Clinical Guidelines & Standard Operating Procedure for the Implementation of the Short & Long DR-TB regimens for Adults, Adolescents and Children ...
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
CHIEF DIRECTORATE: HEALTH PROGRAMMES
Acting Chief Director: Mr James Kruger
Enquiries: Dr Vanessa Mudaly/ Ms Razia Vallie
Ref: 19/5/1/11/1
Clinical Guidelines & Standard Operating Procedure for
the Implementation of the Short & Long DR-TB regimens
for Adults, Adolescents and Children
Updated November 2018
(In accordance with “Interim Clinical Guidance for the implementation of injectable-free
regimens for Rifampicin-resistant tuberculosis in adults, adolescents and children”
published by National Department of Health- South Africa: September 2018)
1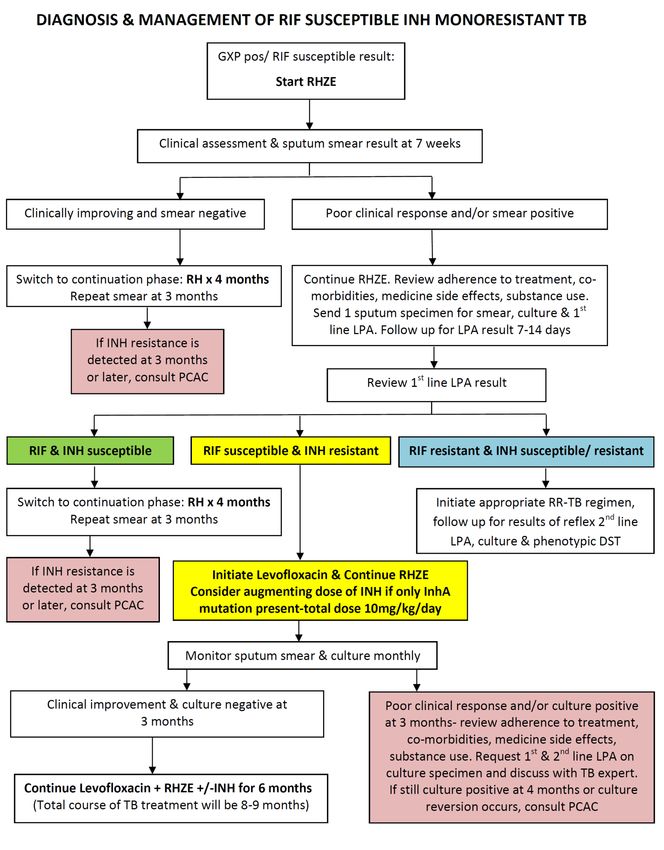
Compiled by
Dr Vanessa Mudaly & Ms Jacqueline Voget
Acknowledgements
We acknowledge the invaluable contributions received from members of the National & Provincial
DR-TB Clinical Advisory Committee (NCAC & PCAC), Western Cape DR-TB Task Team, National Health
Laboratory Service (NHLS) and Paediatric DR-TB experts, particularly Prof Gary Maartens, Prof
Graeme Meintjes, Prof Keertan Dheda, Dr Anja Reuter, Dr Jenny Hughes, Dr Julian Te Riele, Ms
Chantal Fourie, Dr Lenny Naidoo, Ms Judy Caldwell, Dr Natalie Beylis, Prof Simon Schaaf and Dr
Anthony Garcia-Prats. Special thanks to the City of Cape Town for use of the DR-TB medicine dosing
and clinical monitoring tools.
2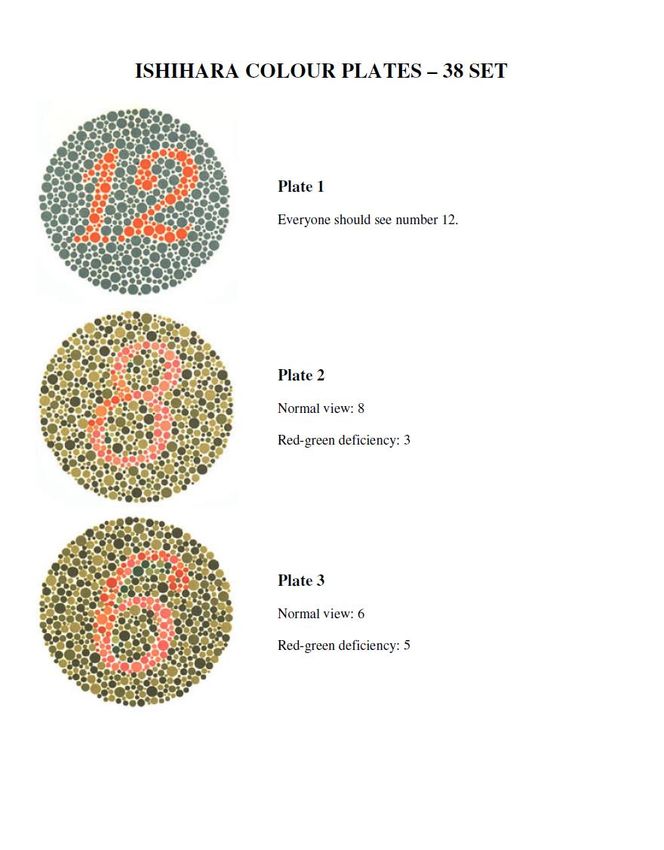
Contents
1. Introduction ................................................................................................................................................... 7
1.1 DR-TB Definitions.......................................................................................................................................... 7
1.1.1 Mono-resistant TB ................................................................................................................................. 7
1.1.2 Poly-drug resistant TB ........................................................................................................................... 7
1.1.3 Rifampicin resistant TB (RR-TB) ............................................................................................................ 7
1.1.4 Multidrug-resistant TB (MDR-TB) .......................................................................................................... 7
1.1.5 Pre XDR-TB ............................................................................................................................................. 7
1.1.6 Extensively drug-resistant TB (XDR-TB)................................................................................................ 7
1.1.7 Heteroresistant TB infection ................................................................................................................ 7
1.2 Background................................................................................................................................................. 8
1.3 Current Treatment Regimens for RR/MDR-TB in South Africa ............................................................... 9
1.4 New Short & Long Treatment Regimens for DR-TB in SA ....................................................................... 9
2. Overview of the Short Regimen for RR/MDR-TB Treatment .................................................................. 10
2.1Eligibility Criteria ......................................................................................................................................... 10
2.1.1 Inclusion Criteria ................................................................................................................................. 10
2.1.2 Exclusion Criteria ................................................................................................................................ 10
2.2 Treatment duration .................................................................................................................................. 11
2.3 Anti-TB Medicines included in the Short Regimen ............................................................................... 11
2.4 Treatment regimen for Adults & Adolescents ≥12 yrs (>30kg) ........................................................... 13
2.5 Treatment regimens for Children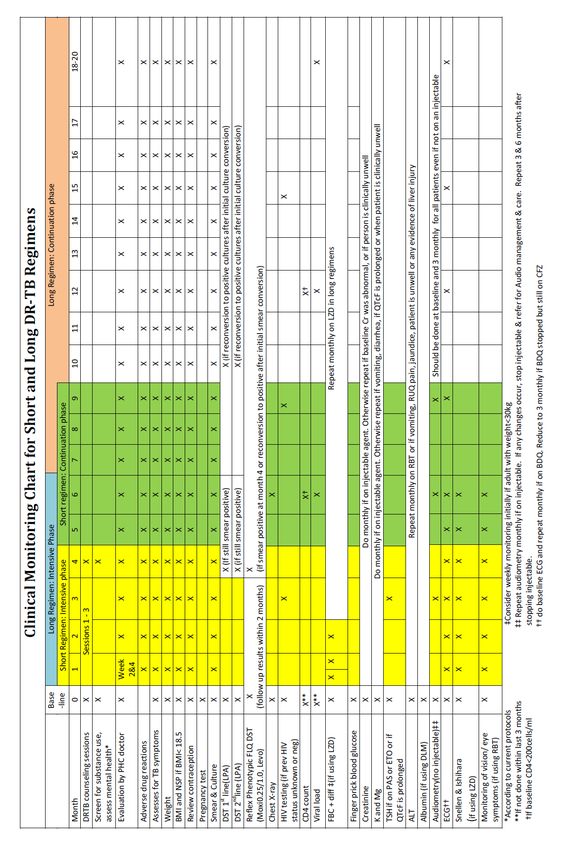
RR/MDR-TB CNS Disease ............................................................................................................................ 21 3.3.3 Treatment regimen for Children
List of Boxes Box 1: Short Treatment Regimen for RR/MDR TB for Adults, Adolescents ≥12 yrs (>30kg) ........................ 13 Box 2: Short Regimen for RR/MDR Treatment in Children6-12 years (15-30kg) .......................................... 14 Box 3: Short Regimens for RR/MDR Treatment in Children
Abbreviations & Acronyms
ART Anti-Retroviral Treatment
BDQ Bedaquiline
CNS Central Nervous System
CFZ Clofazimine
DLM Delamanid
DR-TB Drug Resistant Tuberculosis
DST Drug Susceptibility Test
E Ethambutol
ECG Electro-cardiogram
EDST Extended Drug Susceptibility Test
EPTB Extra-Pulmonary Tuberculosis
ETO Ethionamide
FBC Full Blood Count
FLQ Fluoroquinolone
GXP GeneXpert
HIV Human Immunodeficiency Virus
INH/ INHhigh dose Isoniazid/ Isoniazid high dose
INJ Injectable agent
IRIS Immune Reconstitution Inflammatory Syndrome
KM Kanamycin
LFX Levofloxacin
LPA Line Probe Assay
LZD Linezolid
MO Medical Officer
MFX Moxifloxacin
MDR Multi-Drug Resistant
NCAC National Clinical Advisory Committee
NDoH National Department of Health
PCAC Provincial Clinical Advisory Committee
RIF Rifampicin
RR Rifampicin Resistant
SAHPRA South African Health Products Regulatory Authority
TRD Terizidone
XDR Extensively Drug Resistant
WHO World Health Organization
Z Pyrazinamide
6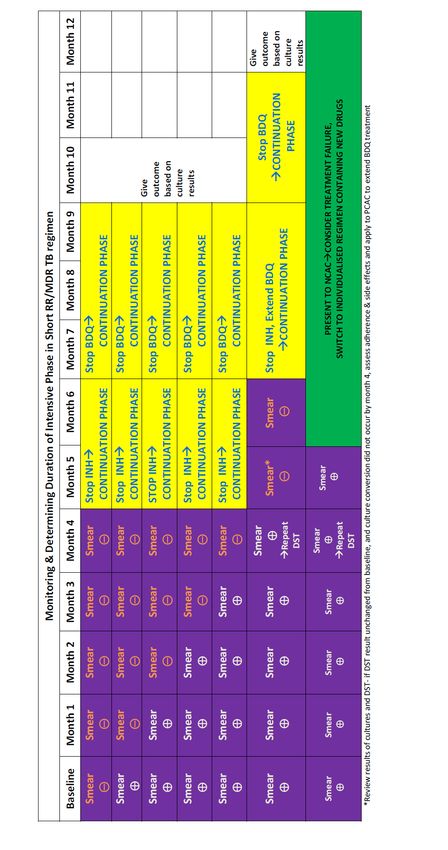
1. Introduction
1.1 DR-TB Definitions
Drug-Resistant tuberculosis (DR-TB) refers to active tuberculosis disease caused by
Mycobacterium tuberculosis (Mtb) bacilli that are resistant to one or more anti-TB medicines.
1.1.1 Mono-resistant TB
Resistance to only one first line anti-TB medicine, without resistance to other anti-TB medicines:
o Rifampicin(RIF) monoresistant TB- resistant to RIF only
o Isoniazid (INH) monoresistant TB- susceptible to RIF and resistant to INH only (section 13.1)
1.1.2 Poly-drug resistant TB
Resistance to more than one anti-TB medicine, other than both RIF and INH.
1.1.3 Rifampicin resistant TB (RR-TB)
Resistance to at least RIF, with or without resistance to other anti-TB medicines. Includes
RIF- mono-resistant TB, MDR-TB, pre-XDR-TB and XDR-TB
1.1.4 Multidrug-resistant TB (MDR-TB)
Resistance to both RIF and INH with or without resistance to other anti-TB medicines
1.1.5 Pre XDR-TB
Resistance to both RIF and INH (MDR-TB) with additional resistance to either a fluoroquinolone or
any one of the second-line injectable medicines (kanamycin, amikacin or capreomycin)
1.1.6 Extensively drug-resistant TB (XDR-TB)
Resistance to both RIF and INH (MDR-TB) with additional resistance to both a fluoroquinolone
and any one of the second-line injectable medicines
1.1.7 Heteroresistant TB infection (section 13.2)
Heteroresistance is defined as the occurrence of drug-resistant and susceptible TB bacteria in
the same patient sample. It is detected by laboratory tests. Heteroresistance can be due to:
development of drug-resistant sub-populations through mutations in original Mtb population
presence of mixed TB infection- more than one clonally distinct Mtb strain, either through
one transmission event involving more than one distinct strain or through multiple
transmission events during a single disease episode
7
1.2 Background Rifampicin-resistant tuberculosis (RR-TB) has been declared a public health crisis by the World Health Organization (WHO). In contrast to the six-month fixed-dose combination treatment regimen offered to people with drug susceptible TB, people diagnosed with RR-TB or multi-drug resistant TB (MDR-TB) are treated with variable combinations of first and second-line anti- tuberculosis drugs, usually for 18 months or more. Numerous studies to investigate shorter, more effective and less toxic treatment regimens are ongoing in an attempt to improve outcomes in children and adults with RR/MDR-TB in South Africa. The WHO’s 2016 DR-TB treatment guidelines include recommendations on the use of a shorter regimen (9-11 months) for patients with RR/MDR-TB under specific conditions [1]. These recommendations were based on studies carried out in multiple countries, including Bangladesh, Benin, Burkina Faso, Burundi, Cameroon, Senegal and Swaziland, that showed a high rate of successful treatment outcomes in selected patients receiving a standardized shorter regimen for

On 15 August 2018 the WHO released a Rapid Communication: Key changes to treatment of
multidrug and rifampicin-resistant tuberculosis (MDR/RR-TB) [7]. This document issues new
guidance on treatment based on a meta-analysis of over 12 000 individual patient RR/MDR-TB
records, and includes changes to the categorization of medicines used to treat RR-TB.
Consolidated, updated and more detailed WHO policy guidelines on RR-TB treatment will be
provided by the end of 2018.
1.3 Current Treatment Regimens for RR/MDR-TB in South Africa
There are several treatment regimens currently being offered for RR/MDR-TB across South Africa:
Most patients with RR/MDR-TB are still receiving the old long regimen made up of KM – MFX
– ETO – TRD – Z (18-20 months duration)
Some patients with RR/MDR-TB have started the short (9-11 months) MDR-TB regimen with an
injectable agent: (4-6) KM – MFX – ETO – INHhd – CFZ – Z – E / (5) MFX – CFZ – Z – E
Some patients have received BDQ to substitute the injectable agent in cases of toxicity or
intolerance, within a short or long RR/MDR-TB regimen
Patients with pre-XDR-TB and XDR-TB currently receive long, individualized regimens
containing new and repurposed medicines.
1.4 New Short & Long Treatment Regimens for DR-TB in SA
Injectable-free regimens are being phased in routinely in South Africa. A document entitled
“Bedaquiline Expansion Plan” [8] was initially circulated to all provinces in July 2018 and this was
followed by the more comprehensive document entitled: “Interim Clinical Guidance for the
Implementation of Injectable-Free Regimens Rifampicin-Resistant Tuberculosis in Adults,
Adolescents and Children” [9] that was circulated in September 2018. In the Western Cape,
injectable-free regimens will be routinely available to treat RR/MDR-TB in adults, adolescents and
children of all ages at all DR-TB treatment sites with the implementation of these new guidelines.
A short injectable-free regimen of 9-11 months may be used for RR/MDR-TB provided specific
criteria are met. Adults and children who do not meet inclusion criteria for the short regimen will be
offered a long injectable-free regimen of 18-20 months. Some patients may initiate treatment with
a short regimen but then switch to a long regimen once further diagnostic or other relevant
information becomes available. Eligibility criteria for the short and the long regimens are listed
under relevant chapters but Annexure 1 gives an overview of eligibility criteria and various
treatment options available for patients with RR-TB. Recommendations on duration of the short
and long treatment regimens are based on WHO guidance on the short course regimen [1] and
new data presented in the Lancet on optimal duration for long treatment regimens [10].
92. Overview of the Short Regimen for RR/MDR-TB Treatment
2.1Eligibility Criteria
2.1.1 Inclusion Criteria
o Patients with Rifampicin (RIF) resistant TB (RR-TB) and no prior exposure (>1month) to
second-line anti-TB medicines- this includes
o RIF-resistant TB- diagnosis based on initial GXP result only, while awaiting further
genotypic 1st & 2nd line LPA results
o RIF- mono-resistant TB -resistant to RIF only, sensitive to INH and sensitive to
Fluoroquinolones(FLQ) & Injectables (INJ)
o Multidrug resistant TB (MDR-TB)- resistant to RIF and INH with either InhA or KatG
mutation but not both, and sensitive to FLQ & INJ
o Uncomplicated RR/MDR Extra pulmonary TB (EPTB) – i.e. lymphadenopathy, pleural
effusion, etc.(with or without PTB)
o People living with HIV: already on ART or due to start/ restart ART
o Pregnant women- if PTB / uncomplicated EPTB, eligible for short regimen, but must be
reviewed by NCAC (see sect 14)
o Children < 12 years: younger children with confirmed or presumed RR/MDR-TB are
eligible for a short regimen and should be treated without an injectable agent - discuss
with paeds DR-TB expert and send application to PCAC (see sect 14)
2.1.2 Exclusion Criteria
o Any previous exposure to second–line anti-TB medicines (i.e. treatment for RR-TB) for
more than 1 month regardless of treatment outcome
o Hb2.2 Treatment duration
A short duration of treatment of 9-11 months should be used to treat adults, adolescents and
children with newly diagnosed RR/MDR-TB if they are eligible according to specified criteria (refer
sect 2.1). The intensive phase is usually 4 months, but may be extended to 6 months if sputum
result remains smear positive at the end of month 4. The continuation phase is fixed at 5 months.
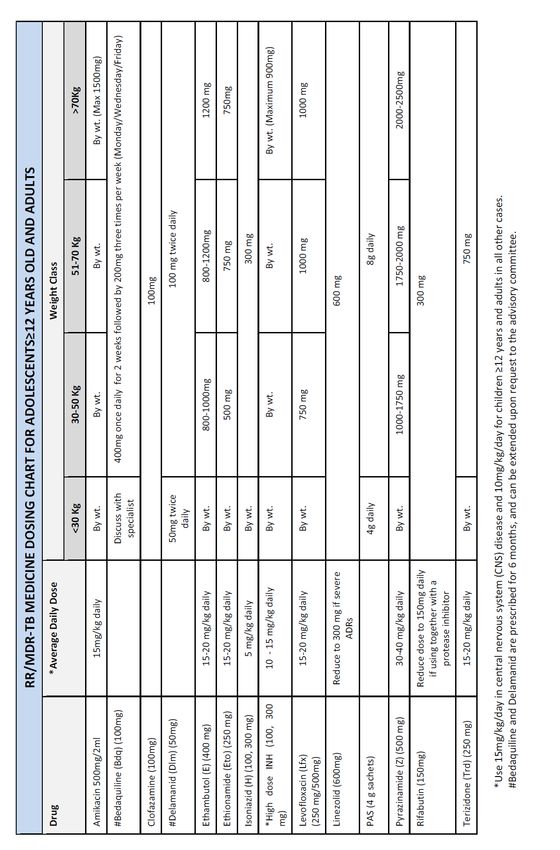
2.3 Anti-TB Medicines included in the Short Regimen
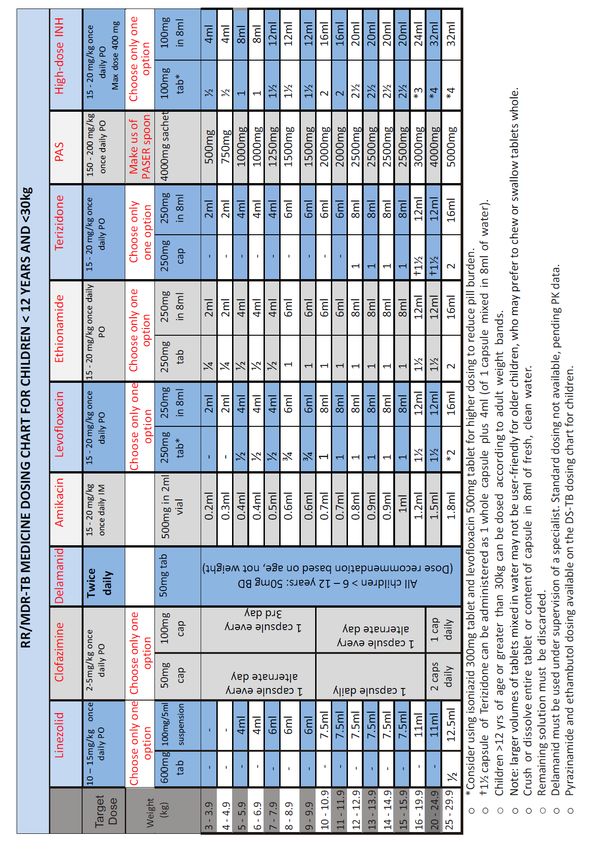
The following medicines are included (see annexure 2 & 3 for dosing):
Bedaquiline (BDQ) replaces the injectable agent in the short regimen and is given for a
minimum duration of 6 months (regardless of duration of intensive phase), unless withdrawn
early due to related toxicity or other contra-indications. Studies suggest that BDQ is superior
to the injectable in terms of safety and efficacy in treatment of RR/MDR-TB [7,10], thus a
modified short regimen including BDQ is considered more effective than the previous
injectable-containing short regimen.
Linezolid (LZD) is routinely included in the regimen up front to protect BDQ in the early
stages of treatment, particularly in cases of RR-TB where sensitivity to a quinolone has not
yet been confirmed. South Africa has a high burden of pre-XDR and XDR-TB and
inadequate regimens at the start of treatment can drive the acquisition of further drug
resistance. Linezolid will be given for the first 2 months only and will contribute to a robust
intensive phase with four core drugs (LZD, BDQ, LFX, CFZ) that are highly likely to be
effective against RR/MDR-TB at the beginning of treatment. Most cases of peripheral
neuropathy associated with LZD occur after 2 months of exposure; however,
myelosuppression tends to occur sooner so there must be close monitoring of FBC including
neutrophil count. Linezolid must be withdrawn in the event of severe haematological side
effects (Hb < 8 g/dl, neutrophils < 0.75 x109/L, platelets < 50 x109/L). Concerns regarding
toxicity must be balanced with the efficacy of LZD.
Delamanid (DLM) is the preferred replacement for the injectable children 6-12 years old (15-
30kg). DLM is not yet registered by SAHPRA, however, it is available through the Delamanid
Clinical Access Programme (DCAP) for children >6 years (as per WHO recommendations
[15] at DCAP-approved sites. This still requires application to the NCAC for use in each
individual case – if approved, DLM is given for a full 6 months. PAS may be used to
substitute the injectable in this age group if DLM is not available
Levofloxacin (LFX) replaces Moxifloxacin (MFX) to reduce the risk of QT prolongation when
used with both BDQ & CFZ
Clofazimine (CFZ) is included for the full duration of treatment and is a key medicine in the
short regimen
11 High dose Isoniazid (INHhd) is included in the short regimen for the duration of the intensive
phase, regardless of which INH mutation (inhA or katG) is detected.
Para-aminosalicylic acid (PAS) should be used to substitute the injectable in children50% and therefore ETO is likely to cause more harm than
benefit when offered routinely for treatment of RR/MDR-TB, particularly in view of the limited
efficacy of this medicine as reported in the recent IPD meta-anlaysis in the Lancet [10]. In
addition, ETO is one of the main contributors to poor adherence to treatment due to the
common side effect of severe nausea and vomiting, which may also lead to sub-optimal
absorption of other TB medicines.
Kanamycin / Amikacin / Capreomycin:
Kanamycin & Capreomycin are no longer recommended in the treatment of RR/MDR-TB
due to recent analyses indicating that use of these injectable agents was associated with
poor TB treatment outcomes [10] and severe adverse events, including reports of
ototoxicity in up to 60% of patients receiving the drug [12]. Amikacin shares a similar toxicity
profile, however it appears to be associated with slightly better treatment outcomes. It may
be considered as an option for drug substitution in the short or long regimen, and may be
the injectable agent of choice in exceptional cases where treatment options are severely
limited.
122.4 Treatment regimen for Adults & Adolescents ≥12 yrs (>30kg)
The short standardized treatment regimen is shown in box 1. There are 7 medicines in the
intensive phase and 4 medicines in the continuation phase.
Box 1: Short Treatment Regimen for RR/MDR TB for Adults, Adolescents ≥12 yrs (>30kg)
4-6 months (intensive phase):
BDQ6months-LZD2months-LFX-CFZ-Z-INHhigh-dose-E
+
5 months (continuation phase):
Continue INHhd for 2 months (extend intensive phase from 4 to 6 months) if smear
remains positive by month 4 of treatment. Dosage:10 mg/kg daily.
Duration of treatment with BDQ may be extended to 9 months :
o if smear remains positive by month 4 of treatment
o if 2nd line LPA uninterpretable or not done, and no phenotypic 2nd line DST results
available
o slow clinical response to treatment
o extensive bilateral cavitatory disease
If smear remains positive after month 4, consider possibility of treatment failure
2.5 Treatment regimens for Children2.5.1 Short Regimen for Children 6-12 years (15-30kg)
Box 2: Short Regimen for RR/MDR Treatment in Children6-12 years (15-30kg)
4-6 months (intensive phase):
LZD2months-DLM*6months- LFX- CFZ-INHhigh-dose -Z-E
+
5 months (continuation phase):
LFX-CFZ-Z-E
*Refer section 2.3
o Recommended dosing for DLM is as follows:
> 35kg: 100 mg twice daily; 20-35 kg: 50 mg twice daily; 10-20 kg: 25 mg twice daily
PAS may be used if DLM is not accessible
Use AMI or BDQ only if recommended by paediatric DR-TB expert, present to NCAC
LZD may be omitted from the short regimen, at the clinician’s discretion, in children with
non-severe RR/MDR-TB disease (i.e. no bacteriological confirmation, unilateral
pulmonary TB disease, non-cavitatory TB disease)
Dose of LZD in children >15 kg is 10mg/kg once daily
2.5.2 Short Regimen for Children3. Overview of Long Treatment Regimens for RR/MDR TB
Patients who are not eligible for the short regimen must be offered a long regimen. The
composition of the long regimen is determined by the TB resistance pattern and previous
treatment history. The WHO has recently reviewed its grouping of medicines recommended for use
in long regimens (see annexure 4) [7] . Long regimens that may be offered are:
o Long standardized regimen for RR/MDR-TB with FLQ sensitivity (without CNS disease)
o Long individualized regimen for RR/MDR-TB with FLQ resistance (without CNS disease)
o Long individualized regimen for RR/MDR-TB with CNS disease
o Long individualized regimen for RR/MDR-TB with previous exposure to new or repurposed
anti-TB medicines or treatment failure
3.1 Long standardized treatment regimen for RR/MDR-TB with FLQ sensitivity
3.1.1 Inclusion Criteria
o Previous exposure to second–line anti-TB medicines (i.e. previous treatment for RR-TB) for
more than 1 month regardless of treatment outcome. If previously exposed to new or
repurposed TB medicines ( BDQ/DLM/LZD or CFZ), request extended phenotypic DST (table
1) and consult PCAC for further advice
o Hb3.1.3 Treatment Duration
The long regimen is given for a total duration of 18-20 months. The intensive phase will usually
be 6 months but may be extended to 8 months in the following situations:
o At the clinician’s discretion in cases of slow clinical response to treatment (i.e. poor
weight gain, ongoing TB symptoms, poor resolution on CXR, delayed smear or culture
conversion)
o Bilateral pulmonary disease with extensive cavitations
o Delayed culture conversion (i.e. positive MTB cultures at month 4)
o Cases where 2nd line LPA results are indeterminate/FLQ sensitivity is not confirmed
The continuation phase is fixed at 12 months.
3.1.4 Treatment regimen for Adults & Adolescents ≥12 yrs (>30kg)
This long regimen is standardized and is based on WHO’s updated classification of anti-TB
Medicines (see annxure 4) [7]. It consists of 5 medicines in the intensive phase and 3 medicines in
the continuation phase- see box 4.
Box 4: Long Treatment Regimen for RR/MDR with FLQ sensitivity for Adults & Adolescents ≥12yrs (>30kg)
6-8 months (intensive phase):
LZD-BDQ-LFX-CFZ-TRD
+
12 months (continuation phase):
LFX-CFZ-TRD
Both BDQ and LZD are included in the intensive phase
In cases of contra-indication or toxicity to one of the five core drugs in the intensive
phase, other drugs from WHO Category C may be used for substitution (see Annexure
6). Two new drugs that are considered to be effective should be used to substitute one
of the five recommended core drugs in the long regimen.
LZD should be stopped if Hb3.1.5 Treatment regimen for Children
3.2 Long regimen for RR/MDR-TB with FLQ resistance
3.2.1 Inclusion Criteria
o Pre-XDR TB with FLQ resistance
o XDR- TB (resistance to both INJ & FLQ)
o Close contacts of patients with Pre-XDR TB with FLQ resistance or XDR- TB
3.2.2 Exclusion Criteria
o CNS disease
o history of any previous RR-TB with exposure to 2nd line anti-TB medicines including new and
repurposed medicines(BDQ, CFZ, DLM, LZD)> 1 month without a successful outcome; these
cases should be presented to NCAC.
o history of any previous RR/MDR-TB with exposure to 2nd line anti-TB medicines > 1 month with
a successful outcome, but a relapse is considered to be likely. These cases should be
presented to NCAC.
o close contact of a patient failing any RR/MDR-TB treatment
3.2.3 Treatment regimen for Adults & Adolescents ≥12 yrs (>30kg)
A treatment regimen for a FLQ resistant Pre-XDR-TB and XDR-TB should be long and individualized,
considering the patients treatment history, DST results and drug toxicity and intolerance. An
intensive phase should include a minimum of 4 medicines that are known or predicted to be
effective. This is followed by a continuation phase that includes a minimum of 3 medicines that
are known or predicted to be effective- see box 6.
Box 6: Long Treatment Regimen for RR/MDR TB with FLQ Resistance for Adults & Adolescents≥12yrs (>30kg)
6-8 months (intensive phase):
LZD-BDQ-(DLM* or PAS)-CFZ-TRD-Z-(INHhigh-dose or ETO)
+
12 months (continuation phase):
LZD-CFZ- Z-(INHhigh-dose or ETO)-TRD
* preferred if available, apply through NCAC
FLQs are not included if there is FLQ resistance on genotypic DST (LPA)
The usual dose of LZD is 600mg daily, but may be reduced to 300mg daily if toxicity occurs
INHhd or ETO usage will depend on the INH mutation present. If only InhA mutation present,
use INH 10mg/kg/day. If only KatG present, use ETO at same dose of RR/ MDR-TB regimen.
If both InhA and KatG mutations present, do not include either of the medicines
18 Do not include TRD if previously exposed to it in a failing regimen >12 months
Z is included in this regimen as it has a low rate of adverse event, however clinicians should
have a low threshold for stopping this medicine if a related adverse event occurs. If Z
resistance is demonstrated on phenotypic DST, Z should be stopped.
Rifabutin (RBT) may be included for 6 months if RIF heteroresistant TB infection is detected
(refer sect 13.2)
If one or more core drugs needs to be omitted or cannot be relied upon as susceptible,
then an alternate agent needs to be added to the regimen. This should be presented to
NCAC for review and recommendation
All patients should have intensive adherence counseling and have challenges to
adherence addressed before starting treatment. Adherence and adverse effects should
be revisited throughout treatment.
If the patient has been on treatment for RR/MDR- TB with either the short or the long regimen
for longer than one month when the diagnosis of FLQ resistance is made, consult NCAC for
a treatment regimen
3.2.4 Treatment regimen for Children3.3 Long regimen for RR/MDR-TB with CNS Disease
3.3.1 Principles of Management
RR/MDR-TB CNS disease (TB meningitis or tuberculomas) is associated with a high mortality
Clinicians should have a low threshold for performing investigations (e.g. CT brain scan or
lumbar puncture) to diagnose CNS TB disease in patients people with headaches/
neurological signs with possible immune compromise (i.e. HIV, children) and with symptoms of
CNS disease
As cerebrospinal fluid findings can be highly variable with TB meningitis and it can be
challenging to differentiate between bacterial, tuberculosis (or mixed) meningitis it is
recommended to include antibiotic cover (for example ceftriaxone 2 g IV) for 10 days or
until bacterial meningitis is ruled out. Co-infection with cryptococcal meningitis should be
ruled out with a CSF CrAg.
Steroids are given with TB medications and are tapered down over 6-8 weeks
Every effort should be made to ascertain TB drug sensitivity results for CNS disease (contact
history, sending cerebrospinal fluid for GeneXpert/LPA/culture and sensitivity as well as
taking TB diagnostic samples from other sites (sputum’s, lymph nodes etc)
Many TB drugs have poor CNS penetration. Thus, the recommended treatment is based on
the inclusion of the second line drugs with the best CNS-perfusion at optimized dosages and
is for the longer duration of treatment
In patients co-infected with HIV and not yet on antiretroviral therapy (ART): ART should be
initiated 4-6 weeks after TB treatment (to minimize the risk of life threatening intracranial IRIS)
Patients already on ART should continue ART throughout TB treatment.
203.3.2 Treatment regimen for Adults & Adolescents ≥12 yrs (>30kg) with
RR/MDR-TB CNS Disease
The recommended regimen for FLQ sensitive disease is shown in box 7.
Box 8: Long Individualized Treatment Regimen for FLQ sensitive RR/MDR CNS Disease in Adults &
Adolescents≥12yrs (>30kg)
6-8 months (intensive phase):
LZD-BDQ-LFX-CFZ-TRD-Z-(INHhigh-dose* or ETO)
PLUS: Dexamethasone 12 mg IVI (0.4mg/ kg/ day) bi-daily 12 hourly followed
by Prednisone 120mg per oral daily.
After 1 week gradually taper dose over 6-8 weeks
+
12 months (continuation phase):
LFX-CFZ-TRD-Z-(INHhigh-dose* or ETO)
*INH dose 15mg/kg/day
Addition of DLM can be considered (good CNS perfusion in rat models) where available
Change from intensive phase to continuation phase is based on clinical response
If LZD is well tolerated and ongoing close monitoring (for haematological, optic and peripheral
neuropathy) is possible, LZD can be extended into the continuation phase
Repeat CT brain scan may be used to monitor response of tuberculomas to treatment.
Residual lesions may be present at end of treatment and do not necessarily represent
treatment failure
All patients with presumed or confirmed FLQ resistant CNS TB must be presented to NCAC for
expert advice, as there is a very high risk of mortality. In addition to the regimen shown in box 7,
DLM should be included, and an intravenous carbepenem may be recommended.
3.3.3 Treatment regimen for Children3.4 Other long individualized regimens for RR/MDR-TB
An individualized long regimen should be used in the following scenarios:
o history of any previous RR/MDR-TB with exposure to 2nd line anti-TB medicines including
new and repurposed medicines (BDQ, CFZ, DLM, LZD)> 1 month without a successful
outcome
o history of any previous RR/MDR-TB with exposure to 2nd line anti-TB medicines > 1 month
with a successful outcome, but a relapse is considered to be likely
o close contact of a patient failing any RR/MDR-TB treatment
An individualized long regimen is constructed according to the previous RR/MDR-TB history and
exposure to 2nd line anti-TB medicines. Send sputum sample for individualized extended
phenotypic DST (see table 1).
Consult PCAC or NCAC for advice before initiating treatment (refer sect 15).
224. Clinical Guidelines for Initiation of the Short or Long regimen
4.1 Sputum Collection for diagnosis
For all patients who have one or more signs or symptoms of TB, collect two sputum
specimens at least one hour apart
The first sputum specimen will be used for GXP testing
If Rifampicin resistance is detected on GXP, the second sputum specimen will be used
for smear microscopy, 1st line & 2nd line LPA and TB culture
Record the above results as “baseline” results
It is no longer necessary to routinely collect a 3rd sputum specimen (previously referred
to as baseline sputum) before initiating treatment
However, an additional sputum specimen must be submitted if the initial sample is
inadequate or has leaked, results are inconclusive, or if requested by the lab
4.2 Laboratory-based Drug Sensitivity Tests (DSTs)
Choice of regimen and duration of treatment is guided by the results of laboratory-
based genotypic & phenotypic DSTs (see table 1)
1st and 2nd genotypic test (LPA) will be conducted routinely on all specimens with GXP
positive RIF resistant results.
1st and 2nd line LPA’s will be repeated on culture isolates if initial results are inconclusive
Phenotypic DST for INH will be routinely performed on culture isolates if 1 st line LPA
indicates INH sensitivity- this will detect phenotypic resistance to INH that may not be
identified on targeted genotypic testing, which has a sensitivity of 86% ( meaning that
about 14% are actually phenotypically resistant) [12]. Phenotypic DST results will not
provide information about the associated mutation if INH resistance is detected.
2nd line phenotypic DST will be done routinely if there is FLQ sensitivity on 2nd line LPA
Extended 2nd line phenotypic DST detects resistance to Bedaquiline, Clofazimine,
Levofloxacin, Linezolid, and Moxifloxacin. This test will routinely be conducted on culture
isolates if resistance to FLQ is detected by routine 2nd line LPA. This is a reflex test and it is
not necessary to send additional specimens. These Pre-XDR and XDR cases are not
eligible for the shorter regimen and should receive individualized longer regimens. The
purpose of carrying out this extended phenotypic DST is to provide the clinician with a
greater repertoire of drugs that MAY be effective in treating Pre-XDR (FLQ) and XDR
cases (the results will be available after a minimum of 14 days)
Repeat LPAs and extended 2nd line phenotypic DST must be requested for patients with
a smear positive result at month 4. Contact the lab to request test on previous culture
positive specimen and follow up for results.
23Table 1: Laboratory-based Drug Sensitivity Tests (DSTs)
Type of test When done Result
GXP pos/RIF resistant Susceptibility to
st
1 line LPA GXPneg/HIVpos if Rif & INH, and INH
culture positive mutation(s)
Genotypic GXP pos/RIF resistant
nd GXPneg/HIVpos & Susceptibility to
2 line LPA
LPA Rif resistant FLQ & INJ
on culture isolate
In-lab reflex when RIF
To confirm
resistant but
Phenotypic INH susceptibility to
susceptible to INH on
st INH- no mutation
1 line LPA
In-lab reflex test for all
Susceptibility to
2nd line LPA results
Phenotypic FLQ LFX/MFX 0.25
that indicate FLQ
ug/ml
susceptibility
In-lab reflex test when
resistance to FLQ or
INJ detected on
nd
2 line LPA
Susceptibility to
Requested by
LFX/LZD/
clinician if 2nd line LPA
MFX 0.25 & 1.0
2nd line Phenotypic DST is susceptible but
ug/ml
nd
resistance to 2 line (to include BDQ &
TB medicines is CFZ in 2019)
suspected (eg due to
previous unsuccessful
RR-TB treatment, or
XDR contact)
Requested by Susceptibility to
clinician when RR-TB multiple 2nd line TB
Individualized
treatment fails, and medicines; results
Extended Phenotypic DST
patient had been will be used to
(from NICD)
previously exposed to construct a
nd
2 line medicines salvage regimen
244.3 Baseline Assessment
Obtain full medical history and assess clinical condition of the patient
Enquire about HIV status and any previous ART exposure
Enquire about close RR/MDR-TB contacts
Screen for non-communicable diseases (hypertension, diabetes mellitus, mental health)
Screen for substance use using available validated screening tool
Enquire about history of cardiac disease and cardiac symptoms (chest pain, palpitations,
dizziness, syncope)
Screen for contraindications to use of BDQ (see annexure 5) and other 2nd line TB medicines
Consult Provincial Clinical Advisory Committee (PCAC) if BDQ contraindicated, or if
significant cardiac history or symptoms present
Pregnant women with newly diagnosed RR/MDR-TB are eligible for treatment with the short
DR-TB regimen- an application should be submitted to the (NCAC), but this should not
delay initiation of treatment in patients with uncomplicated first episode of DR-TB
Breastfeeding women are also eligible for treatment with the BDQ-containing short or long
regimens. The benefits of breastfeeding must be weighed against the risks of transmission of
TB to the baby. Manage risk of transmission with appropriate infection control measures.
Always consult a paeds DR-TB expert before initiating treatment for RR/MDR-TB for
children1000 in previous 3 months)
If CD44.5 Initiation of Treatment
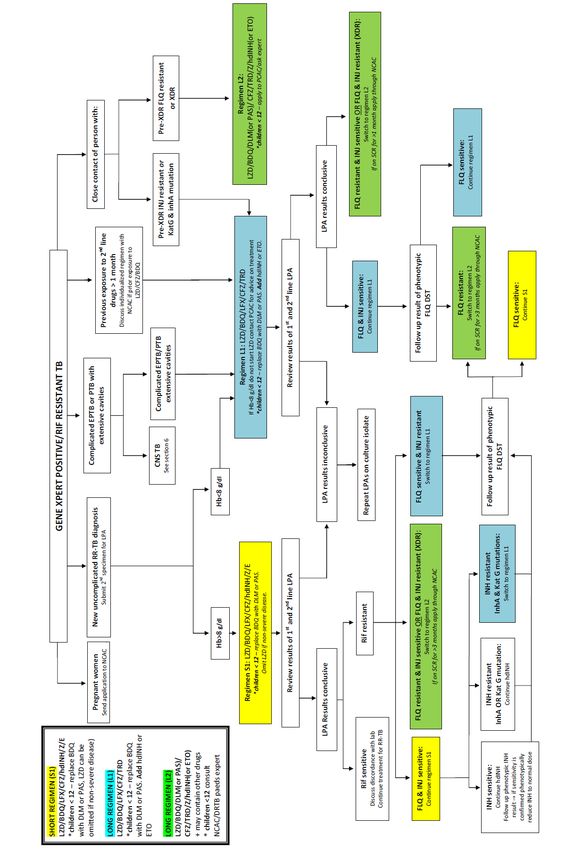
If GXP Pos + Rif resistant, consider history and assess eligibility for short or long regimen
Review results of baseline investigations
Review ECG result: baseline QTcF must be 450ms, address any contributing causes: stop any concomitant QT-
prolonging medicines, correct electrolytes, treat abnormal TSH. Repeat ECG – if QTcF still
>450ms, consult PCAC for advice on regimen (sect 15).
Initiate treatment according to algorithm shown in Annexure 1
Follow up for 1st and 2nd line LPA results after 7-14 days and confirm eligibility for the short or
long regimen with patient if results are conclusive
If on short regimen, amend treatment regimen as shown in table 2
If on long regimen, or if switching from short to long regimen, amend treatment regimen as
discussed in sect 3
Table 2: Amending treatment on short regimen with 1st & 2nd line LPA results
st
1 line LPA Result Action
RIF Susceptible continue DR-TB regimen, discuss discordance with lab
RIF Resistant continue DR-TB regimen with INHhd,
modify according to other LPA results
InhA mutation only continue DR-TB regimen with INHhd
KatG mutation only continue DR-TB regimen withINHhd
Both InhA & KatG switch to long regimen
mutations (patient is no longer eligible for the short regimen)
Susceptible to INH continue DR-TB regimen with INHhd and wait for INH
phenotypic DST result
o if confirmed susceptible to INH, decrease INH to
normal dose
o if resistant to INH, continue with INHhd
2
nd
line LPA Result Action
Susceptible to FLQ continue with DR-TB regimen with 2 months LZD.
Follow up results of phenotypic DST for LFX/MFX 0.25 ug/ml
Resistant to FLQ Switch to longer individualised DR-TB regimen
Follow up results of phenotypic DST for LFX/MFX 0.25, MFX 1.0,
LZD (BDQ and CFZ in 2019)
265. Management of RR/MDR-TB Patients Co-infected with HIV
5.1 Key principles
Patients with HIV and RR/MDR TB are considered to have advanced ( stage 4) HIV disease
and are at high risk of mortality, especially if not on ART [16,17]
Patients with HIV are more at risk of poor outcomes due to:
o immunocompromised status & risk of IRIS
o high pill burden & risk of drug-drug interactions & toxicities
o co-morbid opportunistic infections
Aggressively diagnose and manage co-morbid opportunistic infections
In adults with CD4 < 100, review CrAg test result before initiation of ART. If symptomatic, refer to
hospital for lumbar puncture and IV anti-fungal treatment, which will be followed by oral anti-
fungal therapy with Fluconazole ≥ 1 year (discontinue when CD4 > 200 taken 6 months
apart). Monitor for QTcF prolongation with concomitant use of BDQ and fluconazole.
Bactrim prophylaxis reduces mortality and (unless contraindicated or hypersensitivity
present)should be given with TB treatment regardless of CD4 count [17]. Bactrim can be
used with LZD; regular FBC and neutrophils count monitor for bone marrow suppression
Initiate ART within 2 weeks of starting RR/MDR-TB for patients not on ART (except if CNS
disease present), and optimize treatment for those already on ART
Treatment with the short or long regimen is the same for all patients regardless of HIV status.
However, choice of ART regimens may need to be modified according to the medicines in
the short or long regimen
5.2 Initiation of ART in ART-naïve patients
Timing of ART Initiation:
o initiate ART within 2 weeks of starting treatment [18]
o If TBM or CM, initiate ART 4-6 weeks after starting TB medication due to risk of
intracranial IRIS [19]
Choice of ART regimen:
o Efavirenz (EFV)cannot be used concurrently with BDQ, therefore:
If female & CD45.3 Re-starting ART in patients previously on ART, but currently not on ART
o If previously on 1st line ART, initiate a 2nd line PI-based regimen
o If previously on 2nd line ART, address reasons for treatment interruption and restart same
regimen. If GI side effects experienced with LPV/r and TB meds, consider switch to ATV/r.
Repeat VL after 3 months
5.4 Management of patients currently on ART
o Review recent VL (baseline or within last 3 months)- see table 3
o If VL6. Monitoring of Patients on Short & Long RR-TB Regimens
6.1 Clinical & sputum monitoring
Medical officer must review patient at 2 weeks, 4 weeks, 8 weeks and then monthly
(annexure 6)
Follow up for outstanding DST results and modify regimens accordingly
Monitor clinically for side effects including cardiac symptoms(chest pain, palpitations,
dizziness, syncope), gastrointestinal symptoms (nausea, vomiting, diarrhea),
hepatotoxicity (nausea, fatigue, jaundice), anaemia, optic neuropathy and peripheral
neuropathy
Monitor for side effect of optic neuritis monthly on LZD using Snellen chart (annexure 9)
and Ishihara chart (annexure 10). Stop LZD and refer to ophthalmologist if changes
detected.
Monitor clinically for side effect of uveitis monthly on RBT- visual disturbances, painful
inflamed eye, photophobia. Stop RBT and refer to ophthalmologist if symptoms
detected.
Routine sputum collection monthly for smear & culture
Optimize management of concurrent non-communicable diseases
Repeat audiometric assessment monthly if on injectable agent- stop injectable and refer
for further audiological management if ototoxicity detected
Repeat audiometric assessment 3 monthly even if not on injectable agent-refer for
further audiological management if hearing deficits detected.
Refer to annexure 5 for schedule of clinical review &management in short regimen
6.2 Monitoring of Bloods
• Standard monitoring blood tests according to DR-TB guidelines (annexure 7)
o Check FBC & diff (Hb & neutrophil count)) at 2 weeks, 4 weeks, 8 weeks and then
monthly if using LZD
o Check ALT monthly if using RBT or more frequently if hepatic disease is suspected.
6.3 Monitoring of ECG
Monitor QTcF on ECG monthly until course of BDQ completed or until QTcF 470ms at the end of 6 months of BDQ
Manage according to Table 4
29Table 4: Monitoring QTcF on ECG when using BDQ
QTcF on ECG at baseline Action
Start BDQ and repeat ECG after 2 weeks
(If QTcF>450ms, address any contributing causes7. Switching from Intensive Phase to Continuation Phase
7.1 Switching treatment phases in Short Regimen
The duration of the intensive phase of treatment is dependent on the clinical condition
and timing of smear conversion (annexure 2)
Medical officer must assess clinical condition and smear & culture results of patient at
month 4 to decide if intensive phase should change to continuation phase at this stage, or
if intensive phase should be prolonged for another 2 months (note that it is likely that the
month 3 and month 4 culture results will not be available at that point, and therefore the
decision is based on the clinical condition of patient and monthly smear results)
Switch to continuation phase when the following apply:
o Patient who started treatment being smear positive: If smear negative at the end of
month 4 and patient is clinically improving
o Patient who started treatment being smear negative: if TB smear remains smear
negative up until month 4 of treatment and patient is clinically improving
If patient has not shown signs of clinical improvement, or is deteriorating after initial clinical
improvement, discuss with PCAC regardless of smear results
If the month 4 smear is still positive (has not changed from being positive at baseline),
suspect potential treatment failure. Assess adherence, substance use, co-morbidities and
side effects. Review monthly culture results, and request reflex DST on the latest positive
culture. Prolong the intensive phase to 6 months, and consult PCAC as it will be necessary
to extend course of BDQ. At 6 months, review monthly culture results. Switch to
continuation phase only if culture conversion has occurred by month 4. If culture
conversion does not occur by month 4, consult NCAC for advice on longer individualized
regimen.
If the 4 month sputum has become smear positive after initially being negative at baseline,
or reverted to being smear positive after becoming negative, assess adherence, optimize
management of co-morbidities and request LPA and phenotypic DST on latest sputum
sample. As this is a higher risk of treatment failure, present case to PCAC as soon as
possible
317.2 Switching treatment phases in Long Regimens
Medical officer must assess clinical condition and culture results of patient at month 6 to
decide if intensive phase should change to continuation phase at this stage, or if intensive
phase should be prolonged for another 2 months
If patient has not shown signs of clinical improvement by 2 months, or is deteriorating after
initial clinical improvement, discuss with PCAC regardless of smear or culture results
Switch to continuation phase when the following apply:
o For patient who started treatment being culture positive: culture negative result for
sputum sent at the end of month 4 and patient is clinically improving
o For patient who started treatment being culture negative or indeterminate: all culture
results remain negative including that of sputum sent at the end of month 4 and patient
is clinically improving
If intensive phase is prolonged to 8 months, duration of treatment with BDQ should also be
extended to 8 months- submit application to PCAC
If culture conversion does not occur during extended intensive phase, assess adherence,
substance use, co-morbidities and side effects, and prepare to present to NCAC as
treatment failure
8. Discordance or lack of GXP confirmation
In situations where RR-TB is detected on GXP only and resistance pattern is not confirmed on
LPA or DST (e.g. sample contaminated, sample leaks or results are indeterminate), every
effort should be made to collect another sample as early as possible to obtain confirmation
of drug resistance patterns. Include both BDQ & LZD in the intensive phase.
These patients may have started the short or long regimen, according to clinical history
If patient is on the short regimen, and sensitivity to FLQ & INJ is not confirmed on LPA or DST,
but all other eligibility criteria are met(e.g. patient is not a close contact of XDR, etc.), then
they may still continue with the short regimen
If discordant results are obtained, repeat sputum culture as soon as the discordance is
observed; continue with RR-TB treatment regimen and contact the lab and DR-TB expert or
PCAC to discuss regimen and duration of treatment.
329. Medicine substitution for Patients on Short or Long Regimens
Patients who are currently on a short or long Kanamycin (Km)-containing regimen, are
eligible for medicine substitution with BDQ- consult PCAC
BDQ must be given for a minimum duration of 6 months regardless of when it is started in
the intensive phase
Repeat audiometric assessments at 3 and 6 months after stopping the injectable agent
Patients who develop intolerance or toxicity to any of the core medicines (BDQ-LFX-ETO-
CFZ-INH) in the short regimen, are eligible for substitution with DLM, TRD, PAS and / or LZD.
However, they will have to be switched to a long individualized regimen.
Patients who develop intolerance or toxicity to any of the medicines in a long regimen
are also eligible for substitution- options may include DLM, PAS, ETO, Amikacin and/or an
Imipenem etc.
Applications for medicine substitution in short or long regimens must be submitted to
PCAC (refer sect 15)
10. Reporting of Adverse Drug Reactions
An adverse drug reaction is one type of adverse event, defined as any untoward medical
occurrence that may present during treatment with a pharmaceutical product, but which
does not necessarily have a causal relationship with this treatment
Reporting of serious ADRs provides important information that enables improvement in
the quality of patient care
ADRs may be graded according to the severity of the symptoms (see annexure11)
Medical officers, nurses or pharmacists must report at least grade 3-5 ADRs to the MIC
(see annexure 12), SAHPRA via NDOH APP or via Sinjani
11. Patient education/ Counselling
Counselling of patients with regard to DR-TB treatment should be modified to include
new information about the short regimen, and continue as per current protocols
Patients should be counselled at baseline about their eligibility for the standard short
regimen treatment which is for 9-11 months and this should be confirmed with them
once the results of their LPA’s and/ or DST are available.
All patients should be counseled on the clinical monitoring requirements including
monthly ECGs while on BDQ or DLM, as well as key symptoms to report urgently (i.e.
cardiac symptoms, visual problems, peripheral neuropathy or extreme lethargy)
33 The clinician’s responsibility
o Detailed focused history which should include:
Previous exposure to anti-TB medicines
Co-morbidities including cardiovascular diseases
Family history of cardiac diseases or sudden death
Close contacts on TB treatment or with symptoms suggestive of TB
Other medication usage including ART & contraception
Screening for substance use
Screening for depression & other mental illness
o Discuss frequency and type of investigations to be done:
Baseline & monitoring bloods
Audiology test
Pregnancy test
Monthly ECGs
o Discuss potential side effects / adverse drug reactions – with strong focus on
symptoms to report urgently
o Discuss infection control practices and cough hygiene
Identify & screen close contacts
Counsellor/ TB nurse responsibility
o Provide counseling on:
HIV support and ART
Disease course and treatment journey
Adherence support and enabling tools such as schedules
Infection control practices
Contact tracing
Addressing substance abuse and mental illness
12. Post- Treatment Monitoring for TB Relapse
It is of utmost importance that patients completing the short DR-TB regimen be monitored
for subsequent relapse of TB disease
Give patients appointments for clinical assessments at 6 monthly intervals for 1 year after
successful completion of treatment
The assessment must include review of clinical condition, CXR and collection of sputum
sample for smear & culture.
3413. Management of Other Forms of DR-TB
13.1 RIF Susceptible INH Monoresistant TB
The conventional management of RIF-susceptible TB with 2 months of rifampicin, isoniazid,
pyrazinamide and ethambutol followed by 4 months of rifampicin and isoniazid (2RHZE/4HR) is
more likely to fail in patients who have INH monoresistance compared to those who are INH
susceptible [1, 22]. Therefore, WHO now recommends the addition of Levofloxacin(LFX) for this
group of patients, provided Rifampicin resistance has been excluded (annexure13).
According to the South African Tuberculosis Drug Resistance Survey 2012-2014, the prevalence of
INH monoresistance among TB patients in the Western Cape is 10.8% (CI 8.5-13.7) [23]. Genotypic
DST (1st line LPA) is currently not routinely performed for patients with RIF-susceptible TB(by Xpert),
instead it must be requested for patients who are not improving clinically or who still have smear
positive sputum results at 7 weeks or at any time thereafter. If INH resistance is detected and RIF
resistance has been excluded with 1st line LPA, the new recommendation is to continue RHZE for a
further 6 months with the addition of LFX (see dosing charts- annexure 2 & 3). If only an InhA
mutation is detected (ie. no KatG mutation), a higher dose of INH may be beneficial [24]. The
dose of INH may be augmented to total 10mg/kg/day. The decision to treat with INHhd should be
individualized: consider benefits versus risk of toxicity and increased medicine burden. Consult
PCAC if unsure.
The treatment duration with addition of LFX (with or without INHhd) may be extended beyond 6
months if INH resistance is detected later than 2 months in the course of treatment, or in patients
with extensive disease [22] - discuss with PCAC. Monthly monitoring of sputum smear and culture
results should be performed until treatment is completed. All RIF susceptible INH monoresistant TB
patients should be recorded in the DR TB register and captured in the EDRWeb.
13.2 RIF Heteroresistant TB
Studies show that a significant proportion of RR-TB isolates may still have in-vitro susceptibility to
Rifabutin [25]. Furthermore, treatment outcomes in patients with Rifabutin- susceptible RR-TB can be
improved with the addition of Rifabutin. Therefore, Rifabutin should be added to treatment regimens
for adolescents>12 years and adults where RIF heteroresistant infection is detected by genotypic DST,
for a total of 6 months. Monitor monthly for side effects of neutropaenia, uveitis (visual disturbances,
painful inflamed eye, photophobia) and hepatitis (see annexure 6). Dosing (annexure 2) must be
adjusted when using ART containing protease inhibitors. Submit application to PCAC before adding
Rifabutin to regimen.
3514. Recording and reporting
Recording and reporting will continue as per norm. Stationery has been revised to include
the short and long regimens
Folders, registers and drug prescription charts should be marked to differentiate between
the short and long regimen:
- Green sticker to indicate the short regimen
- Orange sticker to indicate the long regimen
Data will be captured on the EDRWeb
The Medical Officers are responsible for assigning DR-TB outcomes once a patient has
completed treatment (annexures 15 & 16)
15. Role of DR-TB Provincial & National Clinical Advisory Sub-Committees
(PCAC/NCAC) & Provincial DR-TB Review Committee
The Provincial DR-TB Clinical Advisory Committee (PCAC) provides clinical governance and
support for clinicians managing DR-TB patients in the Western Cape. It is no longer
necessary to submit applications for all DR-TB patients initiating BDQ in the shorter regimen.
However, applications should still be submitted for the following:
o New episode of Pre-XDR or XDR TB
o Patient unable to tolerate LZD: Hb The National DR-TB Clinical Advisory Committee (NCAC) provides inputs for
development of national DR-TB policies and guidelines and provides clinical
governance and support for clinicians managing DR-TB patients nationally. Applications
should be submitted for:
o Patients with contraindications to BDQ or other 2nd line TB medicines, or significant
cardiac disease or symptoms
o All pregnant patients initiating RR-TB treatment
o Exposure to standard short RR/MDR TB regimen>1 month before FLQ and/or INJ
resistance detected
o Patients failing treatment on pre-XDR/XDR-TB regimen
o Unable to construct a regimen with at least two of the following four medicines:
BDQ, LZD, FLQ (MFX or LFX), AMI
o Patients who interrupted treatment >2 months on regimens containing BDQ, DLM,
CFZ or LZD and present for restart of treatment
o Patient previously treated for any RR- TB with a successful outcome but present
with a new episode of RR-TB that may be a relapse of previous disease
o Requests for treatment with DLM or extension of DLM treatment beyond 6 months
via the Delamanid Clinical Access Programme (DCAP)
Submission to PCAC or NCAC must be made using the form contained in annexure 17.
This form must emailed to:
PCAC: Vanessa.mudaly@westerncape.gov.za
NCAC : ncac@witshealth.co.za
(Please add patient folder number and reason for application/nature of query in
subject line, and cc the treating clinician if possible)
The Provincial DR-TB Review Committee is a multi-disciplinary team that reviews
management of patients in whom DR-TB treatment is failing despite optimization of
treatment options. Patients who have multiple episodes of treatment interruption, or are
estimated to be taking16. References
1. World Health Organization. WHO treatment guidelines for drug-resistant tuberculosis 2016 update.
World Health Organization; 2016.
2. World Health Organization. Global Tuberculosis Report. Geneva : 2018
3. Ndjeka N et al. Treatment of drug-resistant tuberculosis with bedaquiline in a high HIV prevalence
setting: an interim cohort analysis. The International Journal of Tuberculosis and Lung Disease. 2015;
19:979-85. doi :10.5588/ijtld.14.0944
4. Directorate Drug-Resistant TB, TB & HIV. Introduction of new drugs, drug regimens and
management for drug-resistant TB in South Africa: Policy framework. 1.1. Pretoria: National
Department of Health; 2015.
5. Zhao et al. Improved treatment outcomes with bedaquiline when substituted for second-line
injectable agents in multi-drug resistant tuberculosis: a retrospective cohort study. Clinical Infectious
Diseases, ciy 727, http://doi.org/10.1093/cid/ciy727. Published 24 August 2018.
6. Schnippel Ket al. Effect of bedaquiline on mortality in South African patients with drug-resistant
tuberculosis: a retrospective cohort study. Lancet Respir Med 2018; 2600:1-8. doi : 10.1016/S2213-
2600(18)30235-2.
7. World Health Organization. Rapid communication: key changes to treatment of multidrug and
rifampicin-resistant tuberculosis (MDR/RR-TB). World Health Organization; August 2018.
8. Directorate Drug-Resistant TB, TB & HIV. Bedaquiline Expansion Plan. June 2018
9. Interim Clinical Guidance for the implementation of injectable-free regimens for Rifampicin-
resistant tuberculosis in adults, adolescents and children. National Department of Health ; 2018
10. The Collaborative Group for the Meta-analysis of Individual patient Data in MDR-TB treatment
2017; Ahmed N et al. Treatment correlates of successful outcomes in pulmonary multidrug-reistant
tuberculosis; an individual patient data meta-analysis. Lancet2018; 392:821-34.
11. Ismail N et al. Prevalence of drug-resistant tuberculosis and imputed burden in South Africa: a
national and sub-national cross-sectional survey. Lancet Infect Dis 2018. Published online 20 April
2018.
12. Seddon J A et al. Hearing loss in patients on treatment for drug-resistant tuberculosis. Eur Respir J
2012; 40: 1277–1286.
13. Zignol M et al. Genetic sequencing for surveillance of drug resistance in tuberculosis in hihly
endemic countries: a multi-country population-based study. Lancet Infect Dis. 2018. Pii:S1473-
3099(18)30072-2. doi :10.1016/S1473-3099(18)30072-2.
14. Sentinel Project. Statement on Injectable Free Regimens for Children under the Age of 12 Years
with Rifampicin-Resistant Tuberculosis. Available at http://sentinel-project.org/wp-
content/uploads/2018/07/Recommendations-for-Injectible-Free-Regimens-in-Children-with-Rif-
Resistant-TB.pdf.
3815. World Health Organization. The use of delamanid in the treatment of multidrug-resitant
tuberculosis in children and adolescents: Interim policy guidance 2016.
16. Gandhi NR et al. Risk factors for mortality among MDR-and XDR-TB patients in a high HIV
prevalence setting. The International Journal of Tuberculosis and Lung Disease. 2012 Jan 1;16(1):90-7.
17. Schnippel K C et al. Persistently high early mortality despite rapid diagnostics for drug-resistant
tuberculosis cases in South Africa. Int J Tuberc Lung Dis. 2017;21(10):1106
18. World Health Organization. Guidelines for managing advanced HIV disease and rapid initiation of
antiretroviral therapy, July 2017.
19. Torok ME et al. Timing of initiation of antiretroviral therapy in Human immunodeficiency virus (HIV)
associated tuberculous meningitis. Clin Infect Dis. 2011;52:1374–1383.
20. Paton NI et al. Assessment of second-line antiretroviral regimens for HIV therapy in Africa. New
England Journal of Medicine 2014. 371(3):234-47.
21. World Health Organization. WHO Treatment Guidelines for Isoniazid-resistant tuberculosis.
Supplement to the WHO Treatment Guidelines for drug-resistant Tuberculosis. 2017.
22. Compendium of WHO guidelines and associated standards: ensuring optimum delivery of the
cascade of care for patients with tuberculosis. Version 1. November 2017.
23. National institute for communicable Diseases- Division of the National Health Laboratory Service.
South African Tuberculosis Drug Resistance Survey 2012–14 http://www.nicd.ac.za/assets/files/K-
12750%20NICD%20National%20Survey%20Report_Dev_V11-LR.pdf
24. World Health Organization . Frequently asked questions on the WHO treatment guideline for
isoniazid- resistant tuberculosis. 24 April 2018.
25. Lee et al. Treatment outcomes of rifabutin-containing regimens for rifabutin-sensitve multidrug-
resistant pulmonary tuberculosis. Int J Inf Dis. 65 (2017) 135-141.
-
39You can also read