Dental abscess: A potential cause of death and morbidity - RACGP
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
FOCUS | CLINICAL
Dental abscess:
A potential cause of
death and morbidity
Kristen Bayetto, Andrew Cheng, PATIENTS WITH DENTAL ABSCESSES commonly the period 2002–19. This evidence-based
Alastair Goss initially present to their primary health experience forms the basis of this article.
providers, particularly if they have dental In this article, the authors examine
phobia or are financially constrained. It multiple factors associated with severe
Background
Dental abscess as an end stage of dental is easy to underestimate their condition, odontogenic infections, including:
disease is common in the community, and particularly if the infection has spread • the evidence base for the
patients with dental abscesses are likely beyond the confines of the jaws. In the pathophysiology, which includes the
to seek care from their primary health pre-antibiotic era, dental infection was anatomical basis, microbiology and
provider. Once the infection has spread a common cause of death, with fatality host factors
beyond the confines of the jaws, there is
an increasing risk of airway obstruction
rates of 10–40%.1 With the advent of • patient demographics
and septicaemia. If treated with antibiotics
antibiotics, odontogenic infections • initial assessment of airway risk and
alone, the infection will not resolve and will responded well to penicillin. This may assignment to low- or high-risk cases
become progressively worse. have created a false sense of security, and • hospital management and outcome,
such cases were usually treated by junior morbidity and mortality
Objective
This article reviews the pathophysiology,
hospital staff operating out of hours. It • identified risk factors
demographics and management of
may not have been noticed that antibiotic- • the financial burden.
severe odontogenic infections. It includes resistant bacteria were generally on the
evidence-based studies of a large increase. This was the situation at the
number of cases treated at a single Royal Adelaide Hospital in 2002 when Pathophysiology
tertiary hospital. a patient with a spreading odontogenic The onset of a dental abscess is usually
Discussion infection died of airway obstruction a few slow over many months. Dental decay
Prompt assessment and referral to a hours after operation (Case 1). This event takes several months to reach the dental
tertiary hospital is required for cases at resulted in an immediate review of the pulp. Pulpitis results in pain that is poorly
risk of airway compromise. The morbidity management of such cases, and an audit localised. When pulp necrosis finally
and mortality of cases is presented in this of all 88 inpatient cases treated in the year occurs, there is no pain. However, when
article, with discussion of risk factors and
2003 was performed.2 These key steps an acute periapical abscess develops, a
the financial burden on the health system.
were completed by the time of the coronial severe well-localised pain develops. At this
investigation in 2006.3 Subsequently, stage, the dental abscess is easily treated
there has been a further detailed audit by extraction or root filling. By this time,
of 672 patients in the period 2006–14.4 all patients have had intermittent episodes
Altogether, more than 1000 cases of of pain as a warning that something is
severe odontogenic infection have been wrong. Other causes of dental abscess are
managed at the Royal Adelaide Hospital in pericoronal infections around partially
© The Royal Australian College of General Practitioners 2020 REPRINTED FROM AJGP VOL. 49, NO. 9, SEPTEMBER 2020 | 563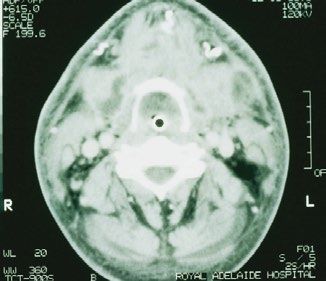
FOCUS | CLINICAL DENTAL ABSCESS
erupted impacted teeth or failed dental the mediastinum. It also connects to the study, the greater the range and type of
treatment.2 Thus, there are clear warning contralateral side.5 bacteria will be shown.8 Current hospital
symptoms; some patients ignore the It is essential to understand that bacteriological studies are usually brief,
symptoms while others receive temporary swelling from the submandibular spaces limited to indicating the general site
relief with antibiotics from medical or can extend over a wide area of the airway (eg oral or respiratory). It is best to involve
dental practitioners. Antibiotic treatment in both length and breadth (Figure 1). infectious disease consultants when
without dental treatment to remove the This is the basis of the term ‘Ludwig’s complex resistant cases are encountered.
cause always fails.2 angina’, with angina meaning ‘choking’. The most common organisms are viridans
Once the infection spreads beyond the Strictly, Ludwig’s angina only refers to streptococci initially, with the subsequent
confines of the jaws and into the soft tissue cases in which the whole neck bilaterally anaerobes being Fusobacterium spp. and
spaces, it becomes much more difficult to from the mandible to the clavicle is Prevotella spp.
treat and potentially life threatening. involved in infection. Such cases have A small but clinically important
a poor prognosis.6,7 However, the subgroup of odontogenic infections is
term ‘Ludwig’s angina’ is commonly those with necrotising fasciitis. Clinically,
Anatomical factors misinterpreted to apply to any localised these infections have extensive tissue
Anatomical factors play a key part in the neck infection.3 destruction, with gas within the tissues
progression of infection once beyond the The other critical area of dental and extensive spread. They are usually
confines of the teeth and jaws. Spread infection is the incisors, canines and associated with Serratia spp., Klebsiella
follows the line of least resistance, which premolars in the anterior maxilla, as oxytoca, Enterococcus faecalis and
is dictated by the fascia and muscles.5 The infections in these areas can spread via the Candida spp. Management of these cases
anatomical space involved depends on infraorbital veins to the ocular veins to the involves infectious disease input, and
the affected tooth. The most dangerous cavernous sinus. Spread is facilitated as patients face a long hospital stay.7
space is the submandibular space, which these veins have no valves.
is bounded by the mandible laterally,
the mylohyoid muscle above and the Pre-existing medical conditions
subcutaneous tissue and skin below. Microbiological factors If the patient is immunocompromised
It contains the submandibular gland, Odontogenic infections are polymicrobial (eg with human immunodeficiency
lymph nodes and the masseter muscle. with a mixture of aerobic, facultative virus/acquired immunodeficiency
When this muscle is irritated by the anaerobic and strict anaerobic organisms. syndrome, haematological neoplasms
inflammation, trismus or difficulty in jaw The deeper the infection, the more or poorly controlled diabetes), there
opening ensues. The submandibular space likely that the involved organisms are is likely to be increased difficulty in
is in direct contact with the pharyngeal anaerobic.4 Generally, the more skilled management and a longer hospital
spaces and down through the neck to and intensive the microbiological stay for the patient.
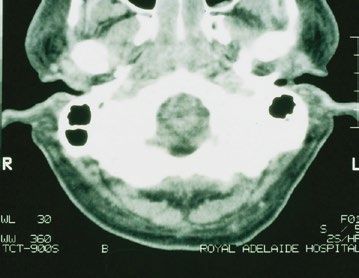
A B C
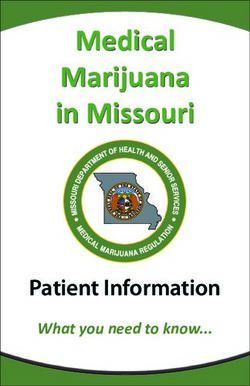
Figure 1. Serial axial computed tomography slices showing the extent of airway compromise in a patient with a left submandibular abscess
who was orally intubated
a. Complete obstruction of the nose and nasopharynx; b. Left aubmandibular pus collection and oropharyngeal obstruction around the tube;
c. Hypopharyngeal obstruction at the level of the hyoid bone with a shift of the airway to the right
Reproduced with permission from Uluibau I, Jaunay, T, Goss A, Severe odontogenic infections, Aust Dent J 2005;50(4 Suppl 2):S74–S81, doi: 10.1111/j.1834-
7819.2005.tb00390.x.
564 | REPRINTED FROM AJGP VOL. 49, NO. 9, SEPTEMBER 2020 © The Royal Australian College of General Practitioners 2020
DENTAL ABSCESS FOCUS | CLINICAL Older patients with cardiovascular whether the patient’s mouth opens
FOCUS | CLINICAL DENTAL ABSCESS
bilateral space involvement than unilateral the ICU. She was elderly and medically general dental practice. Unfortunately, less
space involvement (60% increase). Each compromised, and the odontogenic than half of all Australians have regular or
year of age added 1% to the length of stay. infection had been resolved. Three emergency-only dental care.13 If an abscess
Length of stay was particularly increased patients died of odontogenic- spreads beyond the tooth, it requires
for high-risk cases that involved ICU time; related septicaemia. All had medical dental treatment and will not respond to
for these patients, length of stay was 59% comorbidities and antibiotic resistance on antibiotics alone. If the infection spreads
longer than for those who did not require presentation. into the fascial planes of the neck or face,
prolonged intubation. In an attempt to further characterise risk then there is risk of airway compromise or
In a separate study of 256 patients factors, a detailed study was performed spread to the brain. Appropriate protocols
admitted to an ICU between 2008 and on antibiotic resistance. The study found of management have been established
2013, 230 patients had odontogenic that 10.8% of patients had penicillin- at tertiary hospitals, but there is still and
infections. Of these patients, all were resistant organisms. All had multiple morbidity and mortality.
intubated for an average of 1.5 days prior courses of antibiotics, either for the The condition of dental abscess can
(range: 0.7–2.6 days). Forty-eight per cent odontogenic infection or other conditions be prevented, but this requires better
had medical comorbidities, 2% required or both. As soon as antibiotic resistance access to dental care and careful antibiotic
a tracheostomy and 1% had ventilator- was discovered, they were changed to stewardship by all health professionals.
associated pneumonia. Two patients died broad-spectrum antibiotics on the advice
in the ICU, one of ventilator-associated of the infectious diseases service. It is
pneumonia and one of odontogenic recommended that antibiotic prescribing CASE 1
septicaemia.10 follows Therapeutic Guidelines, ‘Oral and A man aged 27 years, who was otherwise
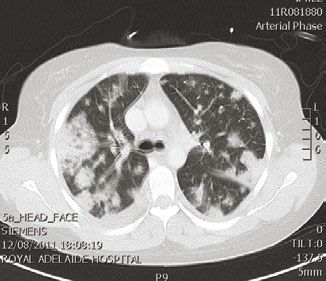
Examples of survival with serious dental’, Version 3.11 medically fit but a heavy smoker,
morbidity included descending Finally, the authors assessed the developed a toothache. He took no action
necrotising mediastinitis (Figure 2), with financial burden of spreading odontogenic beyond analgesics and at least one course
another patient developing a cerebral infections on the healthcare system. The of antibiotics over a four-month period.
mycotic aneurysm of the brain (Figure 3) burden is significant, with the average He then presented to a secondary hospital
with cavernous sinus thrombosis. cost for high-risk patients being $12,228. with a unilateral submandibular swelling
Another developed facial necrosis The total cost over the seven-year period and was directed to the Royal Adelaide
with blindness and required extensive was $5.65M. This needs to be compared Hospital. He presented there 12 hours
rehabilitation (Case 2). with the average cost of a single tooth later and was admitted.
Five patients died during the study extraction in private dental practice, which Under general anaesthesia, he had an
period. One died of airway obstruction is $181 (125 times less expensive).12 incision and drainage of the abscessed
(Case 1). None have died of airway right submandibular space. A general
obstruction since the airway protocol dentist had evidently previously extracted
was instituted in 2002. One patient Conclusion the tooth. As the patient had trismus, he
died of prolonged ventilation respiratory Dental abscess is a common preventable had a difficult fibreoptic intubation. At the
pneumonia that was acquired while in disease that can be simply treated in end of the procedure he was extubated
and sent to the ward.
He recovered from the anaesthetic, had
a shower and rang his mother to tell her
he was doing well. His mother felt that he
was not able to talk properly and told the
nurse. The nurse said she would call the
surgeon who performed the procedure
and told the patient to return to his bed.
He lay down and promptly developed
airway obstruction.
The surgeon and crash team were
present in
DENTAL ABSCESS FOCUS | CLINICAL
3. Coroner’s Court of South Australia. Findings of
Inquest – Daniel Brindley Salmon. Inquest number
CASE 2
27, 2006. Available at www.courts.sa.gov.au/
A woman aged 32 years who was CoronersFindings/Lists/Coroners%20Findings/
Attachments/341/SALMON%20Daniel%20
medically well but used intravenous Brindley.pdf [Accessed 24 June 2020].
drugs presented to the Royal Adelaide 4. Liau I, Han J, Bayetto K, et al. Antibiotic resistance
Hospital with a two-week history of in severe odontogenic infections of the South
Australian population: A 9-year retrospective
increasing facial swelling and trismus. audit. Aust Dent J 2018;63(2):187–92. doi: 10.1111/
In the two-week period she had obtained adj.12607.
two courses of antibiotics from a locum 5. Grodinsky M, Holyoke EA. The fasciae and fascial
spaces of the head, neck and adjacent regions.
medical service and was self-medicating Am J Anat 1938;63:367–408.
for the pain with street drugs. 6. Laskin DM. Anatomic considerations in diagnosis
On admission she had gross oral and treatment of odontogenic infections. J Am
Dent Assoc 1964;69:308–16. doi: 10.14219/jada.
sepsis, perioral necrotising fasciitis and archive.1964.0272.
multi-organ dysfunction. On the day 7. Juang YC, Cheng DL, Wang LS, Liu CY, Duh RW,
of admission, she was intubated and Chang CS. Ludwig’s angina: An analysis of 14
cases. Scand J Infect Dis 1989;21(2):121–25.
had a full dental clearance, drainage doi: 10.3109/00365548909039957.
of multiple infected spaces and 8. Sakamoto H, Kato H, Sato T, Sasaki J.
debridement of necrotic tissue. Wound Semiquantitative bacteriology of closed
odontogenic abscesses. Bull Tokyo Dent Coll
swabs grew both community-acquired 1998;39(2):100–07.
methicillin-resistant Staphylococcus 9. Central Northern Adelaide Health Network,
aureus and Candida tropicalis. The Standards and Procedures Committee. Acute
head and neck infections protocol. Adelaide
patient had little improvement despite SA: Royal Adelaide Hospital. Standards and
multiple drainages, debridement of Procedures Committee 2012.
10. Sundararajan K, Gopaldas JA, Somehsa H,
necrotic tissue and involvement of
Edwards S, Shaw D, Sambrook P. Morbidity and
an infectious disease consultant. She mortality in patients admitted with submandibular
developed cavernous sinus thrombosis space infections to the intensive care unit.
Anaesth Intensive Care 2015:43(3):420–22.
and had a cerebrovascular accident with 11. Oral and Dental Expert Group. Therapeutic
unilateral paresis and decreased vision. Guidelines: Oral and dental. Version 3. Melbourne,
She spent many weeks in intensive Vic: Therapeutic Guidelines Limited, 2019.
12. Han J, Liau I, Bayetto K, et al. The financial
care and was eventually discharged to burden of acute odontogenic infections: The
the rehabilitation centre at 180 days. South Australian experience. Aust Dent J
The patient survived but has multiple 2020;65(1):39–45. doi: 10.1111/adj.12726.
13. Ju X, Brennan DS, Spencer AJ. Age, period
permanent impairments including and cohort analysis of patient dental visits in
hemiparesis, partial blindness and Australia. BMC Health Serv Res 2014;14:13.
doi: 10.1186/1472-6963-14-13.
cognitive impairment.7
Authors
Kristen Bayetto MBBS, BDS, Advanced Oral and
Maxillofacial Surgery trainee, Royal Adelaide
Hospital, SA
Andrew Cheng MBBS, BDS, FRACDS (OMS),
Consultant Oral and Maxillofacial Surgeon, Royal
Adelaide Hospital, SA
Alastair Goss DDSc, FRACDS (OMS), Emeritus
Consultant, Royal Adelaide Hospital, SA; Emeritus
Professor, Oral and Maxillofacial Surgery, The University
of Adelaide, SA. alastair.goss@adelaide.edu.au
Competing interests: None.
Funding: None.
Provenance and peer review: Commissioned,
externally peer reviewed.
References
1. Wilwerding T. History of dentistry 2001. Available
at www.freeinfosociety.com/media/pdf/4551.pdf
[Accessed 24 June 2020].
2. Uluibau IC, Jaunay T, Goss AN. Severe odontogenic
infections. Aust Dent J 2005;50(4 Suppl 2):S74–S81.
doi: 10.1111/j.1834-7819.2005.tb00390.x. correspondence ajgp@racgp.org.au
© The Royal Australian College of General Practitioners 2020 REPRINTED FROM AJGP VOL. 49, NO. 9, SEPTEMBER 2020 | 567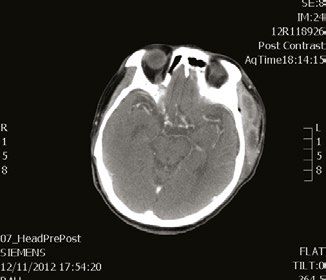
You can also read