Family History in Primary Care Pediatrics - American Academy ...
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
SUPPLEMENT ARTICLE
Family History in Primary Care Pediatrics
AUTHORS: Beth A. Tarini, MD, MS, FAAPa and Joseph D.
McInerney, MA, MSb abstract
aChild Health Evaluation and Research Unit, Department of The family history has been called the first genetic test; it was a core
Pediatrics, University of Michigan, Ann Arbor, Michigan; and
bAmerican Society of Human Genetics, Bethesda, Maryland element of primary care long before the current wave of genetics tech-
nologies and services became clinically relevant. Risk assessment
KEY WORDS
family history, primary care, pediatrics based on family history allows providers to personalize and prioritize
ABBREVIATIONS health messages, shifts the focus of health care from treatment to pre-
AHRQ—Agency for Healthcare Research and Quality vention, and can empower individuals and families to be stewards of
PCP—primary care provider their own health. In a world of rising health care costs, the family his-
www.pediatrics.org/cgi/doi/10.1542/peds.2013-1032D tory is an important tool, with its primary cost being the clinician’s
doi:10.1542/peds.2013-1032D time. However, a recent National Institutes of Health conference high-
Accepted for publication Aug 28, 2013 lighted the lack of substantive evidence to support the clinical utility
Address correspondence to Beth A. Tarini, MD, MS, FAAP, Child of family histories. Annual collection of a comprehensive 3-generation
Health Evaluation and Research Unit, University of Michigan, 300 family history has been held up as the gold standard for practice.
North Ingalls St, Room 6D19, Ann Arbor, MI 48109-5456. E-mail:
However, interval family histories targeted to symptoms and family
btarini@umich.edu
histories tailored to a child’s life stage (ie, age-based health) may be
PEDIATRICS (ISSN Numbers: Print, 0031-4005; Online, 1098-4275).
important and underappreciated methods of collecting family history
Copyright © 2013 by the American Academy of Pediatrics
that yield clinically actionable data and supplement existing family
FINANCIAL DISCLOSURE: The authors have indicated they have
history information. In this article, we review the various applications,
no financial relationships relevant to this article to disclose.
as well as capabilities and limitations, of the family history for pri-
FUNDING: This effort was supported by grant UC7MC21713 from
the Health Resources and Services Administration’s Maternal mary care providers. Pediatrics 2013;132:S203–S210
and Child Health Bureau. The Genetics in Primary Care Institute
is a cooperative agreement between the American Academy of
Pediatrics and the Maternal and Child Health Bureau. Dr Tarini is
funded, in part, by a K23 Mentored Patient-Oriented Career
Development Award from the Eunice Kennedy Shriver National
Institute of Child Health and Human Development
(K23HD057994). Funded by the National Institutes of Health (NIH).
POTENTIAL CONFLICT OF INTEREST: The authors have indicated
they have no potential conflicts of interest to disclose.
PEDIATRICS Volume 132, Supplement 3, December 2013 S203
Downloaded from www.aappublications.org/news by guest on February 26, 2021Often used by genetic specialists as or for a single condition. The review samples sent to laboratories for spe-
a case-finding tool for rare Mendelian found few data to guide recommenda- cialized testing, a family history re-
(single-gene) disorders, a family his- tions on the key elements of an effec- quires only a conversation between the
tory can also be a powerful screening tive family history in primary care clinician and the patient. The family
and diagnostic tool for primary care practice. history has broad clinical utility. Family
providers (PCPs). A family history can Although annual collection of the 3- history is a major risk factor for com-
be used for assessing risk for specific generation family history has been mon chronic diseases, such as car-
conditions; for preventing, detecting, touted as the gold standard, interval diovascular disease, diabetes, several
and managing disease; for informing family histories targeted to symptoms cancers, osteoporosis, asthma, and
a diagnostic evaluation1; for providing and family histories tailored to a child’s psychiatric disorders.1,5,6 It can also
preconception counseling2; and for life stage (ie, age-based health) may reveal the influence of environmental
fostering rapport with patients. The be important and underappreciated (social and natural) and cultural fac-
development of online family history methods of collecting family history tors on an individual’s health. For
tools and the increasing use of elec- that yield clinically actionable data and example, data from the Adverse Child-
tronic health records offer opportuni- hood Experiences study, 1 of the largest
supplement existing family history in-
ties for improving the ability of pediatric studies ever to examine the influence
formation. Ultimately, the goal is to
PCPs to record, standardize, and accu- of childhood environment on adult
have an accurate and comprehensive
rately assess family history information. health, has identified a number of links
assessment of each patient’s family
The challenge is to determine which between a child’s environment and
history. Achievement of this goal will
type of family history information and disease in adulthood.7 SCREEN is an
require multiple and different discus-
method of collection is most useful and easy-to-remember mnemonic that high-
sions (eg, targeted and tailored) about
effective in the pediatric primary care lights important content included in
family history in various clinical con-
setting. Although collection and in- a family history (Table 1).
texts (eg, health maintenance visits,
terpretation of family histories are acute care visits) both to help jog pa- A traditional family history contains
considered standard of care and are tients’ memories about information a wide range of health information on at
endorsed by many professional health they forgot to share, confirm the in- least 3 generations of maternal and
care societies outside the field of ge- formation already collected, and iden- paternal family members: first-degree
netics, evidence that family histories tify newly diagnosed health conditions relatives (children, siblings, and par-
improve health outcomes is lacking. A among family members. ents), second-degree relatives (aunts,
systematic review prepared by the uncles, and grandparents), and third-
Agency for Healthcare Research and degree relatives (first cousins) (Table 2).
WHAT IS A FAMILY HISTORY?
Quality (AHRQ) for the 2009 National A family history is commonly organized
Institutes of Health State-of-the-Science A family history is a collection of infor- and displayed in the form of a pedigree
Conference on family history revealed mation about the health history of an because it facilitates identification of
a paucity of data to support the clinical individual’s biological relatives. Funda- inheritance patterns. Standard pedi-
utility of the family history.3 The review mentally, collecting a family history is gree nomenclature has been in use
attempted to identify which elements an inexpensive, noninvasive screening since 19958,9 and is probably most
of a family history (eg, age, degree of procedure.4 Although “screening pro- helpful when looking for classic Mende-
relationship, number of affected rela- cedure” may conjure images of blood lian patterns of inheritance.1 Although
tives, ancestry) are most useful in
primary care for common medical con- TABLE 1 The SCREEN Mnemonic for Family History Collection
ditions (asthma and allergies [atopic SC Some Concerns “Do you have any (some) concerns about diseases or conditions
disease], diabetes, major depression that run in the family?”
and other mood disorders, stroke, and R Reproduction “Have there been any problems with pregnancy, infertility, or
birth defects in your family?”
cardiovascular disease) and 5 common E Early disease, death, or “Have any members of your family died or become sick at an
cancers (breast, ovarian, colorectal, disability early age?”
prostate, and lung). The majority of E Ethnicity “How would you describe your ethnicity?” or “Where were your
parents born?”
published studies analyzed in the re- N Nongenetic “Are there any other risk factors or nonmedical conditions that
view focused on collection of family run in your family?”
histories in first-degree relatives only Content taken from Trotter TL, Martin HM. Family history in pediatric primary care. Pediatrics. 2007;120(suppl 2):S62.
S204 TARINI and MCINERNEY
Downloaded from www.aappublications.org/news by guest on February 26, 2021SUPPLEMENT ARTICLE
TABLE 2 Important Components of a Family primary care visits. Therefore, we sug- formation from such targeted histories
History (For Each Relative)*
gest that PCPs consider a multimodal can then be incorporated into the com-
Relationship of relative (e.g., full or half siblings, approach to collecting family histories prehensive record of the patient’s
adopted)
Sex of relative over a child’s lifetime that includes family history. Targeted family histo-
Age or year of birth histories targeted to a child’s symp- ries are not new to the pediatric PCP.
Ancestral background/ethnicity toms during an acute visit (targeted They are an integral part of current
Consanguinity (blood relationship between
parents) family histories) as well as histories clinical screening guidelines. For ex-
Medical conditions and age at diagnosis tailored to the child’s life stage (tai- ample, preparticipation physicals for
Pregnancies and any complications (e.g., infertility, lored family histories) (Table 3). If the competitive athletes should include tar-
miscarriages, stillbirths, ectopic pregnancies,
pregnancy terminations, preterm birth, PCP finds a red flag in these family geted questions about sudden death
preeclampsia) histories (Table 4), then he or she can among relatives,11 and a family history
* Courtesy of National Coalition for Health Professional take a more extensive history and of dyslipidemia and early atheroscle-
Education in Genetics. rotic heart disease is considered an
consider additional evaluation or re-
ferral to a specialist. indication for lipid screening in chil-
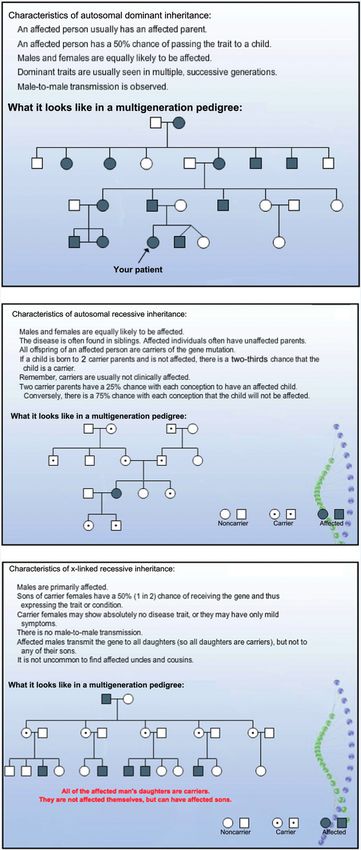
PCPs are unlikely to construct a pedi- Alternatively, a targeted family history dren.12
gree as part of their standard practice, may provide considerable value when In addition, a tailored family history that
a passing familiarity with pedigree a patient presents with symptoms that focuses on health conditions relevant to
nomenclature and patterns will help suggest an underlying genetic condi- the child’s life stage may maximize
them communicate patient information tion in the family. For example, a preteen clinical utility and offer an achievable
to genetics specialists (Figs 1 and 2). who presents to a pediatric PCP with goal within the time constraints of
Although PCPs have been encouraged to recurrent syncope with exertion should a health maintenance visit. A broadly
collect a comprehensive 3-generation raise concern about the possibility of an focused family history may seem ir-
family history or construct a pedigree inherited cardiac condition, such as an relevant to the child’s life stage. For
for each patient,10 there is little evi- arrhythmia or hypertrophic cardiomy- example, familial disease patterns that
dence to support the clinical utility of opathy, and should prompt the clinician are clinically relevant for a newborn
this practice and little time to collect the to take a multigenerational family his- are likely to differ from those for an
necessary information during short tory targeted to these conditions. In- adolescent. PCPs take such differences
into account when tailoring dis-
cussions about safety to the child’s age
(eg, sudden infant death syndrome
versus bike helmet use).13 As the child
grows, the family history is built stage
by stage. Given their long-term re-
lationship with families, pediatric PCPs
are in an ideal position to construct
such progressive family histories.
CHALLENGES TO COLLECTING
FAMILY HISTORIES
Although the decision about when to
collect a comprehensive 3-generation
family history is left to the physician’s
discretion, annual health maintenance
visits tend to be a popular time to col-
lect (or update) such information from
both new and established patients.14 As
noted earlier, a family history is not
a static document collected 1 time. Al-
FIGURE 1 though a family history does contain
Pedigree symbols. Courtesy of the National Coalition for Health Professional Education in Genetics. information about past events, family
PEDIATRICS Volume 132, Supplement 3, December 2013 S205
Downloaded from www.aappublications.org/news by guest on February 26, 2021members’ health issues are dynamic
and evolving. Newly discovered in-
formation about family members, liv-
ing or deceased, and new information
about the clinical significance of pre-
viously identified genetic variants in
the family may require the clinician to
refine the family history. Moreover, as
with most clinical histories that rely on
patient recall, repeated questioning on
different occasions may help patients
to remember forgotten, but important,
information.
Admittedly, there is room for improve-
ment in the collection and documen-
tation of family histories by PCPs. By
self-report, the vast majority of PCPs
(eg, 95% in 1 study) say that they take
a family history as part of routine
care.15 However, direct-observation
studies suggest otherwise. In 1 such
study of family physicians, family his-
tory was discussed during only 24% of
visits on average, and there was sig-
nificant variation between providers,
ranging from 0% to 81% of a given pro-
vider’s visits.14 Frezzo et al16 reported
that 20% of patients in an internal
medicine clinic were at increased risk
for disorders with known genetic con-
tribution, but this risk was not noted in
their medical charts.
A common complaint from PCPs is that
they do not have enough time to collect
a family history during the brief time
allowed for patient visits. In a direct-
observation study of family physi-
cians, the average time spent collecting
a family history was 3 minutes for
established patients and slightly .5
minutes for new patients.14 In addition,
exactly what constitutes a family his-
tory is frequently interpreted through
the eye of the beholder, and this study
did not assess the scope and content of
the information collected. For some
clinicians, “family history” may mean
a comprehensive 3-generation family
FIGURE 2
Examples of inheritance patterns displayed in pedigrees. Courtesy of the National Coalition for Health history, whereas for others, taking
Professional Education in Genetics. a family history may mean asking the
S206 TARINI and MCINERNEY
Downloaded from www.aappublications.org/news by guest on February 26, 2021SUPPLEMENT ARTICLE
TABLE 3 Types of Family History systematic review were collected from
Family History Health Conditions No. of Generations patients in specialty practices, not pri-
Targeted Specific disorders relevant to presenting Multigenerational, not necessarily 3 mary care clinics, the review revealed
symptoms generations that patients reported the absence of
Tailored Range of disorders relevant to child’s Multigenerational, not necessarily 3
age-based health generations
disease more accurately than the
Comprehensive Range of disorders, including 3 generations presence of disease.3 Not surprisingly,
disorders not immediately relevant the closer the degree of relation, the
to child’s age-based health
more accurate the report.
Using the family history to quantify risks
single question “What diseases run in bring some consistency to the collec- for common complex disorders pres-
your family?” These differences in prac- tion, documentation, and interpreta- ents another challenge. The AHRQ review
tice make assessing the clinical utility tion of that information (Appendix). revealed that even when risks for such
of the family history challenging. Unfortunately, few of these tools, in- disorders are known, the sensitivities
Web-based family history tools and the cluding those developed for use in the and positive predictive values are low for
emergence of electronic health records primary care setting, have been vali- most common conditions (,25% and
offer a potential panacea for stan- dated.17 Frezzo et al16 have developed 1 ,10%, respectively). Atopic diseases, as
dardizing collection of family histories of the few family history tools for pri- well as major depression and other
and maximizing their clinical utility. mary care adult medicine that has mood disorders, were notable excep-
Another advantage of electronic health been validated against a gold standard tions, with sensitivities ∼50% and posi-
(eg, an interview by a genetic coun- tive predictive values of 25% to 50%.
records is that some patient-oriented
selor). No validated pediatric family However, the review acknowledged that
tools (eg, online patient portals or
history tools exist. because the data were based on re-
electronic tablets in providers’ offices)
search conducted outside the primary
decrease the collection time during the
care setting, sample bias limits the ap-
actual clinic visit, thus allowing family TRANSLATING THE FAMILY
plicability of the results to primary
histories to be taken in relatively short HISTORY INTO IMPROVED HEALTH
OUTCOMES care.3
primary care visits. Several organ-
Even when the risk of disease can be
izations have aggregated freely avail- For family histories to improve health
determined from a family history, PCPs
able Web- and paper-based tools for outcomes, the information collected
face the challenge of accurately com-
the collection and assessment of family must be accurate, the risk to the patient
municating that risk in a way that
history information in an attempt to identified and effectively communi- patients can understand. Risk com-
cated, and appropriate action taken by munication research has shown that
provider and patient. Each of these formats for communicating risk vary
TABLE 4 Red Flags in a Family History*
steps presents significant challenges. according to the clinical context and
Multiple relatives affected with the same disorder
or related disorders Physicians frequently raise concerns needs of the patient.18 Moreover,
Earlier-than-expected age at onset of disease about the reliability and accuracy of the patients’ family history–based percep-
Intellectual disability (formerly referred to as
family history information that patients tions of their own risk vary with per-
developmental delay or mental retardation)
Diagnosis of a disease in the less-often-affected sex provide. As with any other kind of sonal experiences and might conflict
(e.g., breast cancer in a male) medical history collected from a pa- with the risk estimates of the health
Multifocal or bilateral occurrence in paired organs
tient, a family history will only be as care providers.19 To motivate patients
At least one major malformation, with or without
minor manifestations good as the reporter who provides it. to change their behavior on the basis of
Disease in the absence of risk factors or after Patients are human and therefore may a family history, we require a better
preventive measures understanding of their perceptions of
Abnormalities in growth (growth retardation,
misinterpret, fail to disclose, or simply
asymmetric or excessive growth) be unaware of information. Neverthe- their personal risks of disease, which
Recurrent pregnancy losses less, the utility of the family history may differ depending on the disease
Consanguinity (blood relationship between and individual experiences.20
parents)
should not be dismissed outright.
*Adapted from Core Principles in Family History: Interpre-
Providers should instead be mindful of Data on how family histories affect
tation. National Coalition for Health Professional Education these shortcomings and their potential health outcomes are sparse and show
in Genetics. http://www.nchpeg.org/index.php?option5com_
content&view5article&id5199&Itemid5126. Accessed Febru-
to bias the family history. Although only modest effects on behavior. Studies
ary 22, 2013. much of the data analyzed in the AHRQ have found that knowledge of a family
PEDIATRICS Volume 132, Supplement 3, December 2013 S207
Downloaded from www.aappublications.org/news by guest on February 26, 2021history of breast cancer leads to in- tensions between the right to privacy state laws.25 To assist physicians, pro-
creased adherence to routines for and the duty to inform. For example, fessional organizations such as the
breast self-examination but not to in- some PCPs treat multiple members of American Medical Association have rec-
creased use of mammography.3 A ran- the same family, and genetic infor- ommended that, before initiating test-
domized trial involving .40 primary mation about 1 family member may be ing, physicians explicitly inform patients
care practices showed that partic- highly relevant to the care of his or her of the situations in which they would feel
ipants who used a Web-based tool to relatives. Is it ethical to use information compelled to breach confidentiality.26
assess their familial risk for various learned in treating 1 family member in
diseases found small increases in the care of another without the consent CONCLUSIONS
preventive behaviors such as physical of the first family member? In pediat-
Even when it becomes technically and
activity and healthy eating habits but rics, a child’s genetic information may
financially feasible to generate a com-
decreases in cholesterol monitoring.21 have implications for the parents, for
plete genetic sequence for each patient,
An intervention study to increase folic example, by indicating their carrier
targeted and tailored family histories
acid intake in Irish families with a his- status or revealing misattribution of
will still provide important context
tory of neural tube defects increased the child’s paternity. In these situations, about diseases that may run in the
participants’ knowledge about the the physician must clearly understand family, enabling providers to implement
benefits of folic acid but did not in- the potential consequences of the ge- appropriate screening procedures,
crease their use of folic acid.22 netic information for other family interventions, and management plans.
members, especially if collection of a Although pediatric PCPs are in a posi-
NAVIGATING ETHICAL DILEMMAS family history leads to genetic testing. tion to use family histories to improve
OF THE FAMILY HISTORY Unfortunately, it is not clear how physi- health outcomes for their patients,
In considering the technical- and cians should proceed when collection of several technical, evidential, and ethical
evidence-based challenges to using the a patient’s family history reveals family barriers exist. Failure to address these
family history in primary care, we must members to be at increased risk of barriers will leave pediatric PCPs
not overlook ethical issues, such as disease. Although physicians have without guidance on which data ele-
privacy, confidentiality, and potential been sued for failure to notify an at-risk ments are most effective, on how best to
discrimination, that might arise from relative, mandatory institution of a duty- collect those elements efficiently, and
its use.23,24 Potential ethical challenges to-inform requirement for physicians on how to use the family history to
to improving health outcomes by conflicts with the Health Insurance Por- improve health care behavior and out-
means of the family history include tability and Accountability Act and some comes.
REFERENCES
1. Guttmacher AE, Collins FS, Carmona RH. history be used as a tool for public health ture: update and assessment of the rec-
The family history—more important than and preventive medicine? Genet Med. 2002; ommendations of the National Society of
ever. N Engl J Med. 2004;351(22):2333–2336 4(4):304–310 Genetic Counselors. J Genet Couns. 2008;17
2. Nagle C, Lewis S, Meiser B, Gunn J, Halliday 6. Plomin R, McClearn GE, McGuffin P, DeFries (5):424–433
J, Bell R. Exploring general practitioners’ JC. Behavioral Genetics. 5th ed. New York, 10. Brock JA, Allen VM, Keiser K, Langlois S.
experience of informing women about NY: Worth Publishers; 2008 Family history screening: use of the three
prenatal screening tests for foetal abnor- 7. Centers for Disease Control and Pre- generation pedigree in clinical practice. J
malities: a qualitative focus group study. vention. Adverse Childhood Experiences Obstet Gynaecol Can. 2010;32(7):663–672
BMC Health Serv Res. 2008;8:114 (ACE) study: major findings. Available at: 11. Maron BJ, Thompson PD, Ackerman MJ,
3. Qureshi N, Wilson B, Santaguida P, et al. www.cdc.gov/nccdphp/ace/findings.htm. et al; American Heart Association Council
on Nutrition, Physical Activity, and Metabo-
Family History and Improving Health. Accessed March 15, 2013
lism. Recommendations and considerations
Rockville, MD: Agency for Healthcare Re- 8. Bennett RL, Steinhaus KA, Uhrich SB, et al;
related to preparticipation screening for
search and Quality; 2009. Evidence Reports/ Pedigree Standardization Task Force of the cardiovascular abnormalities in competitive
Technology Assessment 186 National Society of Genetic Counselors. athletes: 2007 update: a scientific statement
4. Pyeritz RE. The family history: the first ge- Recommendations for standardized human from the American Heart Association Council
netic test, and still useful after all those pedigree nomenclature. Am J Hum Genet. on Nutrition, Physical Activity, and Metabo-
years? Genet Med. 2012;14(1):3–9 1995;56(3):745–752 lism: endorsed by the American College of
5. Yoon PW, Scheuner MT, Peterson-Oehlke KL, 9. Bennett RL, French KS, Resta RG, Doyle DL. Cardiology Foundation. Circulation. 2007;115
Gwinn M, Faucett A, Khoury MJ. Can family Standardized human pedigree nomencla- (12):1643–455
S208 TARINI and MCINERNEY
Downloaded from www.aappublications.org/news by guest on February 26, 2021SUPPLEMENT ARTICLE
12. Expert Panel on Integrated Guidelines for a risk assessment tool in internal medi- Effect of preventive messages tailored to
Cardiovascular Health and Risk Reduction in cine. Genet Med. 2003;5(2):84–91 family history on health behaviors: the
Children and Adolescents; National Heart, 17. Reid GT, Walter FM, Brisbane JM, Emery JD. Family Healthware Impact Trial. Ann Fam
Lung, and Blood Institute. Expert panel on Family history questionnaires designed for Med. 2011;9(1):3–11
integrated guidelines for cardiovascular clinical use: a systematic review. Public 22. Byrne J. Folic acid knowledge and use
health and risk reduction in children and Health Genomics. 2009;12(2):73–83 among relatives in Irish families with
adolescents: summary report. Pediatrics.
18. Zikmund-Fisher BJ. The right tool is what neural tube defects: an intervention study.
2011;128(suppl 5):S213–S256
they need, not what we have: a taxonomy of Ir J Med Sci. 2003;172(3):118–122
13. Hagan J, Shaw J, Duncan P. Bright Futures:
appropriate levels of precision in patient 23. Bennett RL. The family medical history.
Guidelines for Health Supervision of Infants,
risk communication. Med Care Res Rev. Prim Care. 2004;31(3):479–495, vii–viii
Children, and Adolescents. 3rd ed. Elk Grove,
2013;70(suppl 1):37S–49S 24. Rich EC, Burke W, Heaton CJ, et al. Recon-
IL: American Academy of Pediatrics; 2008
19. Walter FM, Emery J, Braithwaite D, Marteau sidering the family history in primary care.
14. Acheson LS, Wiesner GL, Zyzanski SJ,
Goodwin MA, Stange KC. Family history- TM. Lay understanding of familial risk of J Gen Intern Med. 2004;19(3):273–280
taking in community family practice: common chronic diseases: a systematic 25. Offit K, Groeger E, Turner S, Wadsworth EA,
implications for genetic screening. Genet review and synthesis of qualitative re- Weiser MA. The “duty to warn” a patient’s
Med. 2000;2(3):180–185 search. Ann Fam Med. 2004;2(6):583–594 family members about hereditary disease
15. Hayflick SJ, Eiff MP, Carpenter L, Steinberger 20. Walter FM, Emery J. ‘Coming down the risks. JAMA. 2004;292(12):1469–1473
J. Primary care physicians’ utilization and line’— patients’ understanding of their 26. Taub S, Morin K, Spillman MA, Sade RM,
perceptions of genetics services. Genet Med. family history of common chronic disease. Riddick FA; Council on Ethical and Judicial
1998;1(1):13–21 Ann Fam Med. 2005;3(5):405–414 Affairs of the American Medical Associa-
16. Frezzo TM, Rubinstein WS, Dunham D, 21. Ruffin MT IV, Nease DE Jr, Sen A, et al; tion. Managing familial risk in genetic
Ormond KE. The genetic family history as Family History Impact Trial (FHITr) Group. testing. Genet Test. 2004;8(3):356–359
PEDIATRICS Volume 132, Supplement 3, December 2013 S209
Downloaded from www.aappublications.org/news by guest on February 26, 2021APPENDIX Online Family Health History Tools
Family History Tool (Organization) Web Site
My Family Health Portrait (US Surgeon General’s https://familyhistory.hhs.gov
Family History Initiative)
Family Health History (Centers for Disease Control www.cdc.gov/genomics/famhistory/
and Prevention)
Family Medical History (American Medical www.ama-assn.org/ama/pub/category/2380.html
Association)
Draw Your Family Tree (National Society of Genetic http://www.nsgc.org/About/FamilyHistoryTool/
Counselors) DrawYourFamilyTree/tabid/227/Default.asp
Family Healthware (Centers for Disease Control http://www.cdc.gov/genomics/famhistory/famhx.htm
and Prevention)
Family History for Prenatal Providers (National http://www.nchpeg.org/index.php?
Coalition for Health Professional Education option=com_content&view=article&id=53
in Genetics)
S210 TARINI and MCINERNEY
Downloaded from www.aappublications.org/news by guest on February 26, 2021Family History in Primary Care Pediatrics
Beth A. Tarini and Joseph D. McInerney
Pediatrics 2013;132;S203
DOI: 10.1542/peds.2013-1032D
Updated Information & including high resolution figures, can be found at:
Services http://pediatrics.aappublications.org/content/132/Supplement_3/S203
References This article cites 22 articles, 5 of which you can access for free at:
http://pediatrics.aappublications.org/content/132/Supplement_3/S203
#BIBL
Permissions & Licensing Information about reproducing this article in parts (figures, tables) or
in its entirety can be found online at:
http://www.aappublications.org/site/misc/Permissions.xhtml
Reprints Information about ordering reprints can be found online:
http://www.aappublications.org/site/misc/reprints.xhtml
Downloaded from www.aappublications.org/news by guest on February 26, 2021Family History in Primary Care Pediatrics
Beth A. Tarini and Joseph D. McInerney
Pediatrics 2013;132;S203
DOI: 10.1542/peds.2013-1032D
The online version of this article, along with updated information and services, is
located on the World Wide Web at:
http://pediatrics.aappublications.org/content/132/Supplement_3/S203
Pediatrics is the official journal of the American Academy of Pediatrics. A monthly publication, it
has been published continuously since 1948. Pediatrics is owned, published, and trademarked by
the American Academy of Pediatrics, 345 Park Avenue, Itasca, Illinois, 60143. Copyright © 2013
by the American Academy of Pediatrics. All rights reserved. Print ISSN: 1073-0397.
Downloaded from www.aappublications.org/news by guest on February 26, 2021You can also read