DEMENTIA CAREGIVER NEEDS - CAREGIVER NEEDS EXIST AND CAN BE ADDRESSED AT ALL STAGES OF THE DEMENTIAS. BY NANCY A. HODGSON, RN, PHD, FAAN ...
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
DEMENTIA CARE
APPROACHES
Dementia Caregiver Needs
Caregiver needs exist and can be addressed at all stages of the dementias.
By Nancy A. Hodgson, RN, PhD, FAAN
It is important to assess the needs of demen- care. The focus at this time is necessarily on the person with
tia caregivers throughout the disease trajectory. dementia and the caregiver may not be present or identified at
This begins at the point of diagnosis, often this time. If a potential caregiver is in the room, the astute clini-
before family or friends identify themselves as cian will assume they have questions and concerns and ask for
caregivers. and evolves and changes as demen- those to be shared after the patient has first had the opportu-
tia progresses.1-3 As the balance of care shifts nity to share their questions and concerns. Creating this oppor-
over time, the questions used to assess needs of the person tunity to ask questions and sharing available resources is often
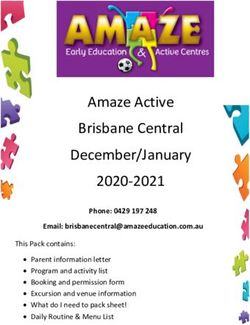
with dementia and their caregiver(s) also shift (Figure). all caregivers can take in at this stage of disease.
There are many resources for educating individuals with
At Diagnosis dementia and their caregivers (Box), including the Alzheimer’s
At the point of diagnosis, the primary need of caregiv- Association, which has a wealth of information useful not just
ers is to have accurate, understandable information about for AD, but for multiple types of dementia. If a more specific
dementia, and the specific disease underlying the dementia, diagnosis is given, there are other resources oriented specifi-
such as Alzheimer disease (AD). Most people think of AD as cally to those conditions (eg, frontotemporal dementia or
a disease affecting memory and are unaware of the commu- Lewy body disease). Often people are diagnosed with a mixed
nication challenges, executive dysfunction, neuropsychiatric dementia, making multiple resources appropriate and useful.
symptoms, and other challenges that affect daily functioning Information about the need for legal and financial plan-
as dementia progresses. These challenges are particularly dif- ning including medical power of attorney, potential long-
ficult for caregivers to address because they limit the ability term care, and property arrangements should be provided.
of the person with dementia to communicate their needs If this is not done at the time of diagnosis, it should be
and to perform complex tasks previously done with ease. done at the first follow-up visit. Although early planning
Helping both the person with dementia and their caregiver can be difficult for patients and their loved ones, it allows
become aware of what to expect with disease progression the person with dementia to be involved and express their
with knowledge, assessment, and referral to appropriate wishes for future care and decisions. This eliminates guess-
educational resources is paramount at this stage.3-6 work for families and allows for the person with dementia
As with any chronic and terminal illness, delivering a diag- to designate decision makers on their behalf. Early planning
nosis to a person with dementia requires thoughtfulness and also allows time to work through the complex legal and
financial issues that are involved in long-term care.7
It is important to note that for some populations, diagnosis
may occur further along in disease progression. This includes
underserved and high-risk communities including underrep-
resented minority groups.4,8,9 As such addressing caregivers’
needs also requires careful attention to cultural norms and
psychosocial resources of the specific individual and family.3,8,9
During Follow-Up Care
As the needs of the person with dementia increase over
time, so too do the needs of caregivers. During follow-up visits,
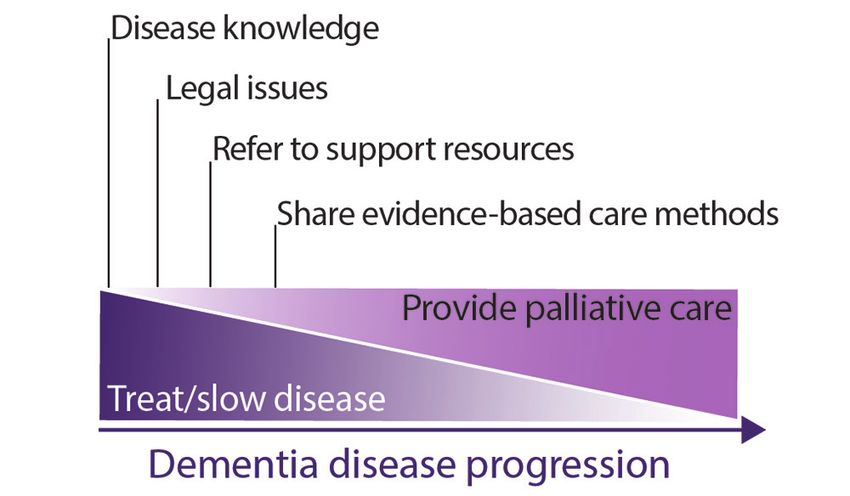
Figure. As dementia progresses, so too do caregiver needs. As it is important to ask caregivers how they are spending their
modeled here, efforts to maintain cognitive reserve and treat or days and what aspects of caring are presenting challenges for
slow the disease gradually decrescendo, palliative care needs them. Caregivers should be asked about what help they have
increase and become essential, focused on symptomatic treat- with caregiving. Because of the stigma associated with demen-
ment to preserve quality of life for as long as possible. tia, many caregivers are at risk for social isolation. Referrals to
48 PRACTICAL NEUROLOGY JUNE 2021
DEMENTIA CARE
APPROACHES
Box. Selected Online Educational by caregivers. Connecting caregivers to social agencies that
offer support for elders and people with dementia is use-
Resources for Dementia ful and may provide opportunities to learn evidence-based
Alzheimer’s Association www.alz.org approaches in dementia care.
Educational information and other resources for people In mid- and later stages of dementia, common neuropsy-
with all types of dementia, including a helpline (800-729- chiatric symptoms many include repetitive questioning, rum-
3900), available 24 hours a day, 7 days a week. maging through belongings, responding to visual cues out of
Benjamin Rose Institute on Aging benrose.org
context, restlessness, and increased roaming and other unsafe
A nonprofit providing services to people in Ohio that also has
behaviors. These symptoms often require increased vigilance
several useful online tools.
on the part of caregivers that is both mentally and physically
exhausting.16-20 This is likely frustrating for a caregiver if they
Family Caregiver Alliance www.caregiver.org do not understand these behaviors as part of the disease—
A community organization providing online resources to that the person with dementia is expressing a need through
anyone from anywhere. Individuals can answer an online behavior that they may no longer be able to express verbally.
questionnaire and receive tailored resources from FCA staff. Helping the caregiver to see that there is usually a need or
Lewy Body Dementia Association www.lbda.org specific stimulus that underlies these behaviors (eg, hunger,
Information and resources specific to Lewy body dementia. discomfort, bathroom needs, visual and auditory stimuli, and
even boredom) can be extremely helpful.
National Institute on Aging (NIA) www.nia.nih.gov
Evidence-based behavioral interventions have been shown
Part of the US Department of Health and Human Services
to help improve caregiver quality of life, some of which
National Institute of Health, provides information on health
also reduce symptom severity for persons with dementia
and disease for elders and their caregivers.
(Table).21-26 Interventions that are variations of person-
National Association of Area Agencies on Aging centered care teach caregivers how to identify underlying
www.n4a.org causes of symptoms with problem-solving skills (eg, Describe-
A nonprofit network of local agencies providing services for Investigate-Create-Evaluate [DICE], Treatment Routes for
elders in the community, including those with dementia. Exploring Agitation [TREA], Tailored Activity Programs [TAP},
Research Institute on Aging By Us For Us Guides and Dementia Care Mapping [DCM]).27-32 In general, these
the-ria.ca/resources/by-us-for-us-guides/ systems provide structured approaches to problem solv-
From the Research Institute on Aging at the University of ing—understanding why symptoms occur when they do.
Waterloo in Canada, these guides, available for free download This approach can empower caregivers to manage symptoms
or for purchase in print, were created by a group of people with simple behavioral interventions and diminish the sense
living with dementia and their care partners. of being overwhelmed. A database of over 40 evidence-based
dementia care interventions is available at https://bpc.caregiv-
The Association for Frontotemporal Dementia er.org/#searchPrograms. Using this database, individuals and
www.theaftd.org organizations can filter and compare programs by dementia
Information specific to frontotemporal dementia. type and other characteristics as well as evidence of benefits.
A Quick Look at Alzheimer’s aboutalz.org When resources are not available locally, it is helpful for
A series of 5 videos, each 2 to 3 minutes long, that provide clinicians to understand the basics of these programs and be
introductory education in a highly digestible format. able to refer caregivers to websites and apps that can guide
them in the use of these methods. It is important for clinicians
counseling, support groups, and social agencies may be made to recognize that nonpharmacologic interventions are often
as needed.10-12 Caregivers who are part of a church or a spiri- the most appropriate and effective approach to reduce for
tual community may also find sources of support there, and neuropsychiatric given the risk and side effects of appropri-
clinicians can ask caregivers about their spiritual practices to ate, pharmacologic treatments (See Behavioral Approaches in
connect them to such supports when available.13-15 Dementia Care in this issue). The benefits of these programs
As individuals with dementia experience declines in for caregivers include reduced stress and improved health
executive function and communication, neuropsychiatric outcomes for caregivers. For persons living with dementia,
symptoms tend to emerge. These can be among the larg- these programs improves quality of life and prolongs the time
est challenges for caregivers often because of low awareness before assisted living or long-term care is needed
that these issues are part of the dementia disease process. Clinicians also play an important role in supporting caregiv-
Yet, with understanding and evidence-based behavioral ers to implement evidence-based care programs that address
approaches, many of these can be managed successfully safety concerns. This includes helping to assess when driving
JUNE 2021 PRACTICAL NEUROLOGY 49DEMENTIA CARE
APPROACHES
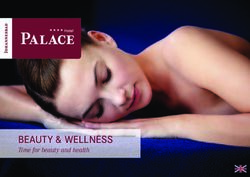
TABLE. EVIDENCE-BASED CARE INTERVENTIONS THAT IMPROVE CAREGIVERS’ QUALITY OF LIFE
Program Delivery model Results of intervention
Active Caregiving: Weekly 2-hour session for 4 weeks led by trained layper- Decreased caregiver depression symptoms and
Empowering Skills (ACES) son professional or paraprofessional improved quality of life for caregiver
Adult Day Services Plus Skills training and check-ins from trained professional or Decreased caregiver depression symptoms,
(ADS Plus) paraprofessional for skills-training, education, and resourc- improved caregiver confidence and skills, and
es. Up to 8 sessions (15 minutes-1 hour) over 1-year improved caregivers' quality of life.
Mindfulness Training for Weekly 90-minute sessions for caregivers over 8 weeks Decreased depression symptoms, improved
Patients with Progressive led by professional or paraprofessional, focused on confidence and skills, quality of life, and health
Cognitive Decline and meditation, movement, yoga for caregivers; also improved depression symp-
their Caregivers Program toms, severity of other symptoms, stress, and
quality of life for person with dementia
REACH TX 4 in-person sessions for caregiver and person with Decreased depression symptoms, improved
dementia with professional or paraprofessional over confidence and skills, quality of life, and health
6-month period for caregivers; decreased symptom severity and
increased independence for activities of daily liv-
ing for person with dementia
Savvy Caregiver Weekly 2-hour session for 6 weeks in-person or online Decreased depression symptoms, improved
from trained layperson, paraprofessional or professional confidence and skills, quality of life, and health
focused on caregiving knowledge and skills, coping with for caregivers; decreased symptom severity for
stress, and encouraging persons living with dementia to person with dementia
participate in daily tasks and activities.
is no longer safe or when individuals can no longer be safe therapists and more that can benefit both patients and
out of the home by themselves. The loss of autonomy and caregivers. For some individuals, introducing a palliative
independence is incredibly difficult for most people living with approach focused on relieving symptoms and maintaining
dementia and their caregivers. When caregivers can refer back quality of life may even be beneficial at early stages of dis-
to clinician recommendations—“what the doctor said”—to ease progression (Figure).
support and reinforce these limits at home, caregivers and
person with dementia may both feel more able to respect Summary
those limitations. The caregiver may feel they have back-up, Clinicians can help meet dementia caregivers needs in
and the person living with dementia may feel supported by a many ways. Perhaps most important, is the simple recog-
team rather than emotionally upset with their family. nition that addressing caregivers needs improves health
outcomes for the person with dementia and the person
In Later Stages of Dementia who cares for them. With that in mind, it is important to
As dementia progresses toward late stages and higher lev- ask caregivers how they are doing; what concerns, worries,
els of care become necessary, transitioning to full-time care or challenges they have; and what they are doing to care
or assistive living can be among the largest of the challenges for themselves and the person with dementia. Having this
caregivers face. Engaging a palliative care approach focused information allows an astute clinician to provide educa-
on preserving dignity and quality of life can be beneficial tional resources, make referrals to community resources
for both persons with dementia and their caregivers.6,7,9,33-37 and social services, share information about evidence-
Whether an individual will die because of complications of based caregiving methods, and incorporate a palliative
the dementia, such as infection or falls or the actual disease approach as appropriate. n
causing the dementia, they will have dementia at the end
1. Gitlin LN, Hodgson NA. Who should assess the needs of and care for a dementia patient’s caregiver?. AMA J Ethics.
of their life. With this understanding, accessing a palliative 2016;18(12):1171-1181.
approach is increasingly recognized as best practice at this 2. Armstrong MJ, Gamez N, Alliance S, et al. Clinical care and unmet needs of Individuals with dementia with Lewy bodies and caregivers:
an interview study. Alzheimer Dis Assoc Disord. 2021;10.1097/WAD.0000000000000459. doi:10.1097/WAD.0000000000000459
stage. Some hospice programs are even beginning to offer 3. Kovaleva MA, Jennings BM, Song MK, Clevenger CK, Griffiths PC, Hepburn K. Caregivers’ experience at an integrated memory care
dementia care even though it can be difficult to prognosti- clinic. Res Gerontol Nurs. 2021;14(2):69-78. doi:10.3928/19404921-20210115-01
4. Abramsohn EM, Paradise KM, Glover CM, et al. CommunityRx: optimizing a community resource referral intervention for minority
cate life expectancy for people with dementia. dementia caregivers. J Appl Gerontol. 2021;7334648211005594. doi:10.1177/07334648211005594
5. Bruinsma J, Peetoom K, Bakker C, et al. Tailoring and evaluating the web-based ‘Partner in Balance’ intervention for family caregiv-
Palliative care offers a whole team approach that ers of persons with young-onset dementia. Internet Interv. 2021;25:100390. doi:10.1016/j.invent.2021.100390
includes social workers, clergy members, nurses, physicians,
(Continued on page 54)
50 PRACTICAL NEUROLOGY JUNE 2021DEMENTIA CARE
APPROACHES
(Continued from page 50)
6. Barrado-Martín Y, Nair P, Anantapong K, et al. Family caregivers’ and professionals’ experiences of supporting people living with
dementia’s nutrition and hydration needs towards the end of life. Health Soc Care Community. 2021;10.1111/hsc.13404.
7. Nguyen T, Levkoff S, Nguyen H. ‘He is just getting old, you know’: the role of cultural and health beliefs in shaping the help-seeking
process of family members caring for persons with dementia in Vietnam Ethn Health. 2021;1-22.
8. Leggett AN, Bugajski BC, Gitlin LN, Kales HC. Characterizing dementia caregiver style in managing care challenges: cognitive
and behavioral components]. Dementia (London). 2021;1471301220988233. doi:10.1177/1471301220988233
9. Geshell L, Kwak J, Radhakrishnan K. Perspectives and experiences of persons with dementia with advance care planning: an
integrative literature review. J Geriatr Psychiatry Neurol. 2019;32(5):231-245.
10. Faw MH, Luxton I, Cross JE, Davalos D. Surviving and thriving: qualitative results from a multi-year, multidimen-
sional intervention to promote well-being among caregivers of adults with dementia. Int J Environ Res Public Health.
2021;18(9):4755.
11. Lauritzen J, Pedersen PU, Sørensen EE, Bjerrum MB. The meaningfulness of participating in support groups for informal
caregivers of older adults with dementia: a systematic review. JBI Database System Rev Implement Rep. 2015;13(6):373-
433.
12. Leggett AN, Meyer OL, Bugajski BC, Polenick CA. Accentuate the positive: the association between informal and formal
supports and caregiving gains. J Appl Gerontol. 2021;40(7):763-771.
13. Friedrich R, Woods B, Williams S. ‘Just because the mind is confused it doesn’t mean the spirit is confused’: exploring the
role of Anglican clergy in ministry to persons with dementia. Dementia (London). 2021;20(2):698-716.
14. Sun F, Hodge DR. Latino Alzheimer’s disease caregivers and depression: using the stress coping model to examine the
effects of spirituality and religion. J Appl Gerontol. 2014;33(3):291-315.
15. Heo GJ, Koeske G. The role of religious coping and race in Alzheimer’s disease caregiving. J Appl Gerontol. 2013;32(5):582-604.
16. Belle SH, Burgio L, Burns R, et al. Enhancing the quality of life of dementia caregivers from different ethnic or racial groups:
a randomized, controlled trial. Ann Intern Med. 2006;145(10):727-738.
17. Kim SK, Park M. Effectiveness of person-centered care on people with dementia: a systematic review and meta-analysis.
Clin Interv Aging. 2017;12:381-397.
18. Judge KS, Yarry SJ, Looman WJ, Bass DM. Improved strain and psychosocial outcomes for caregivers of individuals with
dementia: findings from Project ANSWERS. Gerontologist. 2013;53(2):280-292.
19. Eikelboom WS, Singleton E, van den Berg E, et al. Early recognition and treatment of neuropsychiatric symptoms to
improve quality of life in early Alzheimer’s disease: protocol of the BEAT-IT study. Alzheimers Res Ther. 2019;11(1):48.
20. Gerlach LB, Kales HC. Managing behavioral and psychological symptoms of dementia. Clin Geriatr Med. 2020;36(2):315-327.
21. Gitlin LN, Marx K, Scerpella D, et al. Embedding caregiver support in community-based services for older adults: A multi-
site randomized trial to test the Adult Day Service Plus Program (ADS Plus). Contemp Clin Trials. 2019;83:97-108.
22. Stevens AB, Smith ER, Trickett LR, McGhee R. Implementing an evidence-based caregiver intervention within an integrated
healthcare system. Transl Behav Med. 2012;2(2):218-227.
23. Cho J, Luk-Jones S, Smith DR, Stevens AB. Evaluation of REACH-TX: a community-based approach to the REACH II
intervention [published correction appears in Innov Aging. 2019 Nov 14;3(3):igz041]. Innov Aging. 2019;3(3):igz022.
doi:10.1093/geroni/igz022
24. Sherman CW, Steiner SC. Implementing sustainable evidence-based interventions in the community: a fidelity-focused
training framework for the Savvy Caregiver program. J Appl Gerontol. 2018;37(12):1450-1471.
25. Hepburn K, Lewis M, Tornatore J, Sherman CW, Bremer KL. The Savvy Caregiver program: the demonstrated effectiveness
of a transportable dementia caregiver psychoeducation program. J Gerontol Nurs. 2007;33(3):30-36.
26. Griffiths PC, Whitney MK, Kovaleva M, Hepburn K. Development and implementation of Tele-Savvy for dementia caregiv-
ers: a Department of Veterans Affairs clinical demonstration project. Gerontologist. 2016;56(1):145-154.
27. Brooker D. Dementia care mapping: a review of the research literature. Gerontologist. 2005;45 Spec No 1(1):11-18.
28. van de Ven G, Draskovic I, van Herpen E, et al. The economics of dementia-care mapping in nursing homes: a cluster-
randomised controlled trial. PLoS One. 2014;9(1):e86662. doi:10.1371/journal.pone.0086662
29. Cohen-Mansfield J, Thein K, Marx MS, Dakheel-Ali M, Freedman L. Efficacy of nonpharmacologic interventions for agita-
tion in advanced dementia: a randomized, placebo-controlled trial. J Clin Psychiatry. 2012;73(9):1255-1261.
30. Cohen-Mansfield J, Libin A, Marx MS. Nonpharmacological treatment of agitation: a controlled trial of systematic
individualized intervention. J Gerontol. 2007;62(8):908-916.
31. DiNapoli EA, Scogin F, Bryant AN, Sebastian S, Mundy MJ. Effect of individualized social activities on quality of life
among older adults with mild to moderate cognitive impairment in a geriatric psychiatry facility. Aging Ment Health.
2016;20(3):262-270.
32. Möhler R, Renom A, Renom H, Meyer G. Personally tailored activities for improving psychosocial outcomes for people with
dementia in long-term care. Cochrane Database Syst Rev. 2018;2(2):CD009812. doi:10.1002/14651858.CD009812.pub2
33. Eisenmann Y, Golla H, Schmidt H, Voltz R, Perrar KM. Palliative care in advanced dementia. Front Psychiatry. 2020;11:699.
34. Hines S, McCrow J, Abbey J, et al. The effectiveness and appropriateness of a palliative approach to care for people with
advanced dementia: a systematic review. JBI Libr Syst Rev. 2011;9(26):960-1131.
35. Bolt SR, van der Steen JT, Khemai C, Schols JMGA, Zwakhalen SMG, Meijers JMM. The perspectives of people with demen-
tia on their future, end of life and on being cared for by others: a qualitative study. J Clin Nurs. 2021;10.1111/jocn.15644.
36. Roβmeier C, Hartmann J, Riedl L, et al. How do persons with young and late onset dementia die?. J Alzheimers Dis.
2021;81(2):843-852. doi:10.3233/JAD-210046
37. Bernstein Sideman A, Harrison KL, Garrett SB, Naasan G; Dementia Palliative Care Writing Group, Ritchie CS. Practices, chal-
lenges, and opportunities when addressing the palliative care needs of people living with dementia: specialty memory care
provider perspectives. Alzheimers Dement (N Y). 2021;7(1):e12144. doi:10.1002/trc2.12144
Nancy A. Hodgson, RN, PhD, FAAN
Chair and Professor of Nursing
Department of Biobehavioral Health Sciences
Anthony Buividas Term Chair in Gerontology
University of Pennsylvania School of Nursing
Philadelphia, PA
Disclosures
NAH reports no disclosures
54 PRACTICAL NEUROLOGY JUNE 2021You can also read