T cell responses in patients with - COVID-19 - Nature
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
Progress
typically occurs for only 2–4 days around
T cell responses in patients with symptom onset and rapidly recovers15.
By contrast, COVID-19-associated
lymphopenia may be more severe or
COVID-19 persistent than in these other infections and
seems to be more selective for T cell lineages.
It is possible that the peripheral lymphopenia
Zeyu Chen and E. John Wherry
observed in patients with COVID-19 reflects
Abstract | The role of T cells in the resolution or exacerbation of COVID-19, as well recruitment of lymphocytes to the respiratory
tract or adhesion to inflamed respiratory
as their potential to provide long-t erm protection from reinfection with
vascular endothelium. However, although
SARS-CoV-2, remains debated. Nevertheless, recent studies have highlighted autopsy studies of patients’ lungs and
various aspects of T cell responses to SARS-CoV-2 infection that are starting to single-cell RNA sequencing (scRNA-seq) of
enable some general concepts to emerge. bronchoalveolar lavage fluid do identify the
presence of lymphocytes, the lymphocytic
infiltration is not excessive5,16. In addition,
COVID-19 caused by SARS-CoV-2 observed in patients with severe disease, a recent scRNA-seq analysis of the upper
infection is a global pandemic, with more relevant features of CD8+ versus CD4+ T cell respiratory tract from patients with
than 15.8 million infections and more than responses in patients who are hospitalized, COVID-19 showed that there was a markedly
641,000 deaths as of 25 July 2020, according features of T cell differentiation that may decreased contribution of cytotoxic T
to the COVID-19 Map of the Johns Hopkins be altered and current data on whether the lymphocytes in patients with severe disease
Coronavirus Resource Center. SARS-CoV-2 overall magnitude of the T cell response in compared with those with moderate disease9.
infection can result in a range of clinical patients with COVID-19 is insufficient or In severe disease, lymphopenia may be
manifestations, from asymptomatic or excessive and how these features may relate associated with high levels of IL-6, IL-10 or
mild infection to severe COVID-19 that to disease. Finally, we discuss emerging tumour necrosis factor (TNF)6,10,14, potentially
requires hospitalization. Patients who data on SARS-CoV-2-specific T cells through a direct effect of these cytokines on
are hospitalized often progress to severe found in patients who have recovered from T cell populations17,18 and/or indirect effects
pneumonia and acute respiratory distress COVID-19 and the implications for T cell via other cell types, such as dendritic cells19
syndrome (ARDS)1–3. Although relatively memory. In this rapidly emerging field, and neutrophils20,21. Hyperactivation of T cells
little is known about the immunology we summarize the most recent studies or high levels of expression of pro-apoptotic
of individuals who are asymptomatic or that have addressed T cell responses in molecules, such as FAS (also known as
individuals with mild disease who do not COVID-19. Some of these are as yet only CD95)8, TRAIL or caspase 3 (ref.11), could
require hospitalization, recent studies have available on preprint servers and conclusions also contribute to T cell depletion.
revealed important insights into the immune from non-peer-reviewed data should be Thus, although the mechanisms of
responses of patients who are hospitalized. treated with caution. A summary of the data lymphopenia in COVID-19 remain
Similar to other respiratory viral infections, sets that are published versus those available incompletely understood, the reduction in
adaptive immune responses4–9, particularly as preprints is provided in Table 1 to aid the the number of T cells, in particular, in the
of T cells6,8,10, have a prominent role in reader in establishing the weight of evidence periphery is a prominent feature of many
SARS-CoV-2 infection. However, it remains for particular features. individuals with severe disease. It remains
unclear whether T cell responses are helpful unclear why the lymphopenia is T cell
or harmful in COVID-19, and whether T cell Lymphopenia in COVID-19 biased and perhaps specifically CD8+
responses are suboptimal and dysfunctional One prominent feature of SARS-CoV-2 T cell biased. In animal models, lymphopenia
or excessive, with evidence having been infection is lymphopenia1,6,12,13. Lymphopenia can augment T cell activation and
provided for both ends of the spectrum. is associated with severe disease10,12,13 but is proliferation22. Therefore, determining how
Here, we summarize some of the recent reversed when patients recover4,12. In some lymphopenia in patients with COVID-19
data on conventional T cell responses patients, lymphopenia has been reported might impact T cell hyperactivation
in COVID-19, noting, however, that to affect CD4+ T cells, CD8+ T cells, B cells and, potentially, immunopathology is an
emerging data also highlight impacts on and natural killer cells4,6, whereas other data important future goal, as therapeutics such
other lymphocyte populations, including suggest that SARS-CoV-2 infection has a as IL-7 could be beneficial in this regard.
B cells4,8,11, innate lymphoid cells4, natural preferential impact on CD8+ T cells8,9,14.
killer cells4,11, mucosa-associated invariant Transient lymphopenia is a common feature CD8+ T cell responses in COVID-19
T cells4 and γδT cells11. We highlight some of of many respiratory viral infections, such Early studies of small numbers of patients,
the key observations made for conventional as with influenza A H3N2 virus, human or sometimes even a single patient, reported
αβ CD8+ and CD4+ T cells in COVID-19, rhinovirus or respiratory syncytial virus, alterations in the activation and/or
including the prominent lymphopenia but lymphopenia in these other infections differentiation status of CD8+ T cells in
Nature ReviewS | Immunology volume 20 | September 2020 | 529Progress
Table 1 | Studies reporting T cell analysis in patients with COVID-19
Donor cohort Sample origin Profiling technology Major conclusions for αβT cells Refs
used
3 healthy, 3 mild/ Bronchoalveolar 10x Genomics Greater clonal expansion of T cells in moderate disease than severe 5
moderate disease, lavage fluid scRNA-seq, 10× disease; T cells in moderate disease have stronger signatures of tissue
6 severe disease Genomics scTCR-seq residency
8 moderate disease, Nasopharyngeal 10x Genomics Fewer CTLs in severe disease than moderate disease; hyperactivation of 9
11 severe disease and bronchial scRNA-seq CTLs in the respiratory tract, with a signature of interacting with epithelial
samples cells and other immune cell types
5 healthy, PBMCs 10x Genomics Greater clonal expansion of T cells in late-recovered than in early- 28
5 early-recovered, scRNA-seq, 10x recovered patients; fewer CD8+ T cells but greater cytotoxic signatures
5 late-recovered Genomics scTCR-seq in early-recovered than in late-recovered patients
6 healthy, PBMCs Seq-Well scRNA-seq Heterogeneity of immune responses, including of interferon-stimulated 7
3 non-ventilated, genes; no transcriptional signature of exhaustion; features of T cell
4 with ARDS hyperactivation in some of the patients with ARDS
3 healthy, 6 mild/ PBMCs 10x Genomics Strong T cell lymphopenia in severe disease with potential systemic 25
moderate disease, scRNA-seq, flow adaptive immune dysregulation; altered T cell differentiation and a (Preprint)
4 severe disease cytometry hyperactivation stage in severe disease; thymosin α1 can expand the
memory-like T cell population and prevent T cell hyperactivation
15 healthy, PBMCs 10x Genomics Similar total and activated T cell counts for influenza and COVID-19 40
79 COVID-19 scRNA-seq (3 groups; higher IFNα-responding and IFNγ-responding signatures in the (Preprint)
(15 with ARDS), influenza and 4 severe influenza groups than in the COVID-19 groups
26 influenza COVID-19),
(7 with ARDS) flow cytometry
28 with ARDS, PBMCs Flow cytometry Stronger T cell lymphopenia in more severe COVID-19; lower CD4+ T cell 6
26 non-ARDS, other counts in COVID-19 (n = 17) than in influenza (H1N1; n = 4)
infection controls
12 healthy, PBMCs High-dimensional Stronger T cell lymphopenia in more severe disease; heterogeneity of 4
7 recovered, flow cytometry T cell responses related to activation and cytotoxicity signatures; T cells
7 moderate disease, express more markers of terminal differentiation or exhaustion in severe
27 severe disease disease
60 healthy, PBMCs High-dimensional Stronger T cell lymphopenia in severe disease, with a bias towards CD8+ 8
36 recovered, flow cytometry T cells; heterogeneity of T cell responses based on high-dimensional
125 hospitalized immune profiling, with three potential immune subtypes; T cells more
patients (NIH activated but also express more markers of terminal differentiation
ordinal score 2–5) and exhaustion in patients with COVID-19 than in individuals who are
healthy or who recovered
40 healthy, 522 with PBMCs Flow cytometry Stronger T cell lymphopenia in ICU patients, elderly patients and severe 10
varying disease disease, for both CD4+ and CD8+ T cells; IL-6, IL-10 and TNF levels
severity negatively correlate with lymphocyte count; T cells express higher levels
of PD1 and TIM3 in ICU patients than in non-ICU individuals
55 healthy, PBMCs High-dimensional Stronger T cell lymphopenia in severe disease; increased number of 11
6 mild disease, flow cytometry hyperactivated proliferating CD4+ and CD8+ T cells in severe disease; (Preprint)
26 moderate increased markers of terminal differentiation or exhaustion in severe
disease, 31 severe disease compared with milder disease
disease
10 moderate PBMCs Flow cytometry Higher lymphocyte counts in moderate disease than in severe disease, 13
disease, 11 severe for both CD4+ and CD8+ T cells; more IFNγ-producing T cells in moderate
disease disease than severe disease
20 healthy, 30 with PBMCs Flow cytometry T cell lymphopenia in patients compared with healthy controls, with 14
varying disease an increased ratio of CD4+ T cells to CD8+ T cells; increased proportion
severity of terminally differentiated or senescent CD8+ T cells in patients, with
a reduced proportion of IFNγ-producing cells; tocilizumab improves
lymphocyte counts (n = 5)
30 healthy, 55 mild PBMCs Flow cytometry Stronger T cell lymphopenia in severe disease than in mild disease 23
disease, 13 severe or healthy controls, with recovery of T cell numbers in convalescent
disease individuals; reduced levels of multiple cytokines in CD8+ T cells in
disease groups, with higher levels of NKG2A expression than healthy
controls
6 healthy, 10 mild PBMCs Flow cytometry Increased cytotoxicity but decreased cytokine secretion of T cells, 24
disease, 6 severe particularly CD8+ T cells, in severe disease compared with mild disease;
disease CD8+ T cells in severe disease express more inhibitory receptors
Case report, PBMCs Flow cytometry ICOS+PD1+ circulating TFH cells increase during recovery; activated 26
multiple time points CD4+ and CD8+ T cells peak at day 9 post disease onset and decline after
recovery
530 | September 2020 | volume 20 www.nature.com/nriProgress
Table 1 (cont.) | Studies reporting T cell analysis in patients with COVID-19
Donor cohort Sample origin Profiling technology Major conclusions for αβT cells Refs
used
20 healthy, PBMCs Flow cytometry CD4+ and CD8+ T cells from convalescent patients respond to 29
20 convalescent, SARS-CoV-2 epitopes, including S, M and N proteins and other ORFs;
other common cold T cell reactivity to SARS-CoV-2 also detected in non-exposed donors,
coronaviruses with potential cross-reactivity to other common cold coronaviruses
14 convalescent PBMCs Flow cytometry CD4+ and CD8+ T cells from convalescent patients respond to 30
SARS-CoV-2 epitopes
16 healthy, PBMCs Flow cytometry T cells from convalescent patients with mild or severe disease respond 31
28 recovered to SARS-CoV-2 epitopes; convalescent patients with mild disease have (Preprint)
from mild disease, a better memory CD8+ T cell response than convalescent patients with
14 recovered from severe disease
severe disease
8 healthy, 8 with PBMCs Flow cytometry T cell lymphopenia in COVID-19 compared with healthy controls, with 35
varying disease an increase of T cell activation phenotypes; SARS-CoV-2-specific T cells
severity mainly produce TH1-type cytokines
10 healthy, PBMCs Flow cytometry CD4+ T cells in ICU patients produce more GM-CSF and IL-6 than 37
21 non-ICU, non-ICU individuals and healthy controls
12 in ICU
245 healthy, PBMCs Flow cytometry Stronger T cell lymphopenia in severe disease compared with mild 38
19 mild disease, disease and healthy controls; IL-6 levels negatively correlate with
41 severe disease lymphocyte count; patients who respond to treatment recover
lymphocyte numbers
15 male and PBMCs High-dimensional Male and female patients have T cell lymphopenia; female patients 60
29 female healthy, flow cytometry have more T cell activation than male patients; male patients with (Preprint)
17 male and severe disease have greater reduction of T cell activation and loss
21 female with of IFNγ-producers than those with stable disease
COVID-19
ARDS, acute respiratory distress syndrome; CTL, cytotoxic T lymphocyte; GM-CSF, granulocyte–macrophage colony-stimulating factor; ICOS, inducible co-stimulator;
ICU, intensive care unit; IFNγ, interferon-γ; ORF, open reading frame; PBMC, peripheral blood mononuclear cell; PD1, programmed cell death protein 1; scRNA-seq,
single-cell RNA sequencing; scTCR-seq, single-cell T cell receptor sequencing; TFH cell, T follicular helper cell; TH1 cell, T helper 1 cell; TIM3, T cell immunoglobulin
and mucin domain-containing protein 3; TNF, tumour necrosis factor.
severe COVID-19 (Fig. 1a). For example, observed in many, but not all, patients4,8,11,26. responses5,16, and recent scRNA-seq data
there is evidence of terminally differentiated In other settings, CD38+HLA-DR+ or Ki67+ from the upper respiratory tract imply that
T cells or possibly exhausted T cells in CD8+ T cells that are present in the blood interactions occur there between epithelial
severe disease, with reported increases in during the acute phase of a viral infection cells and cytotoxic T lymphocytes, in
expression levels of the inhibitory receptors or after live-attenuated vaccination contain particular through an interferon-γ (IFNγ)
PD1, TIM3, LAG3, CTLA4, NKG2A and virus-specific T cells27, which indicates that axis9. Indeed, more robust clonal expansion
CD39 (refs4,8,10,11,23,24). However, expression there might be virus-specific CD8+ T cell of CD8+ T cells in peripheral blood28 or
of these receptors could also reflect recent responses in those patients with COVID-19 bronchoalveolar lavage fluid5 may be
activation, and it is not clear whether the who have robust CD38+HLA-DR+ or Ki67+ associated with milder disease or recovery,
T cells in patients with COVID-19 are CD8+ T cell responses. However, not all although it is not clear whether this CD8+
exhausted or just highly activated. By patients have this T cell activation phenotype T cell clonal expansion is the cause or
contrast, at least one blood scRNA-seq study and current data point to potentially diverse consequence of the disease recovery. Last,
has reported limited expression of inhibitory patterns of CD8+ T cell responses in patients there is evidence of SARS-CoV-2-specific
receptors by CD8+ T cells in patients with COVID-19 (ref.8). CD8+ T cells in patients who have recovered,
with COVID-19 compared with healthy Several important considerations arise which provides evidence not only of
controls7. In one report, CD8+ T cells from from these studies: how does heterogeneity virus-specific CD8+ T cell responses but
patients with severe COVID-19 had reduced of the CD8+ T cell response relate to disease; also of CD8+ T cell memory in many
cytokine production upon stimulation23. how do T cell responses in peripheral blood convalescent patients29–32. The precise role of
Alternatively, other data suggest that reflect events in the respiratory tract; and are these virus-specific CD8+ T cells in control
CD8+ T cells might have a hyperactivation the CD8+ T cell responses antigen specific? of initial acute SARS-CoV-2 infection
signature, including high levels of First, multiple studies have indicated and their capacity to protect from future
expression of natural killer cell-related heterogeneity in immune responses to infection remain to be determined.
markers and increased cytotoxicity4,23,25. SARS-CoV-2, including in CD8+ T cells,
Some of these studies imply the presence and emerging data identify potentially CD4+ T cell responses in COVID-19
of an overaggressive CD8+ T cell response distinct patient immunotypes6,8 that might, Similar to CD8+ T cells, there is evidence
or a hyperactive state in patients with in some cases, be related to disease features. of functional impairment and increased
COVID-19 (ref.25). Increased numbers of Second, autopsy studies and scRNA-seq data expression of activation and/or exhaustion
CD38+HLA-DR+ activated CD8+ T cells or from bronchoalveolar lavage fluid suggest markers by CD4+ T cells in patients with
Ki67+ proliferating CD8+ T cells were also the importance of respiratory CD8+ T cell COVID-19 (refs10,14) (Fig. 1b). Case reports
Nature ReviewS | Immunology volume 20 | September 2020 | 531Progress
a Proposed CD8+ T cell response during COVID-19
Cytokines,
Activated chemokines
T cells Cell TCR Cell cycle and Co-inhibitory
Mild number clonality state cytotoxicity signals
disease Effector T cells
IL-2, type I and terminally IFNγ++
differentiated T cells PD1+/–
and type III Dominant IL-2+
Normal or TIM3+/–
interferon clones Ki67+/– CD107a++
increased CD38+
Clonal detected TNF+ CD39+/–
expansion GZMB+
Memory T cells
Naive PD1++
IL-6, IL-10, Less activated IFNγ + TIM3++
T cell IL-1β, CXCL8 T cells? IL-2+/– CD38++
and other Lack of CD107a+ CD39+
Terminally Exhausted- Strongly
CXCLs, TNF dominant Ki67+/+ GZMB++ NKG2A+
differentiated like T cell decreased
clones Perforin++ KLRs+
Severe T cell
CCL3+ LAG3+
disease CCL4++ CTLA4+
Reduced Memory IL-1β+ TIGIT+
T cell pool? ? T cell
b Proposed CD4+ T cell response during COVID-19
Proliferating Co-stimulatory
TH cells Cell Humoral and
Mild Cell Lineage cycle immune co-inhibitory
disease Systemic number specificity state memory signals
IL-2, antiviral response CD38+/–
type I and TH1 cell, ICOS+/–
type III Germinal-centre TH2 cell, CD95–
Normal or CX3CR1+/–
interferon B cell activation increased germinal- Ki67+/– Efficient
centre PD1+/–
Germinal- TFH cell TIM3+/–
centre TFH cell CD39+/–
Naive Plasmablast
T cell hyperactivation
?
IL-6, IL-10, ICOS CD38
+ +
CD38++
IL-1β, CXCL8 circulating TFH cells Circulating
TFH cell, ICOS++
and other Immune CD95+
CXCLs, TNF Systemic TH17 cell,
antiviral response cell subtype hyper-T 1 Ki67
+/+
Unknown CX3CR1+
dependent cell (T H PD1+
Severe reg
TIM3+
disease Hyperactivated cell?)
CD39+
TH1 cells TIGIT+
?
Immunopathology
CCR6+ TH17 cell
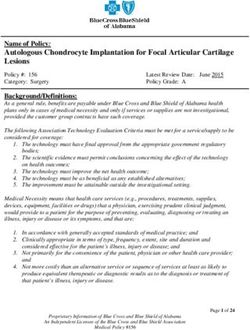
Fig. 1 | Potential model of T cell responses during COVID-19 progres- CX3CR1, CX3C-chemokine receptor 1; CXCL, CXC-chemokine ligand;
sion. A proposed model of CD8+ T cell responses (a) and CD4+ T cell GZMB, granzyme B; ICOS, inducible co-stimulator; IFNγ, interferon-γ; KLR,
responses (b) during COVID-19 progression in mild versus severe disease. killer cell lectin-like receptor; LAG3, lymphocyte activation gene 3; TCR,
Tables show the immune parameters that have been reported to differ T cell receptor; TFH cell, T follicular helper cell; TH1 cell, T helper 1 cell; TH2
between mild and severe COVID-19. Phenotype data are collated from the cell, T helper 2 cell; TH17 cell, T helper 17 cell; TIGIT, T cell immunoreceptor
references cited in this Progress article. Results that have been confirmed with immunoglobulin and ITIM domains; TIM3, T cell immunoglobulin and
by multiple studies are indicated in bold type. CCL, CC-chemokine ligand; mucin domain-containing protein 3; TNF, tumour necrosis factor; Treg cell,
CCR6, CC-chemokine receptor 6; CTLA4, cytotoxic T lymphocyte antigen 4; regulatory T cell.
have suggested that CD8+ T cell activation SARS-CoV-2 spike protein have been indicates a potential role for T helper 17
might be greater than CD4+ T cell activation, identified in acute infection and have a (TH17) cell-mediated immunopathology,
as defined by activation markers such as TH1 cell cytokine profile35. A role for T whereas another study identified possible
CD38 and HLA-DR26,33,34. However, another helper 2 (TH2) cell-type responses in severe increases in the number of CD4+ T cells
study identified a subset of patients with COVID-19 is unclear, although patients producing transforming growth factor-β
higher levels of CD4+ T cell activation with mild disease may have a normal TH2 (TGFβ)36. A population of CD4+ T cells
who possibly do worse clinically8. One cell response11. Given the prominent role of producing granulocyte–macrophage
report has described a higher proportion TH2 cell responses in other lung diseases, colony-stimulating factor (GM-CSF) or
of IFNγ-producing T helper 1 (TH1)-like this is an important area for further study. IL-6 has also been reported in patients with
cells in patients with moderate disease Two individual reports have also described COVID-19 (ref.37), although T cells do not
than in patients with severe disease13. a strong CCR6+CD4+ T cell signature typically produce IL-6. Regulatory T cells36
Moreover, CD4+ T cells specific for the in severe COVID-19 (refs2,34), which and ICOS+CD38+ circulating T follicular
532 | September 2020 | volume 20 www.nature.com/nriProgress
helper (activated cTFH) cells8 may also be consistent with a recent observation of may also paradoxically be pro-inflammatory
altered in patients with COVID-19, with reduced numbers of plasmacytoid dendritic and therefore perhaps contribute to
increased numbers of activated cTFH cells cells11. This observation, however, contrasts immunopathology. Older patients
in some settings perhaps connected to with the robust and consistent upregulation experience more severe lymphopenia during
a reported increase in the number of of the interferon-inducible chemokine COVID-19 (ref.10), although it is not clear
circulating plasmablasts4. CXCL10 observed in one patient cohort11, whether ageing-associated lymphopenia is
Lymphopenia also affects CD4+ T cells, perhaps owing to non-interferon inducers causal to disease severity or vice versa.
although some studies suggest that the of expression of this chemokine. Men with COVID-19 have higher
impact is less than that for CD8+ T cells8,38. Another key gap in our understanding is rates of hospitalization and mortality than
It remains to be determined how the relationship between viral load and the women58, and among severe cases of disease,
lymphopenia might relate to CD4+ T cell immune response. Viral load could have a men have more severe lymphopenia59.
activation and/or dysfunction. Moreover, in major impact on the magnitude and quality There may also be a bias to stronger CD4+
addition to memory CD8+ T cells, patients of the T cell response, and future studies that and CD8+ T cell activation in women with
who have recovered from SARS-CoV-2 quantify virus replication should provide COVID-19 (ref.60). It is unclear whether these
infection have virus-specific memory context for understanding evolving T cell sex biases relate to X chromosome-encoded
CD4+ T cells29–32, which bodes well for the responses during SARS-CoV-2 infection. immune genes58 and/or the role of sex
possibility of T cell memory and, perhaps, A key feature of patients with COVID-19 hormones in regulating immune responses61.
protective immunity. In individuals is the enrichment for co-morbidities such Nevertheless, these data highlight the
who recovered from mild COVID-19, as hypertension and diabetes42 (see next importance of accounting for sex in ongoing
CD4+ T cells gained a typical memory section), but it remains to be defined clinical trials.
phenotype with high levels of expression of how an individual patient’s background A very high proportion of patients
IL-7Rα (ref.32). Interestingly, cross-reactive ‘immune health’ landscape shapes responses with COVID-19 who are hospitalized have
memory CD4+ T cells are also found in to SARS-CoV-2 infection. Although one or more underlying cardiovascular
subjects who have never been exposed to lymphopenia is not a unique feature of co-morbidities44,45,62–64. Moreover, many
SARS-CoV-2 (ref.29). It is unclear how these SARS-CoV-2 infection43, it may be more of the manifestations of severe disease
pre-existing memory CD4+ T cells, which prolonged in patients with COVID-19, relate to coagulopathies and vascular
are presumably generated in response and lymphopenia-induced proliferation complications62,64. Even the newly recognized
to human endemic coronaviruses, affect can clearly affect T cell differentiation and SARS-CoV-2-associated multisystem
immunity or pathology upon SARS-CoV-2 activation; however, the contribution of inflammatory syndrome in children has
infection. There are other settings in which lymphopenia to T cell differentiation in similarities to Kawasaki disease, which
the presence of memory CD4+ T cells patients with COVID-19 has not yet been often involves inflammation of the coronary
in the absence of effective CD8+ T cells or investigated. artery65,66. Other viral infections, including
antibodies can cause pathology39. Thus, Ebola virus and virulent lymphocytic
CD4+ T cell responses are present in patients Co-morbidities and COVID-19 choriomeningitis virus in mice, can cause
with COVID-19 and perhaps form memory Co-morbidities such as cardiovascular damage to the vascular endothelium. These
following resolution of the disease. Whether disease44,45, diabetes42 and obesity46 are viruses infect the vascular endothelium,
CD4+ T cells responding in acute infection some of the most common underlying and T cells can then cause vascular damage
with SARS-CoV-2 are functionally impaired conditions associated with worse clinical by attacking the virus-infected cells67–69.
or hyperactivated, and how these responses outcome and severe COVID-19. Moreover, However, disease presentation in these
relate to disease outcome, remain important older patients experience greater clinical settings is distinct from that for COVID-19,
unanswered questions. severity of COVID-19 (refs1,47), males and extensive SARS-CoV-2 infection of
may experience more severe disease than the vascular endothelium is unlikely in
T cell differentiation in COVID-19 females1,47 and genetic variations, including most patients.
Most acute viral infections in humans the ABO blood type8,48,49, have been reported Obesity also contributes to more
induce the activation and proliferation to affect the clinical outcomes for patients severe COVID-19 and higher rates of
of both CD4+ T cells and CD8+ T cells, with COVID-19. However, how these hospitalization46,70, which are perhaps
so SARS-CoV-2 infection may not be unique co-morbidities are associated with T cell associated with the role of body mass index
in this regard. However, hyperactivation responses during COVID-19 remains in cardiovascular health. However, obesity
or hypoactivation of T cells, or skewing largely unknown. can also directly affect T cell responses
towards an ineffective differentiation state Advanced age is a common co-morbidity to influenza vaccination71 or infection72,
(for example, TH17 cells, exhausted T cells or for severity of disease during respiratory and a role for obesity in altering T cell
terminally differentiated T cells), might not viral infections, and disease severity differentiation has been observed in asthma73
be optimal in some patients with COVID-19. may be associated with altered T cell and chronic inflammation74. Nevertheless,
Several features that have been described responses50,51. Ageing affects T cell repertoire the precise role of T cells in driving the
in patients with severe COVID-19 — diversity52, both for CD4+ T cells53 and for coagulopathies or inflammation that are
including high levels of systemic cytokines CD8+ T cells54. This age-related reduction characteristic of severe COVID-19 in
or chemokines, most notably IL-6, CXCL8, in T cell clonal diversity is associated with patients with cardiovascular co-morbidities
CXCL9 and CXCL10 (refs8,11,40), or delayed impaired responses to viral infections such is unclear.
or defective type I interferon responses41 — as influenza55. Advanced age can also be Finally, a recent genetic association study
could potentially skew T cell responses. associated with T cell senescence, which compared patients with severe COVID-19
The potential type I interferon deficiency perhaps contributes to ineffective responses and ARDS with healthy controls49. Several
described in patients with COVID-19 is to infections56,57. However, senescent T cells chemokine receptor genes, including CCR9,
Nature ReviewS | Immunology volume 20 | September 2020 | 533Progress
CXCR6 and XCR1, and the locus controlling different stages of disease or with different be important. Although evidence of
the ABO blood type were identified as being immune response characteristics and then T cell memory to other coronaviruses is
associated with severe disease. Whether to match them with treatment strategies. encouraging, such immune natural history
these genes are directly or indirectly related Such a precision medicine strategy studies for SARS-CoV-2 will likely be
to T cell responses in COVID-19, however, based on analysis of ‘immune health’ valuable for examining vaccine-induced
remains unknown and needs further could be used to better tailor the use of T cell responses.
investigation. immunostimulatory strategies such as
Thus, although severe COVID-19 is thymosin α1 (ref.25) or type I interferon75 Conclusions
partially characterized by patients with versus immunosuppressive drugs such The accumulating evidence supports a role
co-morbidities, how these co-morbidities as tocilizumab76–78, ruxolitinib79 or for T cells in COVID-19 and probably in
relate to T cell responses remains poorly dexamethasone80 to patients who will receive the immunological memory that forms
understood. Causal associations may most benefit. These efforts should be aided following recovery from SARS-CoV-2
exist, perhaps connected to some of the by the development of better preclinical infection. Most, although not all, patients
underlying genetics. However, it is also models, including human ACE2-expressing who are hospitalized seem to mount both
possible that certain co-morbidities mice81–85. It will be interesting in the future CD8+ and CD4+ T cell responses, and
or pre-existing conditions make to use such models to address key questions evidence points to possible suboptimal,
patients with severe disease less able to including: what is an ‘appropriate’ profile excessive or otherwise inappropriate T cell
tolerate the severe virus-mediated and of T cell activation and differentiation for a responses associated with severe disease.
immune-mediated pathology associated successful antiviral response to SARS-CoV-2 In fact, multiple distinct patterns of T cell
with SARS-CoV-2 infection. without triggering severe pathology; response may exist in different patients,
how does viral load or initial inoculum of which suggests the possibility of distinct
Strength of COVID-19 T cell response SARS-CoV-2 impact T cell responses and clinical approaches tailored to the particular
The published data discussed here indicate pathology; how do T cell responses in the immunotype of a specific patient. Much
that patients with severe COVID-19 can blood relate to lung-infiltrating T cells, of the available data on T cell responses
have either insufficient or excessive T cell considering that many respiratory viruses in patients with COVID-19 who are
responses. It is possible, therefore, that are controlled by tissue-resident immune hospitalized is still available only in preprint
disease might occur in different patients cells that may not be present in the blood; form. This format has been essential for
at either end of this immune response and what are the molecular mechanisms rapid dissemination of information in the
spectrum, in one case from virus-mediated that support a successful T cell response setting of pandemic urgency. However,
pathology and in the other case from during SARS-CoV-2 infection? as these studies move through peer review,
T cell-driven immunopathology4. However, we should gain increasing confidence and
it is unclear why some patients respond T cell memory in COVID-19 clarity about the nature of T cell responses
too little and some patients too much, and A key question is whether protective to SARS-CoV-2 infection. More carefully
whether the strength of the T cell response T cell memory can form following either defining distinct classes of T cell response
in the peripheral blood reflects the T cell SARS-CoV-2 infection or vaccination. types in COVID-19 and delineating how
response intensity in the respiratory tract and Although data on vaccination will await pre-existing conditions, co-morbidities,
other SARS-CoV-2-infected organs. Some trial results, early data from patients race, ‘immune health’ status and other
information exists on SARS-CoV-2-specific with COVID-19 who have recovered are variables influence T cell responses should
T cells in patients who are hospitalized, and promising. Memory CD4+ T cells and reveal novel opportunities for treatment
approaches using activation markers (such CD8+ T cells were detected in 100% and prevention.
as Ki67) likely capture virus-specific T cell and 70% of patients who recovered, Zeyu Chen and E. John Wherry ✉
responses; recent studies are beginning to fill respectively29. Moreover, memory T cell
Department of Systems Pharmacology and
in this picture by identifying virus-specific responses were detected for multiple Translational Therapeutics, Institute for Immunology,
CD4+ T cells and CD8+ T cells in acute SARS-CoV-2 proteins, including not only Perelman School of Medicine, University of
disease5,29,30. However, one missing set of spike protein but also nucleoprotein and Pennsylvania, Philadelphia, PA, USA.
information is a careful immune analysis membrane protein31. Whether these T cells ✉e-mail: wherry@pennmedicine.upenn.edu
of outpatients who, during acute infection provide protective immunity is unclear, https://doi.org/10.1038/s41577-020-0402-6
with SARS-CoV-2, are undergoing a and addressing this question for T cells Published online 29 July 2020
‘successful’ immune response. Moreover, alone will be confounded by the presence of 1. Huang, C. et al. Clinical features of patients infected
it will be crucial to incorporate into any SARS-CoV-2-specific antibodies in patients with 2019 novel coronavirus in Wuhan, China.
Lancet 395, 497–506 (2020).
model of COVID-19 how the magnitude and who recover. Nevertheless, ongoing analysis 2. Xu, Z. et al. Pathological findings of COVID-19
quality of T cell responses relate to signals of patients who have recovered should associated with acute respiratory distress syndrome.
Lancet Resp. Med. 8, 420–422 (2020).
from other parts of the immune system, such provide insights into the protective capacity 3. Matthay, M. A., Aldrich, J. M. & Gotts, J. E.
as innate cytokines, antigen presentation of immune memory, including humoral Treatment for severe acute respiratory distress
syndrome from COVID-19. Lancet Resp. Med. 8,
and myeloid cells. Lastly, the strength of the and cellular memory, as these individuals 433–434 (2020).
T cell response may also relate to the stage are potentially re-exposed to SARS-CoV-2 4. Kuri-Cervantes, L. et al. Comprehensive mapping
of immune perturbations associated with severe
of disease or infection. Accurately assessing in the community. Further studies should COVID-19. Sci. Immunol. 5, eabd7114 (2020)
the different ‘phases’ of acute SARS-CoV-2 also define the differentiation state and 5. Liao, M. et al. Single-cell landscape of bronchoalveolar
immune cells in patients with COVID-19. Nat. Med. 8,
infection may also be valuable in interpreting durability of T cell memory. Moreover, 842–844 (2020).
T cell responses. defining how T cell memory forms in 6. Giamarellos-Bourboulis, E. J. et al. Complex immune
dysregulation in COVID-19 patients with severe
Thus, future studies should provide patients who experience mild symptoms respiratory failure. Cell Host Microbe 27, 992–1000
insights into how to identify patients at of COVID-19 versus severe disease will (2020).
534 | September 2020 | volume 20 www.nature.com/nriProgress
7. Wilk, A. J. et al. A single-cell atlas of the peripheral lack of terminal differentiation, and high proliferative 58. Scully, E. P., Haverfield, J., Ursin, R. L., Tannenbaum, C.
immune response in patients with severe COVID-19. potential. Preprint at bioRxiv https://doi.org/10.1101/ & Klein, S. L. Considering how biological sex impacts
Nat. Med. 26, 1070–1076 (2020). 2020.06.08.138826 (2020). immune responses and COVID-19 outcomes. Nat. Rev.
8. Mathew, D. et al. Deep immune profiling of COVID-19 33. Vabret, N. et al. Immunology of COVID-19: Immunol. 20, 442–447 (2020).
patients reveals distinct immunotypes with therapeutic current state of the science. Immunity 52, 910-941 59. Meng, Y. et al. Sex-specific clinical characteristics
implications. Science https://doi.org/10.1126/ (2020). and prognosis of coronavirus disease-19 infection in
science.abc8511 (2020). 34. Qin, C. et al. Dysregulation of immune response in Wuhan, China: a retrospective study of 168 severe
9. Chua, R. L. et al. COVID-19 severity correlates with patients with coronavirus 2019 (COVID-19) in Wuhan, patients. PLoS Pathog. 16, e1008520 (2020).
airway epithelium–immune cell interactions identified China. Clin. Infect. Dis. https://doi.org/10.1093/cid/ 60. Takahashi, T. et al. Sex differences in immune
by single-cell analysis. Nat. Biotech. https://doi.org/ ciaa248 (2020). responses to SARS-CoV-2 that underlie disease
10.1038/s41587-020-0602-4 (2020). 35. Weiskopf, D. et al. Phenotype and kinetics of outcomes. Preprint at medRxiv https://doi.org/
10. Diao, B. et al. Reduction and functional exhaustion SARS-CoV-2-specific T cells in COVID-19 patients with 10.1101/2020.06.06.20123414 (2020).
of T cells in patients with coronavirus disease 2019 acute respiratory distress syndrome. Sci. Immunol. 5, 61. Bouman, A., Heineman, M. J. & Faas, M. M.
(COVID-19). Front. Immunol. 11, 827 (2020). eabd2071 (2020). Sex hormones and the immune response in humans.
11. Laing, A. G. et al. A consensus Covid-19 immune 36. Wang, W. et al. High-dimensional immune profiling Hum. Reprod. Update 11, 411–423 (2005).
signature combines immuno-protection with discrete by mass cytometry revealed immunosuppression 62. Zheng, Y.-Y., Ma, Y.-T., Zhang, J.-Y. & Xie, X. COVID-19
sepsis-like traits associated with poor prognosis. and dysfunction of immunity in COVID-19 patients. and the cardiovascular system. Nat. Rev. Cardiol. 17,
Preprint at medRxiv https://doi.org/10.1101/ Cell. Mol. Immunol. 17, 650–652 (2020). 259–260 (2020).
2020.06.08.20125112 (2020). 37. Zhou, Y. et al. Pathogenic T-cells and inflammatory 63. Magro, C. et al. Complement associated microvascular
12. Tan, L. et al. Lymphopenia predicts disease severity monocytes incite inflammatory storms in severe injury and thrombosis in the pathogenesis of severe
of COVID-19: a descriptive and predictive study. COVID-19 patients. Natl Sci. Rev. 7, 998–1002 COVID-19 infection: a report of five cases. Transl Res.
Signal. Transduct. Target. Ther. 5, 33 (2020). (2020). 220, 1–13 (2020).
13. Chen, G. et al. Clinical and immunological features 38. Wang, F. et al. Characteristics of peripheral lymphocyte 64. Klok, F. A. et al. Incidence of thrombotic complications
of severe and moderate coronavirus disease 2019. subset alteration in COVID-19 pneumonia. J. Infect. Dis. in critically ill ICU patients with COVID-19. Thromb. Res.
J. Clin. Invest. 130, 2620–2629 (2020). 221, 1762–1769 (2020). 191, 145–147 (2020).
14. Mazzoni, A. et al. Impaired immune cell cytotoxicity 39. Penaloza-MacMaster, P. et al. Vaccine-elicited CD4 65. Viner, R. M. & Whittaker, E. Kawasaki-like disease:
in severe COVID-19 is IL-6 dependent. J. Clin. Invest. T cells induce immunopathology after chronic LCMV emerging complication during the COVID-19 pandemic.
https://doi.org/10.1172/JCI138554 (2020). infection. Science 347, 278–282 (2015). Lancet 395, 1741–1743 (2020).
15. McClain, M. T. et al. Longitudinal analysis of leukocyte 40. Mudd, P. A. et al. Targeted immunosuppression 66. Belhadjer, Z. et al. Acute heart failure in multisystem
differentials in peripheral blood of patients with acute distinguishes COVID-19 from influenza in moderate inflammatory syndrome in children (MIS-C) in the
respiratory viral infections. J. Clin. Virol. 58, 689–695 and severe disease. Preprint at medRxiv https:// context of global SARS-CoV-2 pandemic. Circulation
(2013). doi.org/10.1101/2020.05.28.20115667 (2020). https://doi.org/10.1161/CIRCULATIONAHA.120.
16. Wichmann, D. et al. Autopsy findings and venous 41. Blanco-Melo, D. et al. Imbalanced host response 048360 (2020).
thromboembolism in patients with COVID-19: to SARS-CoV-2 drives development of COVID-19. 67. Frebel, H. et al. Programmed death 1 protects
a prospective cohort study. Ann. Intern. Med. Cell 181, 1036–1045 (2020). from fatal circulatory failure during systemic virus
https://doi.org/10.7326/M20-2003 (2020). 42. Fang, L., Karakiulakis, G. & Roth, M. Are patients infection of mice. J. Exp. Med. 209, 2485–2499
17. Taga, K. & Tosato, G. IL-10 inhibits human T cell with hypertension and diabetes mellitus at increased (2012).
proliferation and IL-2 production. J. Immunol. 148, risk for COVID-19 infection? Lancet Resp. Med. 8, 68. Yang, Z. Y. et al. Identification of the Ebola virus
1143–1148 (1992). e21 (2020). glycoprotein as the main viral determinant of vascular
18. Böttcher, J. P. et al. IL-6 trans-signaling-dependent 43. Panesar, N. S. Lymphopenia in SARS. Lancet 361, cell cytotoxicity and injury. Nat. Med. 6, 886–889
rapid development of cytotoxic CD8+ T cell function. 1985 (2003). (2000).
Cell Rep. 8, 1318–1327 (2014). 44. Li, B. et al. Prevalence and impact of cardiovascular 69. Wolf, T. et al. Severe Ebola virus disease with vascular
19. Malefyt, R. et al. Interleukin 10 (IL-10) and viral metabolic diseases on COVID-19 in China. Clin. Res. leakage and multiorgan failure: treatment of a
IL-10 strongly reduce antigen-specific human T cell Cardiol. 109, 531–538 (2020). patient in intensive care. Lancet 385, 1428–1435
proliferation by diminishing the antigen-presenting 45. Guo, T. et al. Cardiovascular implications of fatal (2015).
capacity of monocytes via downregulation of class II outcomes of patients with coronavirus disease 2019 70. Stefan, N., Birkenfeld, A. L., Schulze, M. B. &
major histocompatibility complex expression. (COVID-19). JAMA Cardiol. 5, 811-818 (2020). Ludwig, D. S. Obesity and impaired metabolic health
J. Exp. Med. 174, 915–924 (1991). 46. Lighter, J. et al. Obesity in patients younger than 60 in patients with COVID-19. Nat. Rev. Endocrinol. 16,
20. Liu, Y. et al. Neutrophil-to-lymphocyte ratio as an years is a risk factor for COVID-19 hospital admission. 341–342 (2020).
independent risk factor for mortality in hospitalized Clin. Infect. Dis. https://doi.org/10.1093/cid/ciaa415 71. Sheridan, P. A. et al. Obesity is associated with
patients with COVID-19. J. Infect. 81, e6–e12 (2020). (2020). impaired immune response to influenza vaccination
21. Ma, Y. et al. Predictive value of the neutrophil-to- 47. Richardson, S. et al. Presenting characteristics, in humans. Int. J. Obes. 36, 1072–1077 (2012).
lymphocyte ratio (NLR) for diagnosis and worse clinical comorbidities, and outcomes among 5700 patients 72. Paich, H. A. et al. Overweight and obese adult
course of the COVID-19: findings from ten provinces hospitalized with COVID-19 in the New York City area. humans have a defective cellular immune response
in China. Preprint at SSRN https://doi.org/10.2139/ JAMA 323, 2052–2059 (2020). to pandemic H1N1 influenza A virus. Obesity 21,
ssrn.3569838 (2020). 48. Zhao, J. et al. Relationship between the ABO blood 2377–2386 (2013).
22. Surh, C. D. & Sprent, J. Homeostasis of naive and group and the COVID-19 susceptibility. Preprint 73. Leiria, L. O. S., Martins, M. A. & Saad, M. J. A.
memory T cells. Immunity 29, 848–862 (2008). at medRxiv https://doi.org/10.1101/2020.03.11. Obesity and asthma: beyond TH2 inflammation.
23. Zheng, M. et al. Functional exhaustion of antiviral 20031096 (2020). Metabolism 64, 172–181 (2015).
lymphocytes in COVID-19 patients. Cell. Mol. Immunol. 49. Ellinghaus, D. et al. Genomewide association study 74. DeFuria, J. et al. B cells promote inflammation in
17, 533–535 (2020). of severe Covid-19 with respiratory failure. N. Engl. obesity and type 2 diabetes through regulation of
24. Zheng, H.-Y. et al. Elevated exhaustion levels and J. Med. https://doi.org/10.1056/NEJMoa2020283 T-cell function and an inflammatory cytokine profile.
reduced functional diversity of T cells in peripheral (2020). Proc. Natl Acad. Sci. USA 110, 5133–5138 (2013).
blood may predict severe progression in COVID-19 50. Lee, N., Shin, M. S. & Kang, I. T-cell biology in aging, 75. Sallard, E., Lescure, F.-X., Yazdanpanah, Y., Mentre, F.
patients. Cell. Mol. Immunol. 17, 541–543 (2020). with a focus on lung disease. J. Gerontol. A Biol. Sci. & Peiffer-Smadja, N. Type 1 interferons as a potential
25. Yu, K. et al. Thymosin α-1 protected T cells from Med. Sci. 67, 254–263 (2012). treatment against COVID-19. Antivir. Res. 178,
excessive activation in severe COVID-19. Preprint at 51. Goronzy, J. J. & Weyand, C. M. Successful and 104791 (2020).
Research Square https://doi.org/10.21203/ maladaptive T cell aging. Immunity 46, 364–378 76. Xu, X. et al. Effective treatment of severe COVID-19
rs.3.rs-25869/v1 (2020). (2017). patients with tocilizumab. Proc. Natl Acad. Sci. USA
26. Thevarajan, I. et al. Breadth of concomitant immune 52. Naylor, K. et al. The influence of age on T cell 117, 10970–10975 (2020).
responses prior to patient recovery: a case report generation and TCR diversity. J. Immunol. 174, 77. Luo, P. et al. Tocilizumab treatment in COVID-19:
of non-severe COVID-19. Nat. Med. 26, 453–455 7446–7452 (2005). a single center experience. J. Med. Virol. 92, 814–818
(2020). 53. Pourgheysari, B. et al. The cytomegalovirus-specific (2020).
27. Miller, J. D. et al. Human effector and memory CD4+ T-cell response expands with age and markedly 78. Guo, C. et al. Tocilizumab treatment in severe COVID-19
CD8+ T cell responses to smallpox and yellow fever alters the CD4+ T-cell repertoire. J. Virol. 81, patients attenuates the inflammatory storm incited
vaccines. Immunity 28, 710–722 (2008). 7759–7765 (2007). by monocyte centric immune interactions revealed by
28. Wen, W. et al. Immune cell profiling of COVID-19 54. Messaoudi, I., Lemaoult, J., Guevara-Patino, J. A., single-cell analysis. Preprint at bioRxiv https://doi.org/
patients in the recovery stage by single-cell sequencing. Metzner, B. M. & Nikolich-Zugich, J. Age-related CD8 10.1101/2020.04.08.029769 (2020).
Cell Discov. 6, 31 (2020). T cell clonal expansions constrict CD8 T cell repertoire 79. Cao, Y. et al. Ruxolitinib in treatment of severe
29. Grifoni, A. et al. Targets of T cell responses to and have the potential to impair immune defense. coronavirus disease 2019 (COVID-19): a multicenter,
SARS-CoV-2 coronavirus in humans with COVID-19 J. Exp. Med. 200, 1347–1358 (2004). single-blind, randomized controlled trial. J. Allergy
disease and unexposed individuals. Cell 181, 55. Yager, E. J. et al. Age-associated decline in T cell Clin. Immunol. 146, 137–146 (2020).
1489–1501.e15 (2020). repertoire diversity leads to holes in the repertoire 80. Abdolahi, N. et al. Letter to the editor: efficacy
30. Ni, L. et al. Detection of SARS-CoV-2-specific humoral and impaired immunity to influenza virus. J. Exp. Med. of different methods of combination regimen
and cellular immunity in COVID-19 convalescent 205, 711–723 (2008). administrations including dexamethasone, intravenous
individuals. Immunity 52, 971–977 (2020). 56. Goronzy, J. J., Li, G., Yu, M. & Weyand, C. M. immunoglobulin, and interferon-β to treat critically ill
31. Dong, T. et al. Broad and strong memory CD4 Signaling pathways in aged T cells—a reflection COVID-19 patients: a structured summary of a study
and CD8 T cells induced by SARS-CoV-2 in UK of T cell differentiation, cell senescence and host protocol for a randomized controlled trial. Trials 21,
convalescent COVID-19 patients. Preprint at bioRxiv environment. Semin. Immunol. 24, 365–372 (2012). 549 (2020).
https://doi.org/10.1101/2020.06.05.134551 (2020). 57. Yu, H. T., Park, S., Shin, E.-C. & Lee, W.-W. T cell 81. Goldman-Israelow, B., Song, E., Mao, T., Lu, P.
32. Neidleman, J. et al. SARS-CoV-2-specific T cells exhibit senescence and cardiovascular diseases. Clin. Exp. Med. & Meir, A. Mouse model of SARS-CoV-2 reveals
unique features characterized by robust helper function, 16, 257–263 (2016). inflammatory role of type I interferon signaling.
Nature ReviewS | Immunology volume 20 | September 2020 | 535Progress
Preprint at bioRxiv https://doi.org/10.1101/2020. Acknowledgements Peer review information
05.27.118893 (2020). Z.C. is supported by grant CA234842 from the National Nature Reviews Immunology thanks Susan L. Swain and the
82. Sun, J. et al. Generation of a broadly useful model for Institutes of Health (NIH). Work in the Wherry laboratory other, anonymous, reviewer(s) for their contribution to
COVID-19 pathogenesis, vaccination, and treatment. is supported by NIH grant AI082630, the Allen Institute the peer review of this work.
Cell https://doi.org/10.1016/j.cell.2020.06.010 for Immunology and the Parker Institute for Cancer
(2020). Immunotherapy. Publisher’s note
83. Hassan, A. O. et al. A SARS-CoV-2 infection model Springer Nature remains neutral with regard to jurisdictional
in mice demonstrates protection by neutralizing Author contributions claims in published maps and institutional affiliations.
antibodies. Cell https://doi.org/10.1016/ The authors contributed equally to all aspects of the article.
j.cell.2020.06.011 (2020).
84. Bao, L. et al. The pathogenicity of SARS-CoV-2 Competing interests Related links
in hACE2 transgenic mice. Nature https://doi.org/ E.J.W. has consulting agreements with and/or is a scientific CoVID-19 Map of the Johns Hopkins Coronavirus resource
10.1038/s41586-020-2312-y (2020). advisor for Merck, Roche, Pieris, Elstar and Surface Oncology. Center: https://coronavirus.jhu.edu/map.html
85. Jiang, R.-D. et al. Pathogenesis of SARS-CoV-2 in E.J.W. has a patent licensing agreement on the PD1 pathway
transgenic mice expressing human angiotensin- with Roche/Genentech. E.J.W. is a founder of Arsenal
converting enzyme 2. Cell 182, 50–58 (2020). Biosciences. Z.C. declares no competing interests. © Springer Nature Limited 2020
536 | September 2020 | volume 20 www.nature.com/nriYou can also read