes makes SDS easier for me” (Survey).........................................................................................................................37 Chart 23: “How happy are you with the conversations you have had about your support with professionals?” (Survey).........................................................................41 Chart 24: “Lack of a regular personal assistant (PA) makes SDS difficult for me” (Survey).........................................................................................................................46 Chart 25: “Access to independent advocacy makes SDS easier for me” (Survey).......49 Chart 26: “Access to independent information and support makes SDS easier for me” (Survey).................................................................................................................50 My Support My Choice: Glasgow - August 2021 3
Acknowledgements COVID-19
and Dedication Data collection ran from 1 November
2018 to 14 February 2020. As
This report is published with thanks such, all responses reflect people’s
to the people who shared their experiences of SDS/ social care
experiences and facilitated the before the appearance of COVID-19
research in Glasgow. It is dedicated in Scotland and people’s experiences
to members of the research during the pandemic are not
team and those who shared covered by the MSMC project.
their experiences as participants
who have since passed away. Nevertheless, this research represents
the most recent and comprehensive
reflection of people’s experiences
About this Report of SDS/ social care in Scotland
prior to COVID-19. As such, MSMC
This report uses data[1] from “My
provides vital evidence, analysis of
Support, My Choice: User Experiences
good practice and recommendations
of Self-directed Support and Social
for improvement in the review
Care in Scotland” (MSMC), a research
and reform of SDS/ social care
project run by the Health and Social
in the aftermath of COVID-19,
Care Alliance Scotland (the ALLIANCE)
based on people’s experiences.
and Self Directed Support Scotland
(SDSS), funded by the Scottish
Government. Focused on people’s
experiences in Glasgow, the report
starts by broadly setting out the
national and local context for Self-
directed Support (SDS) and social care,
followed by information about the
participants.[2] Subsequent chapters
explore people’s experiences of SDS/
social care across Glasgow. Key findings
are highlighted throughout, with a
separate chapter on recommendations.
The report concludes with a response
to the research from Glasgow City
Council and Health and Social Care
Partnership (HSCP). Throughout this
report, “Glasgow” is used to refer
to the Glasgow City local authority
area (which is part of the Greater
Glasgow and Clyde NHS Board).
The document is part of a suite of
MSMC reports that also contains a
national report, other local authority
area reports, and thematic reports,
which are published separately.[3]
My Support My Choice: Glasgow - August 2021 4Executive Summary This report uses data from “My good practice, and increase the Support, My Choice: User Experiences effectiveness and reach of positive of Self-directed Support and Social Care SDS/ social care experiences. The views in Scotland” (MSMC), a mixed-methods expressed by research participants research project run by the Health and analysis of the findings have led and Social Care Alliance Scotland to a number of recommendations, and Self Directed Support Scotland, many of which echo other funded by the Scottish Government. independent reviews of SDS.[4] The aim of this research is to gain a better understanding of people’s Poverty and SDS experiences in Glasgow, filling a data An estimated 24% of Scottish gap and complementing the work of households with a disabled person live other independent evaluations. By in relative poverty after housing costs. highlighting evidence of good practice MSMC found that 86% of research and where improvements can be respondents in Glasgow who provided made, we can assist strategic planning income data lived below the poverty and delivery of future SDS/ social care. threshold. National and local public Between November 2018 and bodies should take action to ensure February 2020, MSMC heard from that reductions in SDS budgets and 52 people in Glasgow who received tightened eligibility criteria do not SDS (or had been assessed in the negatively impact people on low previous 12 months) via a survey incomes who access or are trying to and interviews. Research took place access social care, given that they prior to the appearance COVID-19 can lead to people having to manage in Scotland. Overall, MSMC heard without support, deteriorating from 637 people across Scotland physical and mental health, and via a survey, interviews and focus demands on family and friends to groups. As the largest direct national assume roles as unpaid carers. consultation of its kind to date, the national report provides vital evidence, Data Gathering and Analysis analysis and recommendations for There are concerning gaps in national improvement to SDS/ social care in and regional SDS data gathering the aftermath of the pandemic, based and analysis. Disaggregated data on people’s experiences. This report and intersectional analysis by provides analysis of the results from local and national public bodies Glasgow within that larger context. is essential to develop policy and Research participants in Glasgow practice that prioritises equal acknowledged SDS as important to access to social care for everyone, achieving a higher quality of life and following human rights principles independent living, and reported of equality, non-discrimination, positive experiences across several participation and inclusion. aspects. However, there are key improvements that would respond to people’s concerns, build on existing My Support My Choice: Glasgow - August 2021 5
Overall Experiences of SDS received that information, while
Most participants in Glasgow reported the remainder were unsure.
that SDS had improved their social Recommendations include ensuring
care experience and shared a range of people have good access to high
positive and negative feedback when quality information about SDS/
asked to summarise their experiences. social care, in a range of accessible
and tailored formats at different
Information About SDS points in their journey through the
system. In general, work is needed to
Participants in Glasgow found out ensure everyone is informed about
about SDS from a range of sources. all four SDS options, and supported
Most people highlighted the value to consider the advantages and
of face-to-face communication with disadvantages of each SDS option
independent support organisations before making decisions – rather
and social work, and recommended than being given information about a
that those wanting to know more more limited list of options. Measures
about SDS should get in touch should also be taken to ensure that
with social work, independent people are given full and accessible
advocacy and independent advice information about their budgets and
services as soon as possible. other relevant financial information.
Many participants in Glasgow
indicated they required more high- Informed Choice and Control
quality information at an earlier
stage (before needs assessments) to Overall, most participants in Glasgow
support their decision making about felt they had not had enough
how support would be arranged. Most time to choose their SDS option.
people had not been told about all People reported variable wait times
four options when they started the for assessments and those who
process of accessing SDS. Some had waited the longest also generally
not been provided with accessible reported the highest levels of stress
information or documentation, even and difficulty in accessing SDS.
after requesting it from social work. The majority of respondents in
This pattern of variable information Glasgow indicated that they were on
about the four options continued their preferred SDS option and felt
into people’s needs assessments. involved in decisions and arrangements
A minority of people in Glasgow about their care and support. While
reported that they had “all four this is encouraging, the finding that
options” discussed with them more than a third of people had their
during their assessments. Most SDS option chosen for them by a
people reported that they did not health or social work professional –
have all their questions answered rather than choosing themselves – is
during their needs assessments. more problematic. Professionals play
an important role in supporting access
Just under half of the respondents to appropriate services; however,
in Glasgow indicated that they had this should not extend to making
received information about how decisions on people’s behalf while
much money they could spend on the principles of choice and control
their care and support. However, are clearly embedded in SDS policy.
the same proportion had not
My Support My Choice: Glasgow - August 2021 6Similarly, while it is positive that half Communication and Relationships
of the respondents in Glasgow were with Social Work
offered the choice of who would
manage their personal budget, it is Participants in Glasgow highlighted that
concerning that just over a quarter good, consistent, trusting relationships
reported being offered no choice, with social workers and clear lines of
and a further fifth were unsure; this communication are all essential for
also demonstrates that, amongst positive and effective experiences
other things, they were not fully of SDS. A minority of participants
offered all four SDS options. reported positive and favourable
experiences of assessments and
Most people in Glasgow indicated that reviews with professionals, providing
having sufficient budget to meet their a range of good practice examples.
outcomes made SDS easier for them However, many people outlined
– and highlighted the importance of concerns about their conversations
providing support for social activities with social work professionals,
as well as personal care to ensure a including about not receiving full
good quality of life. People who used answers to questions raised during
SDS budgets to access short breaks assessments and a lack of information
described them as benefiting both about SDS. Some participants shared
individuals and their families – an troubling stories of being treated
important chance for people to relax. with disrespect by professionals.
Budgets and waiting times were Several people raised the need for
prevailing themes when respondents greater transparency about how care
in Glasgow discussed ongoing concerns decisions are made and by whom,
with their needs assessments. alongside inclusive communication
Reductions to budgets and support and easy access to information. Some
has significant negative impacts people reported difficulty obtaining
on people’s mental and physical paperwork and documentation
health. Any proposed reductions in concerning their care arrangements,
SDS budgets or support should be even after repeated requests
communicated clearly and discussed to social work departments.
with people well in advance of any
changes being introduced. Health Recommendations include ensuring
and social care staff should consider that social workers have the time and
the possibility of isolation or mental skills to build relationships and trust
health crisis when changing packages with the people accessing SDS and
and eligibility criteria and be able to unpaid carers that they are working
arrange reassessments and signpost with, building on existing good practice
support services where needed. in Glasgow. People should be informed
promptly if their social worker changes
Recommendations include providing and have a right to request a new
social work professionals with training social worker if trust breaks down.
in supported decision making, and More work is needed to improve the
targeted efforts to ensure that all transparency of process – including
people enjoy equal decision making around how decisions are made
about their SDS option and support. about budgets and accessing SDS.
My Support My Choice: Glasgow - August 2021 7Care Staff Recruitment, Training and Quality People in Glasgow generally reported mixed experiences of support worker recruitment, training and quality. Several participants wrote or spoke eloquently about the positive impact of good care workers. However, many respondents indicated difficulties finding and retaining personal assistants (PAs) and care workers that were suitable for their requirements, and some people would welcome more assistance with staff recruitment and training. Glasgow City Council and HSCP should work with people who access SDS and unpaid carers to improve systems and processes related to care staff recruitment, training and quality. Independent Advocacy and Support Respondents in Glasgow indicated that they value and benefit from the provision of independent advocacy, independent advice and support services, which need sustainable resourcing to continue their important role. Focused efforts are required to ensure all people are aware of – and can access – independent advocacy and support services. Local peer networks should also be encouraged and supported. Glasgow Centre for Inclusive Living (GCIL) and the Glasgow Disability Alliance (GDA) were mentioned several times as helpful in supporting people to navigate and access SDS. My Support My Choice: Glasgow - August 2021 8
Recommendations
People in Glasgow generally reported formats (e.g. hard copy and digital;
that SDS had improved their social face-to-face; large print; Braille; Easy
care experience and have shared Read; BSL). Information is required at
some examples of good practice different points in a person’s journey
from across the region, particularly through the social care system,
about good conversations and
e.g. finding out/ first enquiry about
relationships with social work
professionals, and involvement SDS, pre-needs assessment, during
in care decisions. However, as needs assessment, after needs
this research highlights, there are assessment, once support is in place.
key areas where improvements 4. A wider pool of professionals
could be made to respond to
people’s concerns and increase the (health, education) should be taught
effectiveness and reach of positive SDS about SDS and how to signpost
experiences. The recommendations people to social work, independent
in the MSMC national and thematic support, and appropriate resources.
reports would also usefully 5. More information should be
inform practice in Glasgow.[5]
publicly available for people about
what to expect from interactions with
Poverty and SDS social work, and about their rights.
1. Action is required by national
and local public bodies to ensure
6. People should be provided
with timelines for each stage of
that SDS budget cuts and tightened
the process for accessing SDS, and
eligibility criteria do not negatively
transparency about where and when
affect the physical and mental health
decisions about support are made.
of people on low incomes who access
Transparency would be improved
or are applying for SDS/ social care.
by sharing more publicly available
information in accessible formats.
Data Gathering and Analysis
2. There is a pressing need for local 7. Sufficient time must be
and national public bodies to improve allocated for needs assessments
systematic and robust disaggregated and review meetings, to allow for
data gathering and intersectional detailed questions and consideration
analysis about people who access of the four SDS options.
and apply for SDS/ social care. 8. Further information and
training for professionals may be
Information About SDS required about the SDS options
3. People (service users and and supported decision making.
unpaid carers) need good access 9. Everyone should be informed
to publicly available, high quality about all four SDS options, rather
information about SDS/ social care, than being given information about
in a range of accessible and tailored a more limited list of options, and
My Support My Choice: Glasgow - August 2021 9supported to consider the advantages - and discussed with - people who
and disadvantages of each SDS access SDS/ social care well in advance
option before making decisions. of the changes being introduced.
10. Professionals should proactively
check back in with people after Informed Choice and Control
assessments to ensure any outstanding 17. Systems could be improved
concerns are addressed and resolved, to guarantee short waiting
and their care is working well. times – for a needs assessment,
review, or for support to be put
11. People should be offered a in place – to help people avoid
variety of ways to contact social unnecessary stress and anxiety, and
work, as best fits their access deteriorations in their physical and
needs and preferences. Social work mental health and wellbeing.
departments should consider different
opportunities, including online chat 18. People must be treated
functions, a freephone support line, with dignity and respect in all
and direct email addresses so that interactions with health and
people can communicate effectively social care professionals.
with social work professionals.
19. Any proposed reductions in
12. People should always have SDS budgets/support should be
access to independent advocacy communicated clearly and discussed
and support for assessments and with people well in advance of any
review meetings if they desire. changes being introduced. Health
and social care staff should consider
13. People should be provided the possibility of isolation or mental
with paper or digital (as preferred) health crisis when changing packages
copies of all documentation pertaining and eligibility criteria and be able to
to their SDS, including personal arrange reassessments and signpost
outcome plans, budget agreements, support services where needed.
and decisions about their support
package. These documents should 20. If the support required by
be provided promptly and all an individual is not available then
materials should be available in a any records should reflect that
variety of accessible formats. lack of availability and unmet
need, rather than indicating
14. Everyone must have access to that people refused services.
information about the budget available
to them for their care and support. 21. People need flexible budgets and
a focus on outcomes to enable them
15. People may want to take part to live as independently as possible
in several conversations to support and enjoy the full range of their human
informed decision making about care rights. Flexibility is required in a range
charges, budgets and how they interact of ways: to change SDS option; to
with other income like social security. be able to choose how, where and
16. Any proposed changes when to spend personal budgets;
(particularly increases) in care charges with different amounts of spend and
should be communicated clearly to support at different times of the year.
My Support My Choice: Glasgow - August 2021 1022. Flexible, regular access to short independent oversight of the Scottish
breaks should be strongly encouraged Public Services Ombudsman (SPSO).
because they are an essential element
29. Work is needed to ensure
of SDS that result in good personal
systematic good practice and
outcomes for people who access social
consistent transparency across
care, families and unpaid carers.
several elements of SDS/ social care,
23. Professionals should including eligibility criteria, needs
fully incorporate equality assessments, budgets and support
assessments into their processes packages, changes to support,
for service users and families. participation in decision making
and how to challenge decisions.
Communication and Relationships 30. Professionals should ensure
with Social Work that all unpaid carers are offered
24. Work should continue to carer’s assessments and have
increase positive conversations their rights explained to them.
and meaningful, consistent
31. Professionals should not assume
relationships, with ongoing
that family members and friends are
planning to guarantee high quality
able or suitable to provide unpaid
practice for all people using SDS.
care. People who wish to reduce the
25. Social workers need to amount of unpaid care they provide
have the time and skills to build should be promptly supported by
relationships and trust with the professionals, with appropriate
people accessing SDS and unpaid future planning for contingencies.
carers that they are working with.
32. Health and social work
26. People’s opinions (spoken professionals should respect service
or written) should be recorded users’ preferences if they do not wish
and acknowledged during needs to be reliant on family members and
assessments and review meetings to friends for their care and support.
demonstrate the level of choice and
33. We encourage Glasgow
control exercised over their support.
City Council to indicate document
27. Social work professionals should publication dates and webpage
proactively gather regular feedback timestamps. The Council’s website
– good and bad – from service users, could also provide further information
families and unpaid carers as a way to on their Equality Impact Assessments
support continuous improvement. and the role these play in SDS/ social
care decision making. To strengthen
28. Social work professionals should
participatory decision making,
pro-actively inform service users,
Glasgow City Council could set out
families and unpaid carers on a regular
the steps taken to involve people
basis about how they can challenge
who use support, unpaid carers,
decisions, access independent
and partner organisations in the
advocacy and support, local authority
development of eligibility criteria
complaints procedures and the
and the delivery of support. Further
details of other engagement with
My Support My Choice: Glasgow - August 2021 11people with lived experience would support greater transparency. Care Staff, Recruitment, Training and Quality 34. Some people need more help to recruit and train care staff. Local authorities and health and social care partnerships should work with people who access SDS and unpaid carers to improve systems and processes related to care staff recruitment, training and quality, including diversification of the workforce. 35. Care staff training costs (e.g. specialist first aid or medical training required for them to carry out their job appropriately) should be included in people’s SDS budgets. This would help ensure a quality care workforce (including personal assistants) in each local area. Independent Advocacy and Support 36. Independent advocacy, independent advice and support services need sustainable resources to continue their important role in Glasgow. 37. Local authority and health and social care partnership staff should be given information and training about local independent advocacy, advice and support organisations, so they can refer people to these resources. 38. Social work professionals should proactively provide people with information about independent advocacy, advice and support organisations in accessible formats. 39. Local peer networks should be encouraged and supported. My Support My Choice: Glasgow - August 2021 12
National and Local Context
for SDS/ Social Care
National Context themselves or let the Council do so on
their behalf. Glasgow also published
Self-directed Support (SDS) is information for unpaid carers,
Scotland’s approach to social care. It is including in a range of languages
defined as “the support individuals and (Arabic, Mandarin, Polish, Romanian,
families have after making an informed and Urdu).[11] We welcome the
choice on how their Individual Budget multilingual publication of information
is used to meet the outcomes they for carers – which is unusual in
have agreed.”[6] For more information Scottish local authority websites –
about the national context of SDS/ as an example of good practice.
social care in Scotland, please refer
to the MSMC national report.[7] At time of writing, to obtain more
information on how to access SDS,
Local Context and the eligibility criteria, people
are invited to call the Social Care
Glasgow is the largest city in Scotland, Direct phone number (an 0141
with an approximate population of number). There is no option to
626,000 people across over 290,000 call a freephone number, which
households.[8] It is the centre of the would enable people from low-
“Greater Glasgow” conurbation income households to call without
and is a predominantly urban area, being charged. This consideration
situated to the west of the central is particularly important given the
belt, with Dunbartonshire to the number of people in Glasgow – and
north, Renfrewshire to the west respondents to MSMC specifically
and south, and Lanarkshire to the – who live below the poverty line.
south and east. In 2020, Glasgow
contained the second highest The webpage details the assessment
percentage of areas of deprivation in steps and associated paperwork.
Scotland, after Inverclyde (although According to respondents to MSMC,
it also saw the largest percentile the eligibility criteria used in Glasgow
decrease in deprivation of any local provides support to those people who
authority in Scotland between are at the greatest risk of harm if they
SIMD 2016 and SIMD 2020).[9] are not given support; people assessed
as being at “critical” or “substantial”
Glasgow City Council publishes a risk. Support is not provided via SDS
range of information for people who to people who are assessed as being
access or wish to access SDS on their at a “moderate” or “low” risk levels.
website (searchable via the search bar
on the council website). The relevant A further search on Glasgow City
page is titled “Personalisation” rather Council’s website for “direct payment”
than SDS, with a subtitle “What offers more details on Option 1.[12]
is Personalisation/Self-directed Information includes a description
Support?”.[10] This provides people with of Option 1, how it can be used
a definition of SDS, and states that and managed, who is eligible for
people can manage an SDS budget direct payments, and what records
My Support My Choice: Glasgow - August 2021 13are required from people using We also recommend that Glasgow
Option 1. There is also a link to the City Council indicates document
Glasgow Centre for Inclusive Living publication dates and webpage
(GCIL), under “Related Links”. timestamps. The Council’s website
could also provide further information
We would encourage Glasgow to on their Equality Impact Assessments
publish more information on the four and the role these play in SDS/ social
individual options and outline their care decision making. Finally, to
eligibility criteria online. We would strengthen participatory decision
also recommend that the Council making, Glasgow City Council could
webpages on SDS could usefully set out the steps taken to involve
include direct links to independent people who use support, unpaid
support and advice organisations carers, and partner organisations in
and independent advocacy, as well the development of eligibility criteria
as other resources for people who and the delivery of support. Further
are not deemed eligible for SDS. details of other engagement with
people with lived experience would
support greater transparency.
Research Participants
MSMC heard about the experiences statistics on social care in Scotland.[13]
of 52 people who use or were being While not comprehensive, PHS have
assessed for SDS in Glasgow. We demographic statistics on people
interviewed 11 people who spoke using SDS, and accessing social care
about their own experiences and support services more generally, that is
the experiences of other members provided by local authorities, including
of their household who use SDS Glasgow. PHS include people who use
(spanning the experience of a total of SDS within their wider discussions of
12 people who use SDS or who were people receiving “social care support”,
being assessed for SDS). A further 40 but also include care home residents
people from Glasgow completed the and people who use community
survey. Throughout this report some alarms and telecare services (with or
participant details (e.g. age) have been without SDS) in that wider definition.
changed slightly to preserve anonymity,
while maintaining the most important
information. Where changes have been
made to quotations those alterations
are indicated via square brackets (e.g.
“My advocate, [Name], was great”).
Where possible, we have compared
our participant data to local data and
figures from Public Health Scotland’s
(PHS, formerly Information Services
Division) 2017-2018 experimental
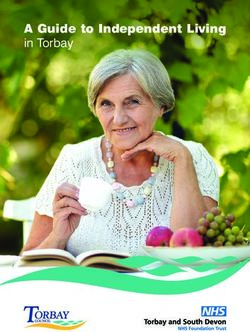
My Support My Choice: Glasgow - August 2021 14Chart 1: Respondents’ gender Chart 2: Respondents’ age
Prefer not 21 21
to say
1
6
Men Women 2
25 26
Under 18-40 41-64 65 or
18 older
PHS figures on the ages of people
Gender receiving social care support in
Overall, 26 women (50% of Glasgow are not available for 2017-
respondents) and 25 men (48% of 2018, as Glasgow City HSCP did
respondents) participated in MSMC in not submit disaggregated data for
Glasgow. One person (2%) preferred that period.[17] In 2016, 62% of the
not to disclose their gender. population of Glasgow was under 45
years old (higher than the Scottish
PHS figures are not available for the average of 53.5%), with the average
division of men and women receiving age expected to increase. The 65 to
social care support services in Glasgow 74 age group is projected to see the
in 2017-2018, as Glasgow City HSCP largest percentage increase between
did not submit disaggregated data 2016 and 2026 (+24.4%).[18] The
across the 19,329 people they overall spread of MSMC respondents
supported during that period (which is slightly younger than 2011 Scottish
also affects analysis of other protected Census data for Glasgow.[19]
characteristics for people accessing
social care services in Glasgow).[14]
Nationally, PHS report that in 2017- Ethnicity
2018 38% of people accessing social 37 MSMC survey respondents in
care support were men and 62% Glasgow identified as white, one survey
were women (of whom, combined, respondent identified as “Asian, Asian
an estimated 45% access SDS).[15] Scottish, or Asian British”, and one as
“Mixed or multiple ethnic groups”.
Age One person chose not to describe
their ethnicity. Most interviewees
We asked all participants to share their did not disclose their ethnicity
age. Of the 50 people who chose to when self-describing themselves,
answer the question, two (4%) were and the majority of those that did
under 18 years old, 21 (42%) were described themselves as “white”.
between 18 and 40 years old, 21 (42%)
were between 41 and 64 years old, and The 2011 Scottish Census indicated
six (12%) were 65 years or older.[16] that 82.7% of the population of
Glasgow identified as “White: Scottish”
(78.6%) or “White: Other British”
My Support My Choice: Glasgow - August 2021 15(4.1%), with a further 5.7% selecting less ethnically diverse than 2011
“White: Irish” (1.9%), “White: Polish” Scottish Census data for Glasgow.[20]
(1.4%), or “White: Other” (2.4%).
The remaining people identified as PHS figures on the ethnicity of
being part of minority ethnic groups: people receiving social care support
8.1% of the population identified as in Glasgow are not available for
“Asian”, “Scottish Asian”, or “British 2017-2018, as Glasgow City HSCP
Asian”, and 3.5% as belonging to did not submit disaggregated
“other ethnic groups”. The overall data for that period.[21]
spread of MSMC respondents is slightly
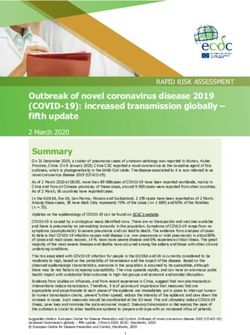
Chart 3: Client group/Disability/Long Term Condition (Survey)
Physical disability 18
Long term condition 16
Mental health 14
Asperger's or autism 13
Learning disability 13
Blind or visual impairment 7
Deaf or hearing impairment 4
Learning and physical disability 3
Prefer not to say 2
Dementia 1
Problems connected with ageing 1
Other 3
accessing SDS were broadly in keeping
Client Group/Disability/ with survey respondents’. Of the 12
Long Term Condition people whose experiences of SDS
MSMC survey respondents in we heard about during interviews,
Glasgow self-identified as living 11 accessed SDS because of their
with a range of conditions, with the own conditions, and one person had
majority reporting that they were found that there were no suitable
living with multiple conditions. Of support services available in their
the 38 people who provided further area, so had ended the process.
details, 18 (47%) selected physical PHS figures on the client groups of
disability, 16 (42%) said they live people receiving social care support
with a long term condition, and 14 in Glasgow are not available for
(37%) selected “mental health.” 2017-2018, as Glasgow City HSCP
Interviewees also discussed their did not submit disaggregated
conditions, and – if they were unpaid data for that period.[22]
carers – those of the people for
whom they care. Their reasons for
My Support My Choice: Glasgow - August 2021 16Religion Most of the interviewees did not
When asked about their religion (if choose to explicitly disclose their
any), 17 survey respondents (43%) religion when self-describing
stated “none”, nine were part of the themselves. The overall spread
Church of Scotland (23%), four were of MSMC respondents is slightly
Roman Catholic (10%), four described less religiously diverse than 2011
themselves as “other Christian” (10%), Scottish Census data for Glasgow.[23]
and one was Muslim (3%). Five people Data about people’s religion is not
(13%) preferred not to answer. available on the PHS dashboard.
Chart 4: Survey respondents’ religion
None 17
Church of Scotland 9
Prefer Not to Say 5
Roman Catholic 4
Other Christian 4
Muslim 1
Sexual Orientation Chart 5: Survey respondents’
25 survey respondents described their sexual orientation
sexual orientation as heterosexual
or straight, two people selected Other, Bisexual,
“other”, and one person was bisexual. 2 1
A further 12 people preferred not
to disclose their sexual orientation.
The 2011 Scottish Census did not
record data on sexual orientation at
local authority level (although the
2022 Scottish Census is expected Heterosexual/
to do so); as such, we do not have Straight, 25
local statistics on sexual orientation
available as a comparison. Data on Prefer not
people’s sexual orientation is not to say, 12
available on the PHS dashboard.
Housing
26 survey respondents (65%)
either rented or owned their own
home, five people (13%) reported
My Support My Choice: Glasgow - August 2021 17that they lived in the home of a When discussing housing, several
family member, two (1%) lived in interviewees spoke about their
supported accommodation, one current situations, spanning a
stated that they live in a “council similar range of options to survey
house”, and one person described respondents. Of those who discussed
their living situation as “homeless their housing arrangements, most
living with a friend”. Five people people lived independently in their
selected “prefer not to say” (13%). own home, followed by those who
lived with a family member.
Chart 6: Survey respondents’ housing arrangements
Owns/Rents Property 26
Prefer not to say 5
Lives in Supported Accomodation 2
Other 7
Household Income
We asked survey respondents
about their household income. We
were interested in this information
because in Scotland an estimated
24% of households with a disabled
person live in relative poverty after
housing costs, compared to 17% of
the population with nobody with
a disability in the household.[24]
None of the interviewees disclosed
their household income when
self-describing themselves,
although many commented on
the negative impact that limited or
reduced SDS/ social care budgets
and social security entitlements
had on their quality of life.
My Support My Choice: Glasgow - August 2021 18Chart 7: Survey respondents’ annual household income
£20,800 - £25,999 10
£15,600 - £20,799 3
£10,400 - £15,599 8
£5,200 - £10,399 7
Up to £5,199 1
Prefer not to say 20
According to Scottish Government
data, the median housing income SDS Option
in Scotland in 2015-2018, before
Of the 34 participants in Glasgow
housing costs, was £499 per week
who shared which SDS option they
(£25,948 per annum).[25] The relative
used, 16 people (47%) indicated
poverty threshold was defined as
they used Option 1, eight people
household income below 60% of
(24%) used Option 2, four people
the median, which for the same
(12%) used Option 3, and three
period was defined as £302 per
people (9%) used Option 4. Three
week (£15,704 per annum).[26] Based
people (9%) stated that they did
on this definition, 16 (86%) of the
not know what option they used.
respondents in Glasgow who chose
to provide details of their household Figures from PHS indicate that in
income are living below the poverty 2017-18 there were 648 people
threshold. Data on the household in Glasgow using SDS Option 1,
incomes of people accessing SDS is 1,1553 using Option 2, 1,597 using
not available on the PHS dashboard. Option 3, and no data was available
on people Option 4.[27] In some
instances, people are logged as being
Poverty and SDS: Reductions on two options simultaneously (e.g.
in SDS budgets and tightened Options 1 and 3) rather than Option
eligibility criteria can pose serious 4, which distorts these figures.
risks to people on low incomes who
access or are trying to access social
care. It can result in people having Data Gathering and Analysis
to manage without support, risks As the chapter on research participants
deterioration in physical and mental demonstrates, there are concerning
health, and places unacceptable gaps in SDS data gathering, analysis
demands on family and friends to and reporting across Scotland. PHS
assume roles as unpaid carers. have reflected on difficulties gathering
disaggregated data on people’s use of
and experiences of SDS/ social care in
their experimental statistics publication
Insights into Social Care in Scotland.[28]
They highlight differences in reporting
My Support My Choice: Glasgow - August 2021 19periods for social care data across local authorities, and that some local authorities and social care partnerships were either not tracking or not able to share disaggregated data about SDS and the people using it in 2017-2018 (including Glasgow).[29] Data gaps are also in part due to existing patterns of data collation – leading, for example, to the PHS Social Care Information Dashboard tracking ethnicity via the limited and problematic categories of “White”, “Other”, and “Not provided/ Not known”.[30] Data Gathering and Analysis: Disaggregated data gathering and intersectional analysis is essential to develop fully realised policies and practices that prioritise equal access to SDS/ social care for everyone, following human rights principles of equality, non-discrimination, participation and inclusion. To avoid gaps and improve analysis, we recommend systematic and robust data gathering by local and national public bodies on people who access SDS, disaggregated by all protected characteristics, including age, gender, sexual orientation, ethnicity, and religion, as well as socio-economic information like household income and the Scottish Index of Multiple Deprivation (SIMD). My Support My Choice: Glasgow - August 2021 20
Overall Experiences of
SDS and Social Care
We asked survey respondents in not only now but in the future
Glasgow whether they felt that and secure it in your funding
SDS had improved their social care from the start. […] It isn’t all
experience. Of the 23 people who plain sailing and sometimes
answered this question, 15 (65%) a struggle, but the best thing
stated that they “strongly agree” or in my life I have ever done.”
“agree” with the statement “SDS
would/has improve/d my social care “Do it. But be determined and stick
experience”. Four people (17%) firm to what you really do need.”
strongly disagreed or disagreed, “I think it’s worth trying.
and four (17%) were unsure. But be prepared for it to
take time and energy.”
Chart 8: “SDS has improved my “If it doesn’t work out there’s no
social care experience” (Survey) shame in that; you come back and
try one of the other options. Things
Unsure change over time as well. I’d say
Strongly give it a go and try and get the
17% agree/ agree balance between having a vision
65% about what you would actually
like, in line with the reality of what
you might actually be able to do.”
“I appreciate the people that help
me, in social work and in Glasgow
Strongly Centre for Inclusive Living.”
disagree/
disagree One interviewee spoke eloquently of
17% the positive impact SDS had had for
their adult child, enabling them to
have more independence and choice:
Survey respondents and interviewees
were asked to share an overall
“[Name] has complete freedom
summary of their experiences and
and my whole plan was for
any advice they might have to offer
[them] to have freedom in every
other people considering using
aspect of [their] life, what with
SDS. Several of the participants’
[Name] being an adult and
statements were positive, such as:
having a right to decide things.”
“Go for it! Make sure that a
Another interviewee reflected
social worker is in place early.”
that SDS provided them with both
“Learn all you can, never think independence and a safety net
you can’t do it. […] Think of all if their health deteriorates:
the aspects of care you will need
My Support My Choice: Glasgow - August 2021 21“I’m independent given that I’ve Some interviewees highlighted that
got help. […] It gives me a level while SDS had previously enabled
of confidence. […] Now, I’ve got them to live a full and independent
no plans for this, but say the day life, cuts to their care had limited
came that I did have a fall or their ability to fully participate in
something, the SDS [care workers] their local communities. One person
would be coming in anyway, and summarised their situation as follows:
of course they’re at the end of
the telephone. So is 999, but it “I’ve got not enough hours to
would be nice to avoid that!” do what you got to do. Because
SDS is supposed to be a tool that
However, some people were more allows you do what you want to
cautious or negative about SDS, do. And if you’ve got not enough
particularly relating to difficulties hours to do that, you can’t do
with paperwork and assessment that. Doing what you want to do
processes, and insufficient budgets: doesn’t just include getting up in
the morning and getting fed.”
“[Have] a good filing system!
It sounds really quite simple,
but I’m aware that I brought
my professional, my working
experience to doing this, and
knowing how to write letters
and file things, and how to
keep everything in order has
helped enormously – and it’s not
something that you get lessons in.”
“Make sure all your needs and
not just hours of support are all
recorded in the care/support plan,
as you may be left to self-fund your
care needs that are not recorded.”
“Be sure that you have all the
relevant information about what
[you] are entitled to and don’t
just accept what you’re offered
without sitting down and getting
a support plan organised, options
offered and explained, and
copies of any minutes relating
to the person requiring care.”
“Don’t get beaten down by the
professionals, and don’t accept
that things can’t be done. They
can, even if the council say ‘no’.”
“It’s not worth the bother.”
My Support My Choice: Glasgow - August 2021 22Information About SDS
Finding Out About SDS (18%) from social media. A further six
people (15%) heard from friends or
We asked participants in Glasgow family members, one from NHS staff,
how they first found out about SDS. one from an independent advocate,
11 (28%) survey respondents first one from a landlord or housing related
heard about SDS from an independent professional, and one from their own
support organisation, eight (20%) professional work. Two people heard
from a social work professional (e.g. a from an unspecified “other” source,
social worker/social work assistant or and one person could not remember.
an occupational therapist), and seven
Chart 9: How did survey respondents first hear about SDS?
Independent support organisation 11
Social work professional 8
Family or friends 6
Other 2
Own professional work 1
Healthcare professional 1
Independent advocate 1
Landlord or housing related… 1
No information / MSMC survey 1
Cannot remember 1
One survey respondent reported that social work. This was followed by
they had never received information people hearing from friends and
about SDS. Some interviewees also family, an advocacy organisation, social
said that they had not had SDS fully media, and a SDS information event
explained to them, even though they run by third sector organisations. The
used SDS, and had done for some time. interviewees who found out about
SDS via their employment worked in
Among the interviewees, social work the social care or education sectors.
and people’s workplaces were the
most common method through which All three interviewees who found out
people first heard about SDS. Three through a social work professional
interviewees heard about SDS for the outlined that this contact was initiated
first time through their professional by them contacting social work
employment, and three heard from
My Support My Choice: Glasgow - August 2021 23to seek support. One interviewee organisation that provided people
described their experience as follows: with useful information about SDS.
Other interviewees suggested that
“I called up social work because they would have welcomed more
I was working to see if there information from health workers, and
was a facility available to help that integrated information sharing
me more getting out and about would have made their experience
[…] so I just contacted them easier. One interviewee stated explicitly
and they had mentioned the that “joint working between social
personalisation package and it work and health services, especially
was them that kind of started GPs, needs to be improved”; another
the ball rolling with that.” stated that “integration of social work
needs to improve so that personal
A second interviewee reflected on information is gathered sensitively
the gap between SDS legislation and without unnecessary repetition.”
and communication with the
wider public, and the need for One person reflected on their
more information sources: experiences of integrated
engagement between their GP
“There was a consultation and and social worker as follows:
a draft bill was created. There
was a debate […] and it passed “Well, it’s definitely not happening
its first reading. It went to from our GP practice anyway. […] I
Committee and there was space mean I have said to her I’m trying
for stage two amendments. They to get more support and she said
heard evidence from disabled ‘well that’s good’. But that’s about
people’s organisations, and it the extent of the conversation
all went through; people who around the support. They certainly
know absolutely nothing about have not pushed anything or
disability thought ‘sounds good asked to link in or asked who
to me’, and they all voted it we were linking in or whatever
through. Except that I had no idea within social work, not at all.”
that it even existed. I’ve been ill
for 33 years and I did not know
that this existed until I got to
the point of phoning the Council
and saying, ‘what services can
I have?’ And they immediately
said, ‘Have you applied for SDS?’
And I was like, ‘What is that?’”
The interviewee who heard about
SDS from their friend commented
that they “always knew from other
friends that lived independently;
my friend always done it, she’d
done it from leaving school, so she
had quite a bit of knowledge.” The
Glasgow Centre for Inclusive Living
(GCIL) was also mentioned as an
My Support My Choice: Glasgow - August 2021 24Option 1: 35% of respondents said that Finding Out About SDS: The they received no information, and 18% research indicates that many received “enough but wanted more”. people in Glasgow had good experiences finding out about SDS Option 2: 47% of respondents from social work professionals and reported that they had “some, but local independent support and not enough” or no information. advice organisations (specifically GCIL). There are some people in Option 3: 56% of respondents Glasgow who require improved said that they had “some, but not access to information about SDS, enough” or no information. and it would be helpful to widen Option 4: 57% of respondents said the pool of professionals who they had received “some, but not are informed about SDS and can enough” or no information. encourage people to access it. Making more use of educational professionals, hospital staff, GPs and other community health practitioners would be valuable in increasing the range of sources of information for people, as well as building on the existing expertise and resourcing of social workers and independent advice and support organisations. Information and Preparedness Before Assessments We asked survey respondents how much information they received on each of the SDS options before meeting with a professional to discuss their support, and whether it was enough information for their requirements. As the chart indicates, across the SDS options, most respondents in Glasgow did not receive “all the information [they] wanted” (respectively, 47% (Option 1), 53% (Option 2), 44% (Option 3) and 43% (Option 4)). It is concerning that among the 17 people who responded to these questions, most people for Options 1, 3 and 4, and a large minority of people across Option 2, either had no information or were left wanting more in advance of their assessment. The detail of those who wanted more information is as follows: My Support My Choice: Glasgow - August 2021 25
Chart 10: Information received before discussing support (Survey)
8 8
7
6 6
5 5
4 4
3 3 3
0 0 0 0
Option 1 Option 2 Option 3 Option 4
All wanted Enough, but wanted more
Some, but not enough None
We also asked survey respondents
whether they felt prepared for Chart 11: “I felt prepared for my
their needs assessment. Of the needs assessment” (Survey)
47 participants who answered the
question, 17 (50%) strongly agreed Unsure
or agreed, 11 (32%) disagreed or 18%
strongly disagreed, and six (18%)
were unsure. While it is encouraging
that half of respondents in Glasgow
felt prepared for their assessment, it Strongly
is concerning that nearly a third felt agree/ agree
unprepared and the rest were unsure.
Strongly 50%
disagree/
disagree
32%
Some interviewees in Glasgow
had been fully informed about the
options prior to their assessments,
but others had not been told about
all four options when they started
the process of accessing SDS. Those
that felt well prepared for their
initial assessment usually credited
an independent support and advice
organisation for providing them with
appropriate information (including
My Support My Choice: Glasgow - August 2021 26You can also read