COVID-19: Variants Update - Ministry of Health
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
COVID-19: Variants Update
Date: 14 May 2021
During the COVID-19 pandemic, the Ministry of Health has seen high interest in all aspects of the virus from not
only the scientific and health community but the general public as well. This update is designed to provide new
information on variants of the virus that are of interest or concern. The first three pages of this update are
provided as a brief overview, followed by the full technical report.
Information gathered in the last week is provided in red text.
Background
SARS-CoV-2, the virus that causes COVID-19, can undergo genetic mutations. These can occur naturally over
time or from selective pressures.[1] While the vast majority of mutations do not change the virus in any
meaningful way, some mutations, particularly those relating to virus’s spike protein, could affect the
transmissibility of the virus, disease severity, and the effectiveness of treatments or vaccines.[2] There is
concern that if infection of SARS-CoV-2 persists for extended periods of time, such as within an
immunocompromised person, it could serve as a way for mutations to accumulate.[3, 4]
Mutation nomenclature (i.e., how mutations are named) describes what has occurred at a specific location of
the viral genome.[5] For example, the ‘E484K’ mutation means that at the position 484, the amino acid changed
from glutamic acid (E) to lysine (K).[6] When a deletion occurs, the location is provided (e.g., deletion 144).
Mutations constitute different lineages of the virus, commonly referred to as ‘variants’. A variant is referred to
as a ‘strain’ when it becomes sufficiently different from its patent virus, either by showing distinct physical
properties or behaving in a pathologically or immunologically different way.
Potentially problematic variants that may have concerning epidemiological, immunological, or pathogenic
properties are raised for formal investigation by two main investigative groups - the Public Health England
Variant Technical Group[7, 8] and the SARS-CoV-2 Interagency Group in collaboration with the Centers for
Disease Control and Prevention (CDC) in the United States (US).[9]
New variants are discovered through whole genome sequencing – a laboratory testing process, for which most
countries have had low testing capacity prior to the COVID-19 pandemic. New Zealand now sequences all viable
SARS-CoV-2 samples, however, the use and application of whole genome sequencing has varied between
countries, and globally genomic surveillance of SARS-CoV-2 remains limited.[10, 11] The Global Initiative on
Sharing Avian Influenza Data (GISAID) is a consortium that promotes and provides open access to genomic
sequence data. Despite its original purpose for sharing avian (bird) flu data, it has proved to be beneficial in the
fight against SARS-CoV-2. Submission of SARS-CoV-2 sequences to this repository has been key in tracking
emerging variants. The US reports weekly published sequences from the National SARS-CoV-2 Strain
Surveillance (NS3) programme, CDC contracts, and other sequencing efforts here and sequencing information
from the UK can be found here.
Within this document, we will provide information on how “variants under investigation” (VUI), “variants of
interest” (VOI), and “variants of concern” (VOC) are identified and describe what is known about their current
epidemiological spread, before reviewing the emerging evidence and research on transmissibility, disease
severity, vaccine protection, treatment effectiveness, and immune escape properties.
1COVID-19: Variants Update
New information in this update
• Public Health England has escalated the variant labelled B.1.617.2 (originally discovered in India) from
VUI to VOC due to emerging evidence it is at least as transmissible as B.1.1.7. However, evidence
regarding disease severity, immunity, and vaccine protection are still limited.
• Based on contact tracing data, Public Health England estimates the secondary attack rate for B.1.617.2
among locally acquired cases to be 9.5% (95% CI: 5.9-14.9%), which is similar to B.1.1.7.
• Two further pre-prints have found that B.1.617.2 is able to moderately reduce neutralisation by antibodies
induced from previous infection or from Pfizer vaccination.
• Up to 10 May 2021, whole genome sequencing in New Zealand has identified the following VOCs:
o 173 sequences of B.1.1.7. This is an increase of 13 sequences since the previous update.
o 28 sequences of B.1.351. There is an increase of one sequence since the previous update.
o 5 sequences of P.1. There is no change in P.1 sequences since the previous update.
o 10 sequences of B.1.617.2. This is the initial report of B.1.617.2 sequences.
• An analysis of national surveillance data in Israel reported high efficacy of the Pfizer vaccine against
infection, asymptomatic infection, and COVID-19 related hospitalisation and death where there was a
very high prevalence of B.1.1.7 (94.5%).
• In a real-world analysis of a mass vaccination campaign in Qatar using the Pfizer vaccine, vaccine
efficacy against the B.1.1.7 variant (which emerged in the UK) was 89.5% (95% CI: 85.9-92.3%) at 14 or
more days after the second dose. Vaccine efficacy was 75% (95% CI: 70.5-78.9%) against the B.1.351
variant (which emerged in South Africa). Vaccine effectiveness against severe disease or death in Qatar,
where both B.1.1.7 and B.1.351 are prevalent, was 97.4% (95% CI: 92.2 to 99.5%).
• Moderna is developing a targeted vaccine towards the B.1.351 variant, currently labelled mRNA-
1273.351. In a clinical study of the mRNA-1273.351 vaccine, individuals were vaccinated with a third
dose (as a booster) of either the original vaccine (mRNA-1273) or the variant targeted vaccine (mRNA-
1273.351), six months after they had completed their first course of vaccination. In blood tests for
immune response, there was an increase in virus neutralisation in those given mRNA-1273.351, the
targeted vaccine, compared to those given the original. This is encouraging evidence suggesting that
vaccines can be altered to target multiple variants, however, trials will continue, and real-world efficacy
for this approach is not yet established.
• Up to date information on global cases can be found at:
o B.1.1.7 (cov-lineages.org and outbreak.info)
o B.1.351 (cov-lineages.org and outbreak.info)
o P.1 (cov-lineages.org and outbreak.info)
o B.1.617.2 (cov-lineages.org and outbreak.info)
2COVID-19: Variants Update
VOC Summary
Current VOCs have “evidence of an increase in transmissibility, more severe disease (increased hospitalisations or deaths), significant reduction in neutralisation by
antibodies generated during previous infection or vaccination, reduced effectiveness of treatments or vaccines, or diagnostic detection failures”.[9] Table 1 collates key
information on nomenclature, transmissibility, severity, immune evasion and countries in which the variants have been identified.
Table 1. Summary of characteristics for Variants of Concern as of 14 May 2021, red text denotes new information, red highlights note variables of particular concern.
Lineage B.1.1.7 B.1.351 P.1 B.1.617.2
Country first identified United Kingdom ‘Kent Variant’ South Africa Brazil India
501Y.V1, VOC-202012/01, 501Y.V2, VOC-202012/02, 501Y.V3, B.1.1.28.1, VOC-
Other names VOC-21APR-02
VOC-20DEC-01 VOC-20DEC-02 202101/02, VOC-21JAN-02
• ~40-80% more transmissible (R0 • Not well established. • Not established. Preliminary • Not well established. Believed
~3.5-5.2)* Preliminary estimate ~50% estimates 40%-160% more to be similar to B.1.1.7 due to
more transmissible transmissible mutations present in both
Transmissibility
variants and can compete with
B.1.1.7 as observed by Public
Health England in the UK
• Mortality: 60-70% increased • Mortality: Not well established. • Mortality: Not established. One • Mortality: Not well established
mortality compared to previous One report of no increased risk report of no increased risk of • Hospitalisation: Not well
variants of mortality mortality established
Severity • Hospitalisation risk: 30-70% • Hospitalisation: Not well • Hospitalisation: Not well
increased risk established. One report of established. One report of
approximately 3.6 times risk of approximately 2.6 times risk of
hospitalisation hospitalisation
Immune evasion Minimal Moderate-Strong Moderate-Strong Not well established
69/70 deletion, 144 deletion, T19R, 156-158 deletion, L452R,
Notable mutations N501Y, E484K, K417N N501Y, E484K, K417T
N501Y, P681H, A570D T478K, P681R, D950N
Countries reporting
125 85 43 43
sequences
*Assuming R0 for original SARS-CoV-2 of approximately 2.5 to 2.9 [12, 13]
3COVID-19: Variants Update
Variants of Concern - further detail
Current VOCs designated by Public Health England are:
• B.1.1.7: VOC-20DEC-01 (VOC-202012/01 or 501Y.V1); emerged in Kent, UK.
• B.1.351: VOC-20DEC-02 (VOC-202012/02 or 501Y.V2); emerged in South Africa.
• P.1: VOC-21JAN-02 (VOC-202101/02 or 501Y.V3); detected in Japan, emerged in Manaus, Brazil.
• B.1.1.7 with E484K: VOC-21FEB-02 (VOC-202102/02); emerged in Bristol, UK.
• B.1.617.2: VOC-21APR-02; emerged in India.
In addition, the CDC also categorises variants B.1.427 and B.1.429 as VOCs (“California variants”).
In a Technical Briefing from Public Health England on 11 March 2021, a variant risk assessment framework was
published, describing how the risk for new variants is determined using the following indicators: zoonotic
emergence and transmission, transmissibility between humans, infection severity, susceptibility and immunity,
vaccines, and drugs and therapeutics.[14] The latest Technical Briefing on the VOCs in England is linked here.
The CDC has introduced an additional category termed ‘Variant of High Consequence’. This will include variants
that show clear evidence that prevention measures or medical countermeasures have significantly reduced
effectiveness relative to previously circulating variants. As of 14 May 2021, the CDC lists no variants in this
category. The link to the CDC’s website describing SARS-CoV-2 variant classifications and definitions is available.
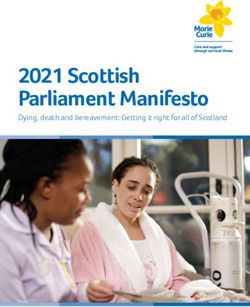
here. The CDC is also tracking the proportion of variants circulating in the US for both VOC and VOI (Figure
1).[15]
Variants under Investigation and Variants of Interest
Variants with unconfirmed or preliminary evidence of immune evasion, increased transmissibility, or other
concerning features are considered Variants of Interest. They may also be designated as a ‘Variant Under
Investigation’ (VUI) by Public Health England.[16]
Variants designated as a VUI are named by a year, month, and number (e.g., VUI-21MAR-02). The CDC defines a
‘Variant of Interest’ (VOI) as a variant with ‘specific genetic markers that have been associated with changes to
receptor binding, reduced neutralisation by antibodies generated against previous infection or vaccination,
reduced efficacy of treatments, potential diagnostic impact, or predicted increase in transmissibility or disease
severity.[9] The CDC has no naming convention for VOIs.
The COVID-19 Science and Technical Advisory team is monitoring the developments of VUI/VOIs, which are
summarised below in Table 2.
4COVID-19: Variants Update
Table 2. Variants Under Investigation by Public Health England and Variants of Interest by CDC as of 14 May 2021
VUI* Classified by Lineage Origin Evidence
P.2 variant • Spike mutations E484K, D614K, and V1176F.[9]
VUI-21JAN-01 Public Health Brazil, December
(descendent of • Possible reduced antibody neutralisation from studies
(VUI-202101/01) England and CDC 2020
B.1.1.28) on the spike protein mutation E484K.[17]
Liverpool, United • Spike protein mutations F157L, V367F, Q613H and
VUI-21FEB-01 Public Health
A.23.1 with E484K Kingdom, P681R. The V367F and Q613H changes are reported
(VUI-2021102/01) England
December 2020 to modestly increase infectivity.[18]
• Spike mutations A67V, 69/70 deletion, 144 deletion,
E484K, D614G, Q677H, and F888L.[9]
• First identified in the UK on 2 February 2021.
VUI-21FEB-03 Public Health UK and Nigeria, Detected in 11 countries, including the US, Canada,
B.1.525
(VUI-202102/03) England and CDC December 2020 Europe, sub-Saharan Africa and Australia as of March
2021.[14] See Public Health England’s Technical
Briefing 7 for in-depth information on genomic and
biological profile.
• Contains spike mutations L5F, T95I, D253G, E484K,
No VUI currently New York, United D614G, and A701V.[9, 19]
assigned by Public CDC B.1.526 States, November
• Reduced antibody neutralisation by monoclonal
Health England 2020
antibodies and post-vaccine sera.[9]
• Contains spike mutations T95I, 144 deletion, E484K,
VUI-21FEB-04 Public Health United Kingdom, P681H, D796H. Identified in England in February 2021
B.1.1.318
(VUI202102/04) England February 2021 through routine genomic surveillance.[14]
• Contains spike mutations E484K, S494P, N501Y,
To be
VUI-21MAR-01 Public Health B.1.324.1 with D614G, P681H, and E1111K. Identified in England on
determined, but
(VUI 202103/01) England E484K 3 March 2021 through routine genomic
detected in UK
surveillance.[14]
To be • Contains spike mutations E484K, N501Y, P681H, 141-
Public Health determined, likely 143del.[21, 22]
VUI-21MAR-02
England
P.3
Philippines [20, • From parent lineage B.1.1.28 (the same as P.1 and P.2
21] detected in Brazil).[23]
• Designated a VOC by the CDC but is being monitored
by Public Health England as of 22 April 2021.[23]
• Characterised by the mutations S13I, W152C, L452R,
Public Health England D614G.[9]
monitoring but has CDC classified as B.1.429/B.1.427 or Southern • May have approximately a 20% increased
not classified as VUI VOC CAL.20C California transmission compared to previous variants. From
or VOC. September 2020 through January 2021, the variant
increased from 0% to 50% of sequenced cases in
California. The increased transmission could be
attributed to a 2-fold increase in viral shedding.[24]
• Genomic surveillance in India reported a variant
containing mutations E484Q and L452R on 24 March
B.1.617 and
2021. The implications of these mutations on disease
B.1.617.3.
severity, transmission, and other factors is still under
Note, B.1.617.2
VUI-21APR-01, VUI- Public Health investigation.[25]
was classified as a India
21APR-03 England • On 12 May 2021, B.1.617 accounted for 80.9% of
VOC on 6 May
sequences submitted to GISAID from India over the
2021 by Public
previous four weeks.[26] However, genomic
Health England
surveillance in India is poor and the true prevalence is
unknown.
*Public Health England changed the nomenclature for VUI in March 2021, using 2-number year and 3-letter month. Old
naming convention provided in parenthesis for cross-reference.
5COVID-19: Variants Update
Additional data on notable VUIs
Pre-print laboratory data suggests B.1.617 is moderately able to reduce antibody neutralisation from previous
infections and from vaccination with the Pfizer vaccine and is completely resistant to monoclonal antibody
medicines.[27] Two further pre-prints corroborate this evidence.[28, 29]
Public Health England has released two detailed reports on the B.1.617 cases in England.[30, 31]
o Public Health England determined that there are 3 clades (otherwise known as lineal descendants of this
variant), named B.1.617.1, B.1.617.2, and B.1.617.3. Information on B.1.617.2 is now covered below
under the evidence on specific VOCs.
New Zealand cases and global spread
Increased cases of VOC are expected in New Zealand MIF/MIQ facilities as the global presence of these variants
extends geographically and new variants become predominant. Figure 1 below displays the variants circulating
in the US in the two weeks ending 10 April 2021.
• Up to 10 May 2021, whole genome sequencing in New Zealand has identified the following VOCs:
o 173 sequences of B.1.1.7. This is an increase of 13 sequences since the previous update.
o 28 sequences of B.1.351. There is an increase of one sequence since the previous update.
o 5 sequences of P.1. There is no change in P.1 sequences since the previous update.
o 10 sequences of B.1.617.2. This is the initial report of B.1.617.2 sequences.
• Up to date information on global cases can be found at:
o B.1.1.7 (cov-lineages.org and outbreak.info)
o B.1.351 (cov-lineages.org and outbreak.info)
o P.1 (cov-lineages.org and outbreak.info)
o B.1.617.2 (cov-lineages.org and outbreak.info)
6COVID-19: Variants Update
Figure 1. SARS-CoV-2 Variants Circulating in the US in the two weeks ending 10 April 2021.
Review of evidence on specific VOCs
B.1.1.7
B.1.1.7: Genomic characteristics
The B.1.1.7 variant is characterised by notable spike protein mutations 69/70 deletion, 144 deletion, N501Y,
P681H, and A570D (Figure 2).[32] There are an additional four spike protein mutations D614G, T716I, S982A,
and D1118H.
Figure 2. Mutations of B.1.1.7 (outbreak.info)
B.1.1.7: Transmissibility
Several studies have reported increased transmissibility of B.1.1.7 with estimates ranging from it being
approximately 30% to 90% more transmissible over previous variants, with most studies estimating an increase
between 40-80%.[33-40]
7COVID-19: Variants Update
B.1.1.7 has gone on to replace previous variants in several countries, for example in the UK, Israel, and US.[8, 15,
39] From 16 January to 27 March, the proportion of variant B.1.1.7 sequenced increased from 3.1% to 44.1% in
the US.[15] Additionally, possible reinfections were identified in 0.7% of cases (95% CI: 0.6-0.8) in a study of
36,059 participants, although the reinfection rate was not considered higher for B.1.1.7 than previous
variants.[38]
One hypothesis for the increased transmissibility of B.1.1.7 relates to the N501Y mutation, which could provide
a selective advantage to the virus by increasing how tightly the spike protein binds to the human host cell ACE2
receptor.[41-45]
Increased transmission may also be the result of patients with B.1.1.7 variant having increased viral loads
compared to those infected with non-B.1.1.7 variants.[46-49] However, others have reported no statistical
difference in viral loads for B.1.1.7 and proposed that the higher viral loads are the result of ascertainment
bias.[50] A further study found no difference in viral replication between B.1.1.7 and earlier variants in primary
human airway epithelial cells.[51]
A modelling study on seasonal transmission of B.1.1.7 found there was an association with increased
transmission of the variant in colder and hotter temperatures.[52] However, these data should be interpreted
cautiously, as it was extrapolating modelling data and is still in pre-print. Other data suggests moderate
temperatures, such as during spring and fall, may decrease transmission of SARS-CoV-2,[53] supporting the
possibility of a slight seasonal component where more extreme temperatures of the winter and summer could
have an effect on transmission in some places. This is in contrast to some communicable diseases such as
influenza that have a strong seasonal component and are present predominantly in winter.
B.1.1.7: Clinical presentation and disease severity
Clinical presentation
The types of symptoms associated with B.1.1.7 are broadly similar to previous variants.[38] The UK Office for
National Statistics undertakes a survey of those testing positive for COVID-19.[54] Individuals with the B.1.1.7
variant may be more likely to have a cough, sore throat, fatigue or myalgia (muscle aches) and may be less likely
to report loss of smell or taste (Figure 3). A separate study reported that patients may present on hospital
admission with hypoxia more often than non-B.1.1.7 cases.[55]
8COVID-19: Variants Update
Figure 3. Comparison of self-reported symptoms for B.1.1.7 (light green) and non-B.1.1.7 variant (dark green) (UK
Office of National Statistics)
Duration
Some studies have found B.1.1.7 to have an increased duration of infection. Daily longitudinal PCR tests were
performed on a cohort of 65 individuals to determine if B.1.1.7 was associated with longer duration of
infection.[56] Among seven participants infected with B.1.1.7, the mean overall duration of infection was 13.3
(95% CI: 10.1-16.5) days compared to 8.2 (95% CI: 6.5-9.7) days for 58 participants with non-B.1.1.7. While the
duration of infection was statistically significant, the small sample size should be noted and interpreted with
caution. A modelling study of publicly available sequencing data supported the hypothesis of B.1.1.7 having
increased duration of infection.[33]
A further study reported a statistically significant longer duration of RNA positivity in nasopharyngeal swabs of
16 days among 136 B.1.1.7 patients versus 14 days among 965 non-B.1.1.7 patients.[48] However, a study of
36,920 users of the COVID Symptom Study app reported no differences in the duration of symptoms associated
with B.1.1.7.[38]
Hospitalisation and mortality
Multiple large epidemiological studies have reported an increased risk of hospitalisation, intensive care
admissions, and mortality for the B.1.1.7 variant compared to previous variants.
Among a cohort of 198,420 patients, the adjusted hazard ratio for critical care admission was 1.99 (95% CI: 1.59-
2.49) for B.1.1.7 compared to non- B.1.1.7,[57] meaning those infected with the B.1.1.7 variant had almost
double the risk of critical care admission than those infected with previous variants. A large surveillance study in
seven countries of the European Union found that B.1.1.7 cases had 1.7 (95% CI: 1.0-2.9) times the risk of
hospitalisation and 2.3 (95% CI: 1.4-3.5) times the risk of intensive care admission compared to non-VOC
9COVID-19: Variants Update
cases.[58] Data from Denmark reported that the B.1.1.7 variant patients had a 64% increased risk of
hospitalisation compared to patients with previous variants.[59] Lastly, a matched cohort analysis of 2,821
B.1.1.7 cases matched to 2,821 non-B.1.1.7 cases in England from October to December 2020 reported a 34%
increased risk in hospitalisation associated with the B.1.1.7 variant compared to non-B.1.1.7 cases.[60] Several
analyses performed by the New and Emerging Respiratory Virus Threats Advisory Group (NERVTAG) concluded
infection with B.1.1.7 is associated with an increased risk of hospitalisation.[61]
Regarding mortality, there is substantial evidence of an increased risk of death for those infected with B.1.1.7
compared to previous variants. Using a database of over two million positive SARS-CoV-2 community tests and
17,452 COVID-19 deaths in England from 1 September 2020 to 14 February 2021, researchers estimated a
mortality hazard ratio of 1.6 (95% CI: 1.4-1.8), meaning a 60% increased risk of death associated with B.1.1.7
compared to previous variants.[62] A matched cohort study of 54,906 pairs estimated an increase of deaths
from 2.5 per 1,000 for non-B.1.1.7 cases to 4.1 per 1,000 for B.1.1.7 cases.[63] Additionally, several analyses by
NERVTAG estimated an increased risk of mortality between approximately 30-70% compared to the previous
variants.[61] In an adjusted analysis accounting for demographics and comorbidities, the risk of death for B.1.1.7
in England from 16 November 2020 through 5 February 2021 was two-thirds higher (hazard ratio 1.67; 95% CI:
1.34–2.09) compared with non-VOC.[64] However, in the same matched cohort of 2,821 B.1.1.7 cases described
above on risk of hospitalisation, there was no statistically significant difference in risk of death.
A study of only hospitalised patients in the UK reported no association of severe disease and death between
B.1.1.7 and non-B.1.1.7.[49] It is important to note that this study evaluates mortality given the patient is
already hospitalised and is therefore an evaluation of a cohort of patients with severe COVID-19. This suggests
that once a patient is admitted to hospital, with regard to mortality at least, the variant is not relevant.
B.1.1.7: Immunity, vaccines, and therapeutics
Laboratory data
Neutralising antibodies remain effective against the B.1.1.7 variant in preventing viral entry into host cells.[65-
68]
Laboratory studies with the Pfizer vaccine have shown a nearly identical antibody response and neutralising
titres against the B.1.1.7 lineage, supporting protection of the vaccine against B.1.1.7.[65, 69-74]
In a clinical trial of the AstraZeneca vaccine, laboratory virus neutralisation activity by vaccine-induced
antibodies was lower against the B.1.1.7 variant than against non-B.1.1.7 among 311 participants.[75]
Clinical data
Novavax[76] and Moderna[77, 78] reported good vaccine efficacy of their vaccines against the B.1.1.7 variant.
Johnson & Johnson/ Janssen did not report on vaccine efficacy with the B.1.1.7 variant specifically.[79]
A study assessing the real-world effectiveness of the Pfizer and AstraZeneca vaccines in the UK (where there is
widespread circulation of B.1.1.7) reported a single dose of either vaccine resulted in an 80% reduction of
hospitalisation.[80] A UK study of staff working in public hospitals found the Pfizer vaccine effectively prevented
both symptomatic and asymptomatic infection despite B.1.1.7 being prevalent.[81]
There is no evidence that suggests B.1.1.7 can evade immunity and cause breakthrough infections among those
fully vaccinated at a rate higher than previous variants.[75, 81, 82] Even with a very high estimated prevalence
10COVID-19: Variants Update
of 94.5% of B.1.1.7 in Israel, an analysis of national surveillance data reported high efficacy of the Pfizer vaccine
against infection, asymptomatic infection, and COVID-19 related hospitalisation and death.[83] In a real-world
analysis of the Pfizer vaccine in Qatar, vaccine efficacy was estimated to be 89.5% (95% CI: 85.9-92.3%) at 14 or
more days after the second dose.[84]
Therapeutics
B.1.1.7 can be efficiently neutralised by the monoclonal antibody treatment Bamlanivimab.[85]
B.1.1.7 with E484K mutation
B.1.1.7 with E484K mutation: transmissibility
As above with B.1.1.7 but contains the E484K mutation. The E484K mutation itself may,[65] or may not impact
affinity.[42]
B.1.1.7 with E484K mutation: clinical presentation and disease
severity
As above with B.1.1.7.
B.1.1.7 with E484K mutation: immunity, vaccines, and therapeutics
Multiple studies have reported a decrease in neutralisation activity against variants with E484K mutation.[17,
70, 78, 86, 87] This is important because VOC B.1.351 and P.1 also carry the E484K mutation.
The monoclonal antibody treatment Bamlanivimab may not provide protection against B.1.1.7 with E484K
mutation.[85]
B.1.351
B.1.351: Genomic characteristics
The B.1.351 is characterised by 17 mutations, with eight spike protein mutations D80A, D215G, 241/243
deletion, K417N, E484K, N501Y, D614G, and A701V (Figure 4).[88, 89]
Figure 4. Mutations of variant B.1.351(outbreak.info)
B.1.351: Transmissibility
Several of the mutations in B.1.351, specifically K417N, E484K, and N501Y, may affect the affinity for the spike
protein to bind to human host cells.
11COVID-19: Variants Update As noted under transmissibility of B.1.1.7, several studies have reported N501Y may increase affinity,[41-45] and when combined with K417N and E484K, studies have estimated between a 3-fold and 19-fold increase in affinity of the B.1.351 variant to bind to human host cells compared to other variants.[42, 43, 87] It is estimated that B.1.351 may be 1.5 (95% CI: 1.2-2.1) times as transmissible as previous variants.[90] B.1.351 was prevalent in a prospective surveillance study in Zimbabwe, accounting for 95% of sequences tested in January 2021.[91] Case reports suggest that reinfection with B.1.351 after prior infection is possible.[92] B.1.351: Clinical presentation and disease severity There is limited evidence for severity of disease for B.1.351. A large surveillance study of 23,343 samples across seven countries in the European Union found 436 B.1.351 cases. In this study, B.1.351 cases had 3.6 (95% CI: 2.1-6.2) times the odds of hospitalisation and 3.3 (95% CI: 1.9-5.7) times odds of intensive care admission compared to non-VOC cases. There was no evidence of association of B.1.351 with risk of death after adjusting for age, sex, and week of reporting, where the adjusted odds ratio was 1.1 (95% CI: 0.4-3.4).[58] However, the estimates of ICU admission were small (
COVID-19: Variants Update
the original vaccine. This is encouraging evidence that suggests vaccines can be altered to target multiple
variants, however, trials will continue, and real-world efficacy is still unavailable.[107]
Clinical data
Results from Novavax[76], Johnson & Johnson/Janssen[79] and Moderna[77, 78] provide strong evidence that
B.1.351 has the ability to evade vaccine-generated immunity to a significant degree.
Johnson & Johnson/Janssen presented data to the FDA on 26 February showing 94.5% of sequenced cases from
participants in South Africa were B.1.351, and vaccine efficacy for moderate to severe disease in South African
participants was 64.0% (95% CI 41.2-78.7%).[108] Data on the Novavax vaccine from a phase 2a/b, randomised
placebo-controlled trial in South Africa found that post-hoc vaccine efficacy in preventing mild to moderate
disease caused by B.1.351 was 51.0% (95% CI: -0.6-76.2%).[109]
The AstraZeneca vaccine had a vaccine efficacy of 10.4% (95% CI: -76.8-54.8%) against mild-to-moderate illness
associated with B.1.351 with onset >14 days after second injection.[110] In this same study, vaccine efficacy
against mild-to-moderate illness associated non-B.1.351 variants with onset >14 days after one dose was 75.4%
(95% CI: 8.9-95.5%). Sample sizes resulted in substantially large confidence intervals. The South African
government halted its rollout of the AstraZeneca vaccine following an analysis that it did not protect against
mild or moderate disease caused by the B.1.351 variant.[111] The World Health Organization has authorised the
AstraZeneca vaccine for emergency use through COVAX.[112]
A study from Israel noted breakthrough infections (i.e., being infected by SARS-CoV-2 after receiving a vaccine)
by variant B.1.351 among those vaccinated with the Pfizer vaccine.[82] However, this study is a pre-print and
there were only a total of nine B.1.351 cases in the study. Pfizer has begun evaluating a third dose that is
formulated based on the B.1.351 variant mutations.[113] In a real-world analysis of the Pfizer vaccine in Qatar,
vaccine efficacy was estimated to be 75% (95% CI: 70.5-78.9%) against B.1.351 at 14 or more days after the
second dose.[84]
Moderna has completed manufacturing of clinical trial material for its B.1.351 variant-specific vaccine candidate,
mRNA-1273.351. It has shipped doses to the National Institutes of Health (NIH) for a Phase 1 clinical trial that
will be led and funded by the NIH’s National Institute of Allergy and Infectious Diseases.[114]
Therapeutics
Monoclonal antibody treatments, including Bamlanivimab and Casirivimab, have been shown to be ineffective
against B.1.351. Studies have reported either partial neutralisation or no neutralisation.[68, 85, 87, 115-117]
The consensus is that escape from monoclonal antibody treatments is due to the E484K, K417N and N501Y
mutations.
P.1.
P.1: Genomic characteristics
The P.1 lineage is characterised by 22 mutations, with 12 spike protein mutations L18F, T20N, P26S, D138Y,
R190S, K417T, E484K, N501Y, D614G, H655Y, T1027I, and V1176F (Figure 5).[118] It is important to note that
E484K and N501Y spike mutations are present in both P.1 and B.1.351. Additionally, the B.1.351 variant contains
a K417N mutation, while P.1 is a K417T mutation, meaning an amino acid change occurred at the same location
13COVID-19: Variants Update in both variants, but the amino acid is different. The implications of the different amino acid between the two variants is unclear, but likely to be similar. Figure 5. Mutations of variant P.1 (outbreak.info) P.1: Transmissibility Some studies have found P.1 to be more transmissible. A modelling study fitting data from the Brazilian national health surveillance of hospitalised individuals in Manaus from December 2020 to February 2021, estimated the P.1 variant to be 2.6 (95% CI: 2.4–2.8) times more transmissible than previous variants.[119] Another modelling study estimates that P.1 is 1.7 to 2.4 times more transmissible than earlier variants.[120] The P.1 variant was found to have approximately a 10-fold higher viral load in upper respiratory tracts than non-P.1 infections, suggesting the P.1 variant is more transmissible.[121] However, given the scarcity of data and the number of assumptions that are required for modelling studies and limitations of real-world estimates, increased transmissibility for this variant is suspected but not well established. P.1: Clinical presentation and disease severity There is limited evidence for severity of disease for P.1. A large surveillance study of 23,343 samples, of which 352 were P.1 variant, across seven countries in the European Union found 2.6 (95% CI: 1.4-4.8) times the risk of hospitalisation and 2.2 (95% CI: 1.8-2.9) times the risk of intensive care admission compared to non-VOC. There was no association found between P.1 and risk of death, with an adjusted odds ratio of 0.6 (95% CI: 0.3-1.0).[58] However, estimates for ICU admission were small (
COVID-19: Variants Update
Alternative possibilities given for the resurgence were that the first wave was overestimated, that immunity
began to wane, or that the new P.1 variant evades immunity generated by previous infection. There have been
several case reports of individuals infected with P.1 after a previous COVID-19 infection.[129-131]
Clinical data
Developments will continue to be monitored and updated when information becomes available.
Therapeutics
Monoclonal antibody treatments such as Bamlanivimab and Casirivimab have been shown to be ineffective
against P.1. Studies have reported either partial neutralisation or no neutralisation by monoclonal antibody
treatments against the P.1 variant.[68, 85, 87, 115-117]
B.1.617.2
B.1.617.2: Genomic characteristics
The B.1.617.2 lineage is characterised by spike protein changes T19R, 156-158 deletion, L452R, T478K, D614G,
P681R, and D950N (Figure 6).[30] The L452R has been associated with increased transmissibility and a reduction
in neutralisation by convalescent plasma and some monoclonal antibody medicines [24]. The P681R mutation
could potentially have an effect on cell entry and infectivity, although this has not been demonstrated in
practice.[34]
Figure 6. Mutations of variant B.1.617.2 (outbreak.info)
B.1.617.2: Transmissibility
There is some evidence that B.1.617.2 may be more transmissible, however the evidence is still preliminary.
Public Health England have assessed B.1.617.2 to be at least as transmissible as B.1.1.7 with moderate
confidence, based on modelled growth estimates suggesting B.1.617.2 can compete with B.1.1.7 in the
population. However, the report also highlighted the need for further analyses to confirm this observation with
targeted comparator groups and improved correction for importation. This assessment was largely based on
B.1.617.2 sharing similar genetic mutations to B.1.1.7.[30] Preliminary analyses conducted by the WHO using
sequences submitted to GISAID suggests that B.1.617.1 and B.1.617.2 have a substantially higher growth rate
than other circulating variants in India, further suggesting potential increased transmissibility. However,
analyses from the European CDC warns that increased detection of B.1.617.2 in the UK may be related to
increased travel to and from India for religious or other large gatherings, and that the expansion within India is
within the context of a relaxation of non-pharmaceutical measures and low vaccination coverage. They argue
that targeted testing of arrivals from India to the UK and countries in the EU may have caused an
15COVID-19: Variants Update
overrepresentation of the B.1.617 variants and further data is needed to assess the true incidence and
transmissibility.[132]
Based on contact tracing data, the estimated secondary attack rate for B.1.617.2 among contacts who had
recently travelled was 3.3% (95% CI: 2.5-4.2%), which is higher than B.1.1.7 at 1.7% (95% CI: 1.6% - 1.8%).[30]
However, in travel settings the contacts reported are not restricted to only close contacts named by the case,
and may include contacts on a plane linked by additional contact tracing efforts. This is likely to lead to a
deflation of secondary attack rates amongst travellers. In addition, people who have recently travelled are
subject to stricter quarantine measures and may moderate their behaviour towards contacts. Among contacts
that had not travelled it was higher at 9.5% (95% CI: 5.9-14.9%), and therefore similar to secondary attack rates
for B.1.1.7.[30]
B.1.617.2: clinical presentation and disease severity
There are insufficient data currently to assess the potential for a change in disease severity.
Public Health England’s assessment highlights that the identified B.1.617.2 cases were still too recent to allow
enough time to assess its impact on disease severity in comparison to other co-circulating variants.[30]
B.1.617.2: immunity, vaccines, and therapeutics
There are insufficient data currently to assess the potential for immune escape.
Available evidence exists only for B.1.617.1, where serum from previously infected and vaccinated individuals
has been shown to neutralise B.1.617.1 equally, or more effectively than other currently circulating VOCs.[132]
16COVID-19: Variants Update
Glossary of Terms
The AstraZeneca vaccine AZD1222 or ChAdOx1
The Pfizer/BioNTech vaccine Comirnaty/BNT162b2
The ability of the virus to evade our body’s immune response. See also
Immune evasion
Immune response.
The response of our immune system to an infection. It includes
Immune response development of specific antibodies to the virus and also cell-mediated
responses (triggered by T cells).
An antibody produced by a single cell line and consisting of identical
Monoclonal antibody
antibody molecules. See also Immune response.
A type of drug that uses monoclonal antibody treatments to bind to
Monoclonal antibody medicine certain cells or proteins to stimulate the body’s immune system to attack
those cells/proteins. E.g., Bamlanivimab.
Small change made to the pattern of nucleotides that make up the virus.
Mutation These occur as the virus spreads and replicates. Most do not confer a
benefit to the virus.
Mutation nomenclature (i.e., how they are named), describes what
occurred at a specific location of the genome. For example, the ‘E484K’
Naming mutations mutation means that at the position 484, the amino acid changed from
glutamic acid (E) to lysine (K). When a deletion occurs, the location is
provided (e.g., deletion 144).
N-terminal domain Part of the spike protein of the SARS-CoV-2 virus.
The reproductive number, R0 (R-naught), indicates how contagious a
Reproductive number disease is in a vulnerable population; it is the average number of people
who will catch a disease from one person with the disease.
A ‘watery’ colourless component of blood in which red blood cells
Serum (plural Sera) (erythrocytes), white blood cells (leucocytes) and platelets are
suspended.
Having detectable antibodies against the virus as measured by a blood
Seropositive
(serological) test.
Viruses with mutations are referred to as variants of the original virus.
Variant New variants of SARS-CoV-2 have been emerging as the virus has spread
and evolved.
SARS-CoV-2 variants that are considered to have concerning
epidemiological, immunological or pathogenic properties are raised for
formal investigation by the New and Emerging Respiratory Virus Threats
Advisory Group (NERVTAG) in the UK. At this point the variants are
Variant of Concern (VOC)
designated Variant Under Investigation (VUI) with a year, month, and
number (since March 2021 2-number year & 3-letter month). Following
risk assessment with the relevant expert committee, they may be
designated Variant of Concern (VOC).
Variant under Investigation (VUI) See Variant of Concern
A disease of infection that can be transmitted from animals to humans.
Zoonosis (plural zoonoses)
There are over 200 known zoonoses.
17COVID-19: Variants Update
Abbreviations
CDC: Centers for Disease Control and Prevention
GSAID: Global Initiative on Sharing Avian Influenza Data
NERVTAG: New and Emerging Respiratory Virus Threats Advisory Group
RBD: Receptor binding domain (of the virus spike protein)
R0: R-naught, reproductive number
18COVID-19: Variants Update
References
1. McNally, A., What makes new variants of SARS-CoV-2 concerning is not where they come from, but the
mutations they contain. BMJ, 2021. 372: p. n504.
2. Lauring, A.S. and E.B. Hodcroft, Genetic Variants of SARS-CoV-2—What Do They Mean? JAMA, 2021.
325(6): p. 529-531.
3. Choi, B., et al., Persistence and Evolution of SARS-CoV-2 in an Immunocompromised Host. New England
Journal of Medicine, 2020. 383(23): p. 2291-2293.
4. Kemp, S.A., et al., SARS-CoV-2 evolution during treatment of chronic infection. Nature, 2021. 592(7853): p.
277-282.
5. Human Genome Variation Society. Sequence Variant Nomenclature, Version 20.05. [cited 2021 7 May];
Available from: http://varnomen.hgvs.org/.
6. Tang, J.W., et al., Introduction of the South African SARS-CoV-2 variant 501Y.V2 into the UK. The Journal of
infection, 2021. 82(4): p. e8-e10.
7. Public Health England (PHE). Investigation of novel SARS-CoV-2 variants of concern. Technical briefing
documents on novel SARS-CoV-2 variants. 01 April 2021 [cited 2021 06 April]; Available from:
https://www.gov.uk/government/publications/investigation-of-novel-sars-cov-2-variant-variant-of-
concern-20201201.
8. Public Health England (PHE). COVID-19 variants: genomically confirmed case numbers. 01 April 2021 [cited
2021 06 April]; Available from: https://www.gov.uk/government/publications/covid-19-variants-
genomically-confirmed-case-numbers.
9. Centers for Disease Control and Prevention (CDC). SARS-CoV-2 Variant Classifications and Definitions. 24
March 2021 [cited 2021 06 April]; Available from: https://www.cdc.gov/coronavirus/2019-ncov/cases-
updates/variant-surveillance/variant-info.html.
10. The Lancet, Genomic sequencing in pandemics. The Lancet, 2021. 397(10273): p. 445.
11. Helmy, M., M. Awad, and K.A. Mosa, Limited resources of genome sequencing in developing countries:
Challenges and solutions. Applied & Translational Genomics, 2016. 9: p. 15-19.
12. Billah, M.A., M.M. Miah, and M.N. Khan, Reproductive number of coronavirus: A systematic review and
meta-analysis based on global level evidence. PLOS ONE, 2020. 15(11): p. e0242128.
13. Centers for Disease Control and Prevention (CDC). COVID-19 Pandemic Planning Scenarios. 19 March 2021
[cited 2021 15 April]; Available from: https://www.cdc.gov/coronavirus/2019-ncov/hcp/planning-
scenarios.html.
14. Public Health England (PHE), SARS-CoV-2 variants of concern and variants under investigation in England:
Technical briefing 7. 2021.
15. Centers for Disease Control and Prevention (CDC). COVID Data Tracker: Variant Proportions. 2021 [cited
2021 16 April 2021]; Available from: https://covid.cdc.gov/covid-data-tracker/#variant-proportions.
16. Public Health England (PHE), Investigation of novel SARS-CoV-2 variant 202012/01: technical briefing 1.
2020.
17. Jangra, S., et al., SARS-CoV-2 spike E484K mutation reduces antibody neutralisation. The Lancet Microbe,
2021.
18. Bugembe, D.L., et al., A SARS-CoV-2 lineage A variant (A.23.1) with altered spike has emerged and is
dominating the current Uganda epidemic. medRxiv, 2021: p. 2021.02.08.21251393.
19. Alaa Abdel Latif, J.L.M., Manar Alkuzweny, Ginger Tsueng, Marco Cano, Emily Haag, Jerry Zhou, Mark
Zeller, Nate Matteson, Chunlei Wu, Kristian G. Andersen, Andrew I. Su, Karthik Gangavarapu, Laura D.
Hughes, and the Center for Viral Systems Biology. B.1.526 Lineage Report. 29 April 2021 [cited 2021 29
April]; Available from: https://outbreak.info/situation-reports?pango=B.1.526.
20. Republic of the Philippines Department of Health. Biosurveillance detects SARS-CoV-2 mutations; further
investigation needed to determine public health implication. 18 February 2021 [cited 2021 01 April];
Available from: https://doh.gov.ph/doh-press-release/BIOSURVEILLANCE-DETECTS-SARS-COV-2-
MUTATIONS-FURTHER-INVESTIGATION-NEEDED-TO-DETERMINE-PUBLIC-HEALTH-IMPLICATION.
19COVID-19: Variants Update
21. Tablizo, F.A., et al., Genome sequencing and analysis of an emergent SARS-CoV-2 variant characterized by
multiple spike protein mutations detected from the Central Visayas Region of the Philippines. medRxiv,
2021: p. 2021.03.03.21252812.
22. Áine O'Toole, E.S., Anthony Underwood, Ben Jackson, Verity Hill, JT McCrone, Chris Ruis, Khali Abu-Dahab,
Ben Taylor, Corin Yeats, Louis du Plessis, David Aanensen, Eddie Holmes, Oliver Pybus, Andrew Rambaut.
PAGNO lineages, Lineage P.3. [cited 2021 01 April]; Available from: https://cov-
lineages.org/lineages/lineage_P.3.html.
23. Public Health England (PHE), SARS-CoV-2 variants of concern and variants under investigation in England:
Technical briefing 8. 2021.
24. Deng, X., et al., Transmission, infectivity, and antibody neutralization of an emerging SARS-CoV-2 variant in
California carrying a L452R spike protein mutation. medRxiv, 2021: p. 2021.03.07.21252647.
25. Ministry of Health and Family Welfare India. Genome Sequencing by INSACOG shows variants of concern
and a Novel variant in India. 24 March 2021 [cited 2021 16 April]; Available from:
https://pib.gov.in/PressReleaseIframePage.aspx?PRID=1707177.
26. GISAID EpiCoV. Tracking of Variants, hcov19-variants. [cited 2021 12 May]; Available from:
https://www.gisaid.org/hcov19-variants/.
27. Hoffmann, M., et al., SARS-CoV-2 variant B.1.617 is resistant to Bamlanivimab and evades antibodies
induced by infection and vaccination. bioRxiv, 2021: p. 2021.05.04.442663.
28. Edara, V.-V., et al., Infection and vaccine-induced neutralizing antibody responses to the SARS-CoV-2
B.1.617.1 variant. bioRxiv, 2021: p. 2021.05.09.443299.
29. Ferreira, I., et al., SARS-CoV-2 B.1.617 emergence and sensitivity to vaccine-elicited antibodies. bioRxiv,
2021: p. 2021.05.08.443253.
30. Public Health England (PHE), SARS-CoV-2 variants of concern and variants under investigation in England:
Technical briefing 10. 2021.
31. Public Health England (PHE), SARS-CoV-2 variants of concern and variants under investigation in England:
Technical briefing 9. 2021.
32. Alaa Abdel Latif, J.L.M., Manar Alkuzweny, Ginger Tsueng, Marco Cano, Emily Haag, Jerry Zhou, Mark
Zeller, Nate Matteson, Chunlei Wu, Kristian G. Andersen, Andrew I. Su, Karthik Gangavarapu, Laura D.
Hughes, and the Center for Viral Systems Biology. B.1.1.7 Lineage Report. 22 April 2021 [cited 2021 22
April]; Available from: https://outbreak.info/situation-reports?pango=B.1.1.7.
33. Davies, N.G., et al., Estimated transmissibility and impact of SARS-CoV-2 lineage B.1.1.7 in England. Science,
2021: p. eabg3055.
34. Public Health England (PHE), Investigation of novel SARS-CoV-2 variant, Variant of Concern 202012/01:
Technical briefing 3. 2021: United Kingdom.
35. Washington, N.L., et al., Emergence and rapid transmission of SARS-CoV-2 B.1.1.7 in the United States. Cell,
2021.
36. Chen, C., et al., Quantification of the spread of SARS-CoV-2 variant B.1.1.7 in Switzerland. medRxiv, 2021: p.
2021.03.05.21252520.
37. Piantham, C. and K. Ito, Estimating the increased transmissibility of the B.1.1.7 strain over previously
circulating strains in England using fractions of GISAID sequences and the distribution of serial intervals.
medRxiv, 2021: p. 2021.03.17.21253775.
38. Graham, M.S., et al., Changes in symptomatology, reinfection, and transmissibility associated with the
SARS-CoV-2 variant B.1.1.7: an ecological study. The Lancet Public Health, 2021.
39. Munitz, A., et al., BNT162b2 Vaccination Effectively Prevents the Rapid Rise of SARS-CoV-2 Variant B.1.1.7
in high risk populations in Israel. Cell Reports Medicine, 2021: p. 100264.
40. Volz, E., et al., Assessing transmissibility of SARS-CoV-2 lineage B.1.1.7 in England. Nature, 2021.
41. Hu, J., et al., Emerging SARS-CoV-2 variants reduce neutralization sensitivity to convalescent sera and
monoclonal antibodies. Cellular & molecular immunology, 2021: p. 1-3.
42. Laffeber, C., et al., Experimental evidence for enhanced receptor binding by rapidly spreading SARS-CoV-2
variants. bioRxiv, 2021: p. 2021.02.22.432357.
43. Ramanathan, M., et al., SARS-CoV-2 B.1.1.7 and B.1.351 Spike variants bind human ACE2 with increased
affinity. bioRxiv, 2021: p. 2021.02.22.432359.
20COVID-19: Variants Update
44. Rambaut, A., Loman, N., Pybus, O., Barclay, W., Barrett, J., Carabelli, A., Connor, T., Peacock, T., Robertson,
D. L., Volz, E., . Preliminary genomic characterisation of an emergent SARS-CoV-2 lineage in the UK defined
by a novel set of spike mutations. 2020; Available from: https://virological.org/t/preliminary-genomic-
characterisation-of-an-emergent-sars-cov-2-lineage-in-the-uk-defined-by-a-novel-set-of-spike-
mutations/563.
45. Dicken, S.J., et al., Characterisation of B.1.1.7 and Pangolin coronavirus spike provides insights on the
evolutionary trajectory of SARS-CoV-2. bioRxiv, 2021: p. 2021.03.22.436468.
46. Borges, V., et al., Tracking SARS-CoV-2 lineage B.1.1.7 dissemination: insights from nationwide spike gene
target failure (SGTF) and spike gene late detection (SGTL) data, Portugal, week 49 2020 to week 3 2021.
Eurosurveillance, 2021. 26(10): p. 2100131.
47. Kidd, M., et al., S-variant SARS-CoV-2 lineage B1.1.7 is associated with significantly higher viral loads in
samples tested by ThermoFisher TaqPath RT-qPCR. The Journal of Infectious Diseases, 2021.
48. Calistri, P., et al., Infection sustained by lineage B.1.1.7 of SARS-CoV-2 is characterised by longer persistence
and higher viral RNA loads in nasopharyngeal swabs. International Journal of Infectious Diseases, 2021.
49. Frampton, D., et al., Genomic characteristics and clinical effect of the emergent SARS-CoV-2 B.1.1.7 lineage
in London, UK: a whole-genome sequencing and hospital-based cohort study. Lancet Infect Dis, 2021.
50. Walker, A.S., et al., Increased infections, but not viral burden, with a new SARS-CoV-2 variant. medRxiv,
2021: p. 2021.01.13.21249721.
51. Brown, J.C., et al., Increased transmission of SARS-CoV-2 lineage B.1.1.7 (VOC 2020212/01) is not accounted
for by a replicative advantage in primary airway cells or antibody escape. bioRxiv, 2021: p.
2021.02.24.432576.
52. Smith, T.P., et al., Environmental drivers of SARS-CoV-2 lineage B.1.1.7 transmission in England, October to
December 2020. medRxiv, 2021: p. 2021.03.09.21253242.
53. Kifer, D., et al., Effects of Environmental Factors on Severity and Mortality of COVID-19. Frontiers in
Medicine, 2021. 7: p. 1088.
54. Office for National Statistics UK. Coronavirus (COVID-19) Infection Survey: characteristics of people testing
positive for COVID-19 in England, 27 January 2021. 27 January 2021 [cited 2021 4 May 2021]; Available
from:
https://www.ons.gov.uk/peoplepopulationandcommunity/healthandsocialcare/conditionsanddiseases/arti
cles/coronaviruscovid19infectionsinthecommunityinengland/characteristicsofpeopletestingpositiveforcovi
d19inengland27january2021.
55. Snell, L.B., et al., First and second SARS-CoV-2 waves in inner London: A comparison of admission
characteristics and the effects of the B.1.1.7 variant. medRxiv, 2021: p. 2021.03.16.21253377.
56. Kissler, S.M., et al., Densely sampled viral trajectories suggest longer duration of acute infection with
B.1.1.7 variant relative to non-B.1.1.7 SARS-CoV-2. medRxiv, 2021: p. 2021.02.16.21251535.
57. Patone, M., et al., Analysis of severe outcomes associated with the SARS-CoV-2 Variant of Concern
202012/01 in England using ICNARC Case Mix Programme and QResearch databases. medRxiv, 2021: p.
2021.03.11.21253364.
58. Funk, T., et al., Characteristics of SARS-CoV-2 variants of concern B.1.1.7, B.1.351 or P.1: data from seven
EU/EEA countries, weeks 38/2020 to 10/2021. Eurosurveillance, 2021. 26(16): p. 2100348.
59. Bager, P.a.W., Jan and Fonager, Jannik and Albertsen, Mads and Yssing Michaelsen, Thomas and Holten
Møller, Camilla and Ethelberg, Steen and Legarth, Rebecca and Fischer Button, Mia Sara and Gubbels,
Sophie Madeleine and Voldstedlund, Marianne and Mølbak, Kåre and Skov, Robert Leo and Fomsgaard,
Anders and Grove Krause, Tyra, Increased Risk of Hospitalisation Associated with Infection with SARS-CoV-2
Lineage B.1.1.7 in Denmark. Lancet Preprints, 2021.
60. Dabrera, G., et al., Assessment of Mortality and Hospital Admissions Associated with Confirmed Infection
with SARS-CoV-2 Variant of Concern VOC-202012/01 (B.1.1.7) a Matched Cohort and Time-to-Event
Analysis. SSRN, 2021.
61. New and Emerging Respiratory Virus Threats Advisory Group (NERVTAG). NERVTAG: Update note on
B.1.1.7 severity - 11 February 2021. Research and analysis 2021 11 February 2021; Available from:
https://assets.publishing.service.gov.uk/government/uploads/system/uploads/attachment_data/file/9610
42/S1095_NERVTAG_update_note_on_B.1.1.7_severity_20210211.pdf.
21COVID-19: Variants Update
62. Davies, N.G., et al., Increased mortality in community-tested cases of SARS-CoV-2 lineage B.1.1.7. Nature,
2021.
63. Challen, R., et al., Risk of mortality in patients infected with SARS-CoV-2 variant of concern 202012/1:
matched cohort study. BMJ, 2021. 372: p. n579.
64. Grint, D.J., et al., Case fatality risk of the SARS-CoV-2 variant of concern B.1.1.7 in England, 16 November to
5 February. Eurosurveillance, 2021. 26(11): p. 2100256.
65. Wang, P., et al., Antibody Resistance of SARS-CoV-2 Variants B.1.351 and B.1.1.7. Nature, 2021.
66. Greaney, A.J., et al., Comprehensive mapping of mutations in the SARS-CoV-2 receptor-binding domain that
affect recognition by polyclonal human plasma antibodies. Cell Host & Microbe, 2021. 29(3): p. 463-476.e6.
67. Rees-Spear, C., et al., The effect of spike mutations on SARS-CoV-2 neutralization. Cell Reports, 2021.
34(12): p. 108890.
68. Hoffmann, M., et al., SARS-CoV-2 variants B.1.351 and P.1 escape from neutralizing antibodies. Cell, 2021.
184(9): p. 2384-2393.e12.
69. Edara, V.V., et al., Neutralizing Antibodies Against SARS-CoV-2 Variants After Infection and Vaccination.
JAMA, 2021.
70. Collier, D.A., et al., Sensitivity of SARS-CoV-2 B.1.1.7 to mRNA vaccine-elicited antibodies. Nature, 2021.
71. Trinité, B., et al., Previous SARS-CoV-2 infection increases B.1.1.7 cross-neutralization by vaccinated
individuals. bioRxiv, 2021: p. 2021.03.05.433800.
72. Marot, S., et al., Neutralization heterogeneity of United Kingdom and South-African SARS-CoV-2 variants in
BNT162b2-vaccinated or convalescent COVID-19 healthcare workers. bioRxiv, 2021: p. 2021.03.05.434089.
73. Becker, M., et al., Immune response to SARS-CoV-2 variants of concern in vaccinated individuals. medRxiv,
2021: p. 2021.03.08.21252958.
74. Muik, A., et al., Neutralization of SARS-CoV-2 lineage B.1.1.7 pseudovirus by BNT162b2 vaccine–elicited
human sera. Science, 2021. 371(6534): p. 1152.
75. Emary, K.R.W., et al., Efficacy of ChAdOx1 nCoV-19 (AZD1222) vaccine against SARS-CoV-2 variant of
concern 202012/01 (B.1.1.7): an exploratory analysis of a randomised controlled trial. The Lancet, 2021.
76. Novavax. Novavax COVID-19 vaccine demonstrates 89.3% efficacy in UK Phase 3 trial. [ Press Release. ]
2021 January 28, 2021.; Available from: https://ir.novavax.com/news-releases/news-release-
details/novavax-covid-19-vaccine-demonstrates-893-efficacy-uk-phase-3.
77. Moderna, COVID-19 Vaccine Retains Neutralizing Activity Against Emerging Variants First Identified in the
U.K. and the Republic of South Africa. . 2021.
78. Wu, K., et al., Serum Neutralizing Activity Elicited by mRNA-1273 Vaccine — Preliminary Report. New
England Journal of Medicine, 2021.
79. Johnson, J., Johnson & Johnson Announces Single-Shot Janssen COVID-19 Vaccine Candidate Met Primary
Endpoints in Interim Analysis of its Phase 3 ENSEMBLE Trial. 2021.
80. Lopez Bernal, J., et al., Early effectiveness of COVID-19 vaccination with BNT162b2 mRNA vaccine and
ChAdOx1 adenovirus vector vaccine on symptomatic disease, hospitalisations and mortality in older adults
in England. medRxiv, 2021: p. 2021.03.01.21252652.
81. Hall, V., Foulkes, S., Saei, A., Andrews, N., Oguti, B., Charlett, A., et al.,, Effectiveness of BNT162b2 mRNA
Vaccine Against Infection and COVID-19 Vaccine Coverage in Healthcare Workers in England, Multicentre
Prospective Cohort Study (the SIREN Study). . The Lancet, 2021.
82. Kustin, T., et al., Evidence for increased breakthrough rates of SARS-CoV-2 variants of concern in BNT162b2
mRNA vaccinated individuals. medRxiv, 2021: p. 2021.04.06.21254882.
83. Haas, E.J., et al., Impact and effectiveness of mRNA BNT162b2 vaccine against SARS-CoV-2 infections and
COVID-19 cases, hospitalisations, and deaths following a nationwide vaccination campaign in Israel: an
observational study using national surveillance data. The Lancet.
84. Abu-Raddad, L.J., H. Chemaitelly, and A.A. Butt, Effectiveness of the BNT162b2 Covid-19 Vaccine against
the B.1.1.7 and B.1.351 Variants. New England Journal of Medicine, 2021.
85. Widera, M., et al., Bamlanivimab does not neutralize two SARS-CoV-2 variants carrying E484K in vitro.
medRxiv, 2021: p. 2021.02.24.21252372.
86. Wibmer, C.K., et al., SARS-CoV-2 501Y.V2 escapes neutralization by South African COVID-19 donor plasma.
Nature Medicine, 2021.
22You can also read