Living Well with a Chronic Condition: Framework for Self-management Support - Self-management - HSE
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below

Living Well with a Chronic Condition:
Framework for Self-management Support
National Framework and Implementation Plan for Self-management Support for
Chronic Conditions: COPD, Asthma, Diabetes and Cardiovascular disease
Self-management
SupportThis framework and implementation plan was developed by a Health Service Executive (HSE) working group, under the
leadership of Dr. Orlaith O’Reilly National Clinical Advisor and Programme Lead Health and Wellbeing, with the support
of an advisory group. Membership of the working group is listed below and membership of the advisory group is listed in
Appendix 1.
Membership of the Self-management Support for Chronic Conditions Working Group
Name Title
Lead for development of National Self-management Support framework, Specialist in Public
Dr Carmel Mullaney
Health Medicine, Health and Wellbeing Division
Mairead Gleeson National Group Programme Manager Health and Wellbeing Division & Clinical Programmes
Geraldine Quinn Health Promotion and Improvement / Quality Improvement Division
Gemma Leane Research Officer, Public Health Department, Health and Wellbeing Division
Margaret Humphreys National Lead for Structured Patient Education
Maeve McKeon Self-management Support Coordinator, Donegal
Brid Kennedy Donegal Long Term Conditions Programme Manager
Specialist in Public Health Medicine, Department of Public Health, HSE North West, Health and
Dr Louise Doherty
Wellbeing Division
Kathleen Jordan Project Manager Self-management Support for Chronic Conditions (October 2016 – April 2017)Self-management Support National Framework and Implementation Plan for Self-management Support for Chronic Conditions: COPD, Asthma, Diabetes and Cardiovascular Disease
Foreword
Healthcare provided by professionals represents just months and years ahead. This work, when fully
the ‘tip of the ice-berg’ in supporting patients with implemented over a number of phases, will re-shape
chronic conditions. The majority of care for chronic and re-direct our focus toward the patient, their lived
conditions is provided by the person themselves. The experiences coping with and managing their health
majority of people over 65 years have two or more and their condition. It will support a collective shift
chronic conditions. Our population aged 65 years in emphasis toward creating enabling, supportive
and over is growing by approximately 20,000 each and transformative environments that put the patient
year, and with it the numbers living with chronic first, realising the value of active participation and
conditions. Enabling our health services to cope with effective collaborative interactions between patients
the increased number of people living with chronic and healthcare staff.
conditions, will depend on the extent to which people Finally, this Framework and the work ongoing to
engage with their own health and health conditions. implement it, will support a shared, common,
Supporting and empowering people in managing evidence–based understanding of how particular
their conditions as well as possible can improve models of care can better support patients and
quality of life and reduce the impact on health and reduce the pressure on healthcare services into
the likelihood of complications, hospitalizations and the future. We look forward to building support
deaths from these conditions. and increasing resources for the implementation
The National Self-management Support Framework of this framework nationally, regionally and locally
for Chronic Conditions: COPD, Asthma, Diabetes in collaboration with Community Healthcare
and Cardiovascular disease, sets out how we in the Organisations and Hospital Groups; in collaboration
health services, and working with patients and our with our patients and with partners in the wider
partners across the wider system, want to support health system, including general practice, academia,
patients to engage with and manage their conditions, voluntary groups and communities. Above all, we
through collaborative relationships and supportive look forward to the positive impacts on the health and
interventions. wellbeing of our patients and their families that will
Supporting self-management is inseparable from high ensue.
quality care for people with long term conditions and
is a priority for patients. Organisational and clinical Dr. Stephanie O’Keeffe,
leadership will be essential to support the culture
National Director, Health and Wellbeing
change necessary in moving from reactive to more
pro-active and person-centred care, with the patient
an active partner in their own healthcare. Dr Aine Carroll,
Self-management support is a critical element of our National Director, Clinical Strategy and Programmes
journey toward building a sustainable health service.
This Framework, focusing on people living with
chronic conditions, supports the implementation of
Healthy Ireland throughout the health services and
beyond. The concept of self-management is one
that cuts across the prevention spectrum (primary,
secondary and tertiary prevention) by establishing a
pattern for health early in life and providing strategies
for mitigating illness and managing it in later life.
The Framework and the approach set out, lays the
foundations for the work that is required over the
2 National Framework and implementation Plan for Self-management Support for Chronic Conditions: COPD, Asthma, Diabetes and Cardiovascular DiseaseIntroduction
Every day, people with long-term health conditions, the intensity of the intervention, but are typically
their family members and carers will make decisions, low relative to the overall cost of care for the chronic
take actions and manage a broad range of factors condition in question and in some instances, can
that contribute to their health. Self-management result in cost savings through reductions or shifts in
support acknowledges this and supports people to healthcare utilisation8,9.
develop the knowledge, confidence and skills they Self-management support is an important aspect of
need to make the optimal decisions and take the the Integrated Care Programme for the Prevention
best actions for their health. Evidence of positive and Management of Chronic Disease, and is key to
outcomes highlights the benefit of supporting people delivering person-centred care, in which patients are
to manage their own health as effectively as possible. empowered to actively participate in the management
These benefits can be felt by people with long-term of their condition.
health conditions, health professionals, and the health
It is closely aligned with the HSE goal of promoting
services1.
health and wellbeing as part of everything we do so
Chronic diseases are recognised as a major that people will be healthier10.
component of health service activity and expenditure,
Self-management support interventions are
as well as a major contributor to mortality and ill-
any interventions that help patients to manage
health. Thirty eight percent of Irish people over 50
portions of their chronic condition or conditions
years have one chronic condition, 11% have two or
through education, training and support8. The most
more of eight chronic conditions2 and 65% of adults
effective self-management support interventions
over 65 years have two or more chronic conditions3.
are multifaceted; tailored to the individual (their
The prevalence of diabetes, cardiovascular and
culture and beliefs) and tailored to specific
respiratory disease continues to increase due to our
conditions. They are underpinned by a collaborative
ageing population and prevalence of risk factors3.
relationship with a healthcare professional within a
People with chronic diseases presently utilise around
healthcare organisation that actively promotes self-
70% of health services resources4. They are more
management11.
likely to attend their GP, to present at Emergency
Departments, to be admitted as inpatients and to This framework sets out what the health services
spend more time in hospital, than people without must do to support people with chronic conditions
such conditions. Approximately 80% of GP in managing their conditions. The provision
consultations and 76% of hospital bed days used are of interventions at patient level is not enough.
related to chronic diseases and their complications5,6. International evidence indicates that we must also
It has been estimated that in Ireland approximately take action at the levels of healthcare professionals –
1 million people suffer from heart disease, diabetes education and training; the organisation – including
or respiratory disease7. For all chronic conditions the resourcing and coordination; and the wider system
prevalence is significantly higher in people with lower through working in partnership with GPs, academia
levels of education and in lower socio-economic and voluntary organisations, and patients themselves,
groups6. in order to successfully support self-management.
Supporting people to self-manage their health
conditions through systematic provision of education Dr. Orlaith O’Reilly,
and supportive interventions increases their National Clinical Advisor and Programme Lead,
skills and confidence and improves outcomes for Health and Wellbeing
patients – ranging from quality of life and clinical
outcomes, to reduced healthcare utilisation including
hospitalisation8. Reported costs vary according to
National Framework and implementation Plan for Self-management Support for Chronic Conditions: COPD, Asthma, Diabetes and Cardiovascular Disease 3Table of Contents
Executive Summary 6
Framework Recommendations 8
1. Background 11
1.1 Aims of the Framework 11
1.2 Methods 11
1.3 What is Self-management Support? 12
1.4 Rationale and Mandate for Self-management Support 13
Policy Context 13
2. Principles of the Self-management Support framework 14
3. Self-management Support Interventions 15
3.1 Current Provision of Self-management Support in Ireland 15
4. Whole System Model for Self-management Support for Chronic Conditions 17
4.1 Care Planning and Self-management Support 19
5. Recommendations 21
5.1 Individual Level - Disease Specific Self-management Support 21
Chronic Obstructive Pulmonary Disease ( COPD) 21
Asthma 21
Diabetes Types I and II 22
Ischaemic Heart Disease 22
Heart Failure 22
Stroke 23
Hypertension 23
5.2 Individual Level - Generic Supports to Self-management 24
Regular clinical review 24
Provision of Information 24
Health Behaviour Change Support 25
Support with Adherence to Medication and Dietary Changes 25
Generic Chronic Disease Self-management Education Programmes 26
Peer and Social Support 26
Carer Support 27
Multimorbidity 27
4 National Framework and implementation Plan for Self-management Support for Chronic Conditions: COPD, Asthma, Diabetes and Cardiovascular Disease5.3 Healthcare Professional Level 28
Workforce Development 28
5.4 Organisational Level 29
Governance 29
HSE Senior Management 30
Financial Support and Incentives 30
Quality Assurance, Evaluation and Monitoring 31
Technological Supports and Telehealth 31
5.5 Wider System 32
6. Priorities for Initial Implementation 33
7. Implementation Plan 34
7.1 Phase 1 2018-2021 34
7.2 Phase 2 42
8. Monitoring Implementation of the Framework 43
8.1 Measuring Initial Phase of Implementation 43
Further Key Performance Indicator Development 43
9. References 44
10. Abbreviations 48
11. Glossary of Terms 49
Appendix 1: Self-management Support framework Advisory Group 52
Appendix 2: Advisory Group terms of reference 54
National Framework and implementation Plan for Self-management Support for Chronic Conditions: COPD, Asthma, Diabetes and Cardiovascular Disease 5Executive Summary
Introduction Rationale and Mandate
Chronic diseases are recognised as a major Healthcare provided by professionals represents
component of health service activity and expenditure the ‘tip of the ice-berg’ in supporting patients with
in Ireland, as well as a major contributor to mortality chronic conditions. The majority of care for chronic
and ill-health. Every day, people with chronic health conditions is provided and coordinated by the person
conditions, their family members and carers will themselves, with the support of family members and
make decisions, take actions and manage a broad carers, at home and in the community. For example,
range of factors that contribute to their health. a person with diabetes has on average 3 hours
Self-management support acknowledges this contact a year with their healthcare team. They self-
and supports people to develop the knowledge, manage their condition for the remaining 8757 hours
confidence and skills they need to make decisions and in the year – dealing with symptoms; the effects of
take actions in relation to their health conditions. treatment; remembering to take medications; trying
This framework provides an overview of self- to change behaviour; dealing with the effects on
management support and offers recommendations emotions and relationships; and on the activities
for implementation of self-management support in of daily living. There is good evidence that certain
Ireland, along with a plan for implementation and interventions which support self-management,
priorities for early implementation. improve outcomes for patients – ranging from
quality of life and clinical outcomes, to reduced
The development of this framework was guided by a
healthcare utilisation including hospitalisation. The
national advisory group and was informed by Irish and
Patients’ Consultative Forum in 2011 identified self-
international evidence, including a Health Technology
management support as an integral part of clinical
Assessment conducted by the Health Information and
care for people living with chronic conditions.
Quality Authority (HIQA). An extensive consultation
Support for patient self-management is a key element
was carried out which included healthcare
of person-centred care, one of the four domains of
professionals within and outside the HSE; patients
quality in Irish healthcare.
and carers; representatives from the voluntary and
community sector; and the department of health. The ageing population and prevalence of risk factors
in the population means that the prevalence of these
chronic conditions will continue to increase year on
What is Self-management Support? year. Healthy Ireland in the Health Services - National
Implementation Plan includes actions to develop a
Self-management support is the systematic provision national framework for self-management support and
of education and supportive interventions, to increase development of services accordingly; and to increase
patients’ skills and confidence in managing their the proportion of patients utilising self-care and self-
health problems, including regular assessment of management supports. Self-management support is
progress and problems, goal setting, and problem- a work stream of the Integrated Care Programme for
solving support. It is an important element of person- the Prevention and Management of Chronic Disease.
centred care, acknowledging patients as partners in
their own care, supporting them in developing the
knowledge, skills and confidence to make informed
decisions.
6 National Framework and implementation Plan for Self-management Support for Chronic Conditions: COPD, Asthma, Diabetes and Cardiovascular DiseasePrinciples of the Self-management Whole System Model for Self-
Support Framework management Support for Chronic
There are four overarching, evidence-based principles Conditions
of self-management support which underpin this A whole system approach to implementation is
framework: recommended to support self-management of
1. Patients should be seen as active partners in their chronic conditions. Within the whole system model,
healthcare key actions are required at the levels of the patient,
2. Supporting self-management is inseparable the professional, the organisation and the wider
from high-quality care for people with long term system.
conditions Individual - Patients should have access to
3. Investment should be prioritised in those disease specific interventions which support their
interventions for which there is good evidence of self-management e.g. cardiac and pulmonary
clinical effectiveness, and rehabilitation, diabetes structured patient
4. A whole system approach to implementation of education, provision of asthma action plans. Generic
self-management support should be taken. interventions should also be provided including
regular clinical review, care and support planning,
provision of information, health behaviour change
Self-management Support support, peer and social support, generic self-
management education, and carer support.
Interventions
Healthcare professionals - Healthcare professionals
These are any interventions which help patients to should be provided with the skills and information
manage portions of their chronic conditions through they need in supporting self-management, including
education, training and support. The most effective adopting a person-centred approach and encouraging
self-management support interventions are those patient engagement.
which are multifaceted, tailored to the individual and Organisation - The healthcare organisation should
tailored to specific conditions; and are underpinned provide policy support; financial support and
by a collaborative relationship with a healthcare resources; coordination of delivery; technology
professional within a healthcare organisation that supports; quality assurance and evaluation.
actively promotes self-management.
Wider system - Wider system support is provided
Core components of these interventions include through partnership with non-HSE healthcare staff
education; psychological strategies; practical support such as General Practitioners (GPs), practice nurses
for physical care; action plans for use in deterioration and pharmacists; voluntary organisations and service
in conditions subject to exacerbations; and social users; community organisations; and academia.
support.
Effective self-management support should be
Evidence from a patient survey indicates a lack underpinned by a collaborative, communicative
of support for self-management in areas such as relationship between the patient and a trusted
information about their condition and provision healthcare professional. A self-management plan
of care plans. A survey of Community Healthcare should be jointly agreed, through a process of
Organisations (CHOs) found that a range of supports personalised care planning, between the patient and
are being provided but with wide variation in a trusted healthcare professional.
provision. This survey may form the baseline for the
development of local directories of available self-
management supports. Self-management support is
better developed in Donegal than other areas. Needs
assessments have indicated that provision of some
key self-management supports which are supported
by the strongest evidence of effectiveness (including
cardiac rehabilitation, diabetes structured patient
education and pulmonary rehabilitation) are well
below required levels.
Regular clinical review and care planning, which can
enable proactive management of chronic disease, are
not currently facilitated in General Practice in Ireland.
National Framework and implementation Plan for Self-management Support for Chronic Conditions: COPD, Asthma, Diabetes and Cardiovascular Disease 7Implementation Framework
Following on from the recommendations, are the Recommendations
actions in the high level implementation plan (Section
7). Some recommendations have been prioritised for Individual Level - Disease Specific
early implementation based on likelihood of maximum
Self-management Support
beneficial impact, and strongest evidence. These are:
•• Standardise and increase provision of cardiac 1. Implement the National Clinical Programmes’
rehabilitation recommendations on self-management support
•• Standardise and increase provision of pulmonary as per the Models of Care for COPD, asthma,
rehabilitation diabetes, heart failure, acute coronary syndromes
and stroke, across clinical settings
•• Increase provision of standardised diabetes
structured patient education 2. Implement the National Clinical Guidance on
Stroke and Transient Ischaemic Attack (TIA) in
•• Increase provision of care planning, initially
relation to self-management support, across
focusing on practice nurse training on asthma
clinical settings
management, including skills training and asthma
action plans 3. Provision of and access to standardised diabetes
structured patient education should be increased.
•• Include self-management support for chronic
Specific self-management support programmes of
conditions as part of the undergraduate curriculum
proven benefit e.g. the DAFNE programme should
for health and social care professionals to ensure
be available for patients with diabetes type I
they have the knowledge, skills and confidence to
embed self-management support (including person- 4. Structured exercise based programmes such as
centred care) into their professional practice cardiac and pulmonary rehabilitation, should be
standardised nationally and provision and access
•• Recruit self-management support co-ordinators
increased
for each CHO to ensure implementation of the
self-management support framework, including 5. Implement support for self-management of
mapping current self-management support hypertension, including self-monitoring of blood
provision; creation of local directories of self- pressure, and information and support for health
management support services; and development of behaviour change, in conjunction with improved
self-management support plans for each CHO diagnosis and treatment of hypertension
•• Develop a patient guide to self-management 6. Future development of national disease
support to engage patients and carers, and to specific guidelines should include evidence-
promote self-management of chronic conditions. based recommendations on supporting self-
management
Monitoring and Implementation of
Individual level - Generic Supports
the Framework
to Self-management
Key performance indicators and other measurement
tools will be developed. Use of existing datasets 7. Put in place regular clinical review incorporating
where appropriate will avoid duplication of effort. care planning – including self-management
Outcome measures will include clinical, healthcare plan - for patients diagnosed with these
utilisation and patient experience measures. chronic conditions (COPD, asthma, diabetes
& cardiovascular disease), supported by
appropriate resources and training for healthcare
professionals - to enable integration of self-
management support into routine clinical care
8. Identify patients’ and carers’ needs and
preferences for information, including health
literacy needs, when developing resources
8 National Framework and implementation Plan for Self-management Support for Chronic Conditions: COPD, Asthma, Diabetes and Cardiovascular Disease9. Promote the development and co-ordination of Healthcare Professional Level
consistent information resources, informed by
patients and carers needs and preferences, across 20. Work in collaboration with third level institutions
care settings and professional organisations to develop
10. Ensure that self-management skills are undergraduate and postgraduate curricula for
incorporated into disease specific patient healthcare professionals in self-management
education and training (e.g. problem solving, goal support for chronic conditions
setting) 21. Training should be provided to frontline
11. A range of health behaviour change interventions healthcare professionals to provide self-
should be available to patients including support management support, including personalised care
from their regular healthcare professional and planning
referral to other services e.g. smoking cessation, 22. Ensure adequate resourcing at CHO and Hospital
exercise interventions - based on the individual’s Group level for delivery of self-management
self-management support needs support; including release for staff training
12. Support the implementation of the “Making Every 23. Promote engagement of healthcare professionals
Contact Count” framework for health behaviour through digital and other means, to increase
change knowledge, awareness and practice of self-
13. Ensure a range of interventions are provided to management support
promote adherence to medications and support
for dietary behaviour change, including those
provided by Pharmacists and Nurses, and dietetic
Organisational Level
services 24. A National SMS programme lead will be assigned
14. Provide generic chronic disease self-management to coordinate the roll-out, implementation,
education programmes as part of a range of phasing and further development of the plan.
available self-management supports and targeted Implementation will be overseen by a National
to those most likely to benefit (younger patients, Oversight Group, with internal, external and
those lacking confidence, and those coping patient representation to advise and guide the
poorly with their condition(s)) work as it develops.
15. Healthcare professionals, and others involved 25. Specific implementation supports will be put
with the care of those with chronic conditions, in place in relation to the national strategy and
should link people with non-medical sources of planning function; operations support; and
social and peer support within the community, clinical supports.
appropriate to their needs, through signposting 26. The supports outlined above will form a national
and /or social prescribing SMS programme team which will also include
16. Social Prescribing should be developed to enable nine self-management support coordinators, one
social and peer support, targeted at identified for each CHO.
‘high need’ groups 27. There should be named leads at CHO and HG
17. Social and peer supports should be included in levels to ensure implementation of the SMS
local CHO self-management support directories framework including governance, co-ordination,
18. Spouses, family or carers should be included in quality assurance, communication and evaluation
patient education and other self-management
support interventions where possible and
appropriate
19. Support the development of effective self-
management support programmes for people
with multiple chronic conditions
National Framework and implementation Plan for Self-management Support for Chronic Conditions: COPD, Asthma, Diabetes and Cardiovascular Disease 928. Each CHO and Hospital Group should have a 36. Continue to develop a central referral,
local plan for self-management support led by the coordination and evaluation system for structured
Health and Wellbeing leads (CHO) and Healthy programmes (commenced in 2015 for diabetes
Ireland leads (Hospital Groups (HG)). These plans structured patient education) to help to facilitate
should include mapping of local services which standardisation, and ongoing audit and evaluation
support self-management for signposting to 37. Quality assurance, and routine and ongoing
patients, identification of service gaps where they evaluation of programmes should be undertaken
exist, considering in particular the needs of ‘hard including patient outcomes and experience of
to reach’ groups, and mechanisms for quality care provided
assurance and evaluation of local programmes
38. Key Performance Indicators (KPIs) and reporting
29. Promote understanding of the value of self- systems should be developed to monitor
management support and its role in person- achievements
centred, integrated care, to ensure its recognition
39. Technological supports, telehealth and telephonic
and incorporation in service development
health coaching should be considered where
30. Ensure adequate resourcing of primary care teams evidence supports them, as a mode of delivery
to facilitate the provision of self-management for self-management support, or as one element
support, addressing the issue of fragmented and of more complex interventions. As technological
inadequate services at community level developments and population requirements
31. Provide resources for education and training of evolve over time, appropriate recommendations
healthcare professionals and facilitate release of should be made accordingly. Cost and evaluation
staff for training must be considered as some telehealth
32. Ensure the development of evidence informed interventions can be high cost.
self-management support interventions for
patients within the HSE and through external
providers
Wider System
33. Ensure existing and future national ICT systems 40. Develop the roles of GPs and practice nurses
including electronic health records; Healthlink; in relation to care planning and signposting to
and other initiatives, are used to support the supports, as an essential part of the delivery of
implementation of SMS, including information care
sharing and continuity across services and care 41. Develop partnerships with the community and
settings, and performance management voluntary sectors which support self-management
34. Support the implementation of self-management 42. Engage with providers such as community
support elements of the clinical programmes pharmacists to maximise their ability to support
models of care and this framework through self-management
financial means - via the GP contract; through
43. Engage with professional and regulatory bodies
Grant Agreements with voluntary and community
regarding the role of Continuous Professional
organisations; and through HSE services:
Development (CPD) in developing and
•• Create budgets for SMS implementation at maintaining relevant self-management support
national and CHO/HG level skills
•• Make available Innovation funding to 44. Develop partnerships with academia to ensure
encourage development of evidence-informed gaps in the evidence are addressed including
self-management support programmes and effective self-management support for patients
initiatives e.g. in providing SMS to ‘hard to with multiple chronic conditions
reach’, or marginalised groups
35. Interventions should be standardised at national
level and subject to routine and ongoing
evaluation
10 National Framework and implementation Plan for Self-management Support for Chronic Conditions: COPD, Asthma, Diabetes and Cardiovascular Disease1. Background
Chronic diseases are recognised as a major
component of health service activity and expenditure,
1.1 Aims of the Framework
as well as a major contributor to mortality and The aims of this framework are to:
ill-health. Thirty eight percent of Irish people over
•• Provide an overview of self-management support
50 years have one chronic condition, 11% have
two or more of eight chronic conditions (heart •• Provide recommendations on how self-management
attack, angina, stroke, diabetes, asthma, COPD, support for four major chronic conditions – chronic
musculoskeletal pain and cancer)2, and 65% of adults obstructive pulmonary disease (COPD), asthma,
over 65 years have two or more chronic conditions3. diabetes and cardiovascular disease - should be
implemented in the Irish health system
It has been estimated that in Ireland approximately
1 million adults have cardiovascular or respiratory •• Inform a plan for the implementation of the self-
disease or diabetes7. Over the age of fifty, it has management support framework
been estimated that 625,000 people suffer from •• Guide prioritisation of investment in self-
cardiovascular disease, respiratory disease or management support initiatives according to the
diabetes*12. For all chronic conditions the prevalence evidence base.
is significantly higher in people with lower levels of
education and in lower socio-economic groups6.
The prevalence of these diseases continues to 1.2 Methods
increase due to our ageing population and prevalence The following methods were used in developing this
of risk factors3. People with chronic diseases presently framework:
utilise around 70% of health services resources4.
•• A Health Technology Assessment (HTA) was
They are more likely to attend their GP, to present at
carried out by the Health Information and Quality
Emergency Departments, to be admitted as inpatients
Authority (HIQA) in 2015 at the request of the HSE
and to spend more time in hospital, than people
to examine the clinical and cost-effectiveness of
without such conditions. Approximately 80% of GP
generic self-management support interventions for
consultations and 76% of hospital bed days used are
chronic diseases and disease-specific interventions
related to chronic diseases and their complications5,6.
for COPD, asthma, cardiovascular disease and
Every day, people with chronic health conditions, diabetes8.
their family members and carers will make decisions,
•• Other key literature – including reviews of
take actions and manage a broad range of factors
implementation evidence on self-management
that contribute to their health. Self-management
support published in 2014 (PRISMS11 and
support acknowledges this and supports people to
RECURSIVE9 studies) – and international policy
develop the knowledge, confidence and skills they
documents were reviewed; together with the
need to make the optimal decisions and take the
relevant National Clinical Programmes models of
best actions for their health. Evidence of positive
care and supporting documents.
outcomes highlights the benefit of supporting people
to manage their own health as effectively as possible. •• A survey was carried out to identify existing self-
These benefits can be felt by people with chronic management support provision in Ireland13
health conditions, health professionals, and the health •• Other evidence on provision in the Irish health
services1. system was reviewed. (See Section 3.1)
* This estimate was made using TILDA data and includes: CHD, Heart failure, stroke, TIA, diabetes, COPD, Asthma, Atrial Fibrillation and
Hypertension12. See acknowledgements in reference section.
National Framework and implementation Plan for Self-management Support for Chronic Conditions: COPD, Asthma, Diabetes and Cardiovascular Disease 111. Background
•• The findings of consultations carried out with the The person
Patients’ Consultative Forum in 2011 were reviewed, •• Knows about their condition
together with the ‘Framework for Self-management
•• Follows a treatment plan (care plan) agreed with
Support, Long-Term Conditions’14 which followed
their health professionals
on from those consultations15. The Patients’
Consultative Forum was established in January 2011 •• Actively shares in decision-making with health
to facilitate communication and consultation with professionals
regards to the design, delivery and evaluation of the •• Monitors and manages signs and symptoms of
national clinical programmes. their condition
•• A national advisory group (Appendix 1) was set up in •• Knows how to respond to a deterioration in their
2016 to assist with development and finalisation of condition
the framework. •• Manages the impact of the condition on their
•• An initial draft of the framework was further physical, emotional and social life
refined through a national consultation in 2016. •• Adopts lifestyles that promote health
This consultation included focus groups with •• Has access to support services and has the
healthcare professionals both within and outside confidence and ability to use them.
the HSE, patients and representatives of patient
organisations; and interviews with HSE senior
Self-management support is defined as
management, and ICGP and Department of Health
the systematic provision of education and
representatives16.
supportive interventions, to increase patients’
•• The national consultation also informed the skills and confidence in managing their health
development of the high level implementation plan problems, including regular assessment of
for the framework. progress and problems, goal setting, and
problem-solving support (Adapted from Institute
of Medicine, 2003)17.
1.3 What is Self-
Person-centred care and support is the first theme
management Support? of “National Standards for Safer Better Healthcare”,
Self-management is defined as the tasks that the national healthcare standards19. Self-management
individuals must undertake to live with one or more support is an important element of person-
chronic conditions. These tasks include having the centred care for people with chronic conditions8,
confidence to deal with medical management, role acknowledging patients as partners in their own care,
management and emotional management of their and supporting them in developing knowledge, skills
condition17. and confidence to make informed decisions20.
Examples of self-management tasks: Self-management is the responsibility of individuals,
however, this does not mean people doing it alone.
•• Monitoring symptoms and signs e.g. weight gain
Successful self-management relies on people having
(in heart failure), peak flow rate (asthma), blood
access to the right information, education, support
glucose levels (diabetes), knowing when to seek
and services. It also depends on professionals
medical assistance and from whom
understanding and embracing a person-centred,
•• Remembering to take medications - at the correct empowering approach in which the individual is
dosage and time, adjusting if appropriate the leading partner in managing their own life and
•• Changing health behaviours e.g. level of physical condition(s)21.
activity, stopping smoking, healthy eating Many self-management support interventions
•• Dealing with the effects of the condition on focus on increasing self-efficacy i.e. increasing an
activities of daily living –adjusting to living with individual’s confidence in their ability to carry out a
disability e.g. for people who have had a stroke, certain task or behaviour, thereby empowering the
dealing with effects on employment individual to self-manage (HIQA 2015)8.
•• Dealing with the effect of the condition on emotions Self-care is defined as the actions people take to
and relationships e.g. with spouse or family; care for themselves, their children and their families
managing symptoms of anxiety or depression to stay fit and well. This includes: staying fit and
resulting from or co-existing with the condition healthy, both physically and mentally; taking action
The following characteristics describe someone who to prevent illness and accidents; correct use of
is able to self-manage their long term condition:18 medicines; treatment of minor, self-limiting illnesses
and better care of long-term conditions. Self-care
is understood to include the self-management of
chronic conditions22.
12 National Framework and implementation Plan for Self-management Support for Chronic Conditions: COPD, Asthma, Diabetes and Cardiovascular Disease1. Background
1.4 Rationale and Mandate In Ireland, a significant increase in the older population
(aged 65 years and over) is predicted, from 532,000
for Self-management in 2011 to over 734,000 in 2021, and over 1.4 million by
Support 204623. This increase, together with the prevalence
of risk factors, will give rise to a continuing increase
Healthcare provided by professionals represents in chronic diseases with the consequent burden on
just the ‘tip of the ice-berg’ in supporting patients individuals and the healthcare system.
with chronic conditions. The majority of care for
chronic conditions is provided by and coordinated
Policy Context
by the person themselves with the support of family
members and carers, at home and in the community. Supporting people with chronic conditions to manage
“A person with diabetes has on average 3 hours their health conditions, enabling them to live as well
contact a year with their healthcare team. They as possible, aligns with the HSE goal of promoting
self-manage their condition for the remaining 8757 health and wellbeing as part of everything we do
hours in the year” 23 so that people will be healthier10. It is an important
element of person-centred care which is a key domain
The Patients’ Consultative Forum in 2011 identified
of quality in Irish healthcare19, 20 and supported under
self-management support as an integral part
legislation in the Health Act 2007.
of clinical care for people living with chronic
conditions15. The 2012 framework which followed, National policies recommend that patients should
recommended a ‘whole systems approach’ in be encouraged and empowered to self-manage
implementing high quality self-management support their conditions: Tackling Chronic Disease – A
within the Irish healthcare system. It identified three Policy Framework for the Management of Chronic
strategic actions as central to this: Diseases5 (2008), states that “patients should actively
participate in the management of their condition”.
•• empowering patients
Future Health3 (2012) recommends “programmes
•• enabling healthcare professionals to support self- of self-care for patients to encourage better self-
management monitoring and treatment of chronic disease”.
•• and improving access to self-management Healthy Ireland: A Framework for Improved Health
supports14. and Wellbeing 2013 – 202527 (2013), recognises the
need to implement a model for the prevention and
Self-management and self-management support are
management of chronic illnesses, empowering
core elements of high quality, evidence based care for
people and communities, with an emphasis on
people with chronic health conditions11. The Chronic
partnership and cross-sectoral work to increase
Care Model makes clear the role of self-management
the proportion of people who are healthy at all
support in the management of chronic conditions24.
stages of life. Healthy Ireland in the Health Services -
This model has broad international acceptance as a
National Implementation Plan28 (2015), addresses this
framework to provide guidance on shifting from our
through actions to develop and implement a national
current model of care which is predominantly acute and
framework for self-care for the major cardiovascular,
episodic care, to a lifelong model of health promotion,
respiratory diseases and diabetes and to develop
prevention, early intervention and chronic care.
services accordingly (Actions 26 and 43) and to
Self-management support interventions can improve increase the proportion of patients utilising self-care
outcomes for patients – ranging from quality of and self-management supports (Action 44).
life and clinical outcomes, to reduced healthcare The self-management support framework for is a
utilisation including hospitalisation8. International work stream of the Integrated Care Programme for
evidence suggests that most self-management the Prevention and Management of Chronic Disease.
support interventions are relatively inexpensive to Other actions arising from the Healthy Ireland
implement. Reported costs vary according to the implementation plan address modifiable risk factors
intensity of the intervention, but are typically low and take a life course perspective on chronic conditions
relative to the overall cost of care for the chronic including supporting self-management, so are strongly
condition in question and in some instances, can linked with the self-management support framework.
result in modest cost savings through reductions or These include the ‘Making Every Contact Count
shifts in healthcare utilisation8,9. framework for health behaviour change’29; and the
Supporting self-management is considered critical by National Policy Priority Programmes: Alcohol; Tobacco
the World Health Organization (WHO) for “countries Free Ireland; Healthy Eating and Active Living; Positive
where ageing populations and the growing burden of Ageing; Wellbeing and Mental Health; and Healthy
non-communicable disease means that there is ever Childhood.
greater demand for health services”25.
National Framework and implementation Plan for Self-management Support for Chronic Conditions: COPD, Asthma, Diabetes and Cardiovascular Disease 132. Principles of the
Self-management Support
framework
The following evidence based principles of self- •• A whole system approach to implementation of
management support underpin this framework: self-management support should be taken. Key
actions are required at the levels of:
•• Patients should be seen as active partners in
their healthcare. Self-management support is key ––The patient
to empowering patients. This means providing ––The healthcare professional
patients with the opportunities and the environment ––The organisation
to develop the skills, confidence and knowledge to
––The wider system.
move from being passive recipients of care to being
active partners in their healthcare30. The healthcare organisation is responsible for
providing the means (both training and time/material
•• Supporting self-management is inseparable
resources) to enable professionals to implement
from high-quality care for people with long term
self-management support and to enable patients to
conditions. This was the key theme from combined
benefit from self-management support, regularly
qualitative and quantitative meta-reviews and an
evaluating self-management support processes and
implementation systematic review published in
clinical outcomes1, 11.
2014. Health services should consider how they
can promote a culture of actively supporting self-
management as a normal, expected, monitored and
rewarded aspect of the provision of care11.
•• Investment should be prioritised in those
interventions for which there is good evidence
of clinical effectiveness. Where chronic disease
self-management support interventions are
provided, it is critical that an agreed definition
of self-management support interventions is
developed and the implementation and delivery of
the interventions are standardised at a national level
and subject to routine and ongoing evaluation8.
14 National Framework and implementation Plan for Self-management Support for Chronic Conditions: COPD, Asthma, Diabetes and Cardiovascular Disease3. Self-management
Support Interventions
Self-management support interventions are Examples of self-management support
any interventions that help patients to manage interventions:
portions of their chronic condition or conditions •• Asthma education supported by written action
through education, training and support8. The most plan and skills training
effective self-management support interventions
•• Structured education programmes incorporating
are multifaceted; tailored to the individual (their
self-management skills (e.g. diabetes structured
culture and beliefs) and tailored to specific
patient education)
conditions. They are underpinned by a collaborative
relationship with a healthcare professional within a •• Cardiac rehabilitation programmes; pulmonary
healthcare organisation that actively promotes self- rehabilitation programmes
management11. •• Regular clinical review incorporating care
planning, and self-management plan
The core components of self-management support •• Health coaching
interventions include:11 •• Support for health behaviour change
•• Education - provision of knowledge and information e.g. smoking cessation support; exercise
about the long term condition interventions; dietetic consultations and support
•• Psychological strategies to support people adjusting •• Provision of high quality consistent information
to life with a long term condition appropriate to the needs of the individual
•• Practical support for physical care tailored to the •• Peer support e.g. support groups – face to face,
specific long term condition including telephone, internet based
––Coping with activities of daily living for people •• Community based supports e.g. walking groups.
with disabling conditions
––Action plans to advise on prompt appropriate
action in the event of deterioration, in conditions 3.1 Current Provision of
subject to marked exacerbations
––Intensive disease-specific training to enable self-
Self-management Support
management of specific clinical tasks in Ireland
•• Social support as appropriate
The surveys of patients and clinical stakeholders
•• Other potentially effective components include by Darker et al.31 published in 2015, provide Irish
self-monitoring with feedback and practical support evidence of the importance of self-management
with adherence strategies tailored to the individual. support to patients, and the current lack of support
No one component has been shown to be more in key areas such as information about their condition
important than any other, or effective in isolation. and provision of care plans. Patients rated the
importance of good knowledge of their condition
as ‘extremely important’, however only a minority of
patients reported receiving written information on
how to manage their chronic condition at home. Only
one in four patients received a written care plan, and
only a minority were asked about their ideas or goals
when making a treatment plan.
National Framework and implementation Plan for Self-management Support for Chronic Conditions: COPD, Asthma, Diabetes and Cardiovascular Disease 153. Self-management Support Interventions
The HSE carried out a survey of Community Other sources indicate that provision of some key
Healthcare Organisations (CHOs) in 2015 to identify self-management supports, including those which are
existing self-management supports13. The survey supported by the strongest evidence of effectiveness,
report was supplemented by other information are well below required levels:
to provide as complete a picture as possible and •• A national needs assessment for cardiac
may form a baseline for the development of local rehabilitation carried out in 2016 found that there
directories of available self-management supports. was capacity to meet only 39% of need. Need was
The services and programmes available in all assessed for patients with coronary heart disease
CHOs were: cardiac rehabilitation, pulmonary or heart failure. When broader referral criteria were
rehabilitation, structured patient education for included, the capacity was even lower32.
diabetes and smoking cessation services. Stroke
•• A national needs assessment for pulmonary
support groups are found throughout the country, but
rehabilitation carried out in 2016 found that there
stroke rehabilitation programmes are not available
was capacity to provide only 11% of need33.
everywhere.
•• An audit of diabetes structured patient education
Generic chronic disease self-management
indicated that in 2014, structured patient education
programmes based on the Stanford model are run in
courses for type II diabetes were completed by 2755
a number of acute hospitals, CHOs, and by voluntary
people34. Estimates of annual increase in number of
organisations.
cases suggest an additional 4,000 cases per year in
Community based programmes (e.g. smoking adults over 45 alone35. It is estimated that 190,000
cessation) and supports (e.g. walking groups, stroke people in Ireland have diabetes (90% type II), and
support groups, community cooking programmes) are the prevalence is increasing every year, in line with
provided to varying extents in different areas. While global trends36, highlighting the need to improve
some areas reported a number of wider community access to and provision of structured education.
supports available, others reported very few of these.
•• A 2015 audit of stroke services found that general
One possible reason for the variation is differing
rehabilitation services for stroke patients are
levels of knowledge among healthcare professionals
lacking in the acute setting and indicated very little
responding. The survey did not provide information
provision of community rehabilitation services37.
about the numbers of patients taking any of these
programmes, waiting lists, or whether provision is
adequate to meet need.
CHO1 has implemented coordination of self-
management support as part of its long-term
conditions work in Donegal, and developed
social prescribing to direct high needs patients to
appropriate social and peer supports.
Personalised care planning, a process which
encourages healthcare professionals and people with
chronic conditions, and their carers, to proactively
manage their conditions, including identifying and
directing them to supports needed by them to self-
manage, is not currently facilitated in primary care.
16 National Framework and implementation Plan for Self-management Support for Chronic Conditions: COPD, Asthma, Diabetes and Cardiovascular Disease4. Whole System Model for
Self-management Support
for Chronic Conditions
A whole system approach to implementation is 2. Healthcare professionals - interventions such as
recommended to support self-management11. Within training and education, which provide healthcare
the healthcare system, patient self-management can professionals with the skills and information they
be supported by interventions provided at different need in supporting self-management, including
levels:11 adopting a person-centred approach and
1. The individual – interventions aimed at enabling encouraging patient engagement
patients and carers to be engaged and informed 3. Organisation – interventions which support
which are provided directly to patients and patient self-management through policy support;
carers include financial support and resources; provision
•• Disease specific interventions of information; promotion of peer support;
coordination of delivery; optimising use of
––By individual disease area – COPD, asthma,
technology; quality assurance and evaluation
diabetes, cardiovascular disease
4. Wider system support e.g. through partnerships
•• Generic interventions
with voluntary organisations; developing the
––Regular clinical review role of GPs and practice nurses; partnerships
––Care and support planning with service user and voluntary organisations;
––Provision of information promoting research and innovation.
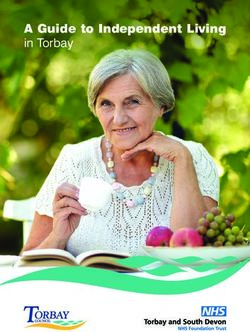
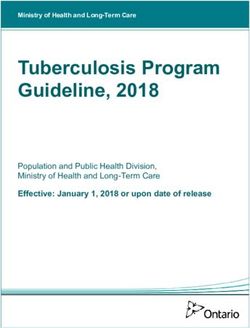
––Health behaviour change support This approach is illustrated in Figure 1. Detailed
––Peer and social support recommendations at each of the four levels are given
in Section 5.
––Generic self-management education
––Carer support
National Framework and implementation Plan for Self-management Support for Chronic Conditions: COPD, Asthma, Diabetes and Cardiovascular Disease 1718
Figure 1: Whole System Model for Support for Self-management for Chronic Conditions
The person who is able to Patients and Carers will have Informed and Skilled Health Organisational Support Wider System Support
self-manage their long term timely access to: Care Professionals for Self-management for Self-management
condition:
• knows about their condition • Disease specific self- Through education and training in • Policy support Through partnership working with
• follows a treatment plan (care management support (e.g. self-management support including: • Coordination of service delivery external providers including:
plan) agreed with their health diabetes structured education, • communication skills • Financial support • General Practitioners
professionals cardiac rehab, pulmonary rehab, • person-centred care • Voluntary/Community
• Resources
asthma education) Organisations
• actively shares in decision- • health behaviour change • Optimising use of technology
making with health • Generic interventions: • Professional and Regulatory
• care and support planning (including telehealth and
professionals – regular clinical review telemedicine) Bodies
• collaborative agenda setting
• monitors and manages signs – care planning • Quality assurance (evaluation to • Academia, including higher
• goal setting, action planning and
and symptoms of their condition – provision of appropriate include patient experience) education institutions
follow up
• knows how to respond to a information • group facilitation
deterioration in their condition – health behaviour change
• manages the impact of the support
condition on their physical, – peer and social support
emotional and social life
– generic self management
• adopts lifestyles that promote education
health
– carer support
• has access to support services
and has the confidence and
ability to use them
t
In
en
fo
rm
Person Supported
to Self-manage
ed an
Care
d Carers
S e l f- m a n a g e m
Plan Engaged a
d S k ill e
san
ng
nd
In t
dH
r ti
en
e
fo r
po
al
th m e d Pati
t
O Ca up
en
sS
rg
an re P n al
r o fe s s i o em
isa g
W tio
nS a na t
id u p p o r t fo r S e l f- m en
er
Sy g em
st
National Framework and implementation Plan for Self-management Support for Chronic Conditions: COPD, Asthma, Diabetes and Cardiovascular Disease
em ana
S u p p o r t f o r S e l f- m
4. Whole System Model for Self-management Support for Chronic ConditionsYou can also read