CUSHING'S SYNDROME BEATRIX SÁRMÁN MD. PHD - SEMMELWEIS UNIVERSITY, FACULTY OF MEDICINE, 2ND DEPT, OF MEDICINE
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
Cushing’s syndrome
Beatrix Sármán MD.
PhD.
Semmelweis University, Faculty of
Medicine, 2nd Dept, of Medicine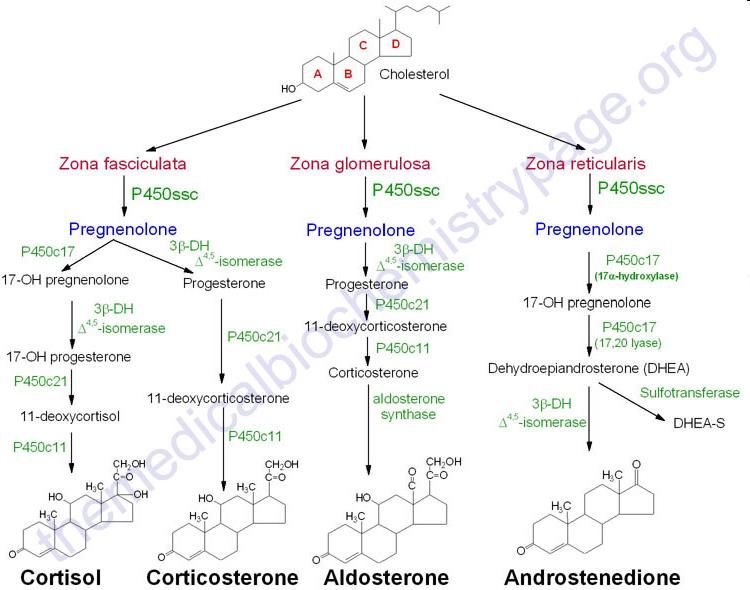
Cushing’s –syndrome: constellation of clinical abnormalities due to chronic exposure to excess of glucocorticoid (cortisol)
Cushing’s Disease (central Cushing): ACTH producing
pituitary adenoma (or excess production of Corticotrophin
Releasing Hormone /CRH/-- extremely rare)
Causes of Cushing’s syndrome:
• adrenal source
• pituitary adenoma
• ectopic ACTH secretion – neoplasm (small cell lung tu)
• iatrogenic
Another classification
ACTH dependent: Cushing’s Disease Bilateral adrenal
Ectopic Cushing hyperplasia
ACTH independent: adrenal source (tumor or hyperplasia)
iatrogenic Cushing’s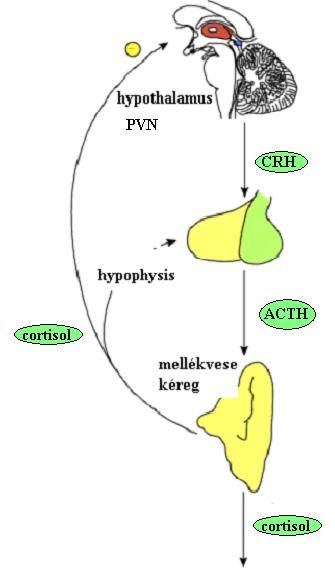
Cushing’s syndrome was discovered by Harvey W. Cushing an american
neurosurgeon.
He described first an endocrine syndrome caused by the basophil
adenomas of the pituitary gland
He published his findings in 1932 as:
"The Basophil Adenomas of the Pituitary Body and Their Clinical
Manifestations pituitary Basophilism".
Born April 8, 1869,
Cleveland, Ohio, USA
Died October 7, 1939 (aged 70)
New Haven Connecticut, USA
Education Yale University
Harvard Medical School
Known for Pioneering brain surgery
Epidemiology of the disease
Most common is iatrogenic Cushing’s syndrome because of the wild
use of steroids. Effect is dose and duration related
Other types of Cushing’s syndrome is rare:
about 70% Cushing’s disease
about 15% ectopic Cushing’s
about 15% primary tumors of adrenal gland
Cushing’s disease and cortisol secreting primary tumors of adrenal
gland adrenal are more common in women 5:1
Manifestation: between 25-40 years of age (but could be at any age)
Ectopic Cushing (lung cc) more common in man, older ageMorbidity/Mortality
Morbidity and mortality caused mainly by excess glucocorticoid
effect and/or the localization and/or malignancy of the tumor
Pituitary origin: visual loss, headache, hypopituitarism,
destruction of surrounding areas
Adrenal gland: adrenal carcinoma 5 years survival is less than
30%
Ectopic ACTH production: malignant tumors
neuroendocrin tumors (carcinoid)
iatrogenic : adrenal atrophy → acute adrenal crisisACTH dependent Cushing’s Disease, the pituitary gland
ACTH producing cells are about 10 % of the adenohypohysis cells
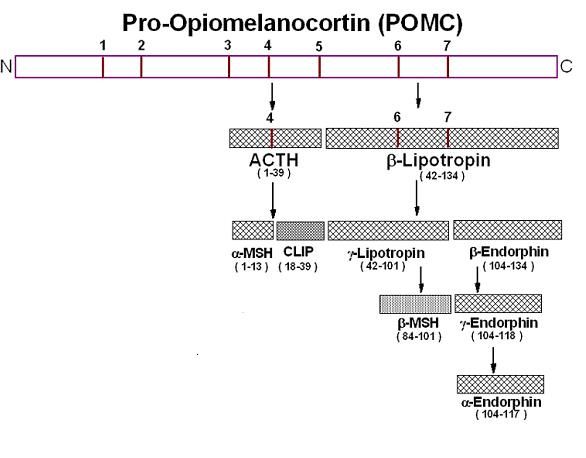
POMC (proopiomelanocortin gene) codes for ACTH, MSH (melanocyte
stimulating hormone), Beta lipotropin, Beta endorphin, metenkephalin.
POMC is induced by CRH (rarely tumors can make CRH causing Cushing's)
and suppressed by glucocorticoids.
Stimulates
adrenal
gland
Endogenous
opiats
melanocyta
stimulating
hormonPituitary ACTH producing adenoma:
adenoma:
micro adenoma < 1cm
macro adenoma > 1cm
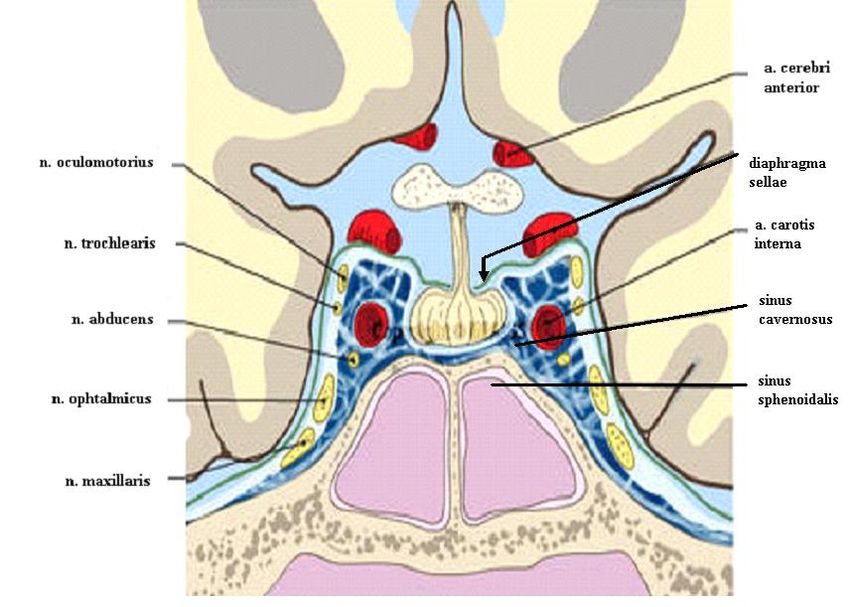
The hypophysis rests in a small,
bony cavity covered by a dural
fold (diaphragma sellae).
A growing adenoma
• destruction of the
surrounding areas
• hormonal failure of the
hypophysisClinical signs of macro adenoma :
•headache
• visual failure, lesions in the field of vision (bitemporal hemianopsy)
•Hormonal changes:
TSH→ secondary hypothyroidism: tiredness, obesity, slow
metabolism
LH/FSH→ female: menstrual disorder, infertility,
man: low libido, infertility
PRL normal or high →pressure of the pituitary stalk
("infundibular stem„), PRL released from the continuous inhibition of
the hypothalamus →hyperprolactinaemia
signs of GH deficiency
Defect of the neurohypophysis -- diabetes insipidus
• cerebral fluid loss
• signs of high cerebral pressure-- ophthalmologistEctopic ACTH production 14% of all Cushing’s Small cell lung carcinoma >50% Thymic carcinoid 15% Islet cell tumors 10% Bronchial carcinoid 10% Other carcinoids 5% Pheochromocytomas 2% Ectopic CRH production less than 1% of all Cushing’s Cushing’s symptoms + primary disease’s symptoms !
ACTH dependent Cushing’s Disease
• high adrenal steroids
•Cortisol
•Andrenal androgen steroids
•Mineralocortioids
hirsutism
Bilateral adrenal gland hyperplasia
Hyperpigmentation (MSH)
Adrenal
gland
ACTH
• lipid metabolism
• increase insulin secretion,
• increase GH secretion GHACTH independent Cushing syndrome 15% of all cases
(except iatrogenic!)
Adrenal gland adenoma 7%
Adrenal gland carcinoma 7%
Adrenal gland hyperplasiaAdrenal gland adenoma:
Usually unilateral
Less than 2-3cm
rarely multiplex, or bilateral.
Incidentaloma: hormonally inactive
tumor found by coincidence
(incidental) without clinical
symptoms or suspicion.
Adrenal gland carcinoma:
rare
40-50 years of age
Usually hormonally inactive
Adrenal gland adenoma on the left side
Bad prognosischolesterin
pregnenolon
17 α hydroxilase
17 α hydroxipregnenolon
3 β hydroxi steroid dehidrogenase
17 α hypdroxiprogesteron progesteron
21 hydroxilase
11 desoxycortisol 11 desoxycorticosteron
11 hydroxilase
corticosteron
18 hydroxilase
cortisol 18 hidroxxsteroid dehidrogenase
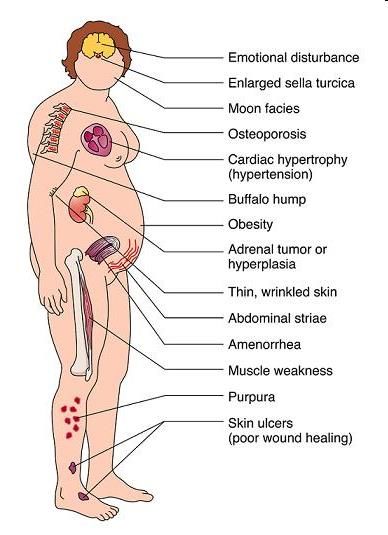
aldosteronMajor clinical features • Weight gain, central obesity • Moon face and plethora • Muscular weakness, especially proximal • Indisposition • Depression and psychosis • Oligomenorrhoea or amenorrhoea in females • Hirsutism • Striae, acne, skin-thinning, bruising • Poliuria, nocturia • decreased libido and impotence in males • Hypertension • diabetes or impaired glucose tolerance
• Truncal obesity • Moon face • Fat deposits supraclavicular fossa and posterior neck- buffalo hump • Hypertension • Hirsutism • Amenorrhea or impotence • Depression • Thin skin • Easy bruising • Purplish abdominal striae • Proximal muscle weakness • Osteoporosis • Diabetes Mellitus • Avascular necrosis • Wound healing impaired • Pysch symptoms • Hyperpigmentation • Hypokalemic alkalosis
Pseudo-Cushing Physical and biochemical abnormalities mimicking Cushing’s syndrome without hormone producing tumor. Treating the cause abolishes symptoms. Alcoholism Depression Anorexia nervosa (high urine free cortisol) Bulimia nervosa Familial cortisol resistance Familial partial lipodystrophy type I
Diagnosis is based on a review of the patient's medical history, physical examination and laboratory tests. No specific general laboratory signs Screening evaluation for suspected Cushing’s • Basic hormone levels • Diurnal rhythm • 24 hour urine free cortisol • Dexamethasone suppression tests • CRH test • Petrosal Sinus Sampling
Basic hormone levels – in the morning:
plasma cortisol, ACTH, androgens (central: TSH, LH/FSH, PRL)
Diurnal rythm: Cushing sy. is characterized by a loss of circadian
rhythmicity.
plasma cortisol: at night 23-24 h cortisol < 5 ug/dl,
morning cortisol 8-25 ug/dl
salivary cortisol is in equilibrium with the free, biologically active
portion of cortisol in the plasma. Not intended to replace the current
standard screening test, - however, the salivary cortisol test is useful for
patients suspected due to the convenience of sample collection,
24 hour urin free cortisol
Reflects cortisol production. Always measure urinary creatinine to insure
completeness of collection. Levels higher than 50–100 micrograms a day for an adult
suggest Cushing's syndrome. The normal upper limit varies in different laboratories,
depending on which measurement technique is used.
Pseudo-Cushing fake positive results!!Dexametason supression tests
Dexamethason is a synthetic steroid. It inhibits CRH/ACTH production in
hypothalamus/hypophysis, however do not influence cortisol measurement.
_1. Low dose dexamethason test
„overnight”test, around midnight patient takes 1 mg dexamethason
blood sampling is next morning
normally: cortisol < 1,8 ug/dl (suppressed)
2 days test: patient takes 0,5mg dexamethason in every 6 hour
urine UFC < 10ug/24h
plasma cortisol < 5 ug/dl 6 h later than last dose of
dexamethason
< 2 ug/dl 2 h later than last dose of
dexamethason
intravenous test if oral test is not possible ( eg. malabsorption)b. High dose dexametason test: Helps to distinguish patients with excess production of ACTH due to pituitary adenomas from those with ectopic ACTH-producing tumors. Pituitary adenomas can still react to high levels of steroids. „overnight”test, patient takes 8 mg dexamethason, blood sampling is next morning, normally cortisol decreases by 50% 2 days test: patient takes 2mg dexamethason in every 6 hour Plasma cortisol decreases < 50% adrenal gland, > 50% central intravenous test if oral test is not possible ( eg. malabsorption)
Other tests to distinguish Cushing’s Disease and ectopic Cushing CRH test: Central Cushing– ACTH producing cells react – ectopic Cushing no reaction Synthetic CRH intravenously (1 ug/bwkg maximum: 100ug) Blood sampling (cortisol, ACTH) -15, 0, 15, 30, 45, 60, 90, and 120 minutes Plasma cortisol raise 20% or higher and ACTH raise 40% or higher is diagnostic
Petrosal Sinus Sampling_ This test is not always required, but in many cases, it is the best way to separate pituitary from ectopic causes of Cushing's syndrome. Samples of blood are drawn from the petrosal sinuses, veins which drain the pituitary, by introducing catheters through the femoral vein in the upper thigh/groin region, X-rays are used to confirm the correct position of the catheters. CRH is given during the test to improve diagnostic accuracy. Levels of ACTH in the petrosal sinuses are measured and compared with ACTH levels in the perifery vein. Central/periferial ratio is higher than 2 at baseline or higher than 3 after CRH is diagnostic No change in ACTH level suggest ectopic ACTH syndrome.
Radiologic Imaging Imaging tests reveal the size and shape of the pituitary and adrenal glands and help determine if a tumor is present. The most common are the CT (computerized tomography) scan – adrenal land MRI (magnetic resonance imaging)--- pituitary gland Imaging procedures are used to find a tumor after a diagnosis has been established. Imaging is not used to make the diagnosis of Cushing's syndrome because benign tumors, sometimes called "incidentalomas," are commonly found in the pituitary and adrenal glands.
Therapy: surgery
Regardless of the adenoma's location, most patients will require steroid
replacement postoperatively at least in the interim as long-term
suppression of pituitary ACTH and normal adrenal tissue does not
recover immediately. Clearly, if both adrenals are removed, replacement
with hydrocortisone is imperative.
1. hypohysis adenoma
Transsphenoidal or supraciliar
After surgery: HORMONE REPLACEMENT????!!!!
1. Baseline hormone levels right after surgery: ACTH, TSH, cortisol,
than 2-3 month later revision and LH, FSH, (GH) PRL
• test for diabetes insipidus (urine amount and, specific gravity)
2. Test of the adrenal gland Synacten test (synthetic ACTH)
Stimulation, if adrenal glands function normally plasma cortisol raise
over > 18ug/dlNelson's syndrome is the rapid enlargement of a pituitary adenoma that occurs after the removal of both adrenal glands. Removal of both adrenal glands, is a rare operation for Cushing’s syndrome to eliminate production of cortisol. The lack of cortisol's negative feedback can allow any preexisting (undetectable) pituitary adenoma to grow unchecked.
Treatment II
Hypophysis adenoma: radiotherapy
childhood
residual tumor
if surgery is not possible
recurrent tumor
gamma-knife
There is a delay from the time radiation therapy is initiated until the
time it takes effect on hypercortisolism; therefore, medical therapy
is initiated and continued for some time until the radiation therapy
takes effect during the lag period.
Hypopituitaris mostly always occursChemical adrenalectomy
Congenital adrenal hyperplasia
Congenital Adrenal Hyperplasia • Congenital Adrenal Hyperplasia (CAH) is an inherited autosomal recessive disease • Enzyme defects affecting cortisol, aldosteron in rare cases sexual steroid synthesis • 90-95% of cases are caused by 21-hydroxylase, deficiency
21 hydroxylase deficiency
(symptoms depends on enzyme defect severity)
Three forms:
1. Salt wasting form (classical CAH 75%)
• Severe cortisol and aldostrone synthesis defect
• Within 6 weeks after birth : hypadrenic crisis (Dehydration,
vomiting and diarrhoea, hyponatreamia, hyperkalemia, acidosis,
hypoglycemia, shock)
• masculinization in females / ambiguous genitalia
LIFE TREATENING STATE!! If not treated fatal
Diagnosis: high serum 17 hydroxy-progesteron
Therapy: cortisol (hydrocortione) and mieralocorticoid
(fludrocortison) supplementation
Prenatal treatment of mother with glucocorticoids (dexamethasone) can
prevent/reduce the virilizing effects of fetal 21-hydroxylase deficiency21 hydroxylase deficiency
2. Simple virilizing form (classical CAH: 25%)
masculinization in females / ambiguous genitalia
excess prenatal production of androgens
hyperpigmentation (high ACTH)
males are usually normal at birth.
Linear growth is accelerated at the beginning, but epiphyses fuse
early
3. Non-classical CAH
* Milder than classical CAH (normal genitalia, hirsutism, irregular
cycles, infertility)
* Androgen excess can cause precocious puberty in both sex
* Males are often undiagnosed / asymptomatic
Diagnosis: 17-OH-progeszteron > 2 ng / ml (follicular phase
ACTH stimulating test (Synacthen)
60 min: 17-OH-progeszteron > 10 ng / ml
Therapy: Oral anticontraceptive, antiandrogensDiagnosis Elevated blood levels of ACTH, 17-hydroxyprogesterone, Androstendion Diferential diagnosis: –True hermaphorditism –Pseudohermaphroditism –Sex chromosome abnormalities None have high 17-hydroxyprogesterone. Treatment: glucocorticoid supplementation – ACTH decreases – 17 OH progesterone decreases
Other forms of CAH 11 beta- hydroxylase 1 in 100,000 live births Females virilized; salt-wasting is rare 17 alpha- hydroxylase less than 1% Males virilized; females fail to achieve puberty. Salt-wasting not observed. 3 beta- hydroxysteroid dehydrogenase: extreme rare Males virilized; female virilization mild. Salt-wasting may be seen. StAR rare ales virilized; females fail to achieve puberty. Salt- wasting occurs.
Thank you!
You can also read

















































