Development of unmanned aerial vehicle (UAV) networks delivering early defibrillation for out- of- hospital cardiac arrests (OHCA) in areas ...
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
Open access Original research
BMJ Open: first published as 10.1136/bmjopen-2020-043791 on 22 January 2021. Downloaded from http://bmjopen.bmj.com/ on September 13, 2021 by guest. Protected by copyright.
Development of unmanned aerial
vehicle (UAV) networks delivering early
defibrillation for out-of-hospital cardiac
arrests (OHCA) in areas lacking timely
access to emergency medical services
(EMS) in Germany: a comparative
economic study
Jan Bauer ,1 Dieter Moormann,2 Reinhard Strametz,3 David A Groneberg4
To cite: Bauer J, Moormann D, ABSTRACT
Strametz R, et al. Development Strengths and limitations of this study
Objectives This study wants to assess the cost-effectiveness
of unmanned aerial vehicle of unmanned aerial vehicles (UAV) equipped with automated
(UAV) networks delivering ►► This is the first large-scale analysis showing the
external defibrillators (AED) in out-of-hospital cardiac arrests
early defibrillation for out- cost-effectiveness of unmanned aerial vehicle (UAV)
(OHCA). Especially in rural areas with longer response times of
of-hospital cardiac arrests equipped with automated external defibrillators
(OHCA) in areas lacking emergency medical services (EMS) early lay defibrillation could
in out-of-hospital cardiac arrests compared with
timely access to emergency lead to a significant higher survival in OHCA.
emergency medical services on national level.
medical services (EMS) in Participants 3296 emergency medical stations in Germany.
►► Depending on UAV coverage, cost-effectiveness was
Germany: a comparative Setting Rural areas in Germany.
examined on national level accounting for existing
economic study. BMJ Open Primary and secondary outcome measures Three UAV
2021;11:e043791. doi:10.1136/
emergency medical services, purchase prize, main-
networks providing 80%, 90% or 100% coverage for rural
bmjopen-2020-043791 tenance, UAV life span and life years gained.
areas lacking timely access to EMS (ie, time-to-defibrillation:
►► However, there are still technical, legal and prac-
►► Prepublication history for >10 min) were developed using a location allocation analysis.
tical issues to be resolved before the actual field
this paper is available online. For each UAV network, primary outcome was the cost-
implementation.
To view these files, please visit effectiveness using the incremental cost-effectiveness ratio
the journal online (http://dx.doi. (ICER) calculated by the ratio of financial costs to additional life
org/10.1136/bmjopen-2020- years gained compared with current EMS.
043791). representative data taken from 31 emergency
Results Current EMS with 3926 emergency stations was able
to gain 1224 life years on annual average in the study area. medical services (EMS).1 If cardiopulmo-
Received 13 August 2020 nary resuscitation (CPR) is applied before
Revised 30 December 2020
The UAV network providing 100% coverage consisted of 1933
UAV with average annual costs of €43.5 million and 1845 the arrival of EMS, the 30-day survival rate is
Accepted 12 January 2021
additional life years gained on annual average (ICER: €23 568). twice as high compared with no CPR before
The UAV network providing 90% coverage consisted of 1074 EMS arrival.2 EMS in Germany are repre-
UAV with average annual costs of €24.2 million and 1661 sented by ambulance vehicles and/or emer-
additional life years gained on annual average (ICER: €14 548). gency physician vehicles. In Germany, during
The UAV network providing 80% coverage consisted of 798 44.6% of OHCA settings, CPR was initiated by
UAV with average annual costs of €18.0 million and 1477 bystanders before the arrival of EMS. Further-
additional life years gained on annual average (ICER: €12 158). more, 22.4% of OHCA in Germany in 2018
Conclusion These results reveal the relevant life-saving
showed a shockable rhythm in the initial
potential of all modelled UAV networks. Furthermore, all
© Author(s) (or their rhythm analysis (ie, ventricular tachycardia or
employer(s)) 2021. Re-use analysed UAV networks could be deemed cost-effective.
However, real-life applications are needed to validate the ventricular fibrillation).1 Since early defibril-
permitted under CC BY-NC. No
commercial re-use. See rights findings. lation within the first 10 min after OHCA
and permissions. Published by onset is a major aspect of CPR in OHCA,
BMJ. shorter time- to-
defibrillation translates into
For numbered affiliations see BACKGROUND higher survival rates.3 Time-to-defibrillation
end of article. The incidence of out-of-
hospital cardiac is defined as the interval from emergency call
Correspondence to
arrests (OHCA) in Germany in 2018 was to first defibrillation. Defibrillation initiated
Dr Jan Bauer; 121 per 100 000 citizens with a survival >10 min after the emergency call has been
j.bauer@med.uni-frankfurt.de to discharge rate of 13.2%, based on placed, has a survival to discharge rate of
Bauer J, et al. BMJ Open 2021;11:e043791. doi:10.1136/bmjopen-2020-043791 1Open access
BMJ Open: first published as 10.1136/bmjopen-2020-043791 on 22 January 2021. Downloaded from http://bmjopen.bmj.com/ on September 13, 2021 by guest. Protected by copyright.
13.2%, whereas patients who were defibrillated inOpen access
BMJ Open: first published as 10.1136/bmjopen-2020-043791 on 22 January 2021. Downloaded from http://bmjopen.bmj.com/ on September 13, 2021 by guest. Protected by copyright.
issue. However, if UAV are deemed to be cost-effective, calculated by the ratio of financial costs to the sum of the
such coverages are likely to be the goal on the long run, additional life years gained by UAV compared with EMS.
to provide equal access within an area. The demand The reference period for the calculation was the first 12
was covered if the time- to-
defibrillation was 10 min, a total of 14 689 life years were
allocation solver was applied using the problem type gained in 12 years with an annual average of 1224.
‘minimum facilities’ within ArcGIS Pro 2.5 (ESRI, Compared with this benchmark the different UAV
Redlands, USA). The location- allocation solver uses network configurations performed as follows (see also
Hillsman editing to generate a set of semi-randomised table 1): in order to provide universal coverage (100%),
solutions. Then a vertex substitution heuristic is applied the analysis revealed that 1933 UAV were necessary. These
to refine the solutions. Finally, the solutions are combined translated into costs of €512.9 million in 12 years. In
by a metaheuristic to return near-optimal results.20 In other words, the average annual costs were €43.5 million.
order to identify the minimum number of UAV base loca- However, in 12 years the UAV network was able to gain
tions covering 80% and 90% of the demand, we applied 22 145 additional life years with an annual average of 1845
an iterative approach: first, we identified the UAV base compared with the benchmark. The ICER for this UAV
location covering the maximum demand within a catch- network configuration was €23 568 per additional life
ment of 8.33 km. Second, this location and its covered year.
demand were removed. With the remaining demand In order to cover 90% of the demand, 1074 UAV were
locations both steps were repeated. Using this approach, necessary. This UAV network would cost €24.2 million
we were able to estimate the minimum number of base per year and 19 932 additional life years could be gained
locations needed to cover 80% and 90% of the demand. in 12 years with costs of €14 548 per additional life year
(ICER).
Cost-effectiveness On the other hand, if only 80% of the demand was
To simulate financial costs of UAV networks, the covered, the UAV network configuration resulted in the
following assumptions were made: (1) UAV purchase following configuration: 798 UAV were necessery, which
prize (inlcuding AED): €50 000, (2) annual UAV mainte- translated into average annual costs of €18.0 million.
nance cost: 20% of purchase prize and (3) UAV lifespan: By using this network, 17 722 additional life years were
4 years.18 The mean life expectancy of OHCA survivor gained in 12 years with an ICER of €12 158 per additional
was assumed to be 12 years as shown in a recent study.21 life year.
Survival to discharge in relation to time-to-defibrillation
was modelled as follows: time-to-defibrillation 5–10 min:
33.1% survival; time- to-
defibrillation >10 min: 13.2% DISCUSSION
survival.4 22 The incremental cost- effectiveness ratio We modelled three different UAV networks for rural areas
(ICER) as the assessment of cost- effectiveness was providing a maximum time- to-
defibrillation of 10 min
Bauer J, et al. BMJ Open 2021;11:e043791. doi:10.1136/bmjopen-2020-043791 3Open access
BMJ Open: first published as 10.1136/bmjopen-2020-043791 on 22 January 2021. Downloaded from http://bmjopen.bmj.com/ on September 13, 2021 by guest. Protected by copyright.
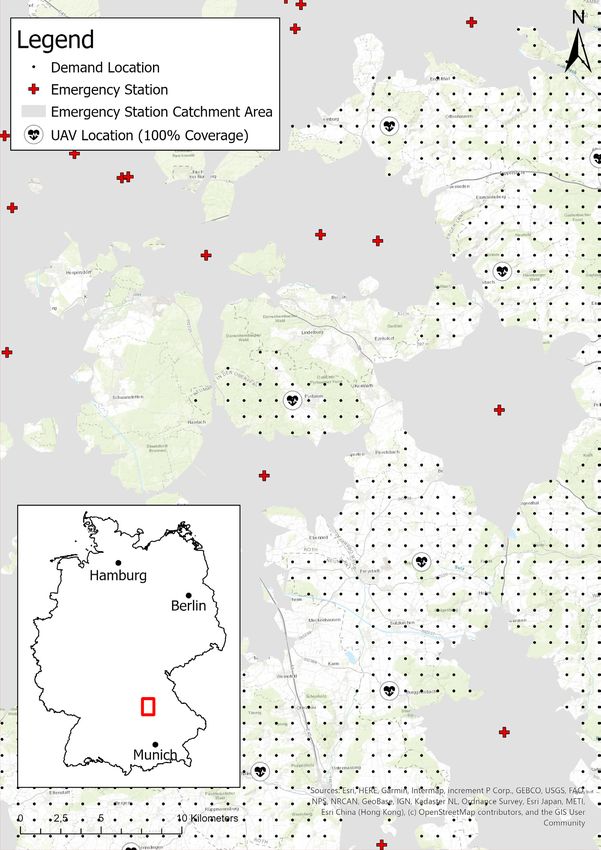
Figure 1 Unmanned aerial vehicle (UAV) network configuration for universal coverage (100%) with adjoining emergency
stations in an exemplary region in southern Germany.
Table 1 Overview of cost-effectiveness analysis using life years for different UAV network configurations
UAV network Cost (million €) Additional life years**
Maintenance Total in 12 Annual Total in 12 Annual
Coverage UAV (n) Purchase* per year years average First year years average ICER (€)
100% 1933 96.7 19.3 521.9 43.5 284 22 145 1845 23 568
90% 1074 53.7 10.7 290.0 24.2 256 19 932 1661 14 548
80% 798 39.9 8.0 215.5 18.0 227 17 722 1477 12 158
*Every 4 years due to UAV lifetime.
†Additional life years compared with the benchmark (ie, no UAV network).
ICER, incremental cost-effectiveness ratio; UAV, unmanned aerial vehicle.
4 Bauer J, et al. BMJ Open 2021;11:e043791. doi:10.1136/bmjopen-2020-043791Open access
BMJ Open: first published as 10.1136/bmjopen-2020-043791 on 22 January 2021. Downloaded from http://bmjopen.bmj.com/ on September 13, 2021 by guest. Protected by copyright.
in Germany and evaluated their cost-effectiveness. Our network, which is monitored centrally translating in low
results revealed the life-saving potential for all modelled personnel expenditure. However, due to technical prog-
UAV networks: providing universal coverage, the UAV ress, costs are expected to decrease in the future, so that
network was able to gain 1845 additional life years on the reported costs represent maximum costs and the
annual average. Even if the coverage was lowered to 80%, ICER is likely to decrease in the future. For these reasons,
the UAV network was still able to gain 1477 additional life the use of UAV networks in real OHCA situations must
years on annual average. The benefit in this cost-effective be evaluated. For such studies, our results could serve as
analysis (ICER) was operationalised by life years gained. a guide for the selection of potential study areas. Still,
However, the quality-adjusted life years (QALY) are often the concept of an AED equipped UAV has already been
used instead. QALY are calculated by combining the life- shown to be potentially feasible.11 The feasibility was
time gained by an intervention with the health-related furthermore shown in a study using an UAV in an out-of-
quality of life.18 23 24 A recent study showed that UAV sight flight to autonomously transport and deliver AED.28
networks can potentially gain 30 267 additional QALY In general, UAV within the medical scope have been
within 4 years.18 However, the concept of QALY is contro- mainly used within three categories: (1) medical trans-
versial, not least because of ethical questions being raised, port (2) medical surveillance and observation and (3)
which is why the unadjusted life years were used in the disaster relief.9 10 In regard to medical surveillance and
present study. observation, UAV have been used for the surveillance
It must be noted that we assumed evenly distrib- of swimmers in a Triathlon,29 simulated scenarios of
uted incidence of OHCA among the grid cells within a drowning at the beach30 and on-site body documentation
municipality. This leads to possible overestimation of in crime scenes of forensic cases.31 Within these studies.
UAV coverage since, in reality, the incidence of OHCA is UAV have been shown to provide better results compared
unevenly distributed within a municipality or even within with traditional approaches. Regarding disaster relief,
the grid cells. This bias was introduced due to a lack of UAV have been studied mainly in search and rescue oper-
data providing the exact location of historical OHCA in ations.32–34 Here, a wider area could be searched faster by
a municipality. an UAV compared with the standard procedure. The same
The National Institute for Health and Care Excellence applied to the use of UAV within mass casualty incidents
in the UK stated that an intervention can be deemed showing their feasibility.35 36 Lastly in regard to medical
cost-effective if the ICER is below €22 278 (£20 000) to transport, UAV have been successfully used to transport
€33 417 (£30 000).25 Accordingly, the UAV networks with laboratory samples,37 blood products,38 39 vaccines40 and
80% and 90% coverage (ICER of €12 158 and €14 548, flotation devices to prevent drowning.41 The use of AED
respectively) could be considered cost-effective. However, equipped UAV can therefore be seen as a reasonable
thresholds regarding cost- effectiveness are difficult to extension of the previous applications.28 However, so far,
determine and therefore different thresholds have been AED equipped UAV have not been implemented within
applied internationally (eg, $A46 400 in Australia).26 The common practice but are the focus of many national
finding of cost-effectiveness was also reported in a study studies (eg, Sweden or Canada).28 33 42 Theoretically,
in North Carolina with an ICER of €768 (US$858).18 police officers and firefighters could be additionally
However, due to the different underlying assumptions, dispatched instead of an UAV to reduce the time- to-
this study is not directly comparable and the lower ICER defibrillation in OHCA settings, where the response time
can be explained by the inclusion of urban areas and a of EMS would be too long. However, this is not standard
significantly lower estimated purchase prize (€15 000 care in Germany but happens occasionally if police or
per UAV). In our study, we excluded urban areas since fire fighters have been dispatched for a different reason
provision of EMS was assumed to be adequate and timely (eg, house fire or a possible crime). Including police and
in urban areas. This is supported by Claesson et al, who fire fighters within the rescue chain of a ‘regular’ OHCA
reported a potential reduction of time-to-defibrillation in would require specific regulations that address the legal,
urban areas by 1.5 min and up to 19 min in rural areas technical and personal aspects in Germany. In other
compared with EMS.27 UAV networks have furthermore countries such dual dispatch systems have already been
been studied in Toronto. Here, the analyses showed that studied or even implemented on regional level showing a
81 bases and 100 drones would be required to deliver an moderate, but significant increase in the 30‐day survival
AED 3 min earlier compared with standard EMS.14 Thus, of OHCA cases.43 However, further studies are needed to
the presented results illustrate the possibilities that UAV address these issues more deeply.
represent for the survival of patients, especially in rural The time-to-defibrillation threshold used in our study
areas. It must be noted that the results were based on (10 min) was chosen due to the significant decline of
simulations and theoretical considerations and there- survival rates associated with delayed defibrillation
fore uncertainties remain regarding financial costs and exceeding 10 min after the emergency call.3 4 However,
the life years gained. The financial costs were estimated real-life application of AED-equipped UAV could heavily
under the assumption of large quantities, since the costs alter the time frames used in our study due to personal
for prototypes are significantly higher. The estimates were issues like aversion to UAV or handling insecurities. It
also based on the assumption of a fully automated UAV must also be noticed that the time frames used have been
Bauer J, et al. BMJ Open 2021;11:e043791. doi:10.1136/bmjopen-2020-043791 5Open access
BMJ Open: first published as 10.1136/bmjopen-2020-043791 on 22 January 2021. Downloaded from http://bmjopen.bmj.com/ on September 13, 2021 by guest. Protected by copyright.
adopted from international studies that may not reflect still technical, legal and practical issues to be resolved
Germany-specific time frames. The principal acceptance before the implementation in current practice.
of UAV for medical purposes has already been demon-
strated in disaster scenarios.44 Also, it simulated OHCA Author affiliations
1
Division of Health Services Research, Institute of Occupational Medicine, Social
settings, positive experiences have been reported inter-
Medicine and Environmental Medicine, Goethe-Universitat Frankfurt am Main,
acting with an AED-equipped UAV.45 In addition, it has Frankfurt, Germany
been shown that the instructions given to first responder 2
Institute for Flight System Dynamics, RWTH Aachen University, Aachen, Nordrhein-
by the dispatchers are crucial to the success of using the Westfalen, Germany
3
AED correctly.19 Therefore, telephone instructions of Wiesbaden Business School, RheinMain University of Applied Sciences, Wiesbaden,
Hessen, Germany
resuscitation (T- CPR) are essential (T- CPR protocols). 4
Institute of Occupational Medicine, Social Medicine and Environmental Medicine,
Furthermore, retrieving an AED in a single bystander Goethe-Universitat Frankfurt am Main, Frankfurt am Main, Hessen, Germany
OHCA situation would require an interruption of CPR:
the median hands-off time in a simulation was reported to Contributors JB designed the study, monitored data collection, cleaned and
be 94 s.19 Since continued CPR is the mainstay of any effort analysed the data, prepared cartographic material and drafted the paper. DM,
made by lay bystanders, CPR must be continued until a RS and DAG revised the paper and contributed to methodological aspects of the
study. All authors discussed and interpreted the results and contributed to the final
dual bystander situation develops where one bystander manuscript.
can proceed with CPR while the other one retrieves the
Funding The authors have not declared a specific grant for this research from any
AED. This issue, however, also applies to publicly acces- funding agency in the public, commercial or not-for-profit sectors.
sible AED in a single bystander situation. Map disclaimer The depiction of boundaries on this map does not imply the
In our study, we assumed that every UAV base location expression of any opinion whatsoever on the part of BMJ (or any member of its
is only equipped with a single UAV. Theoretically, this group) concerning the legal status of any country, territory, jurisdiction or area or
could reduce effectiveness if more than one OHCA occur of its authorities. This map is provided without any warranty of any kind, either
express or implied.
at the same time within the UAV base locations catch-
ment. Another study has shown that by using existing Competing interests None declared.
EMS locations to launch the UAV, 80.1% of the poten- Patient and public involvement Patients and/or the public were not involved in
the design, or conduct, or reporting, or dissemination plans of this research.
tial OHCA sites were reached within 1 min and adding
new sites to launch UAV resulted in 90.3% of demand Patient consent for publication Not required.
being reached.46 In our study, the potential UAV base Provenance and peer review Not commissioned; externally peer reviewed.
locations were not identical to existing EMS locations. Data availability statement Data are available on reasonable request.
Using current EMS locations as UAV base locations would Open access This is an open access article distributed in accordance with the
decrease the effectiveness in rural areas due to increasing Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which
UAV travel times. permits others to distribute, remix, adapt, build upon this work non-commercially,
and license their derivative works on different terms, provided the original work is
Finally, it should be noted that the most frequent barriers properly cited, appropriate credit is given, any changes made indicated, and the use
regarding the application of UAV in the above-described is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
scenarios were legal restrictions and technical problems.
ORCID iD
Such restrictions represent barriers regarding the imple-
Jan Bauer http://orcid.org/0000-0001-6267-9731
mentation and the utilisation of UAV in such a setting:
legal issues (eg, conflicts in airspace or no-fly zones) and
technical issues (eg, weather conditions or maintenance)
may prohibit or hinder the UAV utilisation. From a legal REFERENCES
point of view, UAV must be provided an automatic launch 1 Went J, Gräsner J, Seewald S. Öffentlicher jahresbericht -
ausserklinische reanimation, 2019.
license in case of an OHCA, otherwise obtaining a sepa- 2 Hasselqvist-Ax I, Riva G, Herlitz J, et al. Early cardiopulmonary
rate launch license would exceed both the relevant time resuscitation in out-of-hospital cardiac arrest. N Engl J Med
frames and the costs. Therefore, a future implementation 2015;372:2307–15.
3 Drennan IR, Lin S, Thorpe KE, et al. The effect of time to defibrillation
must be accompanied by both legal and technical aspects. and targeted temperature management on functional survival after
Having said that, the results of this study demonstrate out-of-hospital cardiac arrest. Resuscitation 2014;85:1623–8.
4 Hansen CM, Kragholm K, Granger CB, et al. The role of bystanders,
potential benefits of AED-equipped UAV in a best-case first responders, and emergency medical service providers in
scenario with optimal circumstances. timely defibrillation and related outcomes after out-of-hospital
cardiac arrest: results from a statewide registry. Resuscitation
2015;96:303–9.
5 Nennecke A, Geiss K, Hentschel S, et al. Survival of cancer patients
in urban and rural areas of Germany--a comparison. Cancer
Epidemiol 2014;38:259–65.
CONCLUSIONS 6 Bürger A, Wnent J, Bohn A. The effect of ambulance response time
The presented study demonstrated the relevant life-saving on survival following out-of-hospital cardiac arrest-an analysis from
potential of UAV equipped with AED in out-of-hospital the German resuscitation registry. Dtsch Arztebl Int 2018;115:541–8.
7 Agerskov M, Nielsen AM, Hansen CM, et al. Public access
cardiovascular arrests: 1477 to 1845 additional years of defibrillation: great benefit and potential but infrequently used.
life can be gained on an annual average compared with Resuscitation 2015;96:53–8.
8 Deakin CD, Anfield S, Hodgetts GA. Underutilisation of public access
EMS. In relation, the financial costs UAV equipped with defibrillation is related to retrieval distance and time-dependent
AED can be considered cost-effective. However, there are availability. Heart 2018;104:1339–43.
6 Bauer J, et al. BMJ Open 2021;11:e043791. doi:10.1136/bmjopen-2020-043791Open access
BMJ Open: first published as 10.1136/bmjopen-2020-043791 on 22 January 2021. Downloaded from http://bmjopen.bmj.com/ on September 13, 2021 by guest. Protected by copyright.
9 Rosser JC, Vignesh V, Terwilliger BA, et al. Surgical and of-hospital cardiac arrests vs emergency medical services. JAMA
medical applications of Drones: a comprehensive review. JSLS 2017;317:2332–4.
2018;22:e2018.00018. 29 Homier V, de Champlain F, Nolan M, et al. Identification of swimmers
10 Bhatt K, Pourmand A, Sikka N. Targeted applications of Unmanned in distress using Unmanned aerial vehicles: experience at the Mont-
aerial vehicles (Drones) in telemedicine. Telemed J E Health Tremblant Ironman Triathlon. Prehosp Emerg Care 2020;24:1–8.
2018;24:833–8. 30 Claesson A, Svensson L, Nordberg P, et al. Drones may be used
11 Van de Voorde P, Gautama S, Momont A, et al. The drone ambulance to save lives in out of hospital cardiac arrest due to drowning.
[A-UAS]: golden bullet or just a blank? Resuscitation 2017;116:46–8. Resuscitation 2017;114:152–6.
12 Mathiesen WT, Bjørshol CA, Kvaløy JT, et al. Effects of modifiable 31 Urbanová P, Jurda M, Vojtíšek T, et al. Using drone-mounted cameras
prehospital factors on survival after out-of-hospital cardiac arrest in for on-site body documentation: 3D mapping and active survey.
rural versus urban areas. Crit Care 2018;22:99. Forensic Sci Int 2017;281:52–62.
13 Dijkstra L, Poelman H. A harmonised definition of cities and rural 32 Lygouras E, Santavas N, Taitzoglou A, et al. Unsupervised human
areas: the new degree of urbanisation. WP 01/2014. European detection with an embedded vision system on a fully autonomous
Commission, 2014. http://ec.europa.eu/regional_policy/sources/ UAV for search and rescue operations. Sensors 2019;19:3542.
docgener/work/2014_01_new_urban.pdf 33 Clark DG, Ford JD, Tabish T. What role can unmanned aerial vehicles
14 Boutilier JJ, Brooks SC, Janmohamed A, et al. Optimizing a Drone play in emergency response in the Arctic: a case study from Canada.
network to deliver automated external defibrillators. Circulation PLoS One 2018;13:e0205299–16.
2017;135:2454–65. 34 Karaca Y, Cicek M, Tatli O, et al. The potential use of unmanned
15 Felder S, VanAarsen K, Davis M. Decreasing time to first shock: aircraft systems (drones) in mountain search and rescue operations.
routine application of defibrillation pads in prehospital STEMI. CJEM Am J Emerg Med 2018;36:583–8.
2020;22:82–5. 35 Jain T, Sibley A, Stryhn H, et al. Comparison of unmanned aerial
16 Datenschutzerklärung. Federal statistical office and statistical vehicle technology-assisted triage versus standard practice in
offices of the Länder. Municipality directory information system, triaging casualties by paramedic students in a mass-casualty
2019. Available: https://www.destatis.de/DE/ZahlenFakten/ incident scenario. Prehosp Disaster Med 2018;33:375–80.
LaenderRegionen/Regionales/Gemeindeverzeichnis/ 36 Sibley AK, Jain TN, Butler M, et al. Remote scene Size-up using
Gemeindeverzeichnis.html [Accessed 5 Dec 2019]. an Unmanned aerial vehicle in a simulated mass casualty incident.
17 Eurostat. Population grids, 2018. Available: https://ec.europa. Prehosp Emerg Care 2019;23:332–9.
eu/eurostat/statistics-explained/index.php/Population_grids# 37 Ochieng WO, Ye T, Scheel C, et al. Uncrewed aircraft systems
Methodology [Accessed 17 Jun 2020]. versus motorcycles to deliver laboratory samples in West Africa: a
18 Bogle BM, Rosamond WD, Snyder KT, et al. The case for Drone- comparative economic study. Lancet Glob Health 2020;8:e143–51.
assisted emergency response to cardiac arrest. N C Med J 38 Amukele T, Ness PM, Tobian AAR, et al. Drone transportation of
2019;80:204–12. blood products. Transfusion 2017;57:582–8.
19 Sanfridsson J, Sparrevik J, Hollenberg J, et al. Drone delivery of 39 Wen T, Zhang Z, Wong KKL. Multi-objective algorithm for blood
an automated external defibrillator - a mixed method simulation supply via unmanned aerial vehicles to the wounded in an
study of bystander experience. Scand J Trauma Resusc Emerg Med emergency situation. PLoS One 2016;11:e0155176–22.
2019;27:40. 40 Haidari LA, Brown ST, Ferguson M, et al. The economic and
20 ESRI Inc. Algorithms used by the ArcGIS network analyst extension, operational value of using drones to transport vaccines. Vaccine
2020. Available: https://pro.arcgis.com/en/pro-app/latest/help/ 2016;34:4062–7.
analysis/networks/algorithms-used-by-network-analyst.htm 41 Seguin C, Blaquière G, Loundou A, et al. Unmanned aerial vehicles
[Accessed 17 Dec 2020]. (drones) to prevent drowning. Resuscitation 2018;127:63–7.
21 Andrew E, Nehme Z, Wolfe R, et al. Long-Term survival following out- 42 Mermiri MI, Mavrovounis GA, Pantazopoulos IN. Drones for
of-hospital cardiac arrest. Heart 2017;103:1104–10. automated external defibrillator delivery: where do we stand? J
22 Malta Hansen C, Kragholm K, Pearson DA, et al. Association Emerg Med 2020;59:660–7.
of bystander and first-responder intervention with survival after 43 Hasselqvist-Ax I, Nordberg P, Herlitz J, et al. Dispatch of firefighters
out-of-hospital cardiac arrest in North Carolina, 2010-2013. JAMA and police officers in out-of-hospital cardiac arrest: a nationwide
2015;314:255–64. prospective cohort trial using propensity score analysis. J Am Heart
23 Sassi F. Calculating QALYs, comparing QALY and DALY calculations. Assoc 2017;6. doi:10.1161/JAHA.117.005873. [Epub ahead of print:
Health Policy Plan 2006;21:402–8. 04 Oct 2017].
24 Whitehead SJ, Ali S. Health outcomes in economic evaluation: the 44 Hart A, Chai PR, Griswold MK, et al. Acceptability and perceived
QALY and utilities. Br Med Bull 2010;96:5–21. utility of drone technology among emergency medical service
25 Love-Koh J, Taylor M. Physical activity and the environment - final responders and incident commanders for mass casualty incident
report, 2017. management. Am J Disaster Med 2017;12:261–5.
26 Bertram MY, Lauer JA, De Joncheere K, et al. Cost-effectiveness 45 Zègre-Hemsey JK, Grewe ME, Johnson AM, et al. Delivery of
thresholds: pros and cons. Bull World Health Organ 2016;94:925–30. automated external defibrillators via Drones in simulated cardiac
27 Claesson A, Fredman D, Svensson L, et al. Unmanned aerial vehicles arrest: users' experiences and the Human-Drone interaction.
(drones) in out-of-hospital-cardiac-arrest. Scand J Trauma Resusc Resuscitation 2020;157:83–8.
Emerg Med 2016;24:1–9. 46 Pulver A, Wei R, Mann C. Locating AED enabled medical Drones
28 Claesson A, Bäckman A, Ringh M, et al. Time to delivery of an to enhance cardiac arrest response times. Prehosp Emerg Care
automated external defibrillator using a Drone for simulated out- 2016;20:378–89.
Bauer J, et al. BMJ Open 2021;11:e043791. doi:10.1136/bmjopen-2020-043791 7You can also read