DERMATOLOGY MASTERCLASS - Linda Vogelnest BVSc MANZCVS FANZCVS Specialist in Veterinary Dermatology Philippa Ravens BSc BVSc MVS MANZCVS FANZCVS ...
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below

DERMATOLOGY MASTERCLASS Linda Vogelnest BVSc MANZCVS FANZCVS Specialist in Veterinary Dermatology Philippa Ravens BSc BVSc MVS MANZCVS FANZCVS Specialist in Veterinary Dermatology

Dermatology Masterclass
• How to maximise outcomes for Dermatology Cases?
– Treatments (new knowledge)?
– Money?
– Compliance?
• Optimal outcomes dependent on
– Diagnosis: ease/difficulty of treatment
• OR most likely diagnosis within time/money constraints
– Targeted treatment plans: patient/owner orientated
– Money
– Time
– Patient demeanour
– Owner ability/willingness
www.sashvets.com
CASE ONE
JESSIE
www.sashvets.com
History
Signalment: 2yr FN German Shepherd
Presenting Complaint: pruritus
• 6 mnth duration; progressive
• Currently severe flare
• Itchy face, flanks, ventral abd, axillae, lateral/medial thighs
Previous treatment:
• Dex inj + pred (reducing course x 2wks) + cephalexin (10d): used to help
temporarily, poor recent response
• Apoquel (bid x 2wks, then sid) & cephalexin (14d) - partial initial
response, now not helping, but even worse when stop Apoquel
Routine:
• Sentinel monthly; shampoo (Malaseb) monthly
• Diet - dry/canned foods/treats
• Other pets - 1 cat (no skin problems; no flea control)
• Otherwise healthy
4
www.sashvets.com
History
Signalment: 2yr FN German Shepherd
Presenting Complaint: pruritus
• 6 mnth duration; progressive
• Currently severe flare
• Itchy face, flanks, ventral abd, axillae, lateral/medial thighs
Allergies – AD, AFR; (FBH)
Infections - SBP, MD, Sarcoptes, Demodicosis
Distribution: helpful for allergies - AD, AFR
5
www.sashvets.com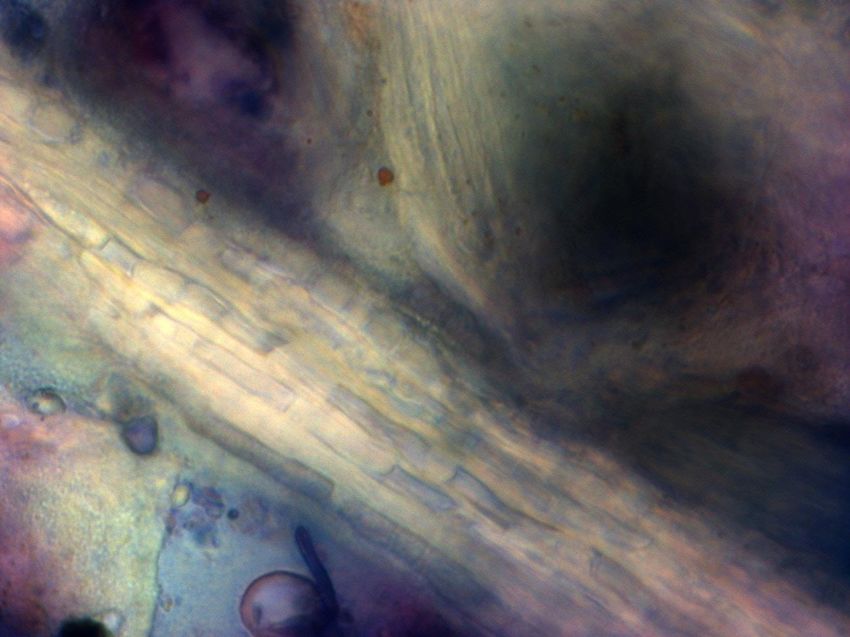
History
Previous treatment:
• Dex inj + pred (reducing course x 2wks) + cephalexin (10d): used to help
temporarily, poor recent response
• Apoquel (bid x 2wks, then sid) & cephalexin (14d) - partial initial
response, now not helping, but even worse when stop Apoquel
Infections - SBP, MD, Sarcoptes, Demodicosis
Inconclusive: could be infections or allergies
6
www.sashvets.com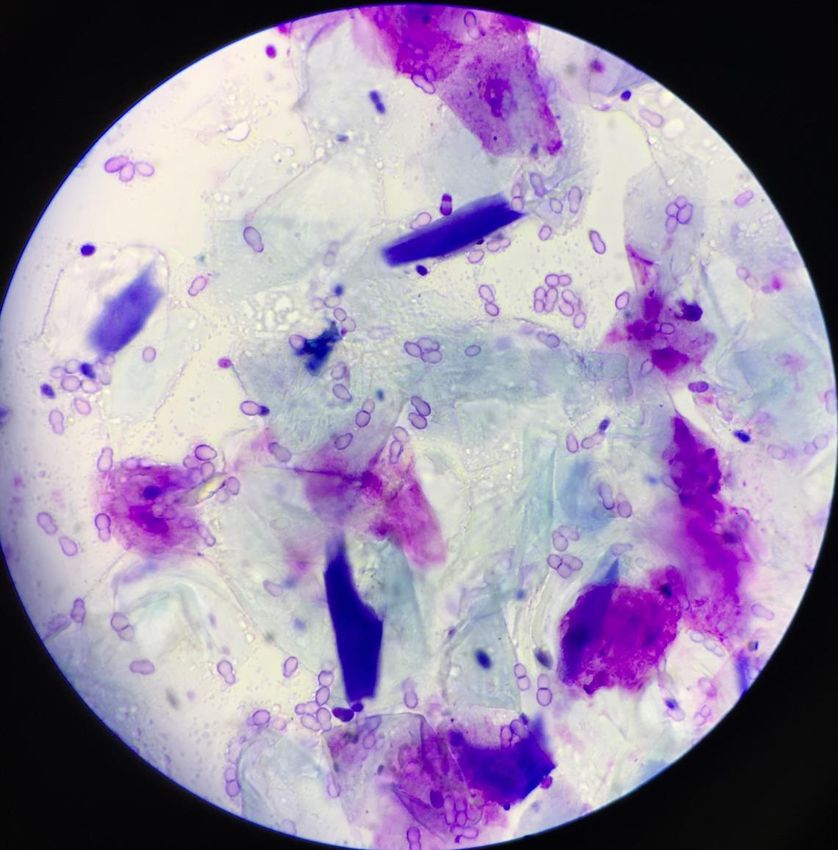
History
Routine:
Sentinel monthly; shampoo (Malaseb) monthly
Diet - dry/canned foods/treats
Other pets - 1 cat (no skin problems; no flea control)
Otherwise healthy
Allergies – FBH
7
www.sashvets.com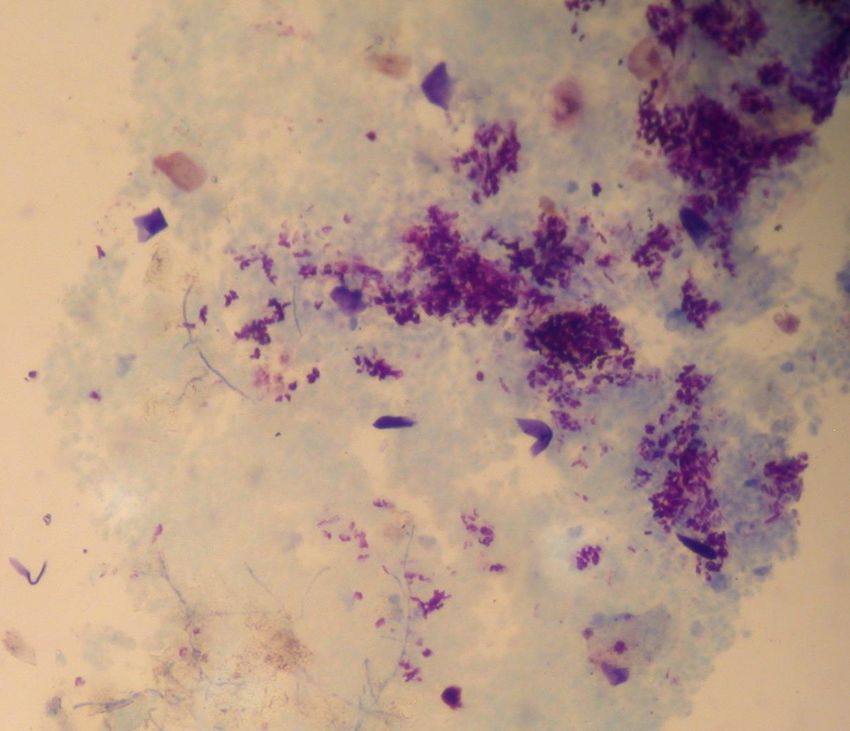
History
Prioritised Differentials
1. Atopic Dermatitis (AD) with secondary infections (SBP and/or MD)
2. Food Allergy (less common) with secondary infections (SBP and/or MD)
3. Sarcoptes (recent) + previous allergies
4. Demodicosis (recent) + allergies
5. Flea Allergy (concurrent only)
www.sashvets.com
8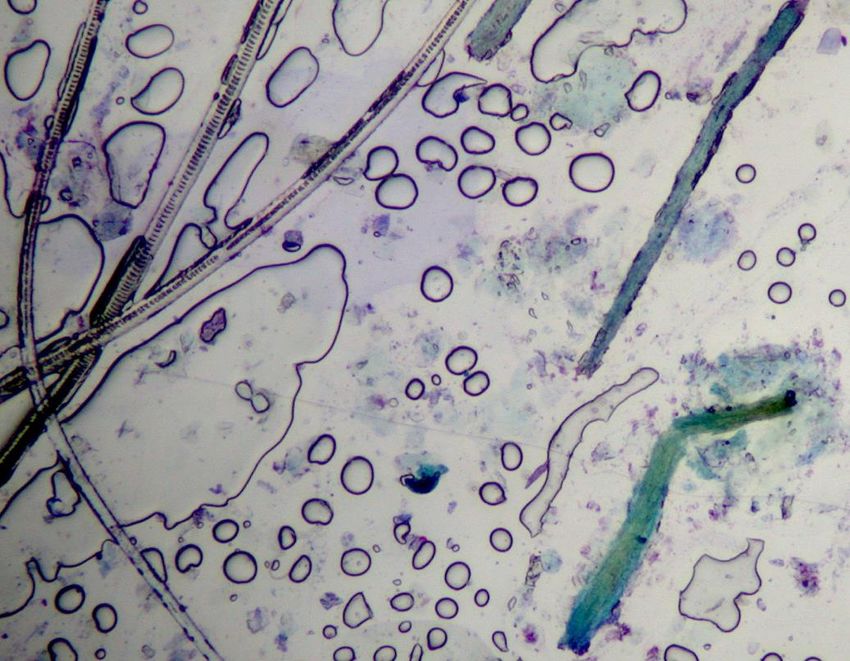
History
Lesions are
symmetrical
www.sashvets.com
9
www.sashvets.com
www.sashvets.com
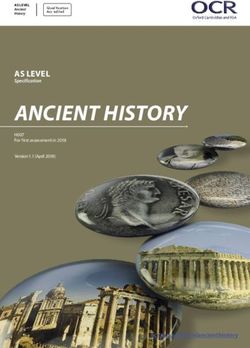
Ventrolateral flank: similar lesions fairly diffuse on
lateral and ventral trunk
www.sashvets.comClinical Exam
Lesions?
• Alopecia – patchy, poorly demarcated
• Papules
• Erosions, Erythema (face)
Distribution:
• Face, legs/feet, ventrolateral trunk
• Symmetrical
www.sashvets.comClinical Exam
Which lesions are more helpful clues?
– Primary Lesions
• Papules
• Pustules
• Wheals
• Well-demarcated alopecia
– Papules
• SBP
• Flea bites
• Mites – sarcoptes, demodicocis; Larval ticks
• Allergies (rarely)
www.sashvets.comClinical Exam
Differentials:
– Infectious
• SBP
• Sarcoptes
• Demodicosis
• MD (not for papules)
– Allergies
• AD
• AFR
• FBH (concurrent only)
www.sashvets.comHistory + Clinical Exam
Combined Differentials:
• Allergies - age of onset, pruritus
• AD – lesions/distribution, breed
• Food allergy – progressive, lesions/distribution
• FBH (concurrent) - papules, partial lesion distribution
• Infections - progressive since outset, poor steroid/Apoquel-response
• Sarcoptes - papules, severe pruritus
• SBP - papules
• MD
• Demodicosis
Is there one top differential or multiple equal?
• AD with secondary infections (SBP +/- MD)
• Especially if intermittent/waxing waning in beginning
• Must exclude sarcoptes, food allergy IF progressive from outset,
+/- other history clues
16
www.sashvets.comHistory
– What further history questions would you ask?
• Sarcoptes potential? (farmland, contagion)
• Same areas affected since onset? (no = new problem?)
• Initial pruritus? intermittently flaring (AD) or persistent (AD and/or AFR)
• Flea presence? (historically, recently)
– Do you have any comments about previous treatment choices?
• No incomplete antibiotic courses (3wks)
• No antibiotics with pred or Apoquel (incomplete resolution)
• Treatment trials should be pred or Apoquel alone OR antibiotics alone
Aim for diagnostic tx trials (long-term solution) vs treatment alone (short-term
solution) ESPECIALLY if persistent or recurrent
www.sashvets.com
17Diagnostics for Jessie
Essential
• Cytology
• Tape impressions: essential for SBP, MD
• Skin scrapings (superficial) – if sarcoptes potential
• Skin scrapings (deep): reliable to confirm or exclude demodicosis (or
squeeze tape impression)
Possibly essential (dependent on further history)
• Sarcoptes tx trial IF sarcoptes potential
• Flea treatment: IF flea history OR previous itch not on back half
Optional (dependent on further history, owner choice)
• Elimination diet - Indicated if pruritus constant, esp if GIT signs too
• Intradermal/serum allergen testing
18
www.sashvets.comJessie’s Diagnostics
More History:
• Suburban yard
• Initial waxing/waning
Cytology
• SBP
• No malassezia
19
www.sashvets.comJessie’s Diagnostics
20
www.sashvets.comMD (Not Jessie)
21
www.sashvets.comTreatment Plan for Jessie
Initial treatments?
1. Treat SBP
– Cephalexin 20-25mg/kg BID x 3wks
– Chlorhexidine 2.5-4% solution BID x 3wks
– Mediderm or Malaseb bath twice weekly if possible
2. Treat itch?
– Stop Apoquel; no pred (definitely by 48 hours)
– If itch not reducing by 48 hours, consider Cytopoint injection
– If itch not much reduced by 7d, repeat cytology (MRSP;
Cyclosporin; Refer)
3. Diagnostic Trials?
– Flea – esp. if history of fleas and/or flank/rump involvement new
– Elimination diet – optional; delay until 3wk review
22
www.sashvets.comTreatment Plan for Jessie
Follow Up?
• Schedule revisit in 3 weeks
– Stress importance of
• Diagnosis: need to review response
• Long-term treatment plan if AD
23
www.sashvets.comCASE THREE
RUFUS
www.sashvets.comHistory
Signalment: 4yr MN Sharpei
Presenting Complaint: Pruritus and alopecia
• Progressive x 12mnths
• Alopecia: left hind leg first, progressively more areas
• Pruritus: severe, constant: licking, rubbing, scratching
Previous tests:
• Skin scrapings (deep) – positive demodex (younger; no pruritus; resolved with
oral ivermectin, recurred 6mnths later: dectomax effective); multiple recent
deep scrapings – negative
Previous treatments:
• Antibiotics (multiple recent courses, no response)
Routine:
• Bravecto (once 3 months ago)
• Shampoo: (Malaseb) once wkly
• Diet: RC Anallergenic x 3mnths (no change); now sardines/rice x 2wks (wt loss)
• Other pets: none; close contact with 2 other dogs regularly (no skin problems)
• Otherwise appears healthy, but mild lethargy recently?
25
www.sashvets.comHistory
Signalment: 4yr MN Sharpei
Presenting Complaint: Pruritus and alopecia
• Progressive x 12mnths
• Alopecia: left hind leg first, progressively more areas
• Pruritus: severe, constant: licking, rubbing, scratching
Allergies – AD, AFR, FBH
Infections - SBP, Demodicosis, Sarcoptes; Dermatophytosis
Distribution: Demodicosis, Dermatophytosis
26
www.sashvets.comHistory
Previous tests:
• Skin scrapings (deep) – positive demodex as younger dog (no
pruritus); resolved with oral ivermectin, recurred 6mnths later:
dectomax effective; multiple recent deep scrapings – negative
Previous treatments:
• Antibiotics (multiple recent courses, no response)
Infections – Demodicosis; SBP (MRSP)
27
www.sashvets.comHistory
Routine:
• Bravecto (once 3 months ago)
• Shampoo: (Malaseb) once wkly
• Diet: RC Anallergenic x 3mnths (no change); now sardines/rice x 2wks (wt loss)
• Other pets: none; close contact with 2 other dogs regularly (no skin problems)
• Otherwise appears healthy, but mild lethargy recently?
Infections – (Demodicosis/Sarcoptes unlikely: check dose); (Dermatophytosis less
likely – no contagion + dz duration)
Allergies – Food allergy less likely
Inconclusive – wt loss, lethargy – diet?; other disease (e.g. pemphigus, systemic)?
28
www.sashvets.comHistory
Prioritised Differentials
1. Atopic Dermatitis (AD)
2. Food Allergy (less common; completed diet)
3. Flea Allergy (progressive?)
4. SBP due to MRSP with allergies
5. MD with allergies
6. Dermatophytosis (progressively more areas)
7. Pemphigus foliaceus
8. Demodicosis/Sarcoptes (check Bravecto dose, admin)
www.sashvets.com
29Clinical Exam
www.sashvets.com
30www.sashvets.com
www.sashvets.com
www.sashvets.com
www.sashvets.com
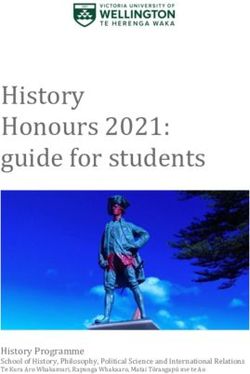
Clinical Exam
Lesions?
• Alopecia – well-demarcated
• Erythema?
• Hyperpigmentation?
Distribution?
• Face, Limbs, Trunk
• Asymmetrical
www.sashvets.comClinical Exam
Which lesions are more helpful clues?
– Well-demarcated alopecia
• Infectious
– SBP
– Demodicosis
– Dermatophytosis
• Sterile
– Pemphigus foliaceus
– Alopecia areata
www.sashvets.comClinical Exam
Differentials?
– Infectious
• Dermatophytosis
• Demodicosis
• SBP (no peripheral crusting, erythema)
– Sterile
• Alopecia areata
• Pemphigus foliaceus (no crusting)
www.sashvets.comHistory + Clinical Exam
Combined Differentials:
• Infectious – progressive, progressively more areas
• Dermatophytosis (not typically severely pruritic)
• MD (pruritus; antibiotic therapy)
• Demodicosis (breed; far less likely due to neg scrapes/Bravecto)
• SBP (no peripheral crusting, erythema)
• Allergies - age of onset, pruritus
• AD + SBP/Demodicosis - lesions/distribution, breed
• Food allergy + SBP/Demodicosis - progressive, lesions/distribution
• Auto-immune
• Pemphigus foliaceus – lesions, lethargy
Is there one top differential or multiple equal?
• Dermatophytosis
• Asymmetry, progressively more areas
• Assuming Bravecto dosed adequately
• Severe pruritus?
38
www.sashvets.comHistory
– What further history questions would you ask?
• Bravecto dose/administration
• Pruritus: sites, frequency, scratching?
• Contagion: owners
• General health: wt loss: appetite, other signs
– Do you have any comments about previous treatment choices?
• Antibiotics: multiple courses?
www.sashvets.com
39Diagnostics for Rufus
Essential
• Cytology
• Tape impressions: MD, SBP; screen for dermatophytosis
• Skin scrapings (deep) – recheck for demodicosis
(or squeeze tape impression)
Possibly essential (dependent on initial diagnostics)
• Fungal culture
• Skin biopsy: PF, exclude demodicosis, dermatophytosis
40
www.sashvets.comRufus’s Diagnostics
More History:
• Bravecto - definite
• Pruritus - mainly licking
Cytology
• No SBP, or MD
• Fungal hyphae
41
www.sashvets.com42 www.sashvets.com
43 www.sashvets.com
Treatment Plan for Rufus
Initial treatments?
1. Treat Dermatophytosis?
– Itraconazole 5mg/kg SID (pre-tx liver profile?)
– Malaseb bath twice weekly (gentle)
2. Treat itch?
– Definitely no pred or Apoquel
3. Diagnostic Trials?
– None indicated
– Balanced diet
44
www.sashvets.comTreatment Plan for Rufus
Follow Up?
• Schedule revisit in 3-4 weeks
– Stress importance of
• Review pruritus – possibly allergies?
• Completion of treatment: repeat fungal culture?
• T-lymphocyte dysfunction? (Demodicosis & Dermatophytosis)
– Avoid immunosuppression: Apoquel, GC
45
www.sashvets.comCASE FIVE
ZAC
www.sashvets.comHistory
Signalment: 3yr old Male Neutered DSH
Presenting Complaint: pruritus
• Intermittently flaring pruritus x 18 months
• Excessive body grooming, some head/neck scratching
• More severe recently and new lip lesion
Previous treatment:
• Dex injection, then tapered prednisolone course – previously helped,
but minimal response recently
• Doxycycline x 10 day course recently – no apparent response
Routine:
• Flea control – none usually
• Predominantly indoors; no other pets
• General health: no previous problems; recent reduced appetite, malaise
47
www.sashvets.comHistory
Signalment: 3yr Male Neutered DSH
Presenting Complaint: pruritus
• Intermittently flaring pruritus x 18 months
• Excessive body grooming, some head/neck scratching
• More severe recently and new lip lesion
Allergies – AD, FBH; (AFR)
Infections - SBP, MD, (D. gatoi?)
Distribution: AD, AFR, FBH
48
www.sashvets.comHistory
Previous treatment:
• Dex injection, then tapered prednisolone course – previously
helped, but minimal response recently
• Doxycycline x 10 day course recently – no apparent response
Allergies – AD, FBH, AFR
Infections - SBP, MD, (D. gatoi?), Dermatophytosis
Inconclusive: SBP still possible (doxy – not reliable?)
49
www.sashvets.comHistory
Routine:
• Flea control – none usually
• Predominantly indoors; no other pets
• General health: no previous problems; recent reduced appetite,
malaise
Allergies – FBH
Inconclusive: consistent with lip lesions/allergies, and multiple causes
50
www.sashvets.comHistory
Prioritised Differentials
1. Atopic Dermatitis (AD) with secondary infections (SBP and/or MD)
2. Flea Allergy with secondary infections (SBP and/or MD)
3. D. gatoi (recent) + previous allergies
4. Dermatophytosis (recent) + previous allergies
5. New problem (lip lesion, malaise) + previous allergies
www.sashvets.com
51Clinical Exam
www.sashvets.comClinical Exam
www.sashvets.comClinical Exam
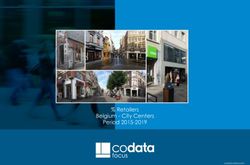
www.sashvets.comClinical Exam
Lesions?
– Erosions/ulceration
– Nodule (eroded)
– Coat discolouration (brown fading)
Distribution:
– Hard palate (ulceration)
– Lip (eroded nodule)
– Ventral neck
www.sashvets.comClinical Exam
Which lesions are more helpful clues?
• Lip (eroded nodule)
– Eosinophilic granuloma/rodent ulcer
– Cryptococcus
– Neoplasia?
• Lip + palatine ulcer
– Allergies: AD, AFR, FBH
www.sashvets.comClinical Exam
Differentials?
– Allergies
• AD, AFR, FBH
– Infectious
• SBP
• Herpes/calicivirus
www.sashvets.comHistory + Clinical Exam
Combined Differentials:
• Allergies - age of onset, pruritus, previous steroid response
• AD, FBH – lesions/distribution, intermittently flaring
• Food allergy – lesions/distribution (concurrent only)
• Infections – minimal recent steroid response
• SBP
• Demodicosis (D. gatoi)
• Herpes/calicivirus
Is there one top differential or multiple equal?
• AD OR FBH
• +/- SBP
58
www.sashvets.comHistory
– What further history questions would you ask?
• Previous flea outbreaks?
• Many pets in neighbourhood?
• Seasonality of flares? - summer/aut (FBH)(; spring/summer/aut (AD)
• History of GIT signs? – AFR; History of herpes/calicivirus
• Other recent details on health: appetite, urine/faeces etc
– Do you have any comments about previous treatment choices?
• Doxycycline x 10 day course:
– Cephalexin or amoxyclav more reliable for SBP
» Convenia (less appropriate 1st line)
– Doxy resistance higher
» Paste easier? (insufficient justification for less effective choice)
www.sashvets.com
59Diagnostics for Zac
Essential
• Cytology
• Tape impressions (neck, lip): essential for SBP
• Swab from palatine ulcer: bacterial infection; viral PCR?
• Flea Treatment Trial
• Quick-kill adulticide: Comfortis, Advantage; Environ IGR
Possibly essential
• Skin scrapings (superficial) – D. gatoi (Still v. rare Australia)
Optional (dependent partly on further history, owner choice)
• Heam/Biochem/Urinalysis (optimal)
• Intradermal/serum allergen testing
• Elimination diet trial (possibly concurrent; esp if GIT signs)
• Delay until oral lesions improved
60
www.sashvets.comZac’s Diagnostics
More History:
• Many pets in area
• No fleas seen
• Seasonal spring flares
• No previous GIT signs
Cytology
• SBP
• Oral: bacterial rods
61
www.sashvets.comZac’s Diagnostics
62
www.sashvets.comTreatment Plan for Zac
Initial treatments?
1. Treat SBP
– Amoxy-clav - 20-25mg/kg BID x 3wks (clindamicin: 2nd line)
– Topical fusidic acid (Conoptal, Fucidin)?
2. Treat itch?
– Oral pred (ideally not for first 1-2wks)
– No Depomedrol (no ability to adjust dose; severe infections)
– Cyclosporin (liquid, capsules)
– Apoquel (safety unknown)
3. Diagnostic Trials?
– Flea trial - Advantage (Capstar, Comfortis) +/- environ IGR
– Elimination diet – optional; delay until more controlled
63
www.sashvets.comTreatment Plan for Zac
Follow Up?
• Schedule revisit in 1 week (assuming no prior deterioration)
– Stress importance of
• Monitoring oral lesion closely: severe bleeding potential
– Aggressive treatment important
• Sustained treatment for resolution of lip lesion
• Diagnosis
– FBH - easily controlled
– AD - life-long management
64
www.sashvets.comYou can also read