Residential Aged Care Covid-19 Pandemic Plan - Barwon ...
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
Residential Aged Care Covid-19 Pandemic Plan Purpose Early recognition of COVID-19 symptoms will enable implementation of infection prevention measures, reduce both transmission to others and the risk of epidemic-prone infection outbreaks. This document provides strategies to effectively confine and contain cases of COVID-19 in the Barwon Health residential aged care population and aims to minimise and prevent further episodes. Target Audience Residential aged care staff Definitions Abbreviations: ARI: Acute Respiratory Infection ARRL: Australian Rickettsial Reference Laboratory DoH: Department of Health DoHHS: Department of Health and Human Services IPS: Infection Prevention Service RACF: Residential Aged Care Facility PCR: Polymerase chain reaction PPE: Personal Protective Equipment COVID-19: An acute respiratory infection caused by SARS-CoV-2. COVID-19 is suspected if the person has a fever (temperature ≥37.5C) OR acute respiratory infection (e.g. cough, sore throat, shortness of breath, runny nose or anosmia). NOTE: Fever may be absent in elderly residents. Older people may also have increased confusion, hypothermia, a worsening of a chronic lung condition and/or loss of appetite. Other symptoms consistent with COVID-19 include headache, myalgia, stuffy nose, nausea, vomiting and diarrhoea. Barwon Health residential aged care population: Residents, staff, visitors and volunteers. Confirmed case: A person who tests positive to a validated SARS-CoV-2 nucleic acid test or has the virus identified by electron microscopy or viral culture. Suspected case: Person who fits the criteria for COVID-19 awaiting COVID-19 test results. Close contact: greater than 15 minutes face-to-face, cumulative over the course of a week, or the sharing of a closed space for more than two hours, with a confirmed case during their infectious period without recommended personal protective equipment (PPE). Recommended PPE includes droplet and contact precautions. Contact needs to have occurred during the period of 48 hours prior to onset of symptoms in the confirmed case until the confirmed case is no longer considered infectious to be deemed close contact. Cohorting: Placing together in the same room residents who are infected with the same pathogen and are suitable roommates. Outbreak: Two or more cases of ARI in residents or staff of a RCF within 3 days (72 hrs) OR at least one case of COVID-19 confirmed by laboratory testing. Physical distance: 1.5 metres between people where practical. N.B. This is not feasible in situations where closer proximity is necessary e.g. assisting residents with some activities – personal hygiene, medical procedures. Communication: Staff can access COVID-19 information on the Barwon Health One Point intranet site. Information is also available at each RACF in the communication folders. 1 Date:1st June 2020 Infection Prevention Service Ph-42155947
Residential Aged Care Covid-19 Pandemic Plan
Procedure
COVID-19 is a contagious viral infection that generally causes respiratory illness in humans.
Presentation can range from no symptoms (asymptomatic) to severe illness with potentially life-
threatening complications, including pneumonia. COVID-19 is spread by contact with respiratory
secretions and contaminated fomites.
There is a high risk of an outbreak of COVID-19 in RACF. The elderly, who may also have co-existing
illnesses, are at increased risk of serious complications if they contract COVID-19. Infection can spread
rapidly through residential and aged care facilities if not managed appropriately.
Objectives
1. Reduce the morbidity and mortality associated with COVID-19 infection through an
organised response that focuses on prevention and containment of infection.
2. Rapidly identify, isolate and treat cases, to reduce transmission to contacts.
3. Characterise the clinical and epidemiological features of cases in order to adjust
required control measures in a proportionate manner.
4. Minimise risk of transmission to population in RACF with good hygiene and infection
prevention and control measures.
5. Ensure all staff and residents of facilities are vaccinated and protected against
influenza, with clear documentation.
6. Prepare a workforce plan, ensure business continuity and promote self-sufficiency
within facilities.
7. Continue to ensure residents and their families are involved in decisions, and respect
resident preferences and values in order to maximise quality of life and wellbeing.
Daily routine during the COVID-19 Pandemic
Daily monitoring of all residents temperature, heart rate and respiratory rate. Any observations
deviating from baseline for that resident are to be reported to nurse in charge, and to be actioned as
clinically appropriate.
Observe for clinical signs and symptoms of COVID - 19
o fever (though this may be absent in the elderly)
o acute respiratory infection (shortness of breath, dry cough, sputum production, sore throat,
runny nose, anosmia with or without a fever);
o tiredness or fatigue;
o less common symptoms may include headache, myalgia/arthralgia, chills, nausea and
vomiting, nasal congestion, diarrhoea, haemoptysis, and conjunctival congestion.
o Older people may also have the following symptoms:
increased confusion
worsening chronic conditions of the lungs
loss of appetite
o Elderly patients often have non-classic respiratory symptoms; RACF should consider testing
any resident with any new respiratory symptom.
Staff self-assessment for COVID-19 is conducted prior to each shift and includes screening
questions, monitoring for signs / symptoms of COVID-19 and checking temperature. This is
documented in the COVID-19 Staff Screening Log Book (maintained by ANUM).
Staff with temperature ≥37.5C or symptoms of COVID-19 must notify their manager. They will not
attend work and must call Staffcare on 4215 3220 to arrange testing for SARS-COV-2.
2 Date:1st June 2020 Infection Prevention Service Ph-42155947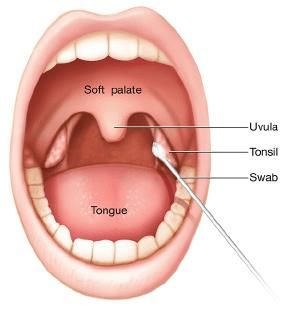
Residential Aged Care Covid-19 Pandemic Plan
Pregnant staff should be allocated to residents, and duties that have reduced exposure to residents
with confirmed or suspected COVID-19 infection.
Physical distancing is to be practiced, workplace checklist available at Safework Australia.
All staff must have had a 2020 influenza vaccination unless medically contraindicated.
Visitors to RACF
Visitors are restricted and are allowed by appointment only after approval by RACF manager. Each
facility maintains a schedule for visitors.
Visiting restriction’s do not apply for residents receiving end of life care.
A health screening check will be conducted prior to each visit, including temperature checking. This
information is recorded in a visitor register.
All visitors must have had a 2020 influenza vaccination. (Exceptions apply) Visitors are asked for
evidence of their 2020 vaccination and records are kept at each RACF.
Visitors are to only visit the resident allocated. They must enter and leave the facility directly without
spending time in communal areas. Hand hygiene is to be performed before entering and on exit of
the resident’s room and RACF.
Additional Lifestyle services and communication strategies have been implemented while visiting
restrictions are in place.
Visitors are to follow the Barwon Health RACF Visitor’s Code of Conduct, as well as the Industry
Code for visiting Residential Aged Care homes during COVID-19.
Procedure if signs and symptoms of COVID-19
Inform resident’s GP immediately of relevant clinical signs and symptoms. Afterhours use locum
service as per standard processes.
To arrange testing phone COVID-19 swabbing service – mob. 0447 311 551
Contact IPS in hours on ext. 55947 or Infectious Disease Registrar after hours on ext. 52379 if
further advice required.
Management Process for Resident with Suspected COVID-19 tool to assist.
Care of residents being tested
Initiate and maintain Droplet and Enhanced Contact Precautions (green sign). Refer to the
Barwon Health Transmission-Based Precautions Staff Information Kit for signs and detailed
information.
Testing includes PCR COVID-19, and if clinically indicated a PCR multiplex respiratory, per
Appendix 7 – Respiratory Swab collection for COVID-19
COVID-19 Mobile Pathology Testing for RAC service can assist with swabbing and delivery of
COVID-19 PCR swab to ARRL– mob. 0447 311 551
o Hours 0900 – 1600 hours daily, leave a message to collect swab if out of hours.
Check for use of nebuliser, BIPAP or CPAP and manage per Aerosol Generating Procedures
Increase monitoring of symptomatic residents and co resident when in a shared room including
temperature, heart rate and respiratory rate to at least twice daily until result known or nurse in
charge assesses resident as clinically stable.
Care for symptomatic resident in a single room if possible, if shared room, move unaffected resident
to single room as soon as able.
Provide resident with Suspected Coronavirus (COVID-19) Patient Information pamphlet.
Initiate Appendix five – Care Plan Suspected / Confirmed COVID-19.
3 Date:1st June 2020 Infection Prevention Service Ph-42155947
Residential Aged Care Covid-19 Pandemic Plan
Testing for COVID-19
People without symptoms should not be tested except in special circumstances as
directed by DoHHS such as:
recovered cases, as part of return-to-work testing for certain occupational groups,
including health care workers or aged care workers
recovered cases returning to high-risk settings such as a healthcare or aged care facility
as part of an outbreak investigation/response (active case finding)
as part of department-led enhanced surveillance (to investigate how widespread COVID-
19 is certain groups in the community).
Patients who meet the following clinical criteria should be tested:
Fever OR chills in the absence of an alternative diagnosis that explains the clinical presentation*
OR
Acute respiratory infection (e.g. cough, sore throat, shortness of breath, runny nose or anosmia)
Note: In addition, testing is recommended for people with new onset of other clinical symptoms
consistent with COVID-19** AND who are close contacts of a confirmed case of COVID-19; who
have returned from overseas in the past 14 days; or who are healthcare or aged care workers
*Clinical discretion applies including consideration of the potential for co-infection (e.g.
concurrent infection with SARS-CoV-2 and influenza)
**headache, myalgia, stuffy nose, nausea, vomiting, diarrhoea
Declaring an Outbreak
A potential COVID-19 outbreak is defined as:
Two or more cases of ARI in residents or staff of a RCF within 3 days (72 hrs).
Notify IPS immediately.
A confirmed COVID-19 outbreak is defined as:
At least one case of COVID-19 confirmed by laboratory testing.
Implement COVID-19 Outbreak Checklist
Supply
PPE, hand hygiene products and cleaning supplies are available in RACF as impress stock.
Additional PPE stock is available in De Forest House and can be accessed by IPS and the AHNC.
On confirmation of a COVID-19 Outbreak an email can be sent to
agedcareCOVIDcases@health.gov.au to activate the release of PPE from the Department of
Health. This is the responsibility of the Co-Director of Aged Care.
4 Date:1st June 2020 Infection Prevention Service Ph-42155947Residential Aged Care Covid-19 Pandemic Plan
COVID-19 Outbreak Management
Residents
Maintain Droplet and Enhanced Contact Precautions for the confirmed case.
Identified close contacts requiring isolation with Droplet and Enhanced Contact Precautions until
14 days after last close contact with the confirmed case.
Monitoring four times a day of temperature, heart rate and respiratory rate for residents with
confirmed COVID-19.
Minimum twice daily monitoring of temperature, heart rate and respiratory rate of all residents. If
symptoms develop initiate Droplet and Enhanced Contact Precautions and manage as a
suspected COVID-19 case.
Medical management of the resident is the responsibility of the GP supported by the ID registrar.
Staff
Staff will continue to self-monitor temperature and acute respiratory illness symptoms and document
in COVID-19 Staff Screening Log book at the beginning of each shift.
StaffCare (or Infectious Disease Registrar out of hours) will determine the exposure risk and close
contacts will be excluded from work and are required to self-quarantine until 14 days after last close
contact with the confirmed case.
Cleaning
Any equipment removed from a positive/suspected COVID-19 case’s room must be cleaned and
disinfected. This is a 2-step neutral wipe, then alcohol wipe, or 2-in-1 step clean disinfectant wipe (V
wipe) as recommended for Cleaning of Patient Equipment.
Minimum twice daily cleaning of communal areas and frequently touched surfaces.
Routine clean of unaffected resident rooms.
Daily 3 stage clean and disinfection of all frequent touch points of all suspected or confirmed COVID-
19 case rooms.
Staff cleaning adhere to Droplet and Enhanced Contact Precautions within all suspected or confirmed
COVID-19 case rooms.
The exit clean of a confirmed COVID-19 case will be a routine three stage clean or a two stage using
hydrogen peroxide vapour.
Waste Management
Dispose of all waste as clinical waste.
Handling of Linen
Bag linen inside resident room. Ensure wet linen is double bagged and will not leak.
Linen reprocessed as per standard precautions.
Food Services
Crockery and cutlery reprocessed per standard precautions. Food trays from resident rooms must be
placed immediately in food trolley.
Disposable crockery and cutlery may be used and will be disposed of as clinical waste.
Visitors in an outbreak
Resident’s authorised representatives will be contacted in the event of an outbreak of COVID-19.
All visitors will be restricted until advised otherwise by the DHHS
Admission and Transfers during an Outbreak
Avoid resident transfer unless clinically required (in consultation with Infectious Disease Registrar)
and respecting the residents Goals of Care.
Notify Ambulance transport and receiving hospital of the risk of COVID-19 verbally and on the
resident transfer advice form.
If transfer outside resident room is necessary, the resident should wear a surgical mask and follow
respiratory hygiene and cough etiquette. All staff should maintain droplet and enhanced contact
precautions.
Non-infected residents may be transferred to family care for the duration of the outbreak. Inform
family or carer that the resident may have been exposed and is at risk of developing COVID-19.
All new admissions to the RACF will be suspended.
5 Date:1st June 2020 Infection Prevention Service Ph-42155947Residential Aged Care Covid-19 Pandemic Plan
Care of the deceased if COVID-19 is suspected or confirmed
The same level of infection and control precautions must be used for a deceased person as were used
prior to their death.
Refer to Death of a Patient, Client or Resident from COVID-19 or Suspected COVID-19
IPS will notify the DoH and DoHHS of any deaths occurring during an outbreak.
End Outbreak
No new cases for 14 days from onset of symptoms in last case.
Confirmation with DoHHS and DoH
Review and evaluate outbreak management
Appendices:
Appendix 1 RAC COVID-19 Outbreak Checklist
Appendix 2 Care Plan Suspected/Confirmed COVID-19
Appendix 3 Initial Report to DoHHS - COVID-19 Outbreak
Appendix 4 Letter to GPs – COVID-19 Outbreak
Appendix 5 Letter to Families – Preventing Spread of COVID-19
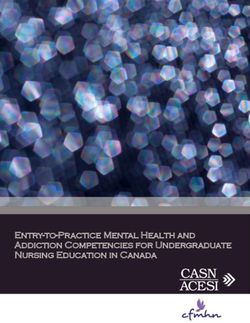
Appendix 6 Cleaning Protective Eyewear
Appendix seven - Respiratory Swab collection for COVID-19
Appendix eight - Residential Aged Care Facility COVID-19 Communication Response Record
Appendix nine – Sample COVID-19 Outbreak Case List
Appendix Ten Management Process for Resident with Suspected COVID-19
Appendix 11 - COVID-19 Staff Screening Log Book
Appendix 12 Nebuliser Therapy
Evaluation
This document is evaluated and revised by IPS and Department of Infectious Diseases following any
outbreak of COVID-19. Evidence is used from microbiology results and recorded outcomes for patients.
The IPS liaises with the DoHHS and DoH throughout the course of an outbreak.
Key Aligned Documents
Contact Tracing Infectious Diseases, PROMPT: Barwon Health \ Infectious Diseases \ Infection
Prevention Services
Death of a Patient, Client or Resident from COVID-19 or Suspected COVID-19, PROMPT: Barwon
Health \ Safety and Quality
Hand Hygiene, PROMPT: Barwon Health \ Infectious Diseases \ Infection Prevention Services
Ill Health Care Workers Responsibilities and Work Restrictions, PROMPT, Barwon Health \ Infectious
Diseases \ Infection Prevention Services
Outbreak Management Procedure and Flow Chart, PROMPT: Barwon Health \ Infectious Diseases \
Infection Prevention Services
Resident Deterioration and Escalation of Care, PROMPT: Barwon Health \Aged Care\Residential Aged
Care
Standard and Transmission-based Precautions, PROMPT: Barwon Health \ Infectious Diseases \
Infection Prevention Services
Transmission-Based Precautions Package, PROMPT: Barwon Health \ Infectious Diseases \ Infection
Prevention Services
6 Date:1st June 2020 Infection Prevention Service Ph-42155947Residential Aged Care Covid-19 Pandemic Plan Key Legislation, Acts & Standards Aged Care Act 1997 (Cwlth). Compilation No. 67. Includes amendments up to Act No. 17, 2018. Retrieved may 28, 2020 from http://www7.austlii.edu.au/cgi- bin/viewdoc/au/legis/cth/consol_act/aca199757/notes.html Aged Care Amendment (Security & Protection) Act 2007. (Cwlth). Act No. 51 of 2007. Retrieved May 28, 2020 from http://www5.austlii.edu.au/au/legis/cth/num_act/acaapa2007390/notes.html Australian Aged Care Quality Agency. (n.d.). Standards: Residential aged care. Retrieved May 28, 2020 from https://www.agedcarequality.gov.au/providers/accreditation-standards Health Records Act 2001 (VIC). Version No. 039. Version incorporating amendments as at 11 April 2018. Retrieved May 28, 2020 from http://www7.austlii.edu.au/cgi- bin/viewdb/au/legis/vic/consol_act/hra2001144/ References Barwon Health (2020) Novel Coronavirus (COVID-19) Cleaning Requirements retrieved: http://covid- 19.barwonhealth.org.au/wp-content/uploads/2020/04/COVID-19-Cleaning-Instructions.pdf COVID-19 CDNA National Guidelines for Public Health Units v2.11. Retrieved May 26, 2020 from https://www1.health.gov.au/internet/main/publishing.nsf/Content/cdna-song-novel- coronavirus.htm Victoria State Government, Health and Human Services. (2020, April 9). Coronavirus (COVID 19) Guidelines for health services and general practitioners. Retrieved May 26, 2020 from Department of Health and Human Services Victoria | Health services and general practice - coronavirus disease (COVID-19) National Health and Medical Research Council. (2019). Australian guidelines for the prevention and control of infection in healthcare. Retrieved May 26, 2020 from Australian Guidelines for the Prevention and Control of Infection in Healthcare (2019) | NHMRC 7 Date:1st June 2020 Infection Prevention Service Ph-42155947
Appendix One – Outbreak management checklist
Facility
Date Number of residents
Responsible Date
Item
commenced
Identification of Case/Outbreak
One or more case in a resident of COVID-19 confirmed by laboratory testing NUM/NIC
Facility to immediately contact Infection Prevention Service (IPS) - Tel: 4215 IPS
2325 (business hours) or via switchboard (outside business hours)
Contact tracing to be conducted. This includes staff, other residents or IPS
visitors who were in the same facility as the confirmed case
Facility to immediately implement infection control measures
Isolate / cohort suspected residents NUM/NIC
Implement droplet and enhanced contact precautions NUM/NIC
Provide PPE outside rooms NUM/NIC
Display Droplet & Enhanced Contact precautions sign outside rooms of NUM/NIC
confirmed or suspected cases
Test all symptomatic suspected cases of COVID-19 NUM/NIC
Identify any resident using nebulisers or non-invasive ventilation i.e. NUM/NIC
CPAP/BIPAP as they will require care with airborne transmission based
precautions whilst these procedures occur & for 30 minutes following. Clean
& disinfected rooms frequent touch points commencing 30 minutes after
procedure ceases
Exclude symptomatic staff & arrange testing at StaffCare Tel: 421553220 NUM/NIC
Reinforce standard precautions (hand hygiene, cough etiquette) throughout NUM/NIC
facility
Display outbreak signage at entrances to facility NUM/NIC
Commence 3 stage cleaning in suspected or confirmed COVID-19 case rooms NUM/NIC
Increase environmental cleaning of frequent touch points throughout facility Environmental
to a minimum of twice daily Services Supervisor
Notification
Arrange Infectious Diseases (ID) to attend facility with IPS, as soon as IPS
practical, to advise & check all above activities have been adequately
undertaken
Contact RAC Clinical Director & Co-Director via AHNC IPS
Contact Communication and Public Affairs via switchboard IPS
Contact Victorian Department of Health and Human Services (DHHS) on Tel: IPS
1300 651 160
Complete initial case list & provide to DHHS IPS
8 Date:1st June 2020 Infection Prevention Service Ph-42155947Email Department of health on agedcareCOVIDcases@health.gov.au to Co-Director /
activate release of PPE Clinical Director
Contact GPs and authorised representatives of suspected or confirmed NUM/NIC
residents
Provide the outbreak letter (Appendix one of RAC COVID-19 Pandemic Plan) NUM/NIC
to all residents’ GP’s
Inform authorised representatives of all residents by telephone & send NUM/NIC
outbreak letter
Inform all Staff Members not on duty NUM/NIC
Outbreak Meeting
Organise Outbreak Management Meeting as soon as practicable with IPS
following participants:
RAC Clinical Director/Co-Director
Facility Manager / NUM
IPS
ID
Public Affairs & Communications
Environmental Services Manager
Provide COVID -19 Incident Management Team (IMT) with daily updates IPS
Restrict
Avoid resident transfer unless clinically required (in consultation with ID) & NUM/NIC/ID/IPS
respecting the residents goals of care
Cancel all non-essential group activities during the outbreak period NUM/NIC
Restrict all visitors until advised by the DHHS IPS/Co-Director
Review staff allocation within RACF NUM/FM
Monitor
Monitor observations for confirmed resident’s with COVID-19 four times a NUM/NIC
day. Monitor all residents for symptoms with a minimum twice daily
observation for temperature, heart rate and respiratory rate
Daily update of case list & submission to DHHS IPS
Conduct asymptomatic COVID-19 testing of all Residents & Staff. Frequency ID/IPS
of further asymptomatic testing to be arranged in consultation with ID &
DHHS
Consultation
Daily consultation & progress update with COVID-19 IMT, DoHHS & IPS/ID
Commonwealth DoH
NUM/FM
Regular updates to residents and authorised representatives
9 Date:1st June 2020 Infection Prevention Service Ph-42155947Appendix Two – Care Plan Suspected / Confirmed COVID-19
Does person have a history of contact with a suspected/ confirmed case of COVID-19? Yes No
Date swab sent ________________Has this been confirmed with a positive swab result? Yes No
DATE: ADMISSION & ONGOING ASSESSMENT CARE PLAN
Reporting case of suspicion / confirmed Department of Health and Human Services notified on phone
case of COVID- 19 infectious illness will number 1300 651 160
be managed by IPS. Date:
Confirmed case only: mailto:agedcareCOVIDcases@health.gov.au
Date:
Advance care planning / Advance Care Confirm advanced care planning, directives and goals of care are
Directives current Yes No
Medical treatment decision maker contact details confirmed and
Staff are clear about each about the
available.
resident’s values and preferences for their
Yes No
future care.
Advance care plans, goals of care and directives: Must be
Staff have identified medical treatment discussed with the resident and family /representative
decision maker communicated to staff.
https://www2.health.vic.gov.au/hospitals-
and-health-services/patient-care/end-of-
life-care/advance-care-planning/medical-
treatment-planning-and-decisions-act
Consultation
Tick who has been contacted GP RESIDENTIAL IN REACH LOCUM
Room isolation with own ensuite Yes No
Infection prevention precautions in place Cohorted apart from other non-infected residents Yes No
Infection control precautions are in place Yes No
Refer to this guideline Single use PPE in place
Mask
Eye protection
Gloves
Long sleeved gowns: Yes No
Use of nebulizer/CPAP/BIPAP Yes No
If yes:
Airborne transmission based precautions during procedure
and for 30 minutes following
Clean and disinfect frequent touch points of resident
room following procedure
10 Date:1st June 2020 Infection Prevention Service Ph-42155947Assessments Baseline typical results for this resident include:
4/24 or QID observations or more frequent as per clinical status
Consider both measurement of resident T,P,R,BP & Oxygen saturations in Room air/on Oxygen (humidified
observations and, timely reporting and and warmed if possible)
review of results by clinical staff
Reportable levels as per GP order, or may include:
T 37.5 °C, notify GP
possible blood cultures required
Persistent tachycardia
Respiratory rate >30 breathes per minute
BP < 90 mmHg systolic, < 60 diastolic
O Sat < 90% humidified O2 via nasal prongs as prescribed by GP
If any changes in clinical status report and escalate as soon as
possible to the Registered Nurse in charge of the Shift
Is the person symptomatic? Sore Throat Yes No
High temperature Yes No
Risk of clinical deterioration Cough present Yes No
If any changes in clinical status report Increased effort to breathe Yes No
and escalate as soon as possible to the
Registered Nurse in charge of the Shift Changed conscious state Yes No
Acute onset confusion change in behaviours Yes No
Evidence of Cyanosis (blue lips or fingers) Yes No
Secretions / Crepitation present Yes No
Audible wheeze present Yes No
Medications Administered as per medication chart
Consider anticipatory medications as per goals of care
Risk of acute pain and discomfort Consider increased assessment for pain and other signs and
symptoms of distress
Nutrition and Hydration Consider resident’s current nutrition care plan including allergies,
modified diets etc., in light of current illness
Commence fluid balance chart monitoring.
Risks of dehydration and monitor
appropriately. Ensure timely referral to
dietician and /or speech therapist
11 Date:1st June 2020 Infection Prevention Service Ph-42155947Mobility Consider resident’s current mobility care plan including mobility,
transfers, etc. in light of current illness and possible functional
Risk of decreased mobility and
decline
functionality due to illness Ensure timely
referral to physiotherapist and /or
occupational therapist
Psychosocial
Risk of impact to health and wellbeing Consider residents current psychosocial needs, in light of current
including risk of increased levels of illness and care management strategies.
anxiety and exacerbation of pre-existing
mental health conditions.
Other /Allied health Consider implementation of measures to reduce complications of
immobility and functional decline: e.g. hourly deep breathing and
Risk of DVT
coughing, regular bed mobility
Risk of development of secondary
complications
Progress notes documentation Documentation should be regular to indicate clear monitoring and
evaluation of resident’s progress and overall health status.
Name:…………………………………………………..Designation:…………………………………….
Signature:………………………………………………..
12 Date:1st June 2020 Infection Prevention Service Ph-42155947Appendix Three - Initial report to DoHHS – COVID-19 Outbreak
Date/time: ___________________ Public Health Officer: _____________________
Contact details:
Person notifying outbreak: _______________ Position: ______________________
Telephone number: ____________________ Email: _________________________
Facility details:
Name of Facility_______________________________________________________
Address: _____________________________________________________________
Facility Manager / Director: ______________________________________________
Telephone number: _____________________ Fax number: ____________________
Email address: _________________________
Description of facility: __________________________________________________
Total number of residents: _______________ Total number of staff: ____________
Age range of residents: ___________________
Number of units / wings / areas in facility: __________________________________
Floorplan provided: Yes / No
Residents:
Unit name Resident no. Long term Short term / High Care Dementia / Other
Respite Secure
RCF Staff:
Staff type No. of RCF staff No. agency staff No. Causal staff No. volunteers
Management
Administrator
Cleaner
Nurse
Carer / Care
Assistant
Agency
Other (specify)
13 Date:1st June 2020 Infection Prevention Service Ph-42155947Appendix Four
Letter to GPs – COVID-19 Outbreak
……/……/……
Respiratory outbreak at [Facility Name]
Dear Doctor,
There is an outbreak of acute respiratory illness affecting residents at the facility named above. The outbreak may
involve some of your patients who may require review.
It is important to establish if the outbreak is caused by SARS-CoV-2. Coronavirus Disease 2019 (COVID-19), caused
by SARS-CoV-2, is a notifiable condition.
We recommend that you:
Establish if any of your residents are affected
Help determine if the outbreak is caused by SARS-CoV-2:
- Cases meeting the suspected case definition for COVID-19 must be tested
- Any aged care resident who has a fever (≥37.5C) OR an acute respiratory infection (e.g. shortness of
breath, cough, sore throat) are classified as a suspected case
- Testing of residents in aged care is processed at University Hospital Geelong, by the Australian Rickettsial
Reference Laboratory:
A single flocked viral swab should be used to sample the nasopharynx via the throat and both nostrils. The same
swab should be used for all three sites.
A second swab for viruses other than COVID-19 coronavirus will require a second swab referred to Australian Clinical
Labs with a separate pathology referral form.
Specimens for COVID-19 testing are to be submitted to Australian Rickettsial Reference Laboratory (ARRL). Infection
Prevention will assist with this in RAC (ext.55947).
Specimens are to be accompanied by an ARRL pathology form and request "COVID-19 PCR."
14 Date:1st June 2020 Infection Prevention Service Ph-42155947If an ARRL referral form cannot be found, an ACL form will be accepted. In such a case, please indicate in writing
that the test is being referred to ARRL and ensure that it is delivered to ARRL, not ACL.
Ensure that your residents are vaccinated against influenza, if there are no contraindications
Ensure that you observe hand hygiene procedures and use appropriate PPE when visiting your residents.
Limit the use of antibiotics to residents with evidence of bacterial superinfection, which is uncommon. There is
significant evidence that antibiotics are over-prescribed during institutional respiratory illness outbreaks.
Control measures that the facility has been directed to implement include:
Isolation of symptomatic residents
Use of appropriate PPE when providing care to ill residents
Exclusion of symptomatic staff from the facility
Restriction/limitation of visitors to the facility until the outbreak has resolved
Promotion of hand hygiene, and cough and sneeze etiquette.
Should you require further information regarding COVID-19, please refer to the Commonwealth
Department of Health website:
https://www.health.gov.au/news/health-alerts/novel-coronavirus-2019-ncov-health-alert
If you require any further information or advice please contact [insert details].
.
Yours sincerely,
[Name]
[Position]
[Facility/Organisation]
15 Date:1st June 2020 Infection Prevention Service Ph-42155947Appendix Five
Letter to Families – Preventing Spread of COVID-19
……/……/……
Dear residents, relatives and friends,
A resident who resides at Insert Facility Name has tested positive to COVID-19.
While all types of respiratory viruses can cause sickness in the elderly, COVID-19 is a particularly contagious infection
that can cause severe illness and death for vulnerable people.
The following actions have been taken in response to this confirmed case of COVID-19.
The resident with confirmed COVID-19 has been isolated in their room and family have been notified
The department of Health and Human Services have been notified and a COVID-19 Outbreak has been
declared
Barwon Health will work closely with the Department of Health and Human Services as well as the
Department of Health, to minimise the spread of infection
The Residential Aged Care COVID-19 Pandemic Plan has been implemented
Staff caring for the affected resident will take additional precautions and wear a mask, eyewear, gown and
gloves at all times
Barwon Health’s Infection Prevention Services are conducting contact tracing to identify all staff, residents and
visitors who would have had recent contact with this resident
All staff, residents and visitors who are identified as having recent contact with this resident will be tested for
COVID-19
Anyone identified as having had close contact with someone diagnosed with coronavirus disease (COVID-19)
must quarantine in a home, hotel or health care setting for 14 days after last contact with this person.
All staff suspected to have COVID-19 will be excluded from work until cleared by Infection Prevention
Services
All residents suspected to have COVID-19 will be isolated in their rooms until cleared by Infection Prevention
Services
All visitors suspected to have COVID-19 will be instructed to call the Coronavirus hotline on 1800 675 398
Surveillance for further cases of COVID-19 continues, including increasing our current practice of daily vital
sign observations on residents to twice a day
Increased cleaning includes twice daily touch point cleaning for frequently used surfaces such as handrails
and door knobs
All group Lifestyle group activities have been suspended
All visitors are now restricted from entering the facility including non-essential staff
Barwon Health is committed to keeping the safety and wellbeing of our residents and staff as the focus of our
decisions and we appreciate your assistance in protecting this vulnerable group.
We will keep you informed on the progress of the outbreak and notify you when there are updates to the restriction of
visitors.
16 Date:1st June 2020 Infection Prevention Service Ph-42155947If you have any queries or concerns please contact the Facility Manager on …. Should you require further information regarding COVID-19, please refer to the Victorian Department of Health and Human Services website: https://www.dhhs.vic.gov.au/coronavirus Yours sincerely [Name] [Position] [Facility/Organisation] 17 Date:1st June 2020 Infection Prevention Service Ph-42155947
Appendix Six - Cleaning Reusable Eye Protection 18 Date:1st June 2020 Infection Prevention Service Ph-42155947
Appendix seven - Respiratory Swab collection for COVID-19
Equipment:
Personal protective equipment (PPE) for the health care worker taking the swab, including gown, gloves, eye protection (goggles or face shield) and
surgical mask.
One dry, sterile, flocked swab nb. Two dry, sterile, flocked swabs if collecting a respiratory PCR.
o Label the swabs with patient’s full name, date of birth, specimen type, date and time of collection.
Preparation:
• Don PPE as per Sequence for putting on PPE
• Explain the procedure to the patient and obtain consent.
• Place patient standing or sitting with head tilted at 70, supported against a bed, chair or wall.
Step one – throat swab
Stand at the side of the patient’s head and ensure their head is resting against a supporting surface.
Place your non-dominant hand on the patient’s forehead.
Ask patient to open mouth widely and say “aaagh” Throat
Using the flocked swab, insert the swab into the mouth, avoiding any saliva. swab
Place lateral pressure on the swab to collect cells from the tonsillar fossa to ensure the swab contains epithelial cells (not
mucus)
Step two – Nasal swab Nb. Respiratory PCR testing will only require swabbing of the nasal septum (not throat).
Remain at side of patient’s head and place your non-dominant hand on the patient’s forehead with your thumb at the tip
of the nose. Nose
The other hand inserts the same swab used for the throat swab horizontally into the patient’s nostril, approx. 2-3 cm swab
Place pressure on the swab in order to collect sells from the midline nasal septum.
Rotate the swab twice (2 x 360 turns) collecting the epithelial cells (not mucus) from the nostril.
Repeat procedure in other nostril.
Place specimen in biological transport bag, preferably held by staff outside room to keep outside of bag clean.
Alternatively, clean bag with alcohol wipe after doffing PPE
On completion
Remove PPE inside patient’s room per Sequence for taking off PPE and dispose of PPE into clinical waste receptacle.
Specimen Handling and Transport
Place transport tube with the COVID-19 PCR specimen (i.e. nose and throat swab) into a plastic bag and include request form.
Deliver to Australian Rickettsial Reference Laboratory (ARRL) located on 3rd level of Douglas Hocking Research Institute.
19 Date:1st June 2020 Infection Prevention Service Ph-42155947COVID-19 Testing Guidance Using ‘Kang Jian Swab’
Tests Viruses Tested Indications for Test Results Timeline
COVID-19 PCR SARS-CoV-2* COVID-19 testing 6 – 24 hours
(**ARRL request form) (depending on when received at laboratory)
Multiplex Respiratory Influenza A & B Adenovirus Mycoplasma Non COVID-19 viral respiratory testing is 1 x Dry flocked swab >24 hours
PCR RSV pneumonia indicated.
(Australian Clinical Labs Parainfluenza 1-4 Chlamydophila pneumonia
request form) Human C. psittaci
metapneumovirus, Bordatella pertussis
Rhinovirus/enterovirus
Swabs
Kang Jian Virus collection and preservation system swab
How to conduct a oropharyngeal and nasal swab
Perform hand hygiene before and after procedure.
Don appropriate personal protective equipment (PPE): such as non-sterile gloves, gown, surgical mask and protective eyewear.
Tilt patient’s head back slightly.
First, insert the swab into the posterior pharynx and tonsillar areas. Rub swab over both tonsillar pillars and posterior oropharynx and avoid
touching the tongue, teeth, and gums.
With the same swab conduct a ‘deep nasal swab’
Using a pencil grip and while gently rotating the swab, insert the tip 2–3 cm (or until resistance is met), into the nostril, parallel to the palate, to
absorb mucoid secretion.
Rotate the swab several times against the nasal wall for 10-15 seconds.
Repeat swabbing (as above) with the same swab in the other nostril
Put the swab into the tube.
Break off the swab from the break point (approx. 1cm above the head of the swab)
Tighten the lid & shake
*SARS-CoV-2 is the virus that causes COVID-19
**Australian Rickettsial Reference Laboratory
20 Date:1st June 2020 Infection Prevention Service Ph-42155947Appendix eight - Residential Aged Care Facility COVID-19 Communication Response Record
Facility name:
Source Document Distribution date Distributed to Distribution Signature
mechanism
One point Coronavirus
information for staff
One point Today’s health news
Press clippings
One point Infection Prevention
Service page
Communique from the
CEO. Please print and
display to support staff
who are not frequently
accessing email.
Department of health Fact sheets
Department of health Website
21 Date:1st June 2020 Infection Prevention Service Ph-42155947
6
5
4
3
2
1
Case Number
PHO
Resident or Staff (R or S)
DHHS Use only
DATE: 13/03/20
Outbreak number
Location
22 Date:1st June 2020
Occupation (Staff only)
FACILITY:
Surname
Firstname
Sex (M or F)
DOB (dd-mm-yyyy)
Date of
symptoms worked
(dd/mm) (dd/mm)
onset of Date last
Sudden onset of symptoms (Y/N)
Fever or Temp >38°C (Y/N)
Appendix nine – Sample COVID-19 Outbreak Case List
Respiratory symtoms (cough, sore throat,
Clinical
coryza, SOB) (Y/N)
General symptoms (myalgia, malaise,
COVID-19 - ILLNESS REGISTER (LINE LISTING) - RESIDENTS and STAFF
lethargy, headache) (Y/N)
Hospitalised (Y/N)
Deceased (Y/N)
Died
COVID-19 PCR
Date swab taken (dd-mmm)
Result
Swab
PCR multiplex respiratory
TOTAL NUMBER OF STAFF:
TOTAL NUMBER OF RESIDENTS:
Date taken
Infection Prevention Service Ph-42155947
Result
Vaccinated 2020 (Y/N)
FluAd (A)
/ other Fluvax (X)
Vaccination
0
3
Date vaccinated
Prophylaxis
Treatment
Antivirals
Date commenced
results)
** (Includes swab
Other Comments
Prevention
by Infection
be provided
This will
excel format.
Services in anAppendix Ten Management Process for Resident with Suspected COVID-19
Identify suspected COVID-19 Managing a suspected Stopping transmission based
resident COVID-19 case precautions for COVID-19
•Patients who meet the following •Immediately commence droplet and •A negative result for COVID-19
clinical criteria should be tested: enhanced contact precautions communicated to nurse unit manager -
•Fever temperature ≥37.5C OR chills •Contact GP available on BOSSnet
in the absence of an alternative •If GP unavailable - phone Infection
diagnosis that explains the clinical Prevention Service ext.55947/52325 •Droplet transmission based
presentation 0700 - 2100 hrs. or ID registrar Mob. precautions to continue if an influenza
•OR 0434 181 822 2100 2100 – 0700 hrs. like illness, await results from
•Acute respiratory infection that is •Testing: respiratory PCR
characterised by cough, sore throat or •Single flocked viral swab
shortness of breath •Swab both nostrils and throat for COVID- •COVID-19 confirmed cases remains in
19 PCR droplet and enhanced contact
•Note: In addition, testing is transmission based precautions until
•Swab to ARRL* for COVID-19 PCR decided by Infectious Disease
recommended for people with new • ph -0435 405 253 COVID-19 support
onset of other clinical symptoms Registrar.
nurse for collection of swab
consistent with COVID-19* AND who •Respiratory multiplex PCR (if taken)
are close contacts of a confirmed case swab to ACL**
of COVID-19 or who have returned
from overseas in the past 14 days. •Do not refrigerate specimen
•Cleaning:
•*headache, myalgia, runny or stuffy •Triple clean resident's room daily
nose, anosmia, nausea, vomiting, •*ARRL - Australian Rickettsial Reference
diarrhoea Laboratory at UHG
•**Australian Clinical Laboratory
•Residential aged care workers who are
unwell are to notify manager and contact
Staffcare on ph. 0408 127 147
23 Date:1st June 2020 Infection Prevention Service Ph-42155947Appendix 11 - COVID-19 Staff Screening Log Book
Please complete the table – use a tick or X to indicate if you have any COVID symptoms, a high temperature or contact with a COVID case.
If any box contains an X, then please discuss with ANUM / Manager immediately before commencing work
Date Name Staff ID Area of work I have NO My Temperature is I have had NO close Signature
number COVID less than 37.5 contact with COVID
symptoms case
9/4/2020 Florence Nightingale 007007 Percy Baxter √ √ √
24 Date:1st June 2020 Infection Prevention Service Ph-42155947Appendix 12 Nebuliser Therapy
You can also read