Dr. Anwar I. El-Sheikh Khalil - By
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
By:
Dr. Anwar I. El-Sheikh Khalil
Consultant Pediatrician and Neonatologist
C.A.B.P (Arab Board), D-Ped, A.M.S
Fellowship
Former Director of Al-Nassr Pediatric
Deputy Dean Islamic University of Gaza
INFECTIOUS DISEASES

Infectious diseases
Cause Maculopapular rash Papulovesicular
Viral Measles, Rubella, Small pox
Roseola infantum Chicken pox
Erythema infectiosum Herpes simplex
Infect. Mononucleosis Coxsackie virus
Echo, Coxsackie virus
Bacterial Scarlet fever Impetigo
Meningococcemia
Typhoid fever
Fungal Tinea Tinea
Allergic Insect bite Insect bite
Parasitic Scabies -
Collagen SLE, Rheumatoid -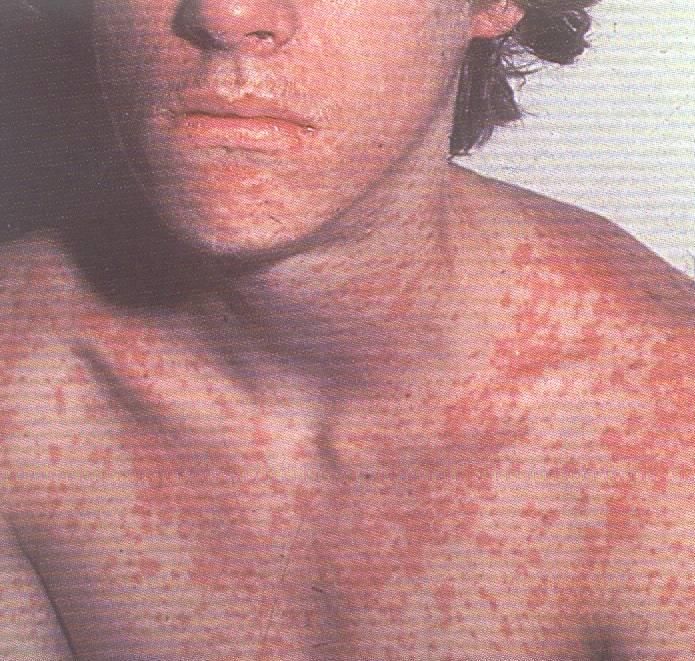
Primary Skin Lesions
Macule Change in skin colour but not felt
Papule Palpable skin lesion < 1cm
If > 1cm : nodule
Vesicle Raised, fluid filled lesion 0.5 cm : bullus
Pustule Vesicle containing pus
plaques Aggregation of any primary lesions
Macules

papules

Vesicle

bullae

Pustule

Several plaques on the arm
Papules and plaques
Macules and patches
weal
Secondary Skin Lesions
Scales Compressed layers of stratum cornium cells
that are raised on skin surface
Ulcers Excavation of necrotic tissue
excoriations Linear ulcers caused by scratching
fissures Splitting or cracking of skin
crusts Accumulation of blood,serum,pus and
epithelial debris on the surface of a weeping
lesionscales
ulcer
Scabies
crusts
Primary lesions Petechiae: pin point bleeding(platelet problem) Ecchymosis: large bleeding hematoma: large bleeding leading to swelling of skin.
Measles
انسبج 14/7/1431هـ -انًىافق
26/6/2010
أدي حفشٍ انحصبت فٍ يالوٌ إنً وفاة 82شخصا أؼهبهى أطفال ،وأصُب أكثز
يٍ 17أنفا آخزٍَ يُذ حفشٍ انًزض قبم َحى سخت أشهز.
وقال يذَز خذياث انصحت انىقائُت بىسارة انصحت فٍ يالوٌ سخىرٌ كابىنىسٌ
إٌ انجهىد حبذل نخطعُى انًعزضٍُ نخطز أكبز.
وأضاف أَه جزي حسجُم 82وفاة أؼهبهى أطفال و 17496حانت حزاكًُت فٍ
انشهىر انسخت انًاضُت يُذ انبالغ عٍ أول حفش نهحصبت فٍ َُاَز/كاَىٌ انثاٍَ هذا
انعاو.
وأشار انًسؤول انصحٍ إنً أٌ انحكىيت بذأث حًهت حطعُى حزكش عهً انًُاطق
انزَفُت حُث َعُش %80يٍ انسكاٌ انبانػ عذدهى 13يهُىٌ َسًتETIOLOGY RNA virus in the family Paramyxoviridae. 6 major structural proteins.
EPIDEMIOLOGY Historically: USA:90% of children acquiring the infection before 15 yr of age. the incidence declined dramatically following the introduction of the measles vaccine 1963. It is most common in the winter and spring. A nationwide : 1989–1991 resulting in >55,000 cases, 11,000 hospitalizations, and 123 deaths, The current rate is
TRANSMISSION through the respiratory tract or conjunctivae. Droplet Patients are infectious from 3 days before the rash up to 4–6 days after its onset. 90% of the exposed develop measles. viable virus may be suspended in air up to 1 hr after a source case leaves a room.
PATHOLOGY
necrosis of the respiratory tract epithelium.
lymphocyte infiltrate.
small vessel vasculitis on the skin and on the oral mucous
membranes.
Histology :
- intracellular edema and dyskeratosis
- formation of epidermal syncytial giant cells with up to 26 nuclei.
Viral particles are identified within the giant cells.
lymphoid hyperplasia is prominent.
Warthin-Finkeldey giant cells: pathognomonic for measles, with
up to 100 nuclei and intracytoplasmic and intranuclear inclusions.PATHOGENESIS
4 phases: incubation period, prodromal illness, exanthematous phase, and
recovery.
Incubation:
-measles virus migrates to regional lymph nodes.
-primary viremia : virus spreads to the reticuloendothelial system.
-secondary viremia spreads virus to body surfaces.
prodromal illness:
- begins following the secondary viremia.
- associated with epithelial necrosis and giant cell formation in body tissues.
- killing of cells including CNS
- viral replication
exanthematous phase: -with onset of the rash, antibody production begins and
viral replication and symptoms begin to subside.
-Measles virus also infects CD4+ T cells, resulting in suppression of the Th1
immune response.CLINICAL
MANIFESTATIONS
I.P: 8–12 days
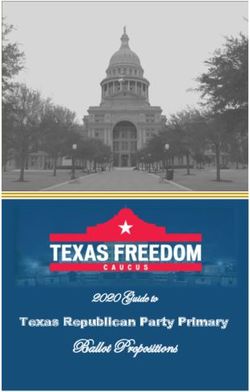
high fever, an enanthem, cough, coryza, conjunctivitis, and a prominent
exanthem.
the prodromal phase begins with a mild fever followed by the onset of
conjunctivitis with photophobia, coryza, a prominent cough and increasing
fever.
Koplik spots (enanthem):
-pathognomonic sign of measles
-appears 1 to 4 days prior to the onset of the rash
- first appear as discrete red lesions with bluish white spots in the center on
the inner aspects of the cheeks at the level of the premolars.
-may spread to involve the lips, hard palate, and gingiva.
-may occur in conjunctival folds and in the vaginal mucosa.
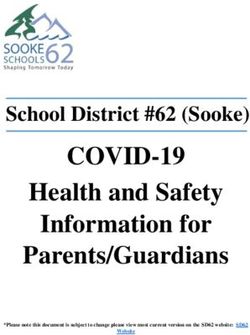
-reported in 50–70% of cases but probably occur in the great majorityCLINICAL MANIFESTATIONS Symptoms increase for 2–4 days until the 1st day of the rash. The rash begins around the forehead (around the hairline), behind the ears, and on the upper neck as a red maculopapular eruption. spreads downward to extremities, reaching the palms and soles in up to 50% of cases.
CLINICAL
MANIFESTATIONS
With the onset of the rash, symptoms begin to
subside.
rash fades over about 7 days in the same
progression.
leaving a fine desquamation of skin.
cough lasts the longest, often up to 10 days. In
more severe cases,
generalized lymphadenopathy may be present,
with cervical and occipital lymph nodesINAPPARENT MEASLES INFECTION Subclinical infection: -In individuals with passively acquired antibody,as with blood products -rash may be indistinct, brief, or, rarely, entirely absent. -also who received vaccine when exposed to measles may develop a rash but few other symptoms. - Persons with inapparent or subclinical measles do not shed measles virus and do not transmit infection to household contacts. atypical measles: severe measles at the time of receiving original formalin- inactivated measles vaccine - Patients had onset of high fever and headache followed by the appearance of a maculopapular rash on the extremities that become petechial and purpuric and progressed in a centripetal direction. -frequently complicated by pneumonia and pleural effusions. - development of circulating immune complexes that formed due to an abnormal immune response to the vaccine.
LABORATORY FINDINGS The diagnosis is clinical. Laboratory: - decr. Total WBCs and lymphocytes. If complicated by bacterial infection, the ESR and CRP levels are normal
DIAGNOSIS serum (IgM) antibody. - appears 1–2 days after the onset of the rash and remains for 1 mo. 4-fold rise in IgG. Viral isolation from blood, urine, or respiratory secretions PCR.
DIFFERENTIAL DIAGNOSIS rubella, adenoviruses, enteroviruses, Epstein-Barr virus. Exanthem subitum (in infants) erythema infectiosum (in older children) Mycoplasma pneumoniae Gp A streptococcus Kawasaki syndrome Drug eruptions
COMPLICATIONS Morbidity and mortality from measles are greatest in patients
Complications by Age for Reported Measles Cases,
USA 1987–2000
NO.(%) OF PERSONS WITH COMPLICATION BY AGE GROUP
COMPLICATION OVERALL (67,032 CASES) 30 yr
(n = 28,730) (n = 6,492) (n = 18,580) 9,161) (n = 4,069)
Any 19,480 (29.1) 11,883 (41.4) 1,173 (18.1) 2,369 (12.8) 2,656 (29.0) 1,399 (34.4)
Death 177 (0.3) 97 (0.3) 9 (0.1) 18 (0.1) 26 (0.3) 27 (0.7)
Diarrhea 5,482 (8.2) 3,294 (11.5) 408 (6.3) 627 (3.4) 767 (8.4) 386 (9.5)
Encephalitis 97 (0.1) 43 (0.2) 9 (0.1) 13 (0.1) 21 (0.2) 11 (0.3)
Hospitalization 12,876 (19.2) 7,470 (26.0) 612 (9.4) 1,612 (8.7) 2,075 (22.7) 1,107 (27.2)
Otitis media 4,879 (7.3) 4,009 (14.0) 305 (4.7) 338 (1.8) 157 (1.7) 70 (1.7)
Pneumonia 3,959 (5.9) 2,480 (8.6) 183 (2.8) 363 (2.0) 554 (6.1) 379 (9.3)COMPLICATIONS
Pneumonia is the most common cause of death in measles.
- giant cell pneumonia caused directly by the viral infection
- 2ry bacterial infection:S. pneumoniae, H. influenzae, and S. aureus.
- bronchiolitis obliterans.
Croup, tracheitis, and bronchiolitis: requires intubation and ventilatory support
until the infection resolves.
Acute otitis media is the most common complication of measles
Sinusitis and mastoiditis
Viral and/or bacterial tracheitis
Suppression of PPD skin test
increased rate of activation of pulmonary tuberculoses.
Diarrhea, vomiting, dehydration: giant cell formation in the epithelium.
Appendicitis: obstruction of the lumen by lymphoid hyperplasia.COMPLICATIONS Febrile seizures occur in
COMPLICATIONS Myocarditis is a rare complication. bacteremia, cellulitis, and toxic shock syndrome. Measles during pregnancy associated with high maternal morbidity, fetal wastage and stillbirths, and congenital malformations in 3% of live born infants.
Subacute Sclerosing Parencephalitis (SSPE)
SSPE is a chronic complication of measles
delayed onset and nearly always fatal.
result from a persistent infection with an altered measles virus that is
harbored intracellularly in the CNS for several years.
After 7–10 yr regains virulence and attacks the cells in the CNS
This “slow virus infection” results in inflammation and cell death,
leading to neurodegenerative process
The incidence:1:100,000
age of onset: early age,Clinical manifestations of SSPE
SSPE begin insidiously 7–13 yr after primary measles infection.
Subtle changes in behavior or school performance appear, including irritability,
reduced attention span, or temper outbursts.
This initial phase (stage I) may at times be missed because of brevity or mildness of
the symptoms.
Fever, headache, or other signs of encephalitis are absent.
2nd stage is massive myoclonus. This coincides with extension of the inflammatory
process site to deeper structures in the brain, including the basal ganglia. Involuntary
movements and repetitive myoclonic jerks begin in single muscle groups but give way
to massive spasms and jerks involving both axial and appendicular muscles.
Consciousness is maintained.
In the 3rd stage, involuntary movements disappear and are replaced by
choreoathetosis, immobility, dystonia, and lead pipe rigidity that result from
destruction of deeper centers in the basal ganglia.
Sensorium deteriorates into dementia, stupor, then coma.
Stage IV is characterized by loss of critical centers that support breathing, heart rate,
and blood pressure.
Death soon ensues. Progression through the clinical stages may follow courses
characterized as acute, subacute, or chronic progressive.Diagnosis of SSPE (1) measles antibody detected in CSF, (2) characteristic electroencephalographic findings, or (3) typical histologic findings and/or isolation of virus or viral antigen in brain tissue obtained by biopsy or postmortem examination. CSF analysis reveals normal cells but elevated IgG and IgM antibody titers in dilutions of >1 : 8. Electroencephalographic patterns are normal in stage I, but in the myoclonic phase suppression-burst episodes are seen that are characteristic of but not pathogenomic. Brain biopsy is no longer routinely indicated for diagnosis of SSPE.
Management of SSPE primarily supportive like other neurodegenerative diseases. A recent clinical trial of the use of oral inosiplex (isoprinosine) alone to oral inosiplex and intraventricular interferon-α2b . Most die within 1–3 yr of onset from infection or loss of autonomic control mechanisms. Prevention of SSPE depends on prevention of primary measles infection through the use of vaccine.
TREATMENT OF MEASLES
Management of measles is supportive.
Antiviral therapy is not effective
Maintenance of hydration, oxygenation, and comfort are goals of
therapy.
Antipyretics for comfort and fever control are useful.
For patients with respiratory tract involvement, airway humidification
and supplemental oxygen may be of benefit.
Respiratory failure due to croup or pneumonia may require ventilatory
support.
Oral rehydration is effective in most cases, but severe dehydration may
require intravenous therapy.
Prophylactic antimicrobial therapy to prevent bacterial infection is not
indicated.
Measles infection in immunocompromised patients is highly lethal.
Ribavirin is active in vitro against measles virus.
ribavirin is not licensed in the United States for treatment of measlesVITAMIN A Vitamin A deficiency in children in developing countries has long been known to be associated with increased mortality from a variety of infectious diseases, including measles. In USA: 22–72% of children with measles had low retinol vitamin A therapy in the developing world and the United States have demonstrated reduced morbidity and mortality from measles. The American Academy of Pediatrics suggests vitamin A therapy for selected patients with measles
Recommendations for Vitamin A Treatment of Children with Measles INDICATIONS Children 6 mo to 2 yr of age hospitalized with measles and its complications (e.g., croup, pneumonia, and diarrhea). (Limited data are available about the safety and need for vitamin a supplementation for infants 6 mo of age with measles who are not already receiving vitamin A supplementation and who have any of the following risk factors: immunodeficiency clinical evidence of vitamin A deficiency impaired intestinal absorption moderate to severe malnutrition
REGIMEN The recommended dosage, administered as a capsule, is: - Single dose of 200,000 IU orally for children ≥1 yr of age (100,000 IU for children 6 mo to 1 yr of age) - The dose should be repeated the next day and again 4 wk later for children with ophthalmologic evidence of vitamin A deficiency
PROGNOSIS In the early 20th century, deaths due to measles varied between 2,000 and 10,000, or about 10 deaths per 1,000 cases of measles. With improvements in health care and antimicrobial therapy, better nutrition, and decreased crowding, the death to case ratio fell to 1 per 1,000 cases. Now in USA: 2.5–2.8/1,000. Pneumonia and encephalitis were complications in most of the fatal cases, and immunodeficiency conditions were identified in 14–16% of deaths.
PREVENTION Patients shed measles virus from 7 days after exposure to 4–6 days after the onset of rash. Exposure of susceptible individuals to measles patients should be avoided during this period. In hospitals, standard and airborne precautions should be observed for this period. Immunocompromised patients with measles will shed for the duration of the illness, and isolation should be maintained throughout
VACCINE
Measles vaccine monovalent preparation or combined with the
rubella (MR) or measles-mumps-rubella (MMR) vaccine,
2nd dose of measles vaccine was added to the schedule.
The current recommendations include a 1st dose at 12–15 mo
followed by a 2nd at 4–6 yr of age.
Seroconversion is slightly lower in children who receive the 1st
dose before or at 12 mo of age (87% at 9 mo, 95% at 12 mo,
and 98% at 15 mo) because of persisting maternal antibody.
For children who have not received 2 doses by 11–12 yr of age,
a 2nd dose should be provided.
Infants who receive a dose before 12 mo of age should be
given 2 additional doses at 12–15 mo and 4–6 yr of age.
In any event, this 2nd dose of vaccine may be given anytime 4
wk after the 1st dose.The National Immunization Schedule in Palestine
Age The Vaccine
1 d. BCG Hep.B1
1m. Hep.B2 IPV1
2m. IPV2 OPV1 DPT1 Hib
4m. OPV2 DPT2 Hib
6m. Hep.B3 OPV3 DPT3 Hib
9m.
12m. MMR
15m Hib
18m OPV4 DPT4 MMR
6y. OPV DT
12y. Rubella(
girls)
15y. dTPOSTEXPOSURE
PROPHYLAXIS
vaccine administration or immunization with
immunoglobulin.
The vaccine is effective in prevention or modification of
measles if given within 72 hr of exposure.
Immune globulin may be given up to 6 days following
exposure to prevent or modify infection.
Immunocompetent children should receive 0.25 mL/kg
intramuscularly and immunocompromised children should
receive 0.5 mL/kg.
Immune globulin is indicated for susceptible household
contacts of measles patients, especially infantsReferences Nelson textbook of pediatrics Essentials of pediatrics Atlas of pediatric clinical diagnosis Internet - Different pages.
Thank You
You can also read