Consultation on proposed amendments to the list of controlled drugs that podiatrists can independently prescribe across the United Kingdom ...
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
OFFICIAL Publications approval reference: PAR145 Consultation on proposed amendments to the list of controlled drugs that podiatrists can independently prescribe across the United Kingdom October 2020
OFFICIAL
This information can be made available in alternative
formats, such as easy read or large print, and may be
available in alternative languages, upon request.
Please email england.cpomedicinesmech@nhs.net.
A patient and public summary version of this
consultation guide is also available.
Equality and Health Inequalities Statement
Promoting equality and addressing health inequalities are at the heart of NHS England and
NHS Improvement’s values. Throughout the development of the policies and processes
cited in this document, we have:
• Given due regard to the need to eliminate discrimination, harassment and
victimisation, to advance equality of opportunity, and to foster good relations
between people who share a relevant protected characteristic (as cited under the
Equality Act 2010) and those who do not share it; and
• Given regard to the need to reduce inequalities between patients in access to, and
outcomes from healthcare services and to ensure services are provided in an
integrated way where this might reduce health inequalities
2OFFICIAL
Contents
What are we consulting on? ................................................................................ 4
Why are the proposed changes being considered? ............................................ 4
Who has been involved? ..................................................................................... 5
Supporting documents ........................................................................................ 5
The questions being asked ................................................................................. 6
Context................................................................................................................ 8
Programme of work ............................................................................................. 8
The role of the podiatrist ................................................................................... 10
The professional bodies .................................................................................... 11
Professional regulation ...................................................................................... 11
How podiatrist independent prescribers are trained .......................................... 12
Continuing professional development (CPD) .................................................... 13
Identification of viable options ........................................................................... 14
Limitations of the current use of medicines mechanisms by podiatrists ............ 16
Rationale for the selection of the additional controlled drugs ............................ 18
Benefits of the proposal .................................................................................... 20
Use in clinical practice ....................................................................................... 23
Management of potential risks associated with the proposal ............................ 25
Education that all non-medical prescribers receive on controlled drugs............ 27
Engagement with Controlled Drugs Accountable Officer (CDAO) ..................... 29
Personal formularies ......................................................................................... 30
Communication of decisions to prescribe controlled drugs ............................... 30
Prescribing controlled drugs in private practice ................................................. 31
Public sector equality duty ................................................................................ 33
Health inequality duties ..................................................................................... 34
Who can respond to this consultation? ............................................................. 35
How to respond ................................................................................................. 35
Alternative formats ............................................................................................ 35
Engagement events .......................................................................................... 36
How your responses will be used ...................................................................... 36
Next steps ......................................................................................................... 36
Appendix A: Scheduling of controlled drugs ...................................................... 38
Appendix B: Contributors .................................................................................. 39
Appendix C: Role of the professional bodies .................................................... 41
Appendix D: Entry criteria for prescribing education programmes .................... 42
Appendix E: Frequently asked questions. ......................................................... 43
3OFFICIAL
Introduction to the consultation
What are we consulting on?
This consultation is on proposals to enable podiatrists to prescribe four additional controlled
drugs.
Podiatrists have been able to train as independent prescribers since 2013 and have been
able to prescribe from a restricted list of four controlled drugs since 2015 in England
Scotland and Wales. Since November 2019, legislative changes permit prescribing of the
same controlled drugs in Northern Ireland. Further legislative amendments are being
progressed to support prescribing in primary care. Controlled drugs are medicines that have
additional controls associated with the prescribing, storage or record keeping because they
can be misused for non-treatment purposes. The medicines are listed in five schedules or
groups and each has different levels of control (see appendix A).
This UK-wide consultation is being led by NHS England and NHS Improvement on behalf of
the four nations and relates to the proposal to enable podiatrist independent prescribers to
prescribe four additional controlled drugs in the course of their professional practice,
namely:
morphine sulfate schedule 2 and 5 oral administration
tramadol hydrochloride schedule 3 oral administration
pregabalin schedule 3 oral administration
gabapentin schedule 3 oral administration
There are two options for consideration in this consultation:
Option 1: no change
Option 2: addition of four controlled drugs to the existing list of controlled drugs that
podiatrist independent prescribers can currently prescribe
The proposed changes require amendment to both the Human Medicines Regulations 2012
and the Misuse of Drugs Regulations 2001. The Human Medicines Regulations apply UK-
wide so subject to the agreement of Ministers, changes to them will apply across the four
countries. The Misuse of Drugs Regulations apply only to England, Wales and Scotland;
the Misuse of Drugs (Northern Ireland) Regulations 2002 will need to be amended
separately and this will be undertaken by the Department of Health in Northern Ireland.
Should legislation be amended, the changes would apply throughout the UK, in any setting
in which podiatrists work including the NHS, independent and voluntary sectors.
The consultation will run for 8 weeks and will close on 10th December 2020.
A glossary of terms used in this guide can be found in section 9.
Why are the proposed changes being considered?
4OFFICIAL
The proposed addition of four controlled drugs to the current list of controlled drugs that
podiatrist independent prescribers can already prescribe would:
• improve patient outcomes through timely access to appropriate pain relief as part of
their podiatric intervention
• reduce the need for patients to have additional appointments with other health
professionals to access medicines required
• provide patients with the right treatment and at the right time
• ensure that patients being treated by podiatrist independent prescribers receive
evidence-based pain management in line with the World Health Organisation (WHO)
analgesic ladder
Further information on the benefits of this proposal is presented in section 4.4. Potential
risks and measures in place to manage the risks can be found in section 4.6.
Who has been involved?
This consultation guide has been developed in partnership with Department of Health and
Social Care; the Medicines and Healthcare products Regulatory Agency; the Northern
Ireland Department of Health, the Scottish Department of Health and Social Care and the
Welsh Department of Health and Social Services.
The College of Podiatry and the Institute of Chiropodists and Podiatrists, the professional
bodies that represent podiatrists in the UK have also collaborated in the development of this
consultation guide and the supporting documents that accompany it.
Supporting documents
The following supporting documents are provided alongside this consultation to inform
consideration of the options and questions:
• Practice guidance entitled Good Practice in Prescribing and Medicines Management
for Podiatrists1
• Outline Curriculum Framework for Education Programmes to Prepare Podiatrists as
Independent/Supplementary Prescribers2
• Consultation Stage Impact Assessment.
Practice guidance
The practice guidance was first published in 2011 by the College of Podiatry and the
Institute of Chiropodists and Podiatrists. The document provides information about the
behaviours, actions, knowledge and skills which should underpin the decision-making and
actions of podiatrist prescribers. The document has been updated as part of this work.
Outline Curriculum Framework
In collaboration with the professional bodies representing radiographers, physiotherapists,
paramedics and dietitians, the College of Podiatry and the Institute of Chiropodists and
Podiatrists developed and published the Outline Curriculum Framework for education
1The College of Podiatry Good Practice in Prescribing and Medicines Management for Podiatrists
2Allied Health Professions Federation (2018) Outline curriculum framework for education programmes to prepare: physiotherapists,
podiatrists, therapeutic radiographers and paramedics as independent/supplementary prescribers and to prepare: diagnostic
radiographers and dietitians as supplementary prescribers
5OFFICIAL
programmes to prepare practitioners to become prescribers. The document is in line with
the Competency Framework for all Prescribers3 and the Health and Care Professions
Council (HCPC) Standards for Prescribing4.
If legislation is amended to enable podiatrist independent prescribers to prescribe an
additional four controlled drugs then no further changes to education programmes will be
required as the HCPC Standards for Prescribing, against which the education programmes
are approved, do not refer to specific medicines. The Outline Curriculum Framework
already reflects the considerations necessary for education in preparation for the
prescribing of any controlled drugs by podiatrist independent prescribers.
Consultation Stage Impact Assessment
Impact assessments are an integral part of the policy making process; the purpose of an
impact assessment is to focus on why the proposed intervention is necessary, what impact
the policy change is likely to have and the highlighting of costs, benefits and risks. The
Outline Curriculum Framework contains evidence of the actual (where available) and
estimated costs and benefits associated with the proposal. The consultation is an
opportunity to gather additional evidence to further inform the costs, benefits and risks of
the proposal.
The questions being asked
Question 1
Should amendments to legislation be made to enable podiatrist independent prescribers to
prescribe additional controlled drugs for their patients?
Question 2
Do you have any additional information on any aspects not already considered as to why
the proposal to amend the list of controlled drugs which podiatrists can independently
prescribe SHOULD go forward?
Question 3
Do you have any additional information on any aspects not already considered as to why
the proposal to amend the list of controlled drugs which podiatrists can independently
prescribe SHOULD NOT go forward?
Question 4
To what extent do you agree or disagree with each of the proposed controlled drugs that
podiatrist independent prescribers would be able to prescribe for their patients?
Question 5
Does the Consultation Stage Impact Assessment give a realistic indication of the likely
costs, benefits and risks of the proposal?
Question 6
Do you think that this proposal could impact (positively or negatively) on any of the
protected characteristics covered by the Public Sector Equality Duty set out in section 149
of the Equality Act 2010 or by section 75 of the Northern Ireland Act 1998?
3 Royal Pharmaceutical Society (2016) A competency framework for all prescribers
4 Health and Care Professions Council (2013) Standards for prescribing
6OFFICIAL
Question 7
Do you feel that this proposal could impact (positively or negatively) on health inequalities
experienced by certain groups?
You will also be asked questions about yourself and / or your organisation so that the views
of different groups can be better understood.
7OFFICIAL
Background
Context
The Chief Professions Officers’ Medicines Mechanisms (CPOMM) programme is set in the
context of the current direction of the NHS which puts patients and the public at the heart of
everything we do. The Five Year Forward View5 sets out the vision for the future of the NHS
in England, a future in which access to health care is intuitive and simplified. The NHS Long
Term Plan6 envisions integrated care systems for England; within which redesigned
services can enable a future where care can be personalised when people need it and can
be joined-up with fewer appointments with health professionals to receive it.
NHS England and NHS Improvement are leading a number of key programmes of work
which aim to put in place the infrastructure to make the vision a reality. The programmes
include the Medicines Value Programme which has been set up to improve health
outcomes from medicines and ensure that the NHS in England gets the best value from the
NHS medicines bill. Whilst the Medicines Value programme is focused on the NHS in
England, similar types of work are taking place in Scotland, Wales and Northern Ireland.
The CPOMM programme aims to enable the selected professions to maximise their ability
to improve the patient’s care, experience and safety. Optimising medicines and improving
access to the right medicines whilst maintaining safety for patients would also be consistent
with the government’s policy to focus on improved outcomes for all and to transform the
way the NHS provides care. The CPOMM programme also supports the achievement of a
number of current ambitions across the UK:
In Scotland: supports the delivery of Achieving Sustainable Quality in Scotland’s
Healthcare: A ‘20:20’ Vision7, Health and Social Care Delivery Plan 20168 and Realising
Realistic Medicine 2015/169
In Wales: supports the achievement of ambitions set out in Taking Wales Forward 2016-
202110, Prosperity for All: the national strategy11 and A Healthier Wales: our Plan for
Health and Social Care12
In Northern Ireland: supports the delivery of Health and Wellbeing 2026: Delivering
Together13 and the Medicines Optimisation Quality Framework14
Programme of work
In 2015 NHS England undertook a scoping project to determine the need for prescribing,
supply and/or administration of medicines responsibilities to be extended to a number of
regulated health professionals. The resultant report indicated the legal mechanism of
5 NHS England (2014) Five year forward view
6 NHS England (2019) The NHS long term plan
7 NHS Scotland (2011) Achieving sustainable quality in Scotland’s healthcare: a 20:20 vision
8 The Scottish Government (2016) Health and social care delivery plan
9The Scottish Government (2017) Realising realistic medicine: Chief Medical Officer’s annual report 2015-16
10 Welsh Government (2016) Taking Wales forward 2016-2021
11 Welsh Government (2017) Prosperity for all: the national strategy
12 Welsh Government (2018) A healthier Wales: our plan for health and social care
13DoH Northern Ireland (2016) Health and wellbeing 2026: delivering together
14 DoH Northern Ireland (2016) Medicines Optimisation Quality Framework
8OFFICIAL
administration, supply or prescribing that best fits the professions considered, and
prioritised certain professions based on current NHS priorities.
The CPOMM programme of work commenced on 1 April 2017 to take forward the identified
priorities. A programme board was established to oversee this work (see appendix B) and a
working group was founded to support the development of this work (see appendix B).
We are leading consultations on behalf of the four nations on proposals which include
changes to medicines responsibilities for eight regulated health professions as follows:
• enabling dental hygienists and dental therapists to supply and administer specific
medicines under exemptions within medicines legislation
• enabling biomedical scientists, clinical scientists and operating department
practitioners to supply and administer medicines using patient group directions
• amending the current lists of controlled drugs that podiatrist and physiotherapist
independent prescribers are legally able to prescribe
• amending the list of medicines that paramedics can administer in emergency
situations using exemptions
All the proposals share the same aim: to make it easier for people to get the medicines they
need when they need them and avoiding the need for people to see additional health
professionals just to receive medicines.
Views are sought on the proposed changes for each of the eight professions separately
because of the differences between the professions, any unique characteristics which apply
to them and the changes being proposed for them. Furthermore, changes to medicines
legislation need to be considered independently for each profession. However, only one
consultation guide has been developed for both dental therapists and dental hygienists due
to the similarity of the professions; although we will still be seeking views on these two
professions separately.
All of the consultations can be found on the NHS England consultation hub website.
9OFFICIAL
Introduction to the podiatrist profession
The role of the podiatrist
Podiatrists are statutory regulated health professionals. There are currently 13,02615
podiatrists registered with the Health and Care Professions Council (HCPC) in the UK. The
terms ‘podiatrist’ and ‘chiropodist’ are protected titles by law. The terms both encompass
the same role; throughout this consultation guide the term ‘podiatrist’ will be used for clarity.
Podiatry pre-registration education is at degree level: level 6 on the Framework of Higher
Education Qualifications (FHEQ) and the Scottish Credit and Qualifications Framework
(SCQF). Undergraduate programmes are delivered within higher education institutions in
the UK. All are approved by the HCPC to provide programmes that enable graduates to
obtain registration to practise as a podiatrist.
The role of the podiatrist encompasses a broad scope of practice to assess, diagnose and
manage a wide range of local and systemic conditions affecting the lower limb. Podiatrists
work in a wide variety of locations such as:
• hospitals
• GP practices
• independent practices
• patients’ homes
• nursing homes
• day centres
• schools
• health centres
• occupational health settings including prisons, schools, industry, sports clubs and for
the Armed Forces
The College of Podiatry and the Institute of Chiropodists and Podiatrists estimate that
around 50% and 82% respectively of their practising members undertake an element of
their work in the private sector although those podiatrists working in advanced practice
largely work in the NHS or private hospital settings.
After registration, podiatrists can choose to develop their skills and experience in one
particular speciality, as well as acquire new skills at a post-graduate level. These
experienced and additionally trained podiatrists are known as advanced podiatrist
practitioners and their role is in line with the national multi-professional definition of
advanced clinical practice and associated framework16 below:
Advanced clinical practice is delivered by experienced, registered health and care
practitioners. It is a level of practice characterised by a high degree of autonomy and
complex decision making. This is underpinned by a master’s level award or
equivalent that encompasses the four pillars of clinical practice, leadership and
management, education and research, with demonstration of core capabilities and
area specific clinical competence.
15 Health and Care Professions Council registrants by profession & route & gender September 2020
16 Health Education England (2017) Multi-professional framework for advanced clinical practice in England
10OFFICIAL
Advanced clinical practice embodies the ability to manage clinical care in partnership
with individuals, families and carers. It includes the analysis and synthesis of
complex problems across a range of settings, enabling innovative solutions to
enhance people’s experience and improve outcomes.
Prescribing is an advanced clinical practice activity that requires specific postgraduate
training but is built upon the underpinning knowledge and competence demonstrated from
the point of initial registration and maintained throughout professional practice. All podiatrist
independent prescribers are advanced practitioners.
Podiatrists can work in a number of speciality areas, some of which are listed below:
• musculoskeletal conditions
• diabetes care
• general podiatric care
• foot surgery
Podiatrist independent prescribers may not currently be prescribing controlled drugs in all
these settings, but this may change in the future.
The professional bodies
The College of Podiatry and the Institute of Chiropodists and Podiatrists are the
professional bodies representing podiatrists in England, Scotland, Wales, Northern Ireland
and the Channel Islands. The roles of the professional bodies are summarised in appendix
C for information.
Professional regulation
The purpose of professional regulation is to protect the public. All podiatrists, whether
working in the NHS, private or voluntary sectors, must be registered with the HCPC. The
HCPC sets the standards that all registrants have to meet in relation to their education,
proficiency, conduct, performance, character and health. These are the standards that the
HCPC considers necessary for safe effective practice. Registrants must meet all these
standards to register and meet the standards relevant to their scope of practice to stay
registered. They must complete a professional declaration every two years thereafter, to
confirm they have continued to practise and continue to meet these standards. Registrants
must also ensure that they have appropriate indemnity in place to cover all of their work.
This indemnity may be provided through an employer, a professional body or by private
arrangement.
There are additional annotations on the register for podiatrists who are:
• eligible to administer, sell and supply prescription-only medicines using exemptions
listed in legislation
• supplementary prescribers
• independent and supplementary prescribers
11OFFICIAL
How podiatrist independent prescribers are trained
Eligibility to access HCPC approved prescribing programmes
Advanced practitioner podiatrists must gain access to, and successfully complete, a HCPC
approved prescribing programme in order to achieve annotation on the HCPC register as a
podiatrist independent prescriber. There are 82 independent / supplementary prescribing
programmes approved for podiatrists by HCPC in the UK - 65 in England, 12 in Scotland
and 5 in Wales. There are no programmes currently available in Northern Ireland.
In line with other allied health professions able to train as prescribers (e.g. physiotherapists,
therapeutic radiographers and paramedics), podiatrists must meet the entry criteria as listed
in the HCPC Standards for Prescribing17 which are developed further in the Outline
Curriculum Framework18 and are listed in appendix D.
HCPC approval of prescribing programmes
Prescribing education programmes are a minimum of 38 days in duration including
supervision in clinical practice and are offered as multi-professional programmes. Each
programme must be approved by the relevant regulator for each prescribing profession and
are approved for podiatrists by the HCPC. The HCPC currently approves independent and
supplementary prescribing education programmes against the HCPC Standards for
Prescribing.
The core content of education programmes is the same for all non-medical prescribers, with
profession-specific elements and practice-specific assessments designed to allow
profession-specific differentiation where required. Programmes are delivered at level 6
(degree level) or level 7 (master’s level). The additional considerations related to the
prescribing of controlled drugs are included within the education programmes.
The HCPC Standards for Prescribing have two purposes:
• They set out the processes and procedures that an education provider delivering
training in prescribing must have in place in order to deliver the training safely and
effectively.
• They also set out the knowledge, understanding and skills that a registrant must
have when they complete their prescribing training and which they must continue to
meet once in practice.
Scope of independent prescribing practice
The HCPC defines scope of practice as the areas in which a registrant has the knowledge,
skills and experience necessary to practise safely and effectively19. The College of Podiatry
and Institute of Chiropodists and Podiatrists have further defined the scope of podiatrist
independent prescribing in the following statement. This ensures that prescribing within the
scope of podiatry practice is aligned with, and remains within, the boundaries of
contemporary professional practice and an individual’s scope of competence.
“The professional bodies agree that it is necessary to direct those members, who are
engaged in the practice of independent prescribing, to ensure that they concern
17 Health and Care Professions Council (2013) Standards for prescribing
18 Allied Health Professions Federation (2018) Outline curriculum framework for education programmes to prepare: physiotherapists,
podiatrists, therapeutic radiographers and paramedics as independent/supplementary prescribers and to prepare: diagnostic
radiographers and dietitians as supplementary prescribers
19 HCPC (2013) Standards of proficiency- chiropodists / podiatrists
12OFFICIAL
themselves only with those medicines which are relevant to the treatment of disorders
affecting the foot, ankle and associated structures, in line with current practice and
consistent with published professional guidance”’20.
Continuing professional development (CPD)
Once registered, podiatrists must undertake CPD and demonstrate that they continue to
practise both safely and effectively within their scope of practice, in order to maintain their
registration. For the duration of their career, registrants are required to maintain a
continuous, up-to-date and accurate record of their CPD activities, which must demonstrate
a mixture of learning activities relevant to current or future practice. Their CPD activities
must contribute to both the quality of their practice and service delivery and benefit service
users.
Those podiatrists who are members of the College of Podiatry are also required to meet the
standards of clinical practice and the code of conduct, ethics and practice as set by the
College of Podiatry. Podiatrists who are members of the Institute of Chiropodists and
Podiatrists are similarly obliged to meet the standards of clinical practice and professional
ethics required for membership.
When the members of a profession within its remit renew their registration, the HCPC
randomly audits the CPD activities of 2.5% of registrants in that profession. Those
registrants who are chosen for audit must submit a CPD profile to show how their CPD
meets the minimum standards of the regulator. A failure to submit or to meet the standards
required leads to administrative removal from the register.
Additional requirements are made of those podiatrists who hold additional annotations on
the HCPC register listed above including those who have successfully completed
prescribing courses approved by the HCPC, which enable the registrant to practise as a
supplementary and/or independent prescriber. Advanced practitioners who are also
qualified as prescribers must meet not only the general standards for all registrants, but
also the additional standards that only apply to prescribers as outlined in the HCPC
Standards for Prescribing21. At the point of re-registration every two years, when podiatrist
prescribers must declare that they remain fit to practise as podiatrists; it is implicit in their
declaration that they remain fit to practise as a prescriber as this is part of their scope of
practice.
Local governance arrangements expect that podiatrist prescribers demonstrate ongoing
CPD in line with the document A Competency Framework for All Prescribers22. Podiatrist
prescribers demonstrate this through the use of personal formularies and at annual
professional development review. Those who intend to prescribe controlled drugs will be
required to clearly demonstrate the continued ability to do this.
20 The College of Podiatry ( 2018) Good Practice in Prescribing and Medicines Management for Podiatrists
21 Health and Care Professions Council (2013) Standards for prescribing
22 Royal Pharmaceutical Society (2016) A competency framework for all prescribers
13OFFICIAL
Case for change
Identification of viable options
The report of the 2015 NHS England scoping project indicated the legal mechanism of
administration, supply or prescribing that best fits the professions considered, and
prioritised certain professions based on current NHS priorities. The report recommended
that further work should be undertaken to increase the number of controlled drugs that
podiatrist independent prescribers can currently prescribe. In addition to being able to
prescribe any licensed medicine within their scope of practice and competence, podiatrist
independent prescribers can currently prescribe four controlled drugs for their patients.
Consequently, they must refer patients to other prescribers, usually GPs, to receive the
controlled drugs that they are currently not permitted to prescribe, even though they have
the knowledge, skills and experience to safely and effectively prescribe them for their
patients.
Three options have been considered in relation to extending the number of controlled drugs
that podiatrist independent prescribers can prescribe for their patients; however, option 3
was deemed to be unviable and therefore only options 1 and 2 are being considered as
part of this consultation.
Option 1: No change
There would be no change to legislation; podiatrist independent prescribers would continue
to prescribe from the current restricted list of four controlled drugs and would continue to
refer patients to other prescribers if treatment of their condition required any of the
proposed controlled drugs and use of supplementary prescribing is impractical.
Benefits
For some patients, the scope of the existing legislation works well, for example for those
patients whose pain is relieved adequately and without adverse effects by the controlled
drugs currently available to podiatrist independent prescribers.
Limitations
Existing arrangements may not best support the needs of all patients, particularly those for
whom the controlled drugs currently available to podiatrist independent prescribers provide
inadequate pain relief or produce intolerable side effects. Those patients who are unable to
access the most appropriate controlled drug for management of their pain from the
podiatrist independent prescriber would have to continue to visit another health
professional, usually a GP, to receive the medicines they require. The existing
arrangements result in unnecessary delays for patients, duplication of appointments and
possibly prolonged pain. The full impact of this option and the limitations of the current
mechanisms available to podiatrists are outlined in section 4.2.
14OFFICIAL
Option 2: addition of further controlled drugs to the list of controlled drugs that
podiatrist independent prescribers can already prescribe
Benefits
Podiatrist independent prescribers primarily need to prescribe controlled drugs for the
management of pain for their patients. Expansion of the current list to include four
controlled drugs commonly prescribed for the management of pain would benefit those
patients for whom best clinical evidence indicates that these medicines work most
effectively. If legislation is amended, when seeing podiatrist independent prescribers,
patients would receive the right treatment at the right time without needing additional
appointments with other health professionals just to receive the medicines they need. The
rationale for the selection of the four controlled drugs can be found in section 4.3.
Limitations
The proposed additions to the current list of controlled drugs that podiatrist independent
prescribers could prescribe may mean that a small number of patients may still need
additional appointments with other health professionals to access controlled drugs outside
of those that podiatrist independent prescribers are permitted to prescribe. This is most
likely to be because they need controlled drugs for a medical condition that is outside of the
usual scope of practice of a podiatrist.
Option 3: independent prescribing of any controlled drug from schedules 2 - 5
An option whereby podiatrist independent prescribers would be able to prescribe any
controlled drug from schedules 2 - 5 was considered but not deemed a viable option due to
governance considerations. This option was therefore not taken further as part of this
consultation.
Benefits:
There is only one benefit of this option perceived and that is that this option would prevent
the need for any further amendments to the list of controlled drugs that podiatrist
independent prescribers can prescribe.
Limitations:
Podiatrist independent prescribers would have access to a large number of controlled drugs
listed in the four schedules, in excess of 100 in schedule 2 alone, most of which would not
ordinarily need to be prescribed as part of podiatry practice. Access to all controlled drugs
within schedules 2-5 is therefore deemed unnecessary and not in line with good
governance procedures.
In summary, there are two options for consideration in this consultation:
Option 1: no change
Option 2: addition of four controlled drugs to the existing restricted list of controlled
drugs that podiatrist independent prescribers can already prescribe
15OFFICIAL
Limitations of the current use of medicines mechanisms by
podiatrists
Supply and administration mechanisms
4.2.1.1 Patient specific directions (PSDs)
Podiatrists can administer and supply medicines to named patients using PSDs. A PSD is a
written instruction to supply or administer a medicine to a named patient who has been
assessed on an individual basis by the authorised prescriber who then prescribes the
medicine23. The PSD then enables a podiatrist to administer or supply the medicine under
certain circumstances.
PSDs are useful in many care settings; they are individually tailored to the needs of a single
patient, wide-reaching and can encompass controlled drugs. However, there are certain
limitations to their use:
• they require direct input from an independent prescriber
• they can be restrictive when access to a prescriber is problematic or if the service
provided is non-prescriber led
• organisations may limit locally who is authorised to supply and/or administer
medicines using PSDs
The use of PSDs has inherent limitations to independent practice; for instance, when in
remote situations, where a GP may not always be immediately available or where a doctor
is not part of the patient pathway.
4.2.1.2 Patient group directions (PGDs)
Since 2000, podiatrists have been able to supply and administer medicines to patients
meeting certain criteria using PGDs. PGDs provide a legal framework that allows the supply
and administration of a specified medicine(s), by named, authorised, registered health
professions, to a pre-defined group of patients needing prophylaxis or treatment for a
condition described in the PGD, without the need for prescription or an instruction from a
prescriber. They are written instructions for the supply or administration of medicines to
groups of patients who may or may not be individually identified before presentation for
treatment. They are NOT a form of prescribing24.
PGDs cannot be used by podiatrists to supply or administer the controlled drugs their
patients need from schedules 2 and 3. This means that PGDs cannot include tramadol
hydrochloride, pregabalin or gabapentin (which are listed in schedule 3). For more
information about the scheduling of controlled drugs, see appendix A.
4.2.1.3 Exemptions
The law defines some medicines as prescription only medicines, which normally need to be
prescribed by a doctor or another prescriber before they can be administered or supplied to
a patient. However, there are a range of exemptions from these restrictions which allow
certain groups of health professionals – for example, midwives, podiatrists, optometrists,
paramedics and orthoptists – to supply and administer listed prescription only medicines
direct to patients.
23 Specialist Pharmacy Service (2018) Questions about patient specific directions
24 NICE (2017) Patient group directions: medicines practice guideline
16OFFICIAL
Since 1980, podiatrists have had the legal ability to supply and administer medicines from a
list of exemptions in medicines legislation. The list of exemptions in medicines legislation
was extended in 2011 to include dihydrocodeine and some commercially available pre-
mixed medicines, such as lidocaine and methylprednisolone combinations. The resultant
list includes selected local anaesthetics, antifungals, analgesics, anti-inflammatories and
antibiotics.
The proposed controlled drugs are not included in the current exemptions list as they are
only appropriate for use by advanced podiatrist practitioners who are also independent
prescribers and not the whole podiatric workforce.
Prescribing mechanisms
4.2.2.1 Supplementary prescribing
Podiatrists have been able to train to become supplementary prescribers since 2005; there
are currently 511 qualified podiatrists annotated as supplementary prescribers on the
HCPC register25. Using supplementary prescribing, the podiatrist prescribes in partnership
with a doctor and the patient within a written clinical management plan (CMP) which must
be created before any prescribing can take place.
A CMP can include almost any licensed or unlicensed medicine, including all controlled
drugs from schedules 2-5. Supplementary prescribing can work well in the management of
long-term conditions where there is a clear existing diagnosis and the doctor is part of the
patient pathway to enable a CMP to be created or reviewed. Patients who benefit from
podiatrists using supplementary prescribing include those with lower limbs at increased risk
of ulceration and/or amputation through disorders such as diabetes or peripheral arterial
disease.
However, for services in which the team is fragmented across sites, where there is no
medical input, or when patients require a medicine that is not included in the CMP, use of
supplementary prescribing can be difficult and patients may need to see other prescribers
to receive some or all the medicines they need.
4.2.2.2 Independent prescribing
Since 2013, an advanced podiatrist practitioner who has undergone additional HCPC-
approved training can practise as an independent prescriber as well as a supplementary
prescriber. All prescribing programmes approved for podiatrists by the HCPC offer
preparatory education towards dual annotation as supplementary and independent
prescribers. There are currently 511 podiatrist prescribers on the HCPC register, 441 of
which are annotated as both independent and supplementary prescribers26.
4.2.2.3 Independent prescribing of controlled drugs
Legislation enacted in 201527 enables podiatrist independent prescribers in England,
Scotland and Wales to prescribe from a restricted list of four controlled drugs, namely:
25 HCPC supplementary prescribing data – September 2020
26 HCPC independent prescribing data – September 2020
27 The Misuse of Drugs (Amendment) (No. 2) (England, Wales and Scotland) Regulations 2015
17OFFICIAL
temazepam (schedule 3) - oral administration
lorazepam (schedule 4 part 1) - oral administration
diazepam (schedule 4 part1) - oral administration
dihydrocodeine tartrate (schedule 5) - oral administration
Since November 2019, legislative changes have permitted the prescribing of the same
controlled drugs in Northern Ireland.
The current list of four controlled drugs continues to be useful for prescribing by podiatrist
independent prescribers where it is clinically indicated for a named patient.
However, patients that are being treated by podiatrist independent prescribers and that
require controlled drugs other than those listed above may need to be referred to other
prescribers, to receive the additional medicines. Further benefit could be gained by
extending the range of controlled drugs that podiatrist independent prescribers could
prescribe which will help ensure patients receive the right treatment and at the right time,
including appropriate pain management in line with evidence-based practice.
Rationale for the selection of the additional controlled drugs
Controlling of medicines
When a prescription only medicine is classified under the Misuse of Drugs Act 1971 and
placed in one of the schedules of the Misuse of Drugs Regulations, it becomes known as a
controlled drug. The impact of this change is that it prevents the medicine being prescribed
by a podiatrist independent prescriber, even though best practice evidence for its use has
not changed, because the medicine is not included in the restricted list of controlled drugs
that they can prescribe. The UK-wide consultation on proposals to introduce podiatrist
independent prescribing took place in 201128 but it was not until 2015 that legislation was
enacted to enable podiatrist independent prescribers to prescribe controlled drugs in
England, Scotland and Wales; and November 2019 in Northern Ireland.
Podiatrist independent prescribers are prevented from prescribing any medicines which
have been scheduled as controlled drugs after the date of the consultation in 2011. An
amendment to the Misuse of Drugs Regulations in 2014 to include tramadol hydrochloride
as a schedule 3 controlled drug resulted in podiatrist independent prescribers being no
longer able to prescribe tramadol hydrochloride for their patients. If tramadol hydrochloride
had been classified prior to the public consultation in September 2011 then it would have
been included in the proposed list of controlled drugs at that stage.
In 2017, the Home Office consulted on proposals to schedule pregabalin and gabapentin as
controlled drugs under the Misuse of Drugs Regulations 200129. This followed the
recommendation to ministers by the Advisory Council on the Misuse of Drugs (ACMD) that
these two medicines should be placed in Schedule 3 of the Misuse of Drugs Regulations
alongside their classification as Class C medicines under the Misuse of Drugs Act 1971.
28 Department of Health (2011) ) Consultation On Proposals To Introduce Independent Prescribing By Podiatrists
29 Home Office (2017) Pregabalin and gabapentin: proposal to schedule under the Misuse of Drugs Regulations 2001
18OFFICIAL
Following the consultation response30 published in October 2018, both pregabalin and
gabapentin were listed in schedule 3 of the Misuse of Drugs Regulations without the
application of safe custody requirements from April 2019. It is therefore being proposed that
gabapentin and pregabalin are added to the proposed list of controlled drugs that
podiatrists can independently prescribe so that they can continue to prescribe these
medicines for their patients.
Management of pain for effective treatment
As part of the ongoing care of their patients, podiatrist independent prescribers are
expected to manage pain which may be as a result of the condition they are treating, during
the podiatric treatment or during recovery following the treatment.
Assessment of pain, including regular, frequent review is fundamental prior to and during
the prescribing of analgesia. The World Health Organisation (WHO) analgesic pain ladder31
provides a guide to relevant medicines in the management of non-cancer pain where an
assessment of pain has been undertaken and is accepted good practice in making
analgesia-choice decisions. Since its initial creation for cancer pain, its use has been
broadened to include the management of acute and chronic non-malignant pain in adults32.
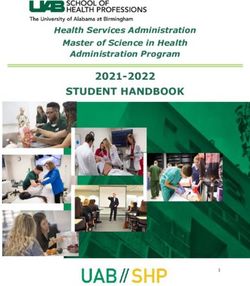
The analgesic ladder provides a three-step approach of sequential use of medicines
according to the pain level reported by the patient. The figure below gives a visual
illustration of the analgesic ladder.
Figure 1: World Health Organisation (WHO) analgesic ladder (adapted)33
30
Home Office (2018) A consultation on proposals to schedule pregabalin and gabapentin under the Misuse of Drugs Regulations
2001: Government response to the consultation
31 World Health Organisation (1996) Cancer pain relief with a guide to opioid availability
32 World Health Organisation Impact of impaired access to controlled medications.
33 Welsh Medicines Resource Centre (WeMeReC) (2014) Management of chronic non-malignant pain
19OFFICIAL
At the current time, podiatrist independent prescribers can prescribe almost all licensed
medicines that step 1 relates to, and only some of the analgesics on steps 2 and 3 of the
analgesic ladder, but not a wide range. This means that where a patient finds one choice of
medicine unsuitable for their needs, the podiatrist independent prescriber may be unable to
prescribe an appropriate alternative from the same class or step, even when clinical
guidelines indicates that an alternative should be used. Subject to local formulary or
guideline variation, tramadol hydrochloride can be used as a second choice for pain,
needing a step 2 treatment if codeine phosphate is not tolerated or is ineffective. Likewise,
morphine sulfate can be useful as a first choice for pain, needing a step 3 treatment if step
2 treatments are ineffective. Currently, the patient may face additional delays to their
treatment whilst waiting for a medical prescriber to modify their medicines regimen.
Management of pain may include stopping medicines because they are no longer needed
or no longer effective and need to be changed to another medicine. In order to cease the
prescribing of any medicine (de-prescribing) the podiatrist independent prescriber must be
able to prescribe that medicine, therefore if a podiatrist independent prescriber identifies
that a patient is being prescribed tramadol hydrochloride unnecessarily they are unable to
stop the prescription themselves but must refer the patient to another prescriber.
There are also a number of national guidelines which recommend the use of the four
proposed controlled drugs for the treatment of pain in conditions that are commonly treated
by podiatrist independent prescribers34 35 36 37 38. It is therefore desirable that podiatrist
independent prescribers are able to prescribe these medicines to mitigate the need for their
patients to see another prescriber, usually a GP, just to access the medicines of choice as
recommended within national guidelines.
Benefits of the proposal
Under the proposals, patients in contact with podiatrist independent prescribers who can
prescribe a wider range of controlled drugs would be able to receive the care and
medicines they need, without having to see another prescriber. A greater number of
patients could benefit from improved care, first time and in the right place. Effective
utilisation of the workforce is also essential in meeting the triple aim of the Five Year
Forward View by enabling improvements in health and wellbeing, reducing duplication and
fragmentation of care and making best use of the resources available in addition to
improving patient outcomes and their experience of care39.
Provision of best care, first time, in the right place
If the proposal is adopted, timely access to appropriate pain relief in conjunction with
podiatric intervention would be possible, without the need for additional appointments with
other health professionals to access medicines required. This would mean that patients will
need to make fewer repeat GP / hospital attendances and the full treatment plan could be
undertaken in one series of appointments with the podiatrist independent prescriber.
Stopping the prescription of medicines is also a prescribing responsibility; early de-
34 NICE (2014) Clinical guideline (CG177) osteoarthritis: care and management
35 NICE (2015) Clinical Knowledge Summaries: mild to moderate pain
36 NICE (2015) Clinical Knowledge Summaries: peripheral arterial disease
37 NICE (2017) Clinical guidelines (CG173) Neuropathic pain in adults: pharmacological management in non-specialist settings
38 NICE (2015) Clinical knowledge summaries: restless legs syndrome: prescribing: pregabalin
39 NHS England (2014) Five year forward view
20OFFICIAL
prescribing of controlled drugs when indicated lessens the risk of both tolerance and
dependence.
Reduced delays
Many podiatric interventions in both primary and acute settings are podiatrist-led and
therefore access to a doctor is not always possible. Podiatrist independent prescribers can
make prescribing decisions and prescribe the required medicines during their consultation
with a patient. If the proposals are adopted, there may be fewer delays for patients whilst
waiting for a doctor to review a patient and consider prescribing controlled drugs. This could
allow quicker management of acute symptoms, reducing absenteeism by workers who
need to take time off work to attend appointments, enable the swifter return to work for
patients whose symptoms can be effectively controlled more quickly, and reduce the need
for patients with greater functional disabilities to make duplicate visits.
Clearer lines of clinical responsibility and accountability
If as is proposed, podiatrist independent prescribers were able to prescribe the necessary
pain relief for patients during the consultation instead of handing off the responsibility for
prescribing certain medicines to a medical prescriber, lines of accountability and
responsibility would be further clarified. Additionally, if as proposed, the podiatrist
independent prescriber could prescribe all the analgesia the patient needed during the
episode of care, this could enable the identification of dependence or misuse more quickly.
Reduced resource usage and cost effectiveness
The proposed amendments to the list of controlled drugs would ensure that the skills of an
advanced podiatrist practitioner are effectively and fully utilised in providing integrated
podiatric care with adjuvant medicines management. These roles have a demonstrated
ability to free up both GP and hospital consultant appointment capacity by reducing the
demand on doctors to provide medication reviews linked to podiatric intervention.
Medicines optimisation
Medicines optimisation looks at how patients use medicines over a period of time. It may
involve stopping some medicines as well as starting others and considers opportunities for
lifestyle changes and non-medical therapies to reduce the need for medicines40.
If as proposed, podiatrist independent prescribers could prescribe further controlled drugs,
they could better enable patients to get the best use of their medicines in line with the
principles of medicines optimisation. For example:
• The proposed medicines are used in evidence-based clinical pathways of care.
• Short courses could be prescribed as the effect would be reviewed at each
appointment.
• Should the medicine no longer be required then podiatrist independent prescribers
could de-prescribe the medicine therefore ensuring patients only take those
medicines that are needed.
• Podiatrist independent prescribers will have full access to patients’ medical records
and will be able to ensure as far as possible, that any additional medicines they
prescribe do not interact with any existing medicines that the patient is taking.
40Royal Pharmaceutical Society (2013) Medicines Optimisation: Helping patients to make the most of medicines Good practice
guidance for healthcare professionals in England
21OFFICIAL
22OFFICIAL
Use in clinical practice
The scenarios below are illustrative examples to demonstrate how podiatrist independent
prescribers might prescribe the four proposed controlled drugs within clinical practice and
the benefits to be gained from this proposal.
Scenario 1- tramadol hydrochloride
Tramadol hydrochloride is an opioid painkiller used to treat moderate acute pain. It may be used
when simple painkillers are not appropriate and when other weak opioids, such as codeine
phosphate, have not been effective. Patients who have operations involving the foot and ankle can
benefit from the pain-relieving effects of tramadol hydrochloride to help them complete the early
stages of their rehabilitation.
Some patients who have acute injuries and/or disease affecting the bones, joints, muscles, soft
tissues and nerves (musculoskeletal conditions) may also benefit from its short-term use for its
pain-relieving effects where codeine phosphate has not been effective.
Some podiatrists undertake surgical procedures of the foot and ankle in hospital settings and
manage patient’s post-surgical needs. They also work in podiatry departments and as part of multi-
disciplinary teams providing care to patients with a myriad of foot, ankle and lower limb complaints.
Good pain relief is essential to support effective recovery and give optimal benefits from podiatry
care.
Podiatrists cannot currently independently prescribe tramadol hydrochloride. This means that if a
patient receiving podiatry care requires tramadol hydrochloride to give effective pain relief the
podiatrist must send the patient to see a doctor. This can mean that patients may temporarily
deviate from their management if they feel it is too painful, which can slow their progress down and
delay their overall recovery.
If podiatrists were able to independently prescribe tramadol hydrochloride, patients would be able to
receive timely access to the appropriate pain relief they required to support their treatment and
rehabilitation. This would include stepping down the patient’s treatment to an alternative painkiller
as the post-operative pain settles. Patients would experience fewer delays in their progress and
would need to make fewer visits to a range of professionals to obtain effective short-term pain relief.
Scenario 2- morphine sulfate
Morphine sulfate is an opioid painkiller used to treat moderate to severe acute and chronic pain. It
is considered when non-opioid painkillers are not appropriate and when other opioid medicines
have not been effective. Patients who have operations involving the foot and ankle can benefit from
the pain-relieving effects of morphine sulfate to help them complete the early stages of their
rehabilitation. Some patients who have acute injuries and/or disease affecting the bones, joints,
muscles, soft tissues and nerves (musculoskeletal conditions) may also benefit from its short-term
use for its pain-relieving effects where other opioids has not been effective. Good pain relief is
essential to support effective recovery and give optimal benefits from podiatry care.
Podiatrists cannot currently independently prescribe morphine sulfate. This means that if a patient
under the care of a podiatrist would benefit from morphine sulfate to support their recovery, the
podiatrist must send the patient to see a doctor, or they must wait until a doctor is available to
discuss the case with the podiatrist. This situation currently occurs frequently and leads to delays in
providing effective pain relief and rehabilitation.
If podiatrists were able to independently prescribe morphine sulfate, patients would be able to
receive timely access to the appropriate pain relief they require to support their treatment and
rehabilitation. Podiatrists would be able to provide optimum levels of care in line with good practice
guidance. GP capacity could be improved through fewer interruptions for medication review.
23You can also read