The Diabetes Attitudes, Wishes, and Needs (DAWN) Program: A New Approach to Improving Outcomes of Diabetes Care
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
Lifestyle and Behavior
The Diabetes Attitudes, Wishes, and Needs (DAWN) Program:
A New Approach to Improving Outcomes of Diabetes Care
Soren E. Skovlund, Msc, Bsc, and Mark Peyrot, PhD, on behalf of the DAWN International Advisory Panel*
*The DAWN International Advisory Committee includes Ib Brorly (a person with diabetes), Denmark; Ruth Colagiuri,
RN, Australia; P. Geelhoed-Duijvestijn, MD, the Netherlands; Hitoshi Ishii, MD, Japan; Line Kleinebreil, MD, France;
Rüdiger Landgraf, MD, Germany; Torsten Lauritzen, MD, Denmark; David Matthews, MD, United Kingdom; A.
Ramachandran, MD, India; Richard Rubin, PhD, United States; and Frank Snoek, PhD, the Netherlands.
The Diabetes Attitudes, Wishes, and studies as one of the possible causes of plications is commonly observed in
Needs (DAWN) program is an inter- poor outcomes of diabetes care in general practice settings. Both patient
national partnership effort to improve general practice.3,4 A multitude of and provider beliefs appear to con-
outcomes of diabetes care by increas- research studies, mainly in the tribute to the delayed use of effective
ing the focus on the person behind the Western world and with relatively therapy (e.g., misconceptions of the
disease, especially the psychosocial small patient samples, has indicated consequences of initiating medication,
and behavioral barriers to effective the potential importance of a multi- that medication is not efficacious or
diabetes management. DAWN was tude of psychological, social, and may have serious side effects).16,17
initiated by an international survey of behavioral factors for patient self- These factors lead to a reluctance to
> 5,000 people with diabetes and management.5,6 Access to patient- intensify treatment regimens, which
almost 4,000 diabetes care providers. centered self-management support may be overcome through improved
The DAWN program has facilitated a and education has been shown in sev- communication.
number of concrete initiatives to eral studies to improve outcomes of
address the gaps in diabetes care iden- diabetes care.7 What Is DAWN?
tified by the DAWN study. Psychosocial research points to an DAWN is an international collabora-
integral role of psychosocial issues in tive program initiated in 2001 by
Why Do We Need DAWN? all aspects of diabetes care,8 and in Novo Nordisk in partnership with the
Diabetes is one of the major world particular comorbid depression is asso- International Diabetes Federation and
health problems. Recent estimates ciated with impaired self-management an international expert advisory panel
from the World Health Organization and metabolic control. Psychological representing leading spokespeople for
predict that if current trends continue, treatment may help to improve both medical, educational, psychological,
the number of people with diabetes quality of life and diabetes self-man- and advocacy issues related to improv-
will more than double, from 176 to agement.9 Furthermore, monitoring of ing a person-centered approach to dia-
370 million people by 2030.1 Diabetes psychological health may improve betes care. Panel members were from
is already the single most costly health patient-reported outcomes as part of Denmark, France, Germany, India,
care problem in Westernized coun- ongoing diabetes care.10 Japan, the Netherlands, the United
tries. Among those diagnosed with the In terms of the structure and Kingdom, and the United States.
disease, at least half still do not processes of care, effective communi- National activities are developed by
achieve satisfactory glycemic control, cation between patients and multidisciplinary national expert
despite the availability of effective providers has been suggested to be groups drawing on relevant best prac-
treatments.2 As a consequence, mil- important for optimal treatment out- tices for putting DAWN into action.
lions of people with diabetes are at comes.11,12 For instance, application The goal of DAWN is to improve
elevated risk of suffering needlessly of motivational interviewing tech- outcomes of diabetes care by increas-
from serious complications of the dis- niques has been shown to improve ing the focus on the person behind the
ease. With the growing number of the success rate of behavior change disease, especially the psychosocial
people with diabetes, there is an consultations.13 and behavioral barriers to effective
urgent need to find better ways of Access to a coordinated interdisci- diabetes management. DAWN was
curbing the human and economic bur- plinary diabetes care team to offer initiated by an international study
den of this chronic progressive dis- appropriate care, whether the need is designed to identify a broad set of
ease, through prevention, detection, self-management education, medical attitudes, wishes, and needs among
and treatment. A review of the litera- advice, or psychosocial support, has diabetes patients and care providers
ture suggests several important areas been identified as an important factor (physicians and nurses) in order to lay
that have the potential to address for improving treatment outcomes in a foundation for national and interna-
these problems. diabetes.14,15 tional efforts to improve diabetes
Suboptimal diabetes self-manage- Delayed initiation of medication care.18 The DAWN study examined
ment has been identified by several therapies to prevent long-term com- several factors related to quality of
136
Diabetes Spectrum Volume 18, Number 3, 2005Lifestyle and Behavior
diabetes care: levels of diabetes self- sites, as opposed to rural and subur- taking, glucose testing, and appoint-
management and psychological dis- ban sites. Physicians had a longer ment keeping was low. Fewer than
tress among people with diabetes, average duration of practice (15.9 one in five people with diabetes
quality of relationships between peo- years) than nurses (10.6 years). (19.4% of those with type 1 diabetes
ple with diabetes and their care The third sample consisted of and 16.2% of those with type 2 dia-
providers, collaboration among dia- adults with type 1 or type 2 diabetes betes) reported that they completely
betes care providers (team care), and with a quota for each region of 250 complied with all aspects of their pre-
barriers to effective medication thera- people with self-reported type 1 dia- scribed regimens. Providers rated
py for diabetes. betes and 250 with self-reported type adherence substantially worse than
Once the DAWN study was com- 2 diabetes. For the purpose of analy- did people with diabetes (7.3% of
pleted, the results provided the impe- sis, people were classified as having providers estimated that their typical
tus for a number of initiatives type 1 diabetes if they were diagnosed type 1 patient completely complied
designed to remedy the problems with diabetes before age 40 and treat- with all aspects of their prescribed
identified. Some of these initiatives ed with insulin both at diagnosis and regimens, and 2.9% of providers esti-
were already underway, and the at the time of the survey; others were mated the same for their typical type
results stimulated support for their classified as having type 2 diabetes. 2 patient).
development; other initiatives grew Respondents who did not provide
out of the collaborative efforts of the information necessary to classify type Distress
international community exposed to of diabetes according to this algo- People with diabetes reported that
the findings of the DAWN study. rithm were deleted from the analyses, diabetes-related distress is high at
leaving a usable sample of 5,104. diagnosis (85.2% reported feeling
The DAWN Study People with diabetes were divided shocked, guilty, angry, anxious,
All data are self-reports gathered dur- almost equally by sex (54.0% female) depressed, or helpless). Long after
ing 2001 by structured interviews and lived primarily in urban areas diagnosis (mean duration of almost
conducted face-to-face or by tele- (58.0%). The median age at which 15 years), problems of living with dia-
phone, using DAWN questionnaires formal education was completed was betes were prevalent, including fear of
that had been developed based on a 17 years. Approximately one-third future complications and resulting
literature review and focus groups in were classified as having type 1 dia- social disabilities, as well as immedi-
eight countries and translated into the betes; Japan was an anomaly with ate social and psychological burdens
languages of the countries studied. < 5% having type 1 diabetes. (Table 1). Three of four (73.6%)
Interviews were conducted in 11 Compared to people with type 2 dia- reported at least one of these fears or
regions (representing 13 countries): betes, those with type 1 diabetes had a burdens. Providers reported that the
Australia, France, Germany, India, younger average age (38.0 vs. 59.3 majority of their patients with type 1
Japan, the Netherlands, Poland, years) and a longer average duration or type 2 diabetes experience psycho-
Scandinavia (Sweden, Denmark, and of diabetes (19.2 vs. 11.2 years). logical problems (67.9 and 65.6%,
Norway), Spain, the United Kingdom, respectively). Almost half of all people
and the United States. The What DAWN Taught Us with diabetes in the DAWN study had
Scandinavian samples were evenly The results reported here draw on poor well-being according to the
divided among the three countries. a number of forthcoming articles WHO-5 well-being index.19
The study was conducted with and analyses presented at research There was a linkage between poor
three independent samples. The first conferences. 19–25 adherence and psychological prob-
sample consisted of 2,705 physicians lems. The majority of providers
with a quota of 250 per region: 200 in Adherence (68.3%) reported that psychological
primary care and 50 specialists Reported adherence with recommen- problems influence regimen adher-
(endocrinologists and diabetologists dations for diet, exercise, medication ence. Moreover, a poor reaction at
with 2 years of experience and treat-
ing > 50 diabetes patients per month). Table 1. Percentage of Patients Experiencing Various Aspects
The second sample consisted of 1,122 of Diabetes-Related Distress
nurses with a quota of 100 per region:
50 specialists (treating > 50 people Diabetes-related distress Percentage of respondents
with diabetes per month) and 50 gen- who agree
eralists. Caring for at least five people I feel stressed because of my diabetes. 32.7
with diabetes per month was an inclu- I feel burned out because of my diabetes. 18.1
I feel that diabetes is preventing me from 35.9
sion criterion for the study, and only
doing what I want to do.
one provider was selected from a I am constantly afraid of my diabetes getting worse. 43.8
given practice. I worry about not being able to carry out my 30.1
Physician respondents were pre- family responsibilities in the future.
dominantly male (72.6%), whereas My diabetes causes me worries about my financial future. 25.8
nurses were predominantly female My family and friends put too much pressure 14.7
(95.2%). Both physicians (69.5%) on me about my diabetes.
and nurses (69.0%) worked in urban The community I live in is intolerant of diabetes. 13.6
137
Diabetes Spectrum Volume 18, Number 3, 2005Lifestyle and Behavior
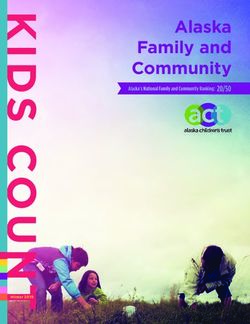
diagnosis (characterized by an inabili-
ty to accept the diagnosis and a strong Table 2. Percentage of Physicians Reporting That Their Typical
negative emotional response) was Patient Sees Various Diabetes Care Providers Annually
associated with a variety of poor
Respondent
patient-reported outcomes, including Discipline Seen Primary Care Diabetes Specialist
regimen nonadherence (Figure 1). Physician Physician
Despite the widespread prevalence Primary Care Physician NA 39.2
of diabetes-related distress and its Diabetes Specialist Physician 38.6 NA
important negative consequences, Diabetes Specialist Nurse* 24.6 35.6
only a small minority of people with Dietitian/Nutritionist* 31.3 40.9
diabetes (3.3%) had received psycho- Eye Specialist 67.0 64.4
logical treatment for diabetes-related Foot Specialist 32.5 35.7
problems within the 5 years prior to Behavioral Specialist* 6.0 14.0
the survey. Data are %.
*Significant (P < 0.05) difference between primary care and diabetes specialist.
Patient-Provider Relationships
The quality of patient-provider rela- four or more additional providers too complicated, and one in three
tionships was rated high by patients; (22.0 vs. 12.0%). Annual appoint- (33.7%) is tired of complying with
88.8% reported that they have a good ments were common only for eye doc- their medication regimen. Of those
relationship with the people who care tors (approximately two or three not taking insulin and who feel that
for their diabetes. However, most respondents described such visits as their diabetes is not well controlled,
providers reported that they need to typical), and typical appointments only one in four (26.9%) believes that
better understand the psychological with most other providers were insulin would help them to manage
consequences of diabetes (69.8%) and reported by only one in three partici- their diabetes better. Nearly one in
the various ethnic cultures that they pants, with behavioral specialists two providers (43.4%) prefers to
deal with (78.8%). reported as team members for the typ- delay initiation of oral medication
ical patient by < 10% of physicians. until it is “absolutely essential.” And
Provider Collaboration Only half of people with diabetes only half (49.2%) of health care
Team care was less than optimal (51%) felt that their diabetes health providers believe that earlier use of
(Table 2). To assess levels of team care providers talked to each other insulin would decrease the overall cost
care, physicians were asked how about their care. of diabetes care. Patients who are
many of seven providers a typical resistant to effective medication regi-
patient of theirs saw on an annual Barriers to Use of Effective mens and who are treated by
basis (primary care practitioner, dia- Medication Therapy providers who share their resistance
betes specialist physician, diabetes Many people with diabetes have wor- are likely to experience delays in the
nurse, dietitian/nutritionist, eye doc- ries about starting diabetes medica- intensification of treatment even in the
tor, foot doctor, behavioral specialist). tion and intensifying existing medica- face of persisting need.
Most providers (65.6%) said their tion regimens. And providers are not
diabetes patients saw two or fewer eager to use medication to achieve Summary
providers in addition to themselves; treatment goals. Of those taking anti- The DAWN study has identified sev-
specialist physicians were more likely hyperglycemic medication, one in six eral important gaps in the manage-
than primary care physicians to report (16.6%) feels that their treatment is ment of diabetes across a number of
countries. Diabetes self-management
is less than optimal and is compro-
mised frequently by diabetes-related
distress, which often is not treated.
Although the quality of patient-
provider relationships is generally
good, providers need a better under-
standing of the social and psychologi-
cal problems that people with dia-
betes face. Team care is uncommon,
with few providers providing their
patients with comprehensive multidis-
ciplinary care. People with diabetes
and health care providers often resist
initiating effective medication thera-
pies. These problems combine and
reinforce one another, leading to an
Figure 1. Poor reaction to diagnosis predicts later problems. QoL, quality of unnecessary increase in the burden of
diabetes.
life.
138
Diabetes Spectrum Volume 18, Number 3, 2005Lifestyle and Behavior
While these findings confirm what overcome the barriers to optimal patients’ needs and providing counsel-
many diabetes health care profession- health and quality of life faced by ing and psychosocial support to peo-
als already believe, the DAWN study people with diabetes. In plenum, vot- ple with diabetes is needed in order to
provided the first quantitative data ing systems enabled all participants to diminish the psychological burden of
from a large-scale, international study take part in the final selection of key living with diabetes and overcome the
regarding both the magnitude and goals for future action. Based on the psychological barriers to effective dis-
nature of these problems. Further- key findings of the DAWN study, the ease self-management.
more, the study offered a host of new following five goals were confirmed
insights about concordance and the for concerted advocacy and action to 3. Enhance communications between
lack thereof in the perceptions of dif- improve diabetes care worldwide people with diabetes and health care
ferent participants in diabetes care. (Table 3).27,28 providers.
Importantly, the study identified Effective patient-centered communica-
major gaps in the provision of dia- 1. Promote active self-management. tion is considered a prerequisite for
betes care today, including a failure Active self-management is a key deter- understanding and addressing the
to take fully into account the individ- minant of treatment outcome in dia- individual psychosocial barriers to
ual barriers to achieving full health betes, and therefore the diabetes care diabetes self-management in daily
and quality of life among people with team’s ability to facilitate active self- care. Because enhanced communica-
diabetes. management and patient involvement tion requires the active involvement of
in the care process is central to achiev- both the person with diabetes and
Implications of the DAWN Study ing optimal treatment outcomes. health care professionals, efforts in
To transform the wealth of insights Health care professionals should this area should involve initiatives to
from the DAWN study into concrete encourage better self-management by empower and engage both people
actions to improve diabetes care, two taking into account individual with diabetes as well as health care
international DAWN summits were patient’s circumstances, needs, and professionals to communicate effec-
held, each attended by > 100 leading resources when creating treatment tively. People with diabetes should be
health care professionals, researchers, plans and considering psychosocial supported in taking responsibility for
decision-makers, people with diabetes, barriers to self-management as an their own disease and expressing their
media personnel, and representatives integral part of the care process. treatment and support needs clearly to
of major nongovernmental diabetes their health care professionals.
organizations and the pharmaceutical 2. Enhance psychological care.
industry. The 1st International Although many people with diabetes 4. Promote communication and
DAWN Summit was held in Oxford, cope well and live normal, healthy coordination between health care
United Kingdom, in April 2002.26 lives with diabetes, far too many suf- professionals.
This 2-day meeting involved presenta- fer emotionally without receiving Diabetes is a complex condition, and
tion and discussion of the primary basic psychosocial support. Improved its effective management requires a
DAWN findings. Major themes were access to health care professionals and coordinated multidisciplinary care
identified through discussion of find- psychologists trained in identifying approach. The role of every team
ings in discipline-specific and country- member should be enhanced, and
specific break-out groups. Table 3. DAWN Goals and strategies are needed to promote team
The 2nd International DAWN Strategies building and dialogue among all dia-
Summit was held in London in betes professionals to ensure a coher-
November 2003 with a goal of initi- Goals of the DAWN Program ent, integrated approach to optimizing
ating concrete action.27 The 2-day 1. Promote active self-management. treatment.
meeting included presentations from 2. Enhance psychological care.
government policymakers, representa- 3. Enhance communications between 5. Reduce barriers to effective therapy.
people with diabetes and health care
tives of the International Diabetes providers.
Patient understanding of the conse-
Federation and the World Health 4. Promote communication and coordi- quences of not treating diabetes opti-
Organization, and leading nation between health care profes- mally requires that health care
researchers. The common theme was sionals. providers give the information and
defining feasible actions that could be 5. Reduce barriers to effective therapy. support necessary to enable patients
taken to address the gaps in diabetes to make informed decisions about
care identified by the DAWN study. Strategies to Achieve DAWN Goals intensification of therapy. All health
1. Raise awareness and advocacy.
Best practices were shared by speak- 2. Educate and mobilize people with
care professionals should be aware of
ers from countries that had already diabetes and those at risk. the health implications of postponing
taken action based on the DAWN 3. Train health care providers and necessary therapy and should enable
findings at a national level. These enhance their competencies. patients to make genuinely informed
presentations laid the foundation for 4. Provide practical tools and systems. choices about therapy. This requires
multidisciplinary, multinational 5. Drive policy and health care systems increased awareness and information
workshops in which participants change. about diabetes treatment options that
could identify concrete and feasible 6. Develop psychosocial research in suit the individual lifestyle and treat-
actions that could be taken to help diabetes. ment needs of each patient.
139
Diabetes Spectrum Volume 18, Number 3, 2005Lifestyle and Behavior
Translating Goals Into Action access to empowering information in Examples of action. In the United
The DAWN Call to Action27,28 was order to make informed decisions States, a continuing medical education
developed on the basis of internation- about their health and quality of life. program on how to put DAWN into
al dialogue among patients, educators, As experts in the management of their clinical practice was created for dia-
physicians, health care researchers, own condition, people with diabetes betes educators based on one of sever-
politicians, and nongovernmental need to be engaged to play a key role al DAWN symposia held as part of
organizations. It identifies concrete in new approaches, tools, and guide- the annual meetings of the American
strategies that can be implemented at lines for patient-centered care. People Association of Diabetes Educators.20
the local, regional, national, and inter- with diabetes inform health care In Poland, the DAWN study revealed
national levels to promote the providers, policymakers, and others a major national need for training pri-
achievement of the five goals of the about the needs and wants of people mary care in an integrated medical
DAWN program and the translation with diabetes. and psychosocial approach to treating
of DAWN study insights into real Examples of action. The Assisting type 2 diabetes. Using DAWN as a
quality-of-life improvements on a Young Diabetics in Egypt Project suc- foundation, train-the-trainer work-
large scale (Table 3). Guided by this cessfully offered psychological sup- shops and simple daily assessment
framework, numerous initiatives have port and therapeutic patient educa- tools were developed and disseminat-
been proposed and implemented by tion to > 2,000 children and families ed widely in that country, and today
groups and organizations in different with diabetes over just 2 years’ time. > 4,500 Polish health care profession-
countries. Below, we define the strate- This project was identified by the als have been trained in both the psy-
gies and provide examples of these DAWN international advisory board chological and medical aspects of
initiatives. as the winner of the 2004 DAWN treating diabetes. In Germany,
Award. The DAWN international > 1,000 general practitioners, and dia-
Strategy 1. Raise awareness and and national advisory boards involve betes specialists and nurses were
advocacy. people with diabetes, and the DAWN trained in skills focusing on communi-
Those individuals and organizations summits offer people with diabetes cation and psychosocial matters in
with an understanding of the benefits opportunities to speak to internation- order to increase patient empower-
of providing psychosocial support for al audiences about their needs. In ment. Drawing on experiences from
people with diabetes must play an Germany and the Netherlands, con- > 300 diabetes nurse specialists from
active role in sharing their knowledge crete activities include the issuance of 14 countries who took part in a new
with their peers and raising awareness diabetes passports to all people with DAWN workshop concept for dia-
in the public about the importance of diabetes to encourage active self-man- betes teams, a set of diabetes team
changing our approach to diabetes agement and clear communication workshops and DVD- and video-
care and focusing more on the atti- and agreement among patients and enhanced training tools was devel-
tudes, wishes, and needs of people providers about the mutual responsi- oped in 2004; these have been adopt-
with diabetes and their caregivers. bilities involved in optimal diabetes ed by many providers in countries
Examples of action. The management. In New Zealand, peo- such as Australia, Germany, Israel,
International Diabetes Federation ple with diabetes attending a large Sweden, the United Kingdom, and the
(IDF) published a special issue of its diabetes center were offered a patient United States.
journal Diabetes Voice, which was involvement form before each consul-
distributed in 140 countries; this issue tation to encourage active patient Strategy 4. Provide practical tools
was dedicated to the implications of participation and clear communica- and systems.
the DAWN study and the resulting tion during diabetes visits. The adequate identification of psy-
international DAWN Call to Action chosocial and educational needs
and triggered many new DAWN Strategy 3. Train health care requires first and foremost effective
activities.28 In the United States, the providers and enhance their listening and communication skills on
American Diabetes Association’s competencies. the part of health care professionals,
patient magazine, Diabetes Forecast, In order to overcome the psychosocial an essential element of the chronic ill-
highlighted the key insights from the barriers to effective diabetes manage- ness care model.30 In addition, patient
DAWN study, reaching millions of ment identified by DAWN, health self-report assessment tools and deci-
readers nationwide.29 In the Arabic care systems need to identify ways to sion-support tools can facilitate inclu-
world, Asia, Europe, and Latin improve the identification of these sion of psychosocial aspects in routine
America, lay media coverage of barriers and develop approaches to clinical encounters between health
DAWN findings has helped reach out effectively address these in general care professionals and patients to
to millions more people at risk for practice settings. Training opportuni- improve patients’ well-being.10,31
and with diabetes. ties should be made more easily avail- Examples of action. In response to
able for diabetes health care the DAWN study, several countries
Strategy 2. Educate and mobilize providers, along with simple and have introduced internationally
people with diabetes and those at practical strategies to promote sus- endorsed measures of psychological
risk. tainable institutionalization of feasible well-being, diabetes-related distress,
People with diabetes and those at risk person-centered approaches to deliv- and barriers to self-management into
of developing the condition need ering diabetes care. quality-of-care monitoring systems.
140
Diabetes Spectrum Volume 18, Number 3, 2005Lifestyle and Behavior
During the period from 2002 to 2004, will be publishing its global treatment program has stimulated momentum to
> 15,000 people with diabetes from guideline by the end of 2005 with a support national action and provided
> 15 countries have completed the separate section on psychosocial care a platform for sharing best practices
WHO-5 well-being index and other in diabetes. worldwide.
diabetes-specific items from the A key challenge for putting the
DAWN survey questionnaire, offering Strategy 6. Develop psychosocial insights from the DAWN study into
a wealth of new insights about the research in diabetes. effect is the ongoing promotion of
needs of people with diabetes and the More collaborative clinical research broad dialogue and the creation of
associations between psychological on psychosocial aspects of diabetes sustainable partnerships involving all
variables, perceived quality of care, needs to be conducted to demonstrate key parties in diabetes care, with peo-
and clinical outcomes. A one-page the health and economic benefits to ple with diabetes at the center. Only
patient form was developed in New society of improved patient-centered through such partnerships can the
Zealand and several other countries for diabetes care and adoption of the call proposed new approach to diabetes be
use by patients prior to each consulta- to action specified here. A better fully embedded into whole communi-
tion to help identify relevant psychoso- understanding is required of the effec- ties and national diabetes programs.
cial issues and promote more active tive patient-centered approaches to Furthermore, an increased focus on
involvement of the patient in the con- support self-management and enhance the attitudes, wishes, and needs of
sultation and decision-making process. long-term health and quality of life of special populations (including chil-
people with diabetes. dren and adolescents with diabetes
Strategy 5. Drive policy and health Examples of action. The European and people with diabetes in under-
care systems change. Depression in Diabetes Research privileged communities or who belong
In diabetes management guidelines, Consortium (EDID), a multinational to ethnic minorities) is critically need-
reimbursement systems, and quality research initiative stimulated by the ed to identify opportunities to
systems, the psychosocial needs of DAWN Call to Action, has begun to improve care and quality of life for
people with the condition should be assess the psychosocial burden of dia- these groups.
approached with the same priority as betes by promoting the use of a com- Continuous and increasing collab-
their medical needs. Toward this end, mon set of measures so that national orative efforts are needed to trans-
governments and health care systems comparisons can be made.33 In coun- form care for diabetes and other
can be lobbied to adopt the chronic tries such as Argentina and Israel, chronic diseases from the acute to the
care model advocated by the World evaluation studies are ongoing to chronic care model. Future focus
Health Organization. assess the impact of intervention and needs to be placed on implementation
Examples of action. The DAWN education programs aimed at bringing and translational research, with inter-
program has facilitated two interna- the DAWN findings into action. A national sharing of effective tools for
tional guideline meetings in 2004 and multicountry DAWN study in Europe furthering a person-centered
2005 aimed at promoting consensus is examining the feasibility of daily approach to chronic disease manage-
regarding evidence-based recommen- use of psychosocial assessments in pri- ment and prevention.
dations for psychosocial care for peo- mary care settings in Europe. In the
ple with diabetes. At the DAWN United States, a large DAWN research
guideline meeting in Wuerzburg, initiative has been launched to evalu- Acknowledgments
Germany, in April 2005, experts in ate specific approaches to increasing The DAWN study was initiated and
psychosocial aspects of diabetes from active participation in diabetes care funded by Novo Nordisk, which pro-
12 different countries developed a among people with diabetes from dif- vided access to the data presented in
joint statement that “diabetes melli- ferent ethnic groups. this article and support for its writing.
tus is an emotionally and behavioral- Aggregate country-specific data may
ly demanding condition, and psy- Next Steps be made available for local quality-of-
chosocial factors are integral to its The paradigm for treating diabetes care improvement activities. (See
prevention, diagnosis, treatment, and care is changing on a global scale. www.dawnstudy.com.) Novo Nordisk
outcomes.” Governments, health insurers, health has provided ongoing support for the
In response to the DAWN Call to care professionals, and nongovern- DAWN program, including DAWN
Action, the national care guidelines in mental organizations are increasingly summits and various national DAWN
Japan were updated to include psy- recognizing the importance of new initiatives.
chosocial treatment recommendations partnerships and new ways of adopt-
for diabetes, and the Psychology and ing more effective approaches to help- References
Behavioral Medicine Council of the ing people with diabetes better self- 1
World Health Organization: Diabetes: total
American Diabetes Association initiat- manage the medical and psychosocial number of people with diabetes [article online].
ed a working group to develop psy- challenges associated with the disease. Available online at www.who.int/ncd/dia/data-
bases4.htm
chosocial care guidelines. In 2003 and The DAWN study has contributed to
2
2004, the Netherlands and Germany highlighting the urgency of making Kristensen JK, Bro F, Sandbaek A, Dahler-
have taken steps towards implement- this change and identifying where Eriksen K, Lassen JF, Lauritzen T: HbAlc in an
unselected population of 4438 people with type
ing evidence-based psychosocial efforts need to be focused at the glob- 2 diabetes in a Danish county. Scand J Prim
guidelines in diabetes,32 and the IDF al and national levels. The DAWN Health Care 19:241–246, 2001
141
Diabetes Spectrum Volume 18, Number 3, 2005Lifestyle and Behavior
3 27
Cramer JA: A systematic review of adherence Oliver D, Thapar A, Mead N, Safran DG, Wroe J: 2nd International DAWN Summit: a
with medications for diabetes. Diabetes Care Roland MO: Identifying predictors of high quali- call-to-action to improve psychosocial care for
27:1218–1224, 2004 ty care in English general practice: observational people with diabetes. Pract Diabetes Int
4
study. BMJ 323:784–787, 2001 21:201–208, 2004
World Health Organization: Adherence to
16 28
Long-term Therapies. Geneva, World Health Hunt LM, Valenzuela MA, Pugh JA: NIDDM International Diabetes Federation: Putting peo-
Org., 2003 patients’ fears and hopes about insulin therapy: ple at the centre of care: DAWN in action.
5
the basis of patient reluctance. Diabetes Care Diabetes Voice 49 (Special Issue):1–49, 2004
Snoek FJ: Breaking the barriers to optimal gly- 20:292–298, 1997 29
caemic control—what physicians need to know Siminerio LM: The DAWN of a new day
17
from patients’ perspectives. Int J Clin Pract Suppl Larme AC, Pugh JA: Attitudes of primary care [Editorial]. Diabetes Forecast 57:11, 2004
129:80–84, 2002 providers toward diabetes: barriers to guideline 30
implementation. Diabetes Care 21:1391–1396, Bodenheimer T, Wagner EH, Grumbach K:
6
Rubin R, Peyrot M: Psychosocial problems and 1998 Improving primary care for patients with chronic
interventions in diabetes: a review of the litera- illness: the chronic care model, part 2. JAMA
18
ture. Diabetes Care 15:1640–1657, 1992 Alberti G: The DAWN (Diabetes Attitudes, 288:1909–1914, 2002
7
Wishes and Needs) study. Pract Diabetes Int 31
Norris SL, Nichols PJ, Caspersen CJ, Glasgow 19:22–24, 2002 Skovlund SE: Patient reported assessments in
RE, Engelgau MM, Jack L, Isham G, Snyder SR, diabetes care: clinical and research applications.
19
Carande-Kulis VG, Garfield S, Briss P, Peyrot M, Rubin R, Lauritzen T, Snoek F, Cur Diabetes Rep 5:115–123, 2005
McCulloch D: The effectiveness of disease and Matthews D, Skovlund S: Psychosocial problems 32
case management for people with diabetes: a sys- and barriers to improved diabetes management: Petrak F, Herpetz S, Albus C, Hirsch, A, Kulzer
tematic review. Am J Prev Med 22:15–38, 2002 results of the cross-national Diabetes Attitudes, B, Kruse J: Psychosocial factors and Diabetes
Wishes and Needs (DAWN) study. Diabet Med. Mellitus: evidence-based treatment guidelines.
8
Delamater AM, Jacobson AM, Anderson B, In press Curr Diabetes Rev. In press. Source document
Cox D, Fisher L, Lustman P, Rubin R, Wysocki available online at http://www.diabetes-psy-
20
T: Psychosocial therapies in diabetes: report of Funnell MM, Peyrot M, Rubin RR, Siminerio chologie.de/en/guidelines.htm
the Psychosocial Therapies Working Group. LM: Steering toward a new DAWN in diabetes
33
Diabetes Care 24:1286–1292, 2001 management: opportunities for diabetes educa- Pouwer F, Skinner TC, Pibernik-Okanovic M,
9
tors to provide psychological support and Beekman ATF, Cradock, S, Szabo S, Metelko Z,
Anderson RJ, Freedland KE, Clouse RE, improve outcomes. Diabetes Educ 31 Snoek FJ: Serious diabetes-specific emotional
Lustman PJ: The prevalence of comorbid depres- (Suppl.):1–18, 2005 problems and depression in a Croatian-Dutch-
sion in adults with diabetes: a meta-analysis.
Diabetes Care 24:1069–1078, 2001 21
Peyrot M, Rubin RR, Siminerio LM: Physician English Survey from the European Depression in
and nurse use of psychosocial strategies and Diabetes (EDID) Research Consortium. Diabetes
10
Pouwer F, Snoek FJ, van der Ploeg HM, Ader referrals in diabetes (Abstract). Diabetes 51 Res Clin Pract. In press. Available online at
HJ, Heine RJ: Monitoring of psychological well- (Suppl. 2):A446, 2002 http://www.sciencedirect.com/science?_ob=Articl
being in outpatients with diabetes: effects on eURL&_udi=B6T5Y-4G7G47D-2&_coverDate
22
mood, HbA(1c), and the patient’s evaluation of Peyrot M, Rubin RR, Siminerio LM: The effect =05%2F23%2F2005&_alid=287840871&_rdo
the quality of diabetes care: a randomized con- of initial response to diagnosis of diabetes on c=1&_fmt=&_orig=search&_qd=1&_cdi=5015
trolled trial. Diabetes Care 24:1929–1935, 2001 later adjustment. AADE 29th Annual Meeting &_sort=d&view=c&_acct=C000049422&_ver-
11
Program Book 28:256, 2002 sion=1&_urlVersion=0&_userid=961290&md5
van Dam HA, van der Horst F, van den Borne
B, Ryckman R, Crebolder H: Provider-patient 23
Rubin RR, Peyrot M, Siminerio LM: Predictors =8f63ddc157a674d58f9be46b40430717
interaction in diabetes care: effects on patient of diabetes self-management and control
self-care and outcomes. a systematic review. (Abstract). Diabetes 51 (Suppl. 1):A437, 2002
Patient Educ Couns 51:17–28, 2003 24
Soren E. Skovlund, Msc, Bsc, is a
Geelhoed-Duijvestijn P, Peyrot M, Skovlund S,
12
Piette JD, Schillinger D, Potter MB, Heisler M: Rubin R, Matthews D, Kleinebreil L, Lauritzen senior adviser at Novo Nordisk in
Dimensions of patient-provider communication T, Colagiuri R, Snoek F: Physician resistance to Bagsvaerd, Denmark. Mark Peyrot,
and diabetes self-care in an ethnically diverse prescribing insulin: an international study PhD, is a professor of sociology at
population. J Gen Intern Med 18:624–633, 2003 (Abstract). Diabetologia 46 (Suppl. 1): A274, Loyola College in Baltimore, Md.
13
2003
Rubak S, Sandbaelig AK, Lauritzen T,
Christensen B: Motivational interviewing: a sys- 25
Peyrot M, Matthews D, Snoek F, Colagiuri R, Note of disclosure: Mr. Skovlund is
tematic review and meta-analysis. Br J Gen Pract Kleinebreil L, Rubin R, Ishi H, Lauritzen T, employed by and Dr. Peyrot has
55:305–312, 2005 Geelhoed-Duijvestijn P, Skovlund S: An interna-
tional study of psychological resistance to insulin
received honoraria and research sup-
14
Ovhed I, Johansson E, Odeberg H, Rastam L: use among persons with diabetes (Abstract). port from and served on an advisory
A comparison of two different team models for Diabetologia 46 (Suppl. 1):A89, 2003 panel for Novo Nordisk, which man-
treatment of diabetes mellitus in primary care.
Scand J Caring Sci 14:253–258, 2000 26
The Oxford International Diabetes Summit:
ufactures products for the treatment
Implications of the DAWN Study, April 7–8, of diabetes and has provided financial
15
Campbell SM, Hann M, Hacker J, Burns C, 2002. Pract Diabetes Int 19:187–195, 2002 support for the DAWN initiative.
142
Diabetes Spectrum Volume 18, Number 3, 2005You can also read