Mycobacterial disease in cats in Great Britain: I. Culture results, geographical distribution and clinical presentation of 339 cases
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
Journal of Feline Medicine and Surgery (2011) 13, 934e944
doi:10.1016/j.jfms.2011.07.012
Mycobacterial disease in cats in Great Britain:
I. Culture results, geographical distribution
and clinical presentation of 339 cases
Danièlle A Gunn-Moore BSc, BVM&S, PhD, MACVSc, MRCVS, RCVS Specialist in Feline Medicine1*,
Sarah E McFarland BVM&S, MRCVS1,a, Jacqueline I Brewer2,
Timothy R Crawshaw BVetMed, MSc3, Richard S Clifton-Hadley MA, VetMB, PhD, MSc, MRCVS2,
Marcel Kovalik Dr VetMed, PhD, MRCVS1, Darren J Shaw BSc, PhD1
1
Royal (Dick) School of Veterinary This study investigated 339 cases of feline mycobacterial disease from cats with
Studies and the Roslin Institute, cutaneous lesions or masses found at exploratory laparotomy. Tissue samples
Division of Clinical Veterinary were submitted to the Veterinary Laboratories Agency for mycobacterial culture
Sciences, The University of over a 4-year period to December 2008. The study assessed which species of
Edinburgh, Easter Bush Veterinary culturable mycobacteria were involved, where the cats lived, and their clinical
Centre, Roslin, Midlothian, presentation (physical findings, serum biochemistry, radiography, feline
Scotland EH25 9RG, UK leukaemia virus and feline immunodeficiency virus status). Mycobacterium
2
VLA Weybridge, New Haw, microti was cultured from 19%, Mycobacterium bovis 15%, Mycobacterium avium
Addlestone, Surrey KT15 3NB, UK 7%, non-M avium non-tuberculous mycobacteria 6%, with no growth in 53% of
3
VLA Starcross, Staplake Mount, samples. M microti, M bovis and M avium were found in almost mutually
Starcross, Exeter EX6 8PE, UK exclusive clusters within Great Britain (GB) (ie, M bovis in South-West England/
Wales/Welsh Border, M avium in eastern England and M microti south of London
and in South-West Scotland). While differences were seen in the clinical
presentation and distribution of lesions caused by the different infections, these
were not sufficiently different to be diagnostic. Cats commonly presented with
single or multiple cutaneous lesions (74%), which were sometimes ulcerated or
discharging, located most frequently on the head (54%). Lymph nodes were
usually involved (47%); typically the submandibular nodes. Systemic or
pulmonary signs were rarely seen (10e16%). When a cat is suspected of having
mycobacteriosis, accurate identification of the species involved helps to
determine appropriate action. Our findings show that knowing the cat’s
geographic location can be helpful, while the nature of the clinical presentation is
less useful. Most cases of feline mycobacterial disease in GB are cutaneous.
Date accepted: 16 July 2011 Ó 2011 ISFM and AAFP. Published by Elsevier Ltd. All rights reserved.
M
ycobacterial infections are recognised as tuberculosis (typically caused by Mycobacterium
a global health concern, both in humans bovis or Mycobacterium microti), feline leprosy
and other animals.1e3 One species that is (Mycobacterium lepraemurium, and other similar
known to be infected by a number of different myco- bacteria), and non-tuberculous mycobacteriosis
bacteria is the domestic cat. Unfortunately, many as- caused by non-tuberculous mycobacteria (NTM)
pects of mycobacterial infections in this species (Mycobacterium fortuitum, Mycobacterium aviume
remain unknown; there have been few recently pub- intracellulare complex [MAC], and others).5e14 In the
lished research papers on feline mycobacteriosis in UK, the majority of recently reported cases of feline
general, and even fewer on feline tuberculosis in mycobacterial disease have been primarily cutaneous
particular.4 in nature and they presented with nodules, draining
Mycobacterial disease in the domestic cat can tracts, ulceration and local lymphadenopathy.4 Where
result in several different syndromes including systemic disease is seen, infection with a member of
the tuberculosis group or a MAC organism is most
*Corresponding author. Tel/Fax: þ44-0131-650-7650. E-mail: likely8,15 although occasional cases have been seen
danielle.gunn-moore@ed.ac.uk with other NTM.16
a
Present address: Marbacher Weg, 52, Marburg 35037, Germany.
1098-612X/11/120934+11 $36.00/0 Ó 2011 ISFM and AAFP. Published by Elsevier Ltd. All rights reserved.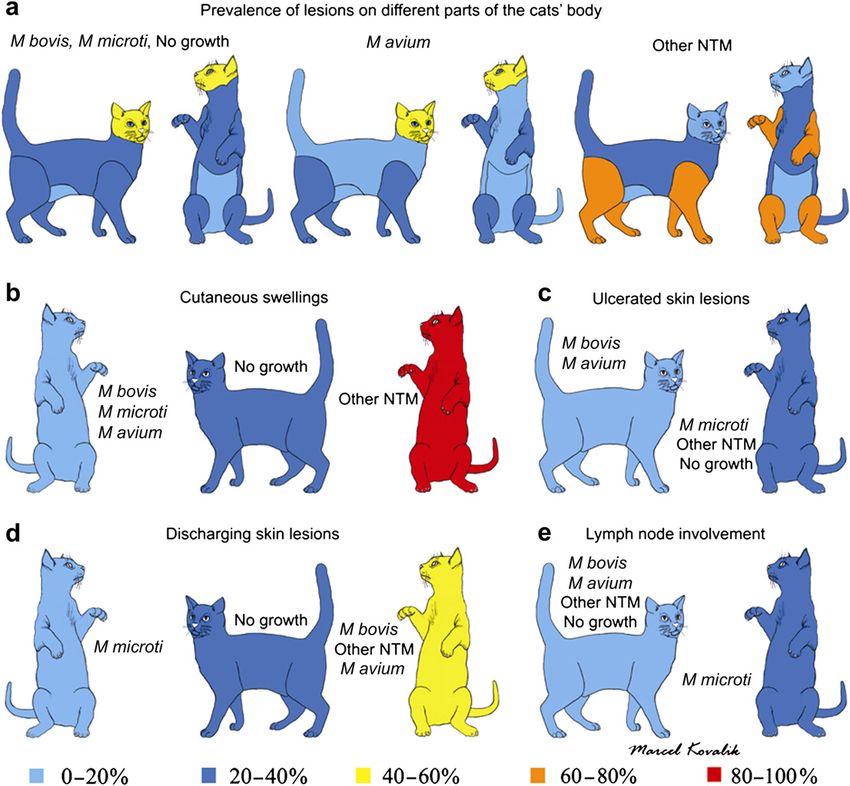
Mycobacterial disease in cats in Great Britain 935
Cats may become infected via a number of different histopathology the tissue was found to have lesions sug-
routes. Historically, tuberculosis in cats resulted from gestive of mycobacterial infection with typical granulo-
the ingestion of tuberculous milk and was seen as matous or pyogranulomatous inflammation, consisting
gastrointestinal disease.17e19 However, following the in- of multifocal to coalescent infiltration with large num-
troduction of pasteurisation of milk and tuberculous bers of foamy macrophages containing variable num-
testing of cattle, gastrointestinal disease is now a rare bers of acid-fast bacilli. The veterinary surgeons then
presentation and most cases affect the skin, at least ini- took a second sample and submitted it without fixation
tially, but may later spread to the lungs.4 The current ep- to the VLA for mycobacterial culture.
idemiology of feline tuberculosis is unclear but infection Veterinary surgeons that submitted the samples to the
could occur through a number of possible routes. Direct VLA were contacted by one of the authors (SMcF) and
spread from wild rodents has been suggested because asked to provide information on where the cat lived
hunting rodents has been shown to be a risk factor for tu- (ie, the postcode of the owner’s house), plus the cat’s sig-
berculosis in cats13,15 and some small mammal species in nalment (age, breed, gender) and its clinical presentation
the UK are naturally infected with either M microti20,21 or including the diagnostics that had been performed to as-
M bovis.22,23 Direct spread of M bovis from badgers fol- sess possible systemic involvement (serum biochemistry,
lowing interspecific aggression is also possible. Alterna- radiography, feline leukaemia virus and feline immuno-
tively, M bovis-infected cattle and badgers could cause deficiency virus [FeLV/FIV] status). Information on the
environmental contamination24 and cutaneous wounds histopathological findings, treatment (surgery, drugs
on cats (eg, from fighting) could become secondarily in- given, and duration of treatment) and eventual outcome
fected. This latter method of infection is also believed to are presented in the accompanying paper.27 In some cases
occur with feline leprosy which arises from contami- the requested information was incomplete or not avail-
nated rodent bites or following soil or plant contamina- able so where data were missing the number of samples
tion of cutaneous wounds.4,5,7,9,10 As NTM are typically included in the analysis has been noted. Complete post-
found in soil, water and decaying vegetation, NTM in- codes, where available, were converted into Ordinance
fections are also believed to be secondary to wound con- Survey eastings and northings. For incomplete postcodes
tamination.6,11,12,25 (For DEFRA Guidance notes on (ie, information only available up to postcode district
tuberculosis in cats go to: CatsTBbriefing (VIPER23 level), the average easting and northing for the postcode
App Y5)_March 08 update.doc.) district was taken.
Given the paucity of our knowledge about the nature
of current feline mycobacterial infections in Great Brit- Statistical analyses
ain (GB), the primary aims of this study were to use
the exceptional number of feline mycobacterial cases Geographical Information System (GIS) analyses incor-
collected by the Veterinary Laboratories Agency (VLA) porating the SaTScan (v7.0.3 www.satscan.org) statistic
to determine which mycobacterial species are present were carried out to ascertain whether there were any sta-
in cats in GB and where they occur, and how these infec- tistically significant clusters of samples that could be cul-
tions most commonly present. Knowing which bacteria tured and whether the different cultured species
are present permits determination of which cases are ap- clustered in particular parts of GB. Two groups of factors
propriate to treat, which are more likely to respond to were considered for analyses: (i) signalment and (ii) clin-
treatment and how best to tailor the treatment protocols. ical presentation. For each group standard univariate lo-
In addition, it is particularly important to identify cats gistic regression risk factor analysis was performed to
infected with M bovis and M microti as these have the see whether particular factors were associated with
most significant potential zoonotic risk. As culture can whether culture and classification of the sample was
take up to three months13 and access to molecular diag- possible. In addition, odds ratio (OR) and associated
nostics is currently still limited and is expensive, the sec- 95% confidence interval (CI) were calculated. The cul-
ondary aim of the study was to determine if analysis of ture results were divided into four groups: (i) M bovis,
the data could enable prediction of which mycobacterial (ii) M microti, (iii) NTM and (iv) no growth, and Fisher
species is present based on a cat’s geographical location exact tests were carried out to identify any association
within GB and its clinical presentation. with the signalment or clinical presentation. The NTM
group was also divided further into M avium and non-
M avium NTM for some of the comparisons. In all cases,
Materials and methods statistical significance was set at P < 0.05.
Tissue samples
Between January 2005 and December 2008, 339 feline Results
samples were submitted to the VLA Weybridge by vet-
erinary surgeons in GB for mycobacterial culture.26 Mycobacterial species identified and the
The samples came from cats that had been found to
geographical location of the infected cats
have cutaneous lesions or suspicious masses at explor-
atory laparotomy, and when formalin-fixed samples Table 1 summarises the culture results obtained for the
were sent to private pathology laboratories for 339 samples. Mycobacteria could be cultured from 159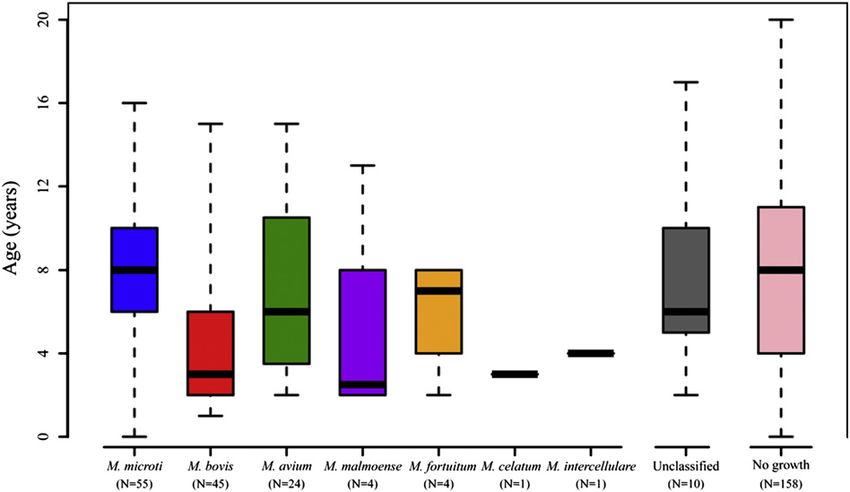
936 DA Gunn-Moore et al
(47%: 95% CI 41e52) of the samples. Of these 159 sam-
Table 1. Mycobacterial culture results. The samples ples, three species made up 87% of the isolates (M mi-
had histopathological changes indicative of myco- croti: 40%, M bovis: 33% and M avium: 15%, Table 1).
bacterial infection and were submitted to the Veteri- Complete postcodes were available for 277 samples
nary Laboratories Agency for mycobacterial culture and incomplete postcodes for 49 samples, with no
between January 2005 and December 2008. postcode available for 13 samples. SaTScan analysis
Culture results Number Percentage (%) of the 326 samples with complete or incomplete post-
of cultured codes revealed that there were no apparent clusters in
terms of being able to culture a sample (P ¼ 0.544,
M microti 63 39.6 Fig 1a). The samples with no postcode information
M bovis 52 32.7 were two M bovis and 11 no growth.
Non-tuberculous mycobacteria (NTM) The spatial distribution for the M microti samples and
M avium 24 15.1 some of the M bovis samples have already been pub-
M malmoense 4 2.5 lished by Smith et al,13 who focused on M microti-posi-
M fortuitum 4 2.5 tive samples from cats collected by the VLA over the
M celatum 1 0.6 last 14 years, and they found there were two areas where
M intracellulare 1 0.6 M microti dominated; Northern England/Southern Scot-
Unclassified 10 6.3 land and Southern England (Fig 1b). The current
SaTScan analysis identified two smaller more well de-
Cultured total 159 fined M microti clusters within these areas; one south
No growth 180 of London and the other in South-West Scotland
Grand total 339 (P < 0.015). All of the 10 culture-positive samples in
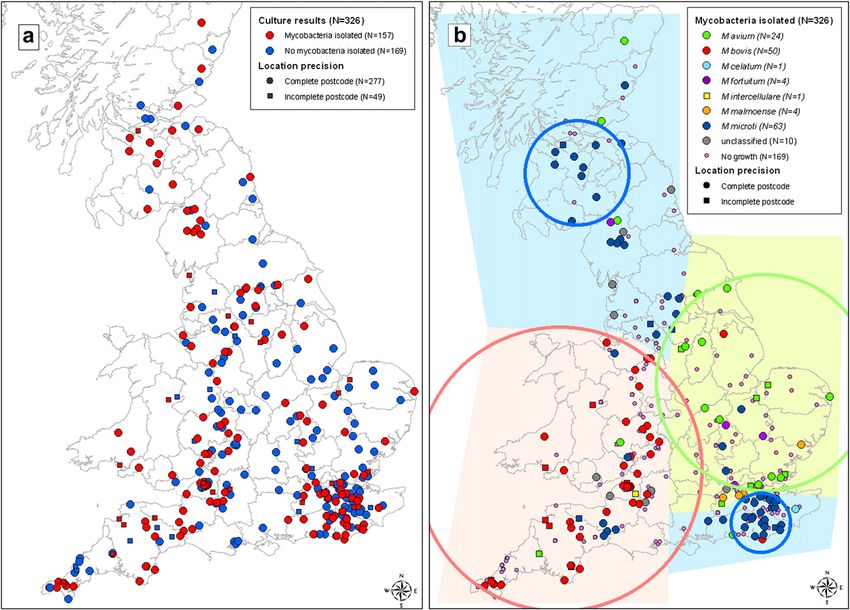
Fig 1. Map of GB showing the location of 326 feline samples obtained between January 2005 and December 2008 for which
the VLA tried to culture mycobacteria. (a) Samples have been subdivided into samples that could (red symbols) and could
not be cultured (blue symbols). (b) Samples which could be cultured were subdivided into either the Mycobacteria species
isolated or as unclassified mycobacteria. Also indicated is whether the position on the maps is from a complete postcode
(C) or the mean easting and northing of the postcode district (-). The coloured shaded areas correspond to predominance
by one Mycobacteria species and the coloured circles the spatial clusters identified by the SaTScan analysis.Mycobacterial disease in cats in Great Britain 937
the Scottish cluster were M microti, and all but one of the presumed to have outdoor access as they had a history
28 culture-positive samples in the south of London clus- suggestive of this, with yearly administration of vac-
ter were M microti, with the other cultured sample being cines, regular flea and worming treatment and/or treat-
the M bovis isolate described below. While there were ment for cat bite abscesses. Only 2% of the cats were
four M microti culture-positive samples apparently reported as living exclusively indoors.
tightly clustered together in Cumbria this cluster was Table 2 summarises the univariate analyses of the re-
not identified as statistically significant by the SaTScan lationships between being able to culture mycobacteria
analysis, nor were they included in the Southern Scot- from the sample and the signalment of the cat. The only
land cluster. The two other main Mycobacteria species statistically significant relationship was with age, with
also separated into quite distinct areas in GB (Fig 1b). a decrease in the odds of having a positive culture in-
This was confirmed by the SaTScan analysis that identi- creasing with age (OR (years) 0.93 (0.88e0.98)). If the
fied a large M bovis cluster in South-West England/ different species of mycobacteria were considered
Wales/Welsh Border (P < 0.001), with all but two of then differences in the age distributions of cats were ob-
the 50 M bovis samples (where location was known) be- served (Fig 2), with M bovis samples coming from sig-
ing within this cluster, and M bovis samples comprising nificantly younger cats than those with M microti or
76% (95% CI 63e86) of the cultured samples within the where no bacteria could be grown (P < 0.001). No sig-
cluster. One of the M bovis isolates outwith the main nificant variation was observed in the percentage of
cluster coincides with a reported M bovis cluster in cattle (i) males (58e65%, P ¼ 0.934), (ii) neutered cats
in Sussex.28 The other M bovis isolate outwith the cluster (92e100%, P ¼ 0.318), (iii) DSH/DLH (76e93%,
is from a cat reported in Lincolnshire. This cat was a stray P ¼ 0.071), or (iv) known to be outdoor cats
cat handed into the local Cats Protection centre with no (96e100%, P ¼ 0.720) when the samples were divided
previous history available. Finally, there was a large into the different Mycobacteria species identified.
M avium cluster in Eastern England (Fig 1b), with 66%
(44e84) of the Mycobacteria species culture-positive sam-
ples in the cluster being M avium (P < 0.001). Clinical presentation
Lumps and lesions were the most common presenting
Case signalment and risk factors
signs (85%, Table 3), with 74% of cases presenting with
Male cats constituted 61% of the samples (Table 2), with cutaneous lesions (where the location of the lumps/le-
93% of cats having been neutered (92% male, 94% sions was reported). Lumps/lesions were the sole pre-
female). Eighty-three percent of the cats were either do- senting sign in 59% of the cats. The most common
mestic shorthair (DSH) or domestic longhair (DLH). The localisation of the lumps/lesions was on the head
remaining breeds identified were Siamese (n ¼ 18), Bur- (54%), but they were also seen all over the body. Multiple
mese (five), Bengal (three), British Shorthair (BSH) lesions were present in almost half of the cats. For the
(three), Persian (three), Maine Coon (two), Abyssinian 145 cats for which descriptions of the lumps/lesions
(one), Burmilla (one), Oriental (one), Russian (one) and were available there was no single predominate descrip-
Ragdoll (one) cats. Sixty-five percent of the cats were tion, with ulceration, discharge and bite wound/abscess
known to have outdoor access, and a further 33% were being roughly equal in occurrence (26e35%).
Table 2. Summary of the recording and occurrence (number [N], prevalence and 95% exact binomial
confidence intervals [CI]) of signalment factors (age, gender, neutered status, whether they were DSH/
DLH cats, and whether they had outdoor access).*
Risk factor N Positive % P value OR (95% CI)
Age 302 0.011 0.93 (0.88e0.98)
Sex ¼ male 289 175 60.6 (54.6e66.2) 0.802 1.06 (0.66e1.70)
Status ¼ meutered 258 241 93.4 (89.6e96.1) 0.326 0.60 (0.21e1.67)
DSH/DLH ¼ yes 303 250 82.5 (77.7e86.6) 0.310 1.36 (0.75e2.49)
Cat ¼ known outdoor access 168 109 64.9 (57.1e72.1) 0.357 1.35 (0.71e2.54)
Cat ¼ known plus presumed outdoor accessy 168 164 97.6 (94.0e99.3) 0.981 1.02 (0.14e7.45)
*Signalment data were not available in all cases with the age of 37 cats, the gender of 50, the neutered status of 81, and
the breed of 50 cats being unknown. Also included is the statistical significance (Wald P value) and OR (and 95% CI)
for these factors associated with mycobacterium being grown from the samples. For the continuous variable (age),
the OR refers to the change in odds for an increase in age of 1 year, for the remaining categorical variables the
odds of the second category relative to the first category for each factor.
y
Where it could not be confirmed that a cat had outdoors access, its file was assessed for a history suggestive of
outdoor access, including the administration of yearly vaccines, regular flea and worming treatment and/or treat-
ment for cat bite abscesses.938 DA Gunn-Moore et al Fig 2. Boxplot of the age distribution (in years) associated with the particular mycobacteria isolated. Horizontal thick lines indicate the median age, boxes indicate the interquartile range and whiskers the range. Also included is the number of iso- lates of each particular Mycobacterium species for which the age of the cat was identified. Lymph node involvement was noted in 49% of cases in the percentage of samples with any of the presenting (where it was possible to determine whether lymph no- conditions (P > 0.097). That said, there was variation be- des were involved), with submandibular lymph nodes tween some of the groups for some of the findings, for affected most commonly (29%, Table 3). However, in example, the percentage of samples where lumps/le- 12% of the cats multiple lymph nodes were affected e sions were observed on the head (P ¼ 0.036), with with a combination of submandibular and other pe- NTM having a lower percentage (31%) compared to M ripheral lymph nodes (typically the pre-scapular no- bovis (52%) or M microti (62%) and no growth (55%) des) the most common multiple site combination in (Fig 3). The same was not true for lumps/lesions ob- 18/27 cases. Internal lymph node involvement was re- served either on limbs or the body (P > 0.112). The per- corded in only 12% of the cases. centage of samples with multiple lesions also differed Having lumps/lesions as a presenting sign was not between the four groups (P ¼ 0.002), with M microti hav- associated with being able to culture mycobacteria ing a much higher percentage (70%), compared to M bo- from the sample, either if considering lumps/lesions vis (34%), NTM (30%) and no growth (46%). There was as the sole presenting condition or where there was little variation in the percentage of samples in all but more than one presenting condition (P > 0.266, one of the descriptions of the lumps/lesions Table 3). Furthermore, there was no association between (P > 0.123). The exception was a much lower percentage being able to culture mycobacteria and the description of M microti samples (16%) having a discharging lesion of the lesion, its location, or whether multiple or single (34e52%, P ¼ 0.026) (Fig 3). There was also marked var- lesions were observed (P > 0.219). The only presenting iation in the percentage of samples where the lymph no- sign that was associated with being able to culture my- des were thought to be involved (P ¼ 0.004), ranging cobacteria was weight loss, but this was not a strong as- from 73% of M bovis samples to 39% with no growth sociation (P ¼ 0.041, OR 2.01 (1.03e3.93)), with 63% of (Fig 3). If just whether the submandibular lymph nodes the samples from cats that presented with weight loss were involved was analysed, there was little difference being able to be cultured, compared to 46% of the sam- between M bovis (41%) and M microti (46%), but the other ples from cats that did not present with weight loss. two groups had much lower percentages (17e22%, A stronger association was observed with whether P ¼ 0.005). Finally, internal lymph node involvement lymph nodes were involved, (P ¼ 0.004, OR 2.19 was more likely with M bovis and M avium (21% and (1.28e3.75)); with 61% of samples from cats where 27%, respectively). This was also reported, but to a lower lymph nodes were involved being able to be cultured, degree, with M microti (4/45 cases; 9%) and cases with compared to 42% of samples from cats where lymph no- no growth (9/106 cases; 8.5%), but it was not reported des were not involved. This association was also ob- in any of the cats with non-M avium NTM. served if just submandibular or other peripheral lymph nodes were considered, though the associations Diagnostics tests were much weaker (P < 0.036). If the culture results were divided into which myco- Further diagnostic tests were performed in some of the bacterial species could be grown (M bovis, M microti, cases to determine if the cats were concurrently in- NTM, or no growth) there was little overall difference fected with FeLV and/or FIV and to see if there was
Mycobacterial disease in cats in Great Britain 939
Table 3. As for Table 2, but for information about clinical presentation. Presenting signs were not available
for 57 cases.
N Positive % P value OR (95% CI)
Presenting information available 282
Lame 270 16 5.9 (3.4e9.4) 0.181 0.48 (0.16e1.41)
Ocular 271 18 6.6 (3.9e10.3) 0.757 0.86 (0.33e2.25)
Respiratory 272 28 10.3 (6.9e14.5) 0.846 0.93 (0.42e2.03)
Weight loss 272 43 15.8 (11.6e20.7) 0.041 2.01 (1.03e3.93)
Off colour 272 44 16.2 (12.0e21.1) 0.058 1.89 (0.98e3.67)
Lumps/lesions (LL) 281 240 85.4 (80.7e89.3) 0.266 0.68 (0.35e1.33)
LL only presenting condition 167 59.4 (53.4e65.2) 0.538 0.86 (0.54e1.39)
(a) LL location
Head 228 124 54.4 (47.6e61.0) 0.308 0.77 (0.47e1.27)
Limbs 226 70 31 (25.0e37.4) 0.974 1.01 (0.59e1.72)
Body 223 60 26.9 (21.2e33.2) 0.264 1.38 (0.78e2.45)
Not cutaneous 224
Abdomen 20 8.9 (5.5e13.5) e e
Eye 8 3.6 (1.5e6.9) e e
Oropharynx/throat 2 0.9 (0.11e3.2) e e
Oedema 1 0.4 (0.01e2.5) e e
(b) Multiple lesions 227 106 46.7 (40.0e53.4) 0.866 1.05 (0.62e1.76)
(c) LL description 145
Bite wound/abscess 39 26.9 (19.8e34.9) 0.568 1.24 (0.59e2.59)
Ulcerated 38 26.2 (19.2e34.2) 0.251 0.64 (0.30e1.37)
Discharging 51 35.2 (27.4e43.5) 0.691 1.15 (0.58e2.28)
Swelling 30 20.7 (14.4e28.2) 0.551 0.78 (0.34e1.77)
Lymph node 15 10.3 (5.9e16.5) 0.219 1.98 (0.67e5.89)
Nodular 6 4.2 (1.5e8.8) e e
Lymph nodes involved 223 109 48.9 (42.1e55.6) 0.004 2.19 (1.28e3.75)
Submandibular lymph nodes 220 64 29.1 (23.1e35.6) 0.035 1.89 (1.04e3.44)
Other peripheral lymph nodes 218 51 23.4 (17.9e29.6) 0.031 2.04 (1.07e0.91)
Internal lymph nodes 220 26 11.8 (7.8e16.8) 0.145 1.89 (0.80e4.44)
e ¼ No logistic regression analysis performed.
evidence of systemic dissemination of mycobacterial Discussion
infection. Seventy-two cats were tested for FIV/FELV, This paper (and its sister paper focussing on histopa-
of which two were positive for FIV. Blood calcium con- thology, treatment and outcome27) reports on the
centration was only assessed in 39 cats, and was ele- largest study of feline mycobacterial disease reported
vated in nine (calcium concentration up to to date. The largest previous studies looked at 179
3.95 mmol/l; reference interval 2.00e2.95 mmol/l). Of cases of feline leprosy from New Zealand;29 52 cases
these nine cats, four had systemic disease and three of M bovis from the US;30 49 cases of NTM from Aus-
had respiratory disease (all of which had M microti); tralia;6 101 cases of M microti from GB;13 and 10 cases
while M fortuitum was cultured from one cat with ex- of M avium from Australia and the US.8 From GB, the
tensive cutaneous disease overlying its thorax (and previous largest studies of M bovis infection included
concurrent sternal lymph node involvement); and the 1317 and 12 cases,31 and 43 cases where the focus was
ninth case involved the inguinal fat pads but the bacte- purely on the regional distribution.13 Analysis of the
ria failed to grow. Thirty-six of 72 cats that had chest unique data set available in the current study has
radiographs taken were found to have pulmonary pa- generated some fascinating results. These relate to
thology, but this was not associated with increased the frequency with which different mycobacterial
odds of successful culture (P ¼ 0.633, OR 1.26 species cause disease in cats in GB, their geographi-
(0.49e3.21)). Nor was there any association between cal distribution, and their clinical presentation.
which mycobacterium was isolated and the percentage The study revealed which culturable mycobacterial
of chest radiographs with pathology (P ¼ 0.319) M bovis species are currently causing disease in cats in GB.
50%, M microti 67%, 3/8 NTM (two of which were Mycobacterium microti and M bovis are responsible for
M avium), and 14/30 with no growth. similar levels of infection, and between them they940 DA Gunn-Moore et al Fig 3. Pictorial representations of the (a) prevalence of lesions due to the different infections on different parts of the cats’ body, (b) the overall prevalence of cutaneous lesions, and whether they were (c) ulcerated or (d) discharging lesions, and (e) whether there was lymph node involvement. account for a third of the submitted cases. While there The data in the current study was also divided into have been few recently reported cases of feline tubercu- four groups so that the two most important infections losis, those that have been published were also caused (M microti and M bovis) could be clearly defined, and by either M microti or M bovis, or they quote or present then compared to the more heterogeneous NTM and VLA data.4,13,15,31e33 No cases of Mycobacterium tubercu- the no-growth group. Since successful culture of M bovis losis were identified, probably because cats are thought can take up to two months and M microti can take up to to be naturally resistant to this infection,18,34 in addition three months13 and access to molecular diagnostics is to which this infection is now much less prevalent in currently still limited and expensive, one aim of the the human population of GB.35 Importantly, our find- study was to determine if it was possible to predict ings confirm that M microti is a significant pathogen which mycobacterial species was present based on the of cats in GB.13,15,36 Confusingly, M microti infection cat’s geographical location within GB and its clinical in cats was previously termed M microti-like as it was presentation. unclear at the time that it was actually the same organ- Analysis of the postcode data showed that when ism.15,37,38 In addition, some reports have discussed a cat’s location was mapped within GB there was cases where the infection was reported to be M tubercu- marked clustering of the three most significant infec- losis39 or M tuberculosis var bovis,15,40 which on further tions. The two M microti clusters have previously been investigation appear to have been M microti. The cur- reported by Smith et al13 with one cluster south of Lon- rent study isolated M avium less frequently than don and the other in Northern England/Southern Scot- M microti or M bovis and this is in agreement with cur- land (Fig 1b). In addition, most of the isolates found in rent literature where few cases of this infection have South-West England/Wales/Welsh Border were M bovis been reported in cats.8,41e43 (Fig 1b). This confirms the reported spatial distribution
Mycobacterial disease in cats in Great Britain 941 from Smith et al13 which was based on a smaller sub-set cutaneous lumps or lesions (74%), which were some- of the current M bovis data. However, there was also times ulcerated or discharging, and most frequently lo- a M avium cluster e where isolates were predominately cated on the head (54%), and multiple lesions were found in Eastern England. Interestingly, where clusters found in 47% of cases. When looking at the different in- were identified other species of mycobacteria tended fections, NTM were the least likely to cause lesions on to be absent.13 This suggests that knowing a cat’s loca- the head (31% compared to 52e60% for the other tion can be useful in suggesting which infections are groups) (Fig 3). The presence of multiple lesions differed more likely, for example, if a cat is seen in Scotland, it between the groups, being more common with M microti is unlikely to have M bovis (unless it has moved from (70%), compared to the other groups (30e46%). Having a high risk area). a discharging lesion also varied between groups, as it It is unclear exactly how the cats are becoming in- was less likely for M microti (16%) compared to the other fected with M bovis and M microti. While the current groups (34e52%) (Fig 3). Lymph nodes were frequently study could not determine if the cats came from urban involved (49%); most typically the submandibular and/ and non-urban regions, the majority (98%) were pre- or other peripheral lymph nodes; with lymph node in- sumed to be outdoor cats from the information obtained volvement being very common with M bovis (73%) from their veterinary surgeons. The previous study on and less common with the no-growth cases (39%). a larger set of VLA M microti isolates, suggested that When submandibular lymph node involvement was an- cats with M microti infection were more likely to come alysed M bovis (41%) and M microti (46%) were similar, from extra-urban areas.13 This supports the hypothesis and in both groups this was more likely than for the that these infections are probably gained when the cats other two groups (17e22%). These findings support are outside their homes, most probably in their garden the theory that most cases of mycobacterial infections territories. Cats could become infected by a number of in cats in GB are seen as cutaneous lesions affecting different routes. These include hunting small rodents ‘fight and bite sites’ and/or presenting as submandibu- (infected with either M microti or M bovis), interspecific lar lymphadenopathy. aggression with badgers (infected with M bovis), and/ It has previously been reported that systemic involve- or following environmental contamination, for example, ment is more likely with infection by a member of the tu- M bovis being shed by badgers that have domestic gar- berculosis group or a MAC organism;8,15 with only dens as part of their territory.4,44 The current study find- occasional cases been caused by other NTM.16 There- ing that most (74%) of the cats had cutaneous lesions at fore, it was hoped that the presence of systemic disease ‘fight and bite sites’ correlates well with this theory. would be a useful indicator of M microti, M bovis, or What role cats may have in the onward transmission M avium infections and it would make a diagnosis of of these mycobacteria is unknown. non-M avium NTM less likely. In support of this, internal The study supports previous findings that in GB cases lymph node involvement was found more frequently of reported mycobacterial disease typically occurs in with M bovis and M avium (21% and 27%, respectively) adult cats (mean age 7.2 years; 95% CI 6.7e7.7), that and, to a lesser extent, M microti (4/45 cases; 9%) and are neutered (93%), male (61%), and non-pedigree cases with no growth (9/106 cases; 8.5%). Importantly, (83%), and have outdoor access (98%).4 While all but it was not reported in any of the cats with non-M avium two of the cats were over a year of age, the mean age NTM. This was also supported when looking at the of the cats with the different infections did vary, as cases where chest radiographs were taken; the percent- cats with M bovis infection had a mean of three years age of cases which showed pathology consistent with of age, compared to eight years of age for M microti mycobacterial infection was 67% with M microti, 50% (Fig 2). The percentage of cats with known outdoor ac- with M bovis, 47% with no growth, and 3/8 (38%) with cess was similar to that for most domestic cats in GB NTM (two of these were caused by M avium and the (98%).45 This was also the case for the percentage of third was unclassified). Overall, the current study sup- non-pedigree cats as approximately 90% of pet cats in ports the assumption that non-M avium NTM are less the GB are non-pedigree (Pet Food Manufacturers’ As- likely to spread systemically than other mycobacterial sociation [PFMA] Annual Report 2004). However, cats infections; however, it also shows that systemic infec- with M microti were slightly more likely to be pedigree tions can still be caused by these bacteria. (24% pedigree cats) than the cats with the other infec- Cats with systemic involvement are believed to have tions. The Siamese breed may be over-represented in a poorer prognosis and may be more resistant to the current study as 18/39 pedigree cats were Siamese, treatment.5,7e9,12,15,46 Because of this it is important to as- while this breed is only the second most popular cat sess each cat for possible systemic spread. At presenta- breed in GB (General Council of the Cat Fancy tion, systemic signs (such as weight loss, involvement [GCCF], data from 2008; www.gccf.org). Interestingly, of internal lymph nodes and/or respiratory disease) while previous papers have suggested that Siamese were seen in only 10e16% of cases. No cats were FeLV cats may be predisposed to MAC infections,46e48 none positive and only 2/72 cats tested were FIV positive. As of the Siamese cats in the current study were found to discussed above, where chest radiographs were taken have this infection. (possibly because of a suspicion of pulmonary involve- Where the information was reported, the cats in this ment) pulmonary pathology was seen most commonly study most commonly presented with single or multiple with M microti cases, to a lesser extent with M bovis and
942 DA Gunn-Moore et al
no-growth cases, and least frequently with NTM. Where different from that of all the samples that could
blood calcium concentration was assessed (again, possi- be cultured. This could suggest that many of the
bly because of suspicion of systemic involvement) hyper- no-growth samples were NTM. However, false
calcaemia was found in 9/39 (23%) cases; seven of which negative results could also have occurred, with
were infected with M microti and had systemic or pulmo- the failure to culture M bovis or M microti resulting
nary disease, and two had extensive cutaneous disease from the paucity of organisms and/or, reduced vi-
(one caused by M fortuitum and one from which myco- ability of organisms due to recent antimicrobial
bacteria could not be grown). Hypercalcaemia has previ- treatment or decomposition of the sample.
ously been reported in only four cats with mycobacterial (i) NTM: When looking at the non-M avium NTM,
disease, all of which had systemic M avium infection.8 four cats with Mycobacterium malmoense came
This study adds to our understanding of hypercalcaemia from the same part of England, as did 3/4 cats
associated with mycobacterial infection as this has not with M fortuitum. While this is an interesting ob-
previously been documented in so many cats, in cats servation, care should be taken not to over-
with M microti or M fortuitum infections, or in cats with interpret this as the numbers involved are small.
only cutaneous (albeit extensive) disease. These data The cats in the NTM group were generally similar
show that evidence of systemic spread of mycobacterial to the cats in the three other groups. However,
infection was not uncommon. Unfortunately, when re- they tended to have multiple lesions less fre-
viewing the presentation data, no group of cats was quently than the other groups (30% compared to
found to be significantly more likely to have either pul- 34e70%), which affected the head less frequently
monary and/or systemic involvement, although, they than other groups (30% compared to 52e60%),
tended to occur less frequently when infection was and there was slightly less lymph node involve-
caused by the non-M avium NTM. ment than with M bovis and M microti (46% com-
Overall, by reviewing the data, the different infec- pared to 57% with M microti and 73% with
tions were found to be associated with slightly differ- M bovis). When considering only the cats with
ing patient and disease profiles (Fig 3): M avium infection, they tended to be located in
eastern England, had a median age of six years,
and had an increased risk of internal lymph
1. M microti: Cats with M microti infections were most node involvement (27% of M avium cases had in-
typically from South-West Scotland and Northern ternal lymph node involvement, compared to
England or south of London,13 with a median age 21% of M bovis cases, 9% of M microti cases, 8%
of eight years. They were slightly more likely to be of no-growth cases). This is in contrast to the rest
pedigree cats (24% pedigree cats) than those with of the NTM (after removal of the M avium cases),
M bovis 7% or NTM 12%, and they usually had mul- where none of the cases had systemic lymph
tiple lesions (70%), particularly on the head (60%), node involvement. One footnote to the current
which were typically non-discharging (only 16% study is that Mycobacterium celatum is reported in
had discharging lesions), and submandibular lymph this study for the first time in a cat. The cat was
nodes were involved in 46% of cases. While only 39 a 3-year-old neutered female cat from Kent with
cats were assessed for serum total calcium concen- a 2-year history of pyrexia and recurrent full-
tration nine were found to have elevated levels, thickness punctuate lesions over her dorsum and
and seven of these had M microti infections, which right thigh that oozed seropurulent material.
in each case involved either pulmonary and/or sys- (ii) No-growth group: The cats in this group had similar
temic infection. clinical presentations to the other groups, although
2. M bovis: Cats with M bovis infections were typically peripheral or systemic lymph node involvement
from the South-West England/Wales/Welsh Bor- was less typical. Peripheral lymphadenopathy was
der (in agreement with reference13) with a median only seen in 39% of cases (compared to 73% with
age of three years. They were unlikely to be pedi- M bovis) and internal lymphadenopathy was only
gree cats (93% DSH/DLH), and they more typically seen in 8% of cases (compared to 21% with M bovis
had single lesions (only 34% had multiple lesions), and 27% with M avium).
which were on the head (52%) more frequently
than anywhere else. Lymph nodes were frequently
affected (73%), with the submandibular lymph no- Interestingly, the cats in the no-growth group were
des being involved in 41% of cases. statistically older than the cats with M bovis; although
3. NTM and no-growth groups: This data is more there was no difference between them and the cats
difficult to interpret because the culture system with M microti. The increased likelihood of gaining
used by the VLA has been optimised to detect M a positive culture from samples from younger cats could
bovis, and is, therefore, not ideal for detecting perhaps result from the younger cats having a less effec-
many species of NTM. Therefore, in addition to tive immune response and so being more permissive for
the NTM that did grow, others may have been mycobacterial growth, as has previously been hypoth-
contained in the no-growth group. The spatial dis- esised.10,49 This could, in turn, result in higher bacterial
tribution of the no-growth samples was no numbers and a greater chance of a positive culture.Mycobacterial disease in cats in Great Britain 943
Clearly, there are a number of caveats to this study. location of the cat can be very helpful in this respect,
These include: (i) being unable to accurately define the nature of the clinical signs helps less. Since culture
the population from which the cases came (see below), takes up to three months and is frequently unsuccessful,
(ii) having to rely on clinical files for case data some of we recommend concurrent use of molecular diagnostics
which was sometimes absent, (iii) using a culture sys- (such as polymerase chain reaction and sequencing) and
tem that is optimised for M bovis and (iv) not having further development of cat specific assays (such as the
the resources to undertake molecular diagnostics to interferon (IFN)-gamma test), as these can result
identify which bacteria were involved in the cases in more precise and faster identification of the
where the mycobacteria did not grow in culture. The mycobacteria.
prevalence of mycobacterial infections in cats in GB re-
mains unclear because we were unable to accurately
define the population to which these cases belong.
This is because a large number of steps have to be
Acknowledgements
taken before a sample is submitted to the VLA. These Thank you to all of the veterinary surgeons, nurses
include: the lesions have to be large enough for the and reception staff who helped in this study. The
owner to notice and/or the cat needs to be sufficiently VLA cultures and histopathology were funded by
ill, the owner has to be able to afford to take their cat to DEFRA under the project SB4510.
a veterinary surgeon, the veterinary surgeon has to
send the sample off to a diagnostic laboratory for histo-
pathology, the laboratory has to recommend that the References
primary clinician collect a second sample and send it 1. Glaziou P, Floyd K, Raviglione M. Global burden and epi-
to the VLA for culture, the cat has to have another le- demiology of tuberculosis. Clin Chest Med 2009; 30: 621e36.
sion suitable for biopsy, and the owner has to be will- 2. Lobue PA, Enarson DA, Thoen CO. Tuberculosis in hu-
ing to pay for the repeat procedure. Unfortunately, mans and animals: an overview. Int J Tuberc Lung Dis
2010; 14: 1075e8.
few veterinary surgeons have mycobacterial infections
3. Shiloh MU, DiGiuseppe Champion PA. To catch a killer.
on their differential diagnosis list when they collect the What can mycobacterial models teach us about Mycobac-
primary sample so it is only when the diagnostic labo- terium tuberculosis pathogenesis? Curr Opin Microbiol
ratory reports their findings that the veterinary surgeon 2010; 13: 86e92.
knows they need a fresh sample for culture. Ideally, 4. Gunn-Moore DA. Mycobacterial infections in cats and
when a veterinary surgeon takes a biopsy from a suspi- dogs. In: Ettinger S, Feldman E, eds. Textbook of veteri-
cious lesion or an enlarged lymph node, they would nary internal medicine. 7th edn. Philadelphia: WB Saun-
section it and send one sample for histopathology ders, 2010: 875e81.
and store the second sample in the freezer pending 5. McIntosh DW. Feline leprosy: a review of forty-four
the histopathology result. Despite these caveats, this cases from Western Canada. Can Vet J 1982; 23: 291e5.
6. Malik R, Wigney DI, Dawson D, Martin P, Hunt GB, Love
study is the largest study of feline mycobacteriosis
DN. Infection of the subcutis and skin of cats with rapidly
ever published and it has produced some fascinating growing mycobacteria: a review of microbiological and
results. clinical findings. J Feline Med Surg 2000; 2: 35e48.
In conclusion, this large study looking at 339 cases of 7. Malik R, Hughes MS, James G, et al. Feline leprosy: two dif-
feline mycobacterial infection was able to show which ferent clinical syndromes. J Feline Med Surg 2002; 4: 43e59.
species of mycobacteria most commonly cause disease 8. Baral RM, Metcalfe SS, Krockenberger MB, et al. Dissem-
in cats in GB, geographically where the infected cats inated Mycobacterium avium infection in young cats:
are most likely to live, and how M microti and M bovis in- over-representation of Abyssinian cats. J Feline Med
fections occur in almost mutually exclusive spoligotype Surg 2006; 8: 23e44.
clusters (and see Smith et al13). The study found 9. Greene CE, Gunn-Moore DA. Infections with slow-
growing mycobacteria. In: Greene CE, ed. Infectious dis-
M microti in 19% of reported cases, with M bovis in
eases of the dog and cat. 3rd edn. St Louis: Saunders,
15%, M avium in 7%, non-M avium NTM in 6%, and no Elsevier, 2006: 462e77.
growth in 53%. While there were some differences be- 10. Malik R, Hughes MS, Martin P, Wigney D. Feline leprosy
tween the patterns of disease caused by the different my- syndromes. In: Greene CE, ed. Infectious diseases of the
cobacterial species, these were not diagnostic, and dog and cat. 3rd edn. St Louis, Missouri: Saunders,
regardless of the mycobacteria involved, affected cats Elsevier, 2006: 477e80.
most commonly presented with single or multiple cuta- 11. Malik R, Martin P, Wigney D, Foster S. Infections caused
neous lumps or lesions, which were sometimes ulcer- by rapidly growing mycobacteria. In: Greene CE, ed. In-
ated or discharging, and most frequently found on the fectious diseases of the dog and cat. 3rd edn. St Louis,
head. Lymph nodes were usually involved; most typi- Missouri: Saunders, Elsevier, 2006: 482e8.
12. Horne KS, Kunkle GA. Clinical outcome of cutaneous
cally the submandibular nodes. Therefore, clinical signs
rapidly growing mycobacterial infections in cats in the
and lesion distribution are useful at suggesting that a di- south-eastern United States: a review of 10 cases
agnosis of mycobacterial infection should be considered. (1996e2006). J Feline Med Surg 2009; 11: 627e32.
However, accurate identification of the species involved 13. Smith NH, Crawshaw T, Parry J, Birtles RJ. Mycobacte-
is needed to determine the appropriate course of action. rium microti: more diverse than previously thought.
Our findings show that while knowing the geographic J Clin Microbiol 2009; 47: 2551e9.944 DA Gunn-Moore et al
14. Gunn-Moore DA, Dean R, Shaw S. Mycobacterial infec- 31. Monies B, Jahans K, de la Rua R. Bovine tuberculosis in
tions in cats and dogs. In Pract 2010; 32: 444e52. cats. Vet Rec 2006; 158: 245e6.
15. Gunn-Moore DA, Jenkins PA, Lucke VM. Feline tubercu- 32. Gunn-Moore D, Shaw S. Mycobacterial disease in the
losis: a literature review and discussion of 19 cases cat. In Pract 1997; 19: 493e501.
caused by an unusual mycobacterial variant. Vet Rec 33. Anon. Animal Health 2007: The report of the Chief
1996; 138: 53e8. Veterinary Officer. London: DEFRA Publications 2008:
16. Couto SS, de Bolla GJ, Artacho CA. Mycobacterium fortui- 34e40, http://www.defra.gov.uk/animals/cvo/report.
tum pneumonia in a cat and the role of lipid in the patho- htm (accessed Nov 11, 2008).
genesis of atypical mycobacterial infections. Vet Pathol 34. Aranaz A, Liébana E, Pickering X, Novoa C, Mateos A,
2007; 44: 543e6. Domı́nguez L. Use of polymerase chain reaction in the
17. Jennings AR. The distribution of tuberculous lesions in diagnosis of tuberculosis in cats and dogs. Vet Rec
the dog and cat, with reference to the pathogenesis. Vet 1996; 138: 276e80.
Rec 1949; 27: 380e4. 35. Grange JM, Gandy M, Farmer P, Zumla A. Historical de-
18. Smith JE. Symposium on diseases of cats e III. Some path- clines in tuberculosis: nature, nurture and the biosocial
ogenic bacteria of cats with special reference to their public model. Int J Tuberc Lung Dis 2001; 5: 208e12.
health significance. J Small Anim Pract 1965; 5: 517e24. 36. Rüfenacht S, Bögli-Stuber K, Bodmer T, Bornand Jaunin
19. Parodi A, Fontaine M, Brion A, Tisseur H, Goret P. My- VF, Gonin Jmaa DC, Gunn-Moore DA. Mycobacterium
cobacterioses in the domestic carnivora e present day microti infection in the cat: a case report, literature review
epidemiology of tuberculosis in the cat and dog. and recent clinical experience. J Feline Med Surg 2011; 13:
J Small Anim Pract 1966; 6: 309e17. 195e204.
20. Cavanagh R, Begon M, Bennett M, et al. Mycobacterium 37. de Bolla GJ. Tuberculosis in a cat. Vet Rec 1994; 134: 336.
microti infection (vole tuberculosis) in wild rodent popu- 38. Blunden AS, Smith KC. A pathological study of a myco-
lations. J Clin Microbiol 2002; 40: 3281e5. bacterial infection in a cat caused by a variant with cul-
21. Burthe S, Bennett M, Kipar A, et al. Tuberculosis tural characteristics between Mycobacterium tuberculosis
(Mycobacterium microti) in wild field vole populations. and M bovis. Vet Rec 1996; 138: 87e8.
Parasitology 2008; 135: 309e17. 39. Kipar A, Schiller I, Baumgärtner W. Immunopathological
22. Delahay RJ, De Leeuw AN, Barlow AM, Clifton-Hadley studies on feline cutaneous and (muco)cutaneous myco-
RS, Cheeseman CL. The status of Mycobacterium bovis in- bacteriosis. Vet Immunol Immunopathol 2003; 91: 169e82.
fection in UK wild mammals: a review. Vet J 2002; 164: 40. Orr CM, Kelly DF, Lucke VM. Tuberculosis in cats. A re-
90e105. port of two cases. J Small Anim Pract 1980; 21: 247e53.
23. Delahay RJ, Smith GC, Barlow AM, et al. Bovine tuber- 41. Gow AG. What is your diagnosis? Mycobacterial infec-
culosis infection in wild mammals in the South-West tion. J Small Anim Pract 2006; 47: 484e5.
region of England: a survey of prevalence and a semi- 42. de Groot PH, van Ingen J, de Zwaan R, Mulder A, Boeree
quantitative assessment of the relative risks to cattle. MJ, van Soolingen D. Disseminated Mycobacterium avium
Vet J 2007; 173: 287e301. subsp avium infection in a cat, the Netherlands.
24. Biet F, Boschiroli ML, Thorel MF, Guilloteau LA. Zoonotic Vet Microbiol 2010; 144: 527e9.
aspects of Mycobacterium bovis and Mycobacterium aviume 43. Rivière D, Pingret JL, Etievant M, et al. Disseminated
intracellulare complex (MAC). Vet Res 2005; 36: 411e36. Mycobacterium avium subspecies infection in a cat. J Feline
25. Jang SS, Hirsh DC. Rapidly growing members of the ge- Med Surg 2011; 13: 125e8.
nus Mycobacterium affecting dogs and cats. J Am Anim 44. Monies RJ, Cranwell MP, Palmer N, Inwald J, Hewinson
Hosp Assoc 2002; 38: 217e20. RG, Rule B. Bovine tuberculosis in domestic cats. Vet Rec
26. Daniel R, Evans H, Rolfe S, et al. Outbreak of tuberculo- 2000; 146: 407e8.
sis caused by Mycobacterium bovis in golden Guernsey 45. Murray JK, Roberts MA, Whitmarsh A, Gruffydd-Jones
goats in Great Britain. Vet Rec 2009; 165: 335e42. TJ. Survey of the characteristics of cats owned by house-
27. Gunn-Moore DA, McFarland S, Brewer J, et al. Mycobac- holds in the UK and factors affecting their neutered sta-
terial disease in cats in Great Britain: II. Histopathology, tus. Vet Rec 2009; 164: 137e41.
treatment and outcome of 339 cases. J Feline Med Surg 46. Hix JW, Jones TC, Karlson AG. Avian tubercle bacillus
2011; 13: 945e52. infection in a cat. J Am Vet Med Assoc 1961; 138: 641e7.
28. Green LE, Cornell SJ. Investigations of cattle herd break- 47. Drolet R. Disseminated tuberculosis caused by Mycobacte-
downs with bovine tuberculosis in four counties of rium avium in a cat. J Am Vet Med Assoc 1986; 189: 1336e7.
England and Wales using VETNET data. Prev Vet Med 48. Jordan HL, Cohn LA, Armstrong PJ. Disseminated
2005; 70: 293e311. Mycobacterium avium complex infection in three Siamese
29. Thompson EJ, Little PB, Cordes DO. Observations of cat cats. J Am Vet Med Assoc 1994; 204: 90e3.
leprosy. N Z Vet J 1979; 27: 233e5. 49. Gross TL, Ihrke PJ, Walder EJ, Affolter VK. Infectious
30. Snider WR, Cohen D, Reif JS, Stein SC, Prier JE. Tubercu- nodular and diffuse granulomatous and pyogranuloma-
losis in canine and feline populations. Study of high risk tous diseases of the dermis. Skin disease of dog and cat:
populations in Pennsylvania, 1966e1968. Am Rev Respir clinical and histopathological diagnosis. 2nd edn.
Dis 1971; 104: 866e76. St Louis: Mosby Year Book, 2005: 272e340.
Available online at www.sciencedirect.comYou can also read