Diagnosis, Management, and Treatment of Female Genital Mutilation or Cutting in Girls
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
CLINICAL REPORT Guidance for the Clinician in Rendering Pediatric Care
Diagnosis, Management, and Treatment
of Female Genital Mutilation or Cutting
in Girls
Janine Young, MD, FAAP,a Nawal M. Nour, MD, MPH, FACOG,b Robert C. Macauley, MD, FAAP,c Sandeep K. Narang, MD, JD, FAAP,d
Crista Johnson-Agbakwu, MD, MSc, FACOG,e SECTION ON GLOBAL HEALTH, COMMITTEE ON MEDICAL LIABILITY AND RISK
MANAGEMENT, COMMITTEE ON BIOETHICS
Female genital mutilation or cutting (FGM/C) involves medically unnecessary abstract
cutting of parts or all of the external female genitalia. It is outlawed in the
United States and much of the world but is still known to occur in more than
30 countries. FGM/C most often is performed on children, from infancy to a
Department of General Pediatrics, Denver Health Refugee Clinic, and
adolescence, and has significant morbidity and mortality. In 2018, an Human Rights Clinic, Denver Health and Hospitals and School of
estimated 200 million girls and women alive at that time had undergone FGM/ Medicine, University of Colorado Denver, Denver, Colorado; bAfrican
Women’s Health Center, Department of Obstetrics and Gynecology,
C worldwide. Some estimate that more than 500 000 girls and women in the Brigham and Women’s Hospital and Harvard Medical School, Harvard
United States have had or are at risk for having FGM/C. However, pediatric University, Boston, Massachusetts; cDepartment of Pediatrics, Oregon
prevalence of FGM/C is only estimated given that most pediatric cases remain Health and Science University, Portland, Oregon; dDivision of Child
Abuse Pediatrics, Ann and Robert H. Lurie Children’s Hospital of
undiagnosed both in countries of origin and in the Western world, including in Chicago and Department of Pediatrics, Feinberg School of Medicine,
the United States. It is a cultural practice not directly tied to any specific Northwestern University, Chicago, Illinois; and eRefugee Women’s
Health Clinic, Department of Obstetrics and Gynecology, Valleywise
religion, ethnicity, or race and has occurred in the United States. Although it is Health Medical Center and Office of Refugee Health, Southwest
mostly a pediatric practice, currently there is no standard FGM/C teaching Interdisciplinary Research Center, School of Social Work, Watts College
of Public Service and Community Solutions, Arizona State University,
required for health care providers who care for children, including Phoenix, Arizona
pediatricians, family physicians, child abuse pediatricians, pediatric
urologists, and pediatric urogynecologists. This clinical report is the first Clinical reports from the American Academy of Pediatrics benefit from
expertise and resources of liaisons and internal (AAP) and external
comprehensive summary of FGM/C in children and includes education reviewers. However, clinical reports from the American Academy of
Pediatrics may not reflect the views of the liaisons or the
regarding a standard-of-care approach for examination of external female organizations or government agencies that they represent.
genitalia at all health supervision examinations, diagnosis, complications, The guidance in this report does not indicate an exclusive course of
management, treatment, culturally sensitive discussion and counseling treatment or serve as a standard of medical care. Variations, taking
into account individual circumstances, may be appropriate.
approaches, and legal and ethical considerations.
All clinical reports from the American Academy of Pediatrics
automatically expire 5 years after publication unless reaffirmed,
revised, or retired at or before that time.
To cite: Young J, Nour NM, Macauley RC, et al. AAP SECTION
ON GLOBAL HEALTH, AAP COMMITTEE ON MEDICAL LIABILITY
AND RISK MANAGEMENT, AAP COMMITTEE ON BIOETHICS.
Diagnosis, Management, and Treatment of Female Genital
Mutilation or Cutting in Girls. Pediatrics. 2020;145(6):
e20201012
Downloaded from www.aappublications.org/news by guest on September 21, 2021
PEDIATRICS Volume 145, number 6, June 2020:e20201012 FROM THE AMERICAN ACADEMY OF PEDIATRICS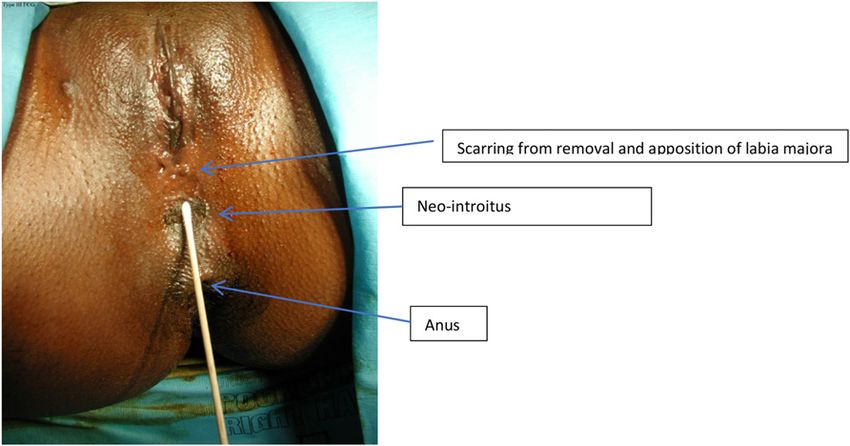
BACKGROUND a traditional rite of passage, and/or risk for having FGM/C performed, but
Female genital mutilation or cutting upholds prescribed religious beliefs these estimates are projections based
(FGM/C)* is currently outlawed in (although no sacred texts recommend on country of origin prevalence data
much of the world. The United this practice).6,7 FGM/C is and may, therefore, not be precise or
Nations,1 the World Health predominantly performed on children accurate.13 To date, no reliable data
Organization (WHO),2 the and adolescents ranging in age from exist quantifying the true number of
International Federation of Obstetrics newborn infants to 15 years; the girls and women residing in the
and Gynecology,3 and the American typical age varies by region of the United States who have had FGM/C
Medical Association4 are among world, country, state, province, and performed.13
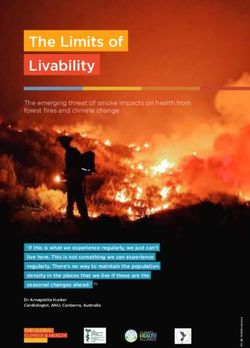
multiple organizations that even town or village8 (see Fig 2).
The majority of FGM/C occurs in 30
unequivocally oppose all forms of However, the vast majority of
African and Middle Eastern countries,
FGM/C (see Table 1). medical literature, teaching, and
with highest prevalence in Egypt,
research is focused on chronic
FGM/C involves medically Somalia, Guinea, Djibouti, Mali, Sierra
issues affecting women of
unnecessary cutting of parts or all of Leone, Sudan, and Eritrea.14 However,
childbearing age and on the
the external female genitalia, FGM/C also occurs with unknown
management of FGM/C during
including the clitoris, prepuce, labia frequency in Yemen, Oman, the
pregnancy and the peripartum and
United Arab Emirates, Bahrain,
minora, and labia majora. FGM/C may postpartum periods.9,10
be associated with significant northern Iraq, India, Malaysia, and
morbidity and mortality and is not To date, there are neither national Indonesia15 and has been reported to
associated with any medical benefit. nor international clinical practice occur sporadically in Russia16,17 and
Notwithstanding this morbidity, it is guidelines that are specifically Colombia.18 The practice of FGM/C is
still performed and has been focused on FGM/C in infants and not uniformly performed throughout
practiced in many cultures for prepubertal and pubertal girls. any given country and may be
thousands of years, predating clustered on the basis of economic
This clinical report’s primary goal is
Judaism, Christianity, and Islam.5 status, level of education, rural versus
to educate pediatric health care
Historically and in present-day, FGM/C urban geographic location, ethnic
providers on the continued
is a cultural practice not directly tied and/or tribal affiliation, and religious
occurrence of FGM/C, the populations
to any specific religion, ethnicity, or beliefs. In half of the countries with
that it affects, diagnosis,
race and has been reported to still available data on FGM/C prevalence,
complications, treatment
occur throughout the world, including most girls have had FGM/C
options, and the provision of
in the United States, but with higher performed before 5 years of age
culturally sensitive counseling,
prevalence in parts of the Middle (see Fig 2).
all while taking into consideration
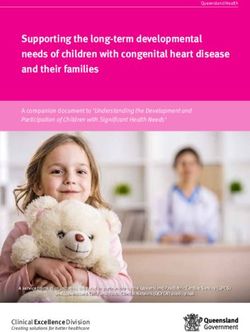
East, Asia, and Africa (see Fig 1). the legal and ethical aspects of Although it is illegal in the United
Reasons why FGM/C is performed a practice that is illegal in the States, FGM/C has been reported in
vary by region and culture and may United States and much of the world the United States in sporadic cases
include a belief that it increases (see Table 2). over the past several years.19,20 The
marriageability, preserves virginity, federal Department of Justice
improves hygiene, perpetuates prosecuted its first case against a US
PREVALENCE physician accused of having
* Currently, there are few experts in the United National and international data on the performed FGM/C across state lines
States who care for children and teenagers with prevalence of FGM/C in children and in up to 100 children (see The Law
FGM/C (see Table 4 for a link to access regional
specialists). As such, it is of utmost importance to adolescents are difficult to obtain and and FGM/C in Minors in the United
identify regional specialists, including child abuse are based on either maternal report States for further current case
pediatricians, gynecologists, urologists, and or estimates derived from data on the details).21 At of time of writing, the
mental health providers, with whom to collaborate adult female population who present charges were dismissed by the
if providing medical care for children and mainly for obstetrical care. The district judge of the Eastern District
teenagers affected by or at risk for FGM/C. FGM/C
is an accepted term adopted by many United Nations Children’s Fund of Michigan.22 This specific case is
international organizations and in medical estimated that in 2018, 200 million focused on the practice of FGM/C in
research papers and, as such, will be used girls and women alive at that time the Dawoodi Bohra community in
throughout this document.9,12,16 Infibulation refers had undergone FGM/C worldwide.11 India and among a subset of the
to type III FGM/C (see FGM/C Types and
Some authors estimate that more Dawoodi Bohra immigrant
Classification in addition to Fig 4). Defibulation
refers to a surgical procedure that opens the scar than 500 000 girls and women who community in the United States. The
formed in patients with type III FGM/C (see live in the United States (as of 2012) illegal practice of US families sending
Defibulation). have had FGM/C performed or are at their children abroad to have FGM/C
Downloaded from www.aappublications.org/news by guest on September 21, 2021
2 FROM THE AMERICAN ACADEMY OF PEDIATRICS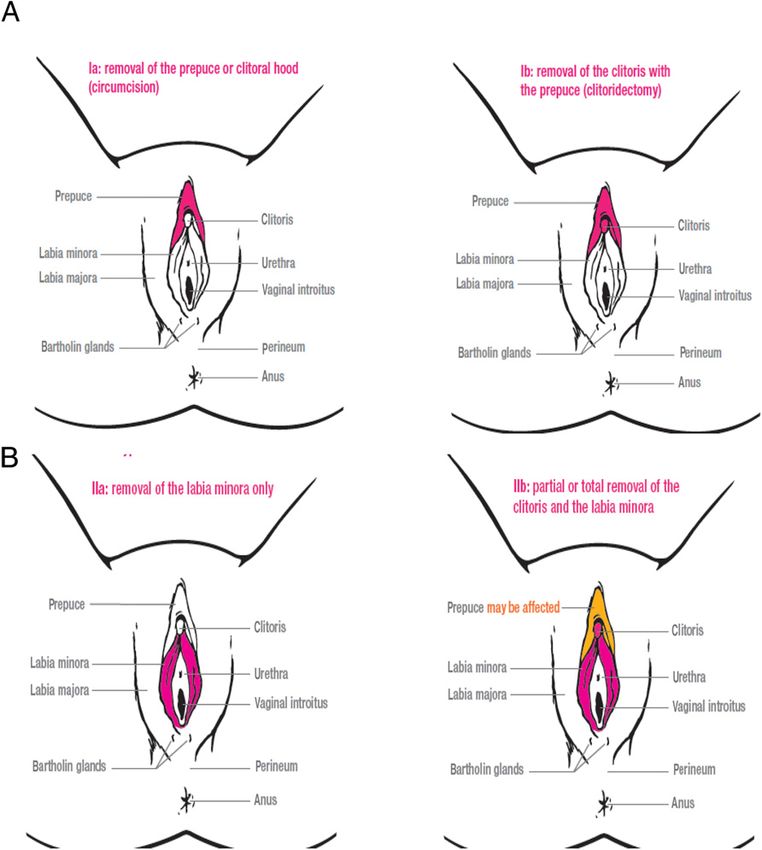
TABLE 1 FGM/C Recommendations
Recommendations
FGM/C is illegal in the United States.
FGM/C is a violation of human rights.
FGM/C has no medical benefit.
FGM/C is associated with serious and potentially life-threatening complications that can have lifelong impacts on health.
Health care providers should not perform any type of FGM/C on female infants, girls, or teenagers.
Health care providers caring for girls at risk for FGM/C should actively counsel families against performing FGM/C, including when families travel to countries
where FGM/C is practiced.
A genital examination allows health care professionals to identify FGM/C and other medical findings of significance.
If genital examination findings are equivocal for the presence of FGM/C and risk factors for FGM/C are present, a specialist trained in identification of FGM/C
should be consulted (see Table 4).
The management of FGM/C should include complete documentation of clinical findings and the use of ICD-10 coding.
Health care providers should recommend defibulation for all girls and teenagers with type III FGM/C, irrespective of whether complications are currently
present.
performed (also known as “vacation FGM/C TYPES AND CLASSIFICATION significant long-term morbidity (see
cutting”) is also presumed to The WHO has classified FGM/C into Complications and Management)
occur.23,24 However, prevalence data four distinct types (see Table 3), with (Figs 3–11). To better delineate
are nonexistent to date.13 type III associated with the most specific findings, the WHO has also
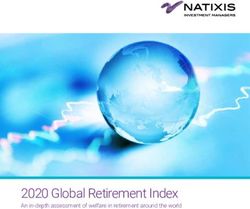
included subtypes of FGM/C,
categorized as Ia and Ib, IIa–IIc, and
IIIa and IIIb (see Fig 12). However,
the practice of FGM/C is not
standardized, and physical findings
may overlap between types and
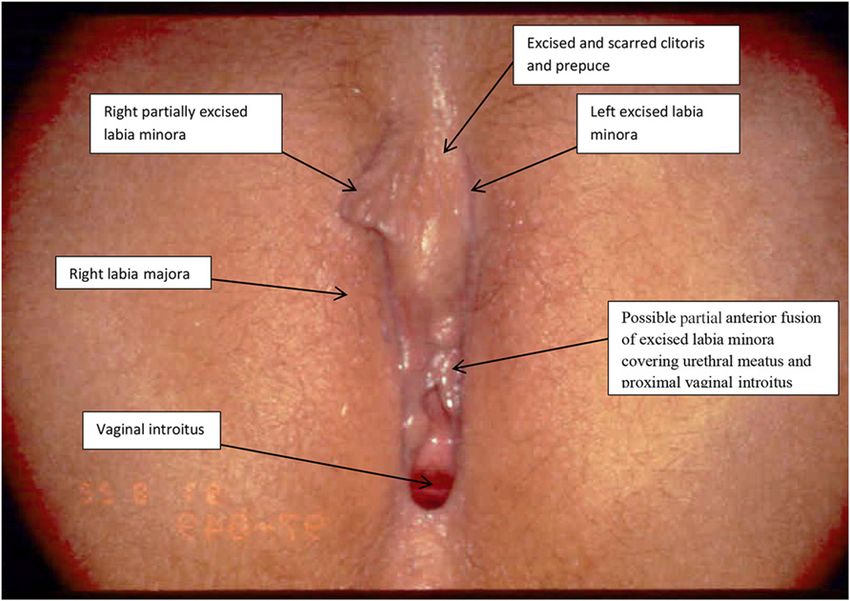
subtypes (see Figs 5 and 6).
Type I FGM/C is classified as
cutting of the glans or part of
the body of the clitoris and/or
prepuce; type II includes
excision of the clitoris and labia
minora, with or without excision
of the labia majora; type III,
infibulation, includes cutting and
apposing the labia minora and/or
majora over the urethral meatus and
vaginal opening to significantly
narrow it and may include
clitoral excision (Figs 10 and 11);
and type IV includes piercing,
scraping, nicking, stretching, or
otherwise injuring the
external female genitalia without
removing any genital tissue
and includes practices that do not fall
into the other three categories
(Fig 13).
Prevalence of FGM/C subtypes is
mainly influenced by ethnicity and
region. Surveys of girls and women
FIGURE 1 older than 15 years reveal that
FGM/C global prevalence. Countries where FGM/C is practiced with unknown frequency and not approximately 10% of cases are
pictured on this map include Oman, the United Arab Emirates, Bahrain, India, Malaysia, Russia, and
Colombia.15–18 South Sudan seceded from Sudan in 2011 but is not noted on this map.107 Repro-
FGM/C type III, or infibulation,
duced with permission from United Nations Population Fund. Demographic Perspectives on Female although these numbers are based on
Genital Mutilation. Copyright © United Nations Population Fund 2015. self-report and likely under- or
Downloaded from www.aappublications.org/news by guest on September 21, 2021
PEDIATRICS Volume 145, number 6, June 2020 3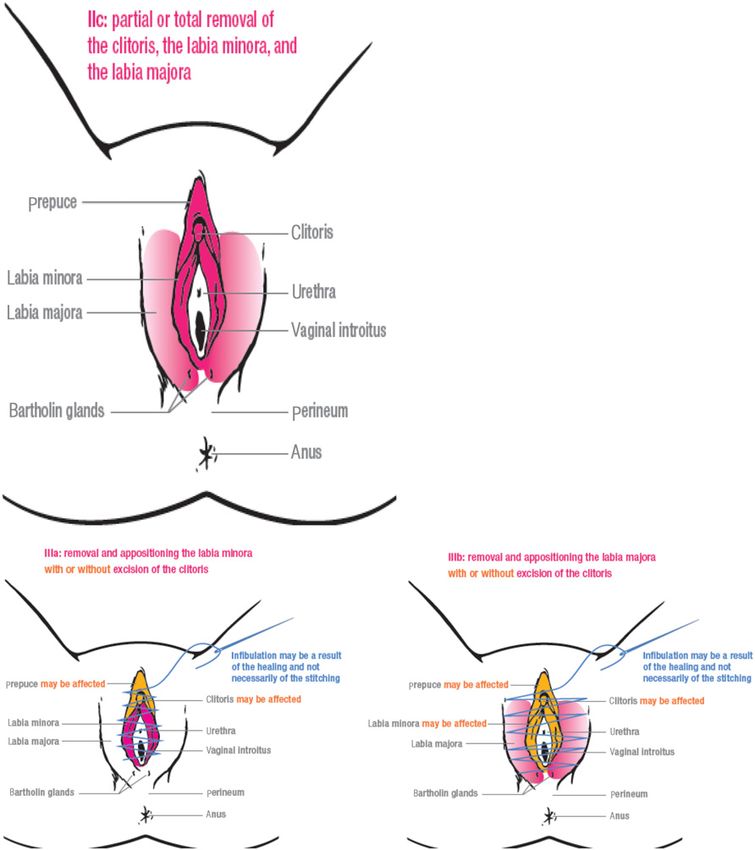
note the lack of training in diagnosis,
management, and cultural and legal
aspects of care in adult women.29–32
One recent US study revealed that of
79 general pediatricians surveyed,
73% had received no previous FGM/C
education, 89% did not feel confident
in their ability to identify FGM/C
types, and frequency of performing
external genital examinations on
female patients at health supervision
visits was inversely related to the age
of the patient (with 75% performing
examinations on infants, down to only
8% in 17- to 18-year-olds).28 In
literature from other high-income
countries with immigrant populations
from regions where FGM/C is
prevalent, pediatricians have
reported identifying FGM/C in
pediatric patients, managing
complications from remote and
recent procedures, and, in some
instances, being asked to perform
FGM/C in children.9,33,34 However,
one survey conducted in Australia
revealed that of pediatricians
surveyed, most reported neither
discussing nor examining children for
FGM/C.34,35
CLINICAL HISTORY TAKING
FIGURE 2 For children with possible risk factors
Maternal report of age that girls have undergone FGM/C, by country. Reproduced with permission for FGM/C (eg, mother or sibling with
from UNICEF. Female Genital Mutilation/Cutting: A Statistical Overview and Exploration of the
Dynamics of Change. New York, NY: UNICEF; 2013:41. Copyright © United Nations Children’s a history of FGM/C, country of origin,
Fund 2013. birth country, and/or history of travel
to a country where FGM/C is
practiced), it is recommended that
overestimate the actual prevalence of KNOWLEDGE OF, ATTITUDE ABOUT, AND clinical assessment of FGM/C status
type III FGM/C.8 The practice of PRACTICE OF FGM/C IN THE UNITED be integrated into routine pediatric
infibulation, the removal and STATES care. Nonetheless, it can be
apposition of the labia minora and/or Knowledge of FGM/C is believed to be challenging. It is of utmost
labia majora with or without cutting limited among US pediatric providers importance for the pediatric health
of the clitoris, is concentrated in because there are no nationally care provider to establish a trusting
northeastern Africa in Djibouti, required courses on diagnosis of type, relationship with the child or
Eritrea, and Somalia. Data management, or treatment of FGM/C teenager and her family to allow for
extrapolated from 2004 to 2008 East for medical students, residents, or nonjudgmental questions and
African regional surveys of girls and fellows in general pediatrics, family ongoing counseling. Experts
women 15 years and older revealed medicine, adolescent medicine, child suggest that health care providers
that 82% to 99% reported to have abuse pediatrics, urology, or ask the patient or parent the term
had undergone FGM/C, and of these gynecology.9,26–28 Instead, existing they use to name female genital
cases, 34% to 79% were type III studies from the United States are cutting. Use of the word
(Somalia having the highest focused on nurse midwives and mutilation is not recommended when
prevalence of type III).25 obstetricians and gynecologists and discussing FGM/C with patients and
Downloaded from www.aappublications.org/news by guest on September 21, 2021
4 FROM THE AMERICAN ACADEMY OF PEDIATRICS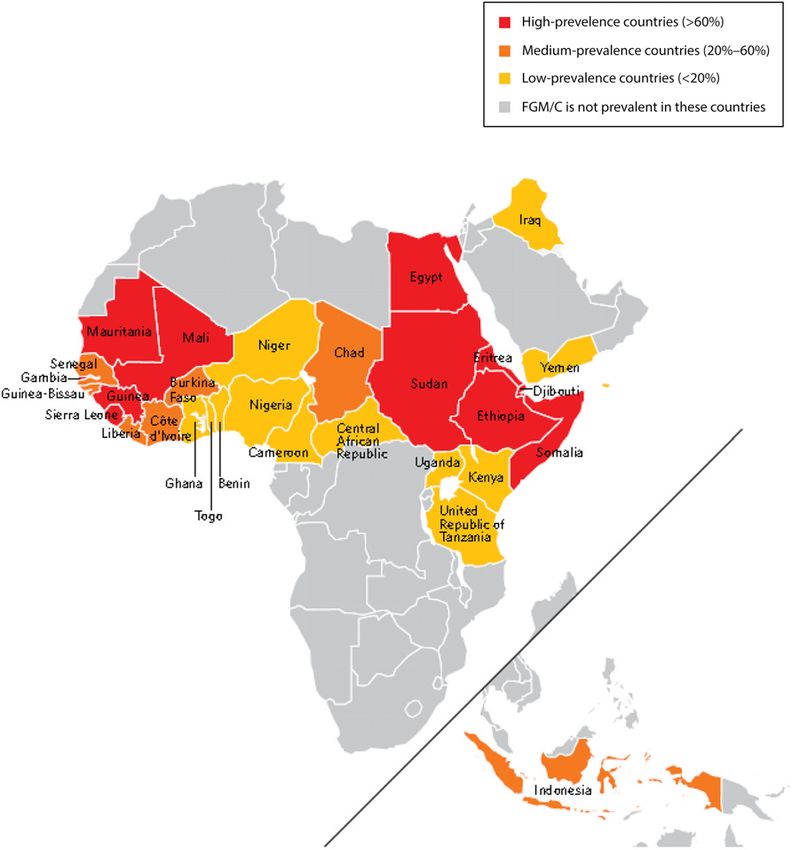
TABLE 2 Timeline of International Legislation Against FGM/C may also be very limited.
Country Year Legislation Enacted a Understanding each girl’s and
Benin 2003
mother’s current knowledge and
Burkina Faso 1996 perception of FGM/C, addressing
Central African Republic 1966, 1996b fears, providing age-appropriate
Chad 2003 education about pelvic anatomy, and
Côte d’Ivoire 1998 sharing information about the
Djibouti 1995, 2009b
Egypt 2008
importance of the annual physical
Eritrea 2007 examination can facilitate ongoing
Ethiopia 2004 rapport and engagement with health
The Gambia 2015108 care. In addition, some girls or
Ghana 1994, 2007b parents may request a female health
Guinea 1965, 2000b
Guinea-Bissau 2011
care provider as well as a female
Iraq (Kurdistan region) 2011 interpreter. For girls at risk for FGM/
Kenya 2001, 2011b C, it is advisable that efforts be made
Mauritania 2005 to honor this request, if at all possible,
Niger 2003 given social and cultural expectations.
Nigeria (some states) 1999–2006
Senegal 1999 It is important for health care
Somalia 2012 providers to assess each patient
Sudan (some states) 2008–2009
Togo 1998
individually and make no
Uganda 2010 assumptions about her and her
United Republic of Tanzania 1998 parents’ beliefs regarding FGM/C.
Yemen 2001 Mothers and fathers may or may not
Reproduced with permission from United Nations Children’s Fund. Female Genital Mutilation/Cutting: A Statistical Over- hold discordant views about FGM/C,
view and Exploration of the Dynamics of Change. New York, NY: United Nations Children’s Fund; 2013:9. Copyright © and some clinical experts suggest that
UNICEF 2013.
a Bans outlawing FGM/C were passed in some African countries, including Kenya and Sudan, during colonial rule. This mothers who have themselves
table includes only legislation that was adopted by independent African nations and does not reflect earlier rulings. undergone FGM/C may nonetheless
b Later dates reflect amendments to the original law or new laws.
oppose subjecting their daughters to
this practice. Instead, treating
patients and caregivers with respect,
caregivers because it is potentially may initially withhold information sensitivity, and professionalism will
inflammatory and also difficult to about previous FGM/C. encourage them to return and
translate (and may not be supports health-seeking behavior.
understood). When caring for girls with or at risk
for FGM/C, it is important to In families with risk factors for FGM/C,
Given that girls who had FGM/C approach FGM/C discussion, physical including having a mother and/or
performed at a young age may not examination, and counseling with other girls who have already been cut
recall being cut (as well as the fact cultural sensitivity. Girls’ genitalia in the family, it is advisable to inquire,
that parents or primary guardians may have never been examined in a nonthreatening manner, whether
may not reveal a history of FGM/C to before, although they may have had the parents are planning to perform
their children), obtaining a history of multiple physical examinations in the FGM/C on their daughter. Raising
FGM/C from the girl alone may yield United States or abroad.28 Girls and such a sensitive topic may elicit
little relevant clinical information. mothers who have been cut may be various emotions, but this is a vital
Instead, it is advisable that the FGM/C afraid to seek care from a health care educational opportunity to reiterate
clinical history taking include both provider because of concerns about child safety, the morbidity and
the girl and parent or guardian disapproval or previous negative mortality associated with FGM/C, and
once rapport has been established. experiences being used to teach its legal consequences. Such
Similarly, some parents or guardians trainees or other health care discussions may occur over multiple
may not be aware that FGM/C providers about FGM/C; many will visits, and it is recommended to
performed in the country of seek a physician’s care only if there is revisit these discussions, particularly
origin before immigration is not a health problem. Irrespective of their if the child is being seen before a trip
prosecutable in the United States (see culture, girls’ and mothers’ to countries where FGM/C is still
The Law and FGM/C in Minors in the knowledge of female anatomy, practiced. Whether to have this
United States) or may fear judgment reproductive health, family planning, discussion in front of the girl depends
from US medical providers, so they and sexually transmitted infections on the developmental age of the child,
Downloaded from www.aappublications.org/news by guest on September 21, 2021
PEDIATRICS Volume 145, number 6, June 2020 5
TABLE 3 FGM/C ICD-10 Coding and WHO Classification
FGM/C Type ICD-10 Code109 WHO Classification (2016)
Female genital mutilation, N90.810
unspecified
Female genital mutilation, N90.811 Partial excision of the clitoris and/or prepuce
type I
— Ia: removal of prepuce only
— Ib: partial or totala removal of clitoris and prepuce
Female genital mutilation, N90.812 Partial or totala removal of the clitoris and labia minora, with or without excision of the labia majora
type II
— IIa: removal of labia minora only
— IIb: partial removal of the clitoris and labia minora
— IIc: partial removal of the clitoris, labia minora and majora
Female genital mutilation, N90.813 Infibulation: narrowing of the vaginal orifice by cutting and apposing the labia minora and/or labia majora over
type III the vaginal opening; may include excision of the clitoris
— IIIa: removal and apposition of the labia minora
— IIIb: removal and apposition of the labia majora
Other female genital N90.818 Unclassified (all other harmful procedures for non-medical purposes), including piercing
mutilation
— IV
—, not applicable.
a Although WHO classification describes total removal of the clitoris, it is the glans or the glans and part of the body of the clitoris that is cut.110
her degree of understanding, and the providers are both aware that EXTERNAL FEMALE GENITAL
dynamics within the family. education about FGM/C medical EXAMINATION: STANDARDS AND
Encouraging parents to reevaluate complications and illegality has been DOCUMENTATION
this practice in a nonjudgmental discussed and aware of what specific Bright Futures: Guidelines for Health
manner and impressing on them that issues have and have not been Supervision of Infants, Children, and
FGM/C causes medical complications, discussed. Similarly, given that FGM/ Adolescents, Fourth Edition,
has no medical indications, and is also C performed overseas and before US recommends that “each visit include
against the law (with associated legal emigration does not constitute a complete physical examination.” A
consequences) will hopefully a violation of US law, it is of utmost complete physical examination
facilitate reconsideration of this importance to document past history includes assessment of genitalia from
practice. It is also essential to and timing of FGM/C in the chart so birth to age 21.36
document these discussions in the that it is clear that there are no legal
It is recommended that pediatricians
medical chart so that health care ramifications for the family.
and other health care providers
include genital inspection as part of
all health supervision examinations
and be knowledgeable about the
variants of normal genital anatomy
and the signs of previous genital
cutting.33
The external genital examination in
girls should include the identification
of the prepuce, clitoris, and labia
minora and majora (see Figs 14–16),
and the examination should be
performed in frog-leg position with
chaperone use documented, per
FIGURE 3 recommendations of the American
Prepubertal female with labial adhesions, Academy of Pediatrics.37 In
no FGM/C. (Reprinted with permission from prepubertal girls, it may be more
American Academy of Pediatrics. Visual Di-
agnosis of Child Abuse on CD-ROM. 3rd ed. Elk FIGURE 4 difficult to identify the clitoris, and in
Grove Village, IL: American Academy of Pediat- Periclitoral adhesions, 18-month-old female these cases, the prepuce may need to
rics; 2008.) patient, no FGM/C (photo credit: J.Y.). be partially retracted to facilitate
Downloaded from www.aappublications.org/news by guest on September 21, 2021
6 FROM THE AMERICAN ACADEMY OF PEDIATRICS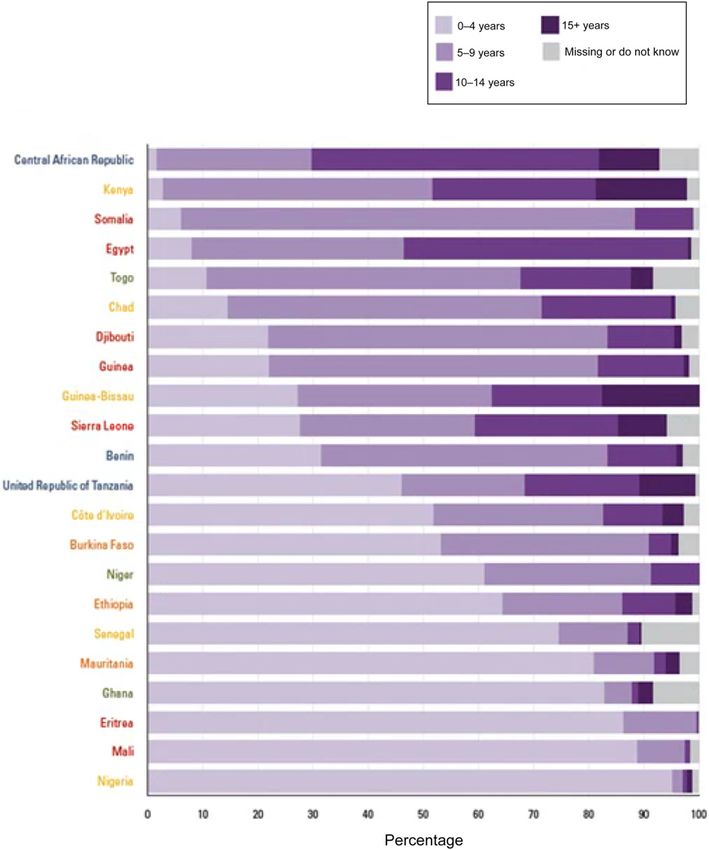
consulted, although currently, there
are few such specialists in the United
States (see Table 4 for a link to access
regional specialists). However, given
the subtleties of some FGM/C, it is
assumed that not all cases will be
identified.
If FGM/C is suspected to have
occurred recently, it may also be
difficult to confirm on physical
examination without prompt
evaluation by a specialist. The
genitalia are highly vascularized
tissues, healing occurs quickly, and
less invasive cutting may easily be
missed in some cases, given minimal
or only subtle scarring.
If FGM/C is identified on examination,
FIGURE 5 it is advisable that the clinician
Type IIb or IIIa FGM/C in a prepubertal girl (excised clitoris, prepuce, partially excised right labia discuss findings with the caregiver
minora, absent left labia minora, and possible partial anterior fusion of excised labia minora
covering urethral meatus and proximal vaginal introitus). This photo was reviewed by three FGM/C and/or child if the child is old enough
experts (J. Abdulcadir, C.J.A, and J.Y), and consensus was either type IIb or IIIa. Arrows were added to participate in medical decision-
by J.Y. (Reprinted with permission from Graham EA. Ritual female genital cutting [RFGC] PowerPoint making. Medical complications,
slides. 2014. Available at: https://ethnomed.org/resource/ritual-female-genital-cutting-rfgc- depending on the type of FGM/C
powerpoint-slides/. Accessed April 30, 2020.)
diagnosed, should be reviewed with
the caregiver and/or child, as well as
identification. Similarly, the labia physical examination, particularly in when to return for care if any of these
minora is less developed, and it is prepubertal girls. Similarly, complications develop (see
advisable that efforts be made to prepubertal labial adhesions may be Complications and Management). If
identify this structure as well. miscategorized as FGM/C (see Figs an older child or teenager is unaware
Although not systematically studied, 3–6). If genital examination findings that she has had FGM/C performed
anecdotal experience by some experts are equivocal for the presence of (as may be the case if a girl had FGM/
suggests that types I, II, and IV FGM/C FGM/C and risk factors for FGM/C are C performed at a young age), it is
and even some type III subtypes may present, a specialist trained in important that a culturally sensitive
be difficult to recognize during the identification of FGM/C should be approach be taken to further discuss
her diagnosis with her (see the
Appendix for further guidance).
Although not systematically studied,
FGM/C is a community practice, and
in some cultures, aunts, grandparents,
or other figures of authority may
make the decision to perform
FGM/C on a child.38 In these cases,
theoretically, a parent may also not
know of a child’s previous FGM/C. It
is suggested that a thoughtful,
supportive discussion occur with the
FIGURE 6
Type Ib FGM/C, scarring with excised clitoris and prepuce, or type IV FGM/C with linear scar from primary caregivers to inform them of
superficial cutting with adhesions, Tanner stage 5 female patient. This photo was reviewed by three the diagnosis, associated potential
FGM/C experts (J. Abdulcadir, C.J.A., and J.Y.), and it was unclear if it was type 1b or type IV on the medical issues, and treatment, when
basis of photos. The author of the source of the photo identifies the photo as type IV FGM/C.
(Reprinted with permission from Creighton SM, Dear J, de Campos C, Williams L, Hodes D. Multi-
clinically indicated. Given that such
disciplinary approach to the management of children with female genital mutilation [FGM] or information may be distressing, it is
suspected FGM: service description and case series. BMJ Open. 2016;6[2]:e010311.) advised to offer mental health
Downloaded from www.aappublications.org/news by guest on September 21, 2021
PEDIATRICS Volume 145, number 6, June 2020 7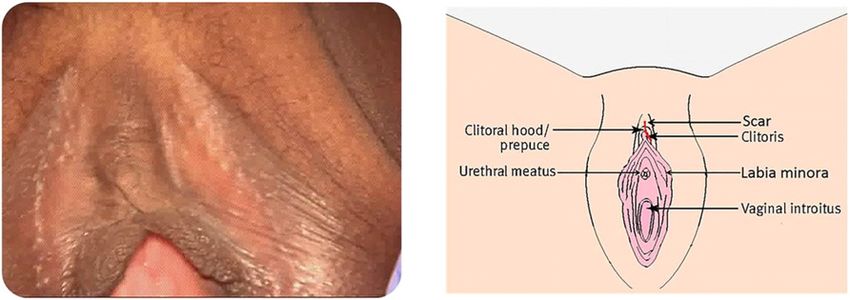
may facilitate timely referral to
gynecologic or urologic specialists, if
needed. However, a recent review of
state-level hospital discharge data in
Arizona revealed that from 2008 to
2014, only 243 cases of FGM/C had
been documented, as identified by
International Classification of
Diseases, Ninth Revision and ICD-10
codes, and that of these 243 cases,
none were documented in children
younger than 18 years (C.J.A,
unpublished observations). As
context, the Population Reference
Bureau estimates that 7459 women
and children are at risk for FGM/C in
Arizona, suggesting that FGM/C is not
being documented consistently by
health care providers.40
FIGURE 7
Type IIa FGM/C, excision of labia minora only, Tanner stage 5 female patient. (Reprinted with permission
from World Health Organization. Copyright © World Health Organization 2016. Also published in COMPLICATIONS AND MANAGEMENT
Abdulcadir J, Catania L, Hindin MJ, Say L, Petignat P, Abdulcadir O. Female genital mutilation: a visual
reference and learning tool for health care professionals. Obstet Gynecol. 2016;128[5]:959.) Immediate Health Complications
Health care providers who work with
professional support to caregivers, as Diseases, 10th Revision (ICD-10) children and live in countries with
indicated. coding,39 as indicated. A guide to intermediate and high prevalence of
ICD-10 coding and definitions and FGM/C are likely to see immediate
descriptions of FGM/C subtypes is health complications; however, such
CODING AND DOCUMENTATION provided in Table 3. In the future, a situation is likely rare in the United
The management of FGM/C should appropriate coding will allow for States.41 Exceptions will be newly
include complete documentation of better estimates of pediatric FGM/C arrived immigrants who underwent
clinical findings and use of the prevalence. Additionally, clinical FGM/C just before entering the
International Classification of documentation of FGM/C findings United States, girls who have recently
returned to the United States after
undergoing FGM/C while temporarily
overseas, or FGM/C that has been
performed in the United States. In
general, medical complications
become more severe with
progression from type I to type III,
tending to reflect the amount of tissue
being removed. If the clitoral dorsal
artery or labial branches of the
pudendal artery are cut, hemorrhage
has been documented in the range of
4% to 19%. Active hemorrhage,
subsequent hypotension,
hypovolemic shock, and death may
occur in these cases.42,43
Given the potential use of traditional
FIGURE 8 nonsterile instruments, girls with
Type IIb FGM/C, partial or total clitoridectomy and excision of labia minora, Tanner stage 5 woman. (Reprinted
FGM/C are at risk for acute infections.
with permission from World Health Organization. Copyright © World Health Organization 2016. Also published
in Abdulcadir J, Catania L, Hindin MJ, Say L, Petignat P, Abdulcadir O. Female genital mutilation: a visual Girls with type III FGM/C most often
reference and learning tool for health care professionals. Obstet Gynecol. 2016;128[5]:959.) have their legs bound for up to
Downloaded from www.aappublications.org/news by guest on September 21, 2021
8 FROM THE AMERICAN ACADEMY OF PEDIATRICS
need to restrain a girl who was not
anesthetized during the procedure42
(Table 5).
If a girl is seen with any immediate
complications, it is recommended that
the health care provider refer for
appropriate emergency care and the
patient receive vaccination against
tetanus. Once stabilized, it is
recommended to consult a health
provider with FGM/C expertise (see
Table 4) to determine the need for
medical and/or surgical management.
Although there are no data that
directly link FGM/C to acquisition of
HIV, hepatitis B, or hepatitis C, some
FIGURE 9
Type IIc FGM/C, partial or total clitoridectomy, excision of the labia minora and majora, Tanner stage clinical experts recommend testing
5 woman. (Reprinted with permission from World Health Organization. Copyright © World Health for these infections at the initial visit
Organization 2016. Also published in Abdulcadir J, Catania L, Hindin MJ, Say L, Petignat P, Abdulcadir and at least 6 months after cutting
O. Female genital mutilation: a visual reference and learning tool for health care professionals.
Obstet Gynecol. 2016;128[5]:959.)
has occurred.44 As in all children, it is
advised that hepatitis B vaccination
be offered to girls with FGM/C if they
1 week after cutting (standard have also been reported. Difficulty
are neither immune nor infected.
practice in type III cases, reportedly urinating, both from pain and
to facilitate scar formation). Such deliberate decreased liquid intake, is In cases in which a girl has been
prolonged binding facilitates bacterial common.41 The urethra, vagina, and/ recently cut, it is recommended to
overgrowth and prevents wound or rectum may also be inadvertently offer mental health supports for her,
healing. Girls may suffer from cut during FGM/C. Fractures of the as indicated. Refer to Reporting Child
cellulitis or wound abscesses; clavicle, femur, or humerus also have Abuse and Ethical Analysis regarding
gangrene, septic shock, and tetanus been reported, resulting from the scenarios in which child abuse
reports are recommended.
Long-Term Complications
Studies reveal that girls and women
with type III FGM/C are also at higher
risk of long-term health complications
than those with type I, II, or IV FGM/
C. A systematic review of the
literature reveals that long-term
health complications include
dysmenorrhea as well as
psychosexual, infertility, and urinary
problems.42 However, physical and
psychological complications are not
necessarily proportionate to the
FGM/C type. Although the authors of
one study state that the relative risk
of obstetric complications (including
increased cesarean delivery rates), of
the need for infant resuscitation, of
FIGURE 10 stillbirths, and of infants with low
Type IIIb FGM/C, with significant narrowing of the introitus from stitching of the labia minora, Tanner birth weight increases with the
stage 5 woman. (Reprinted with permission from World Health Organization. Copyright © World
Health Organization 2016. Also published in Abdulcadir J, Catania L, Hindin MJ, Say L, Petignat P,
severity of FGM/C, data are limited,
Abdulcadir O. Female genital mutilation: a visual reference and learning tool for health care pro- and it is likely that the combination of
fessionals. Obstet Gynecol. 2016;128[5]:961.) obstructed labor and substandard
Downloaded from www.aappublications.org/news by guest on September 21, 2021
PEDIATRICS Volume 145, number 6, June 2020 9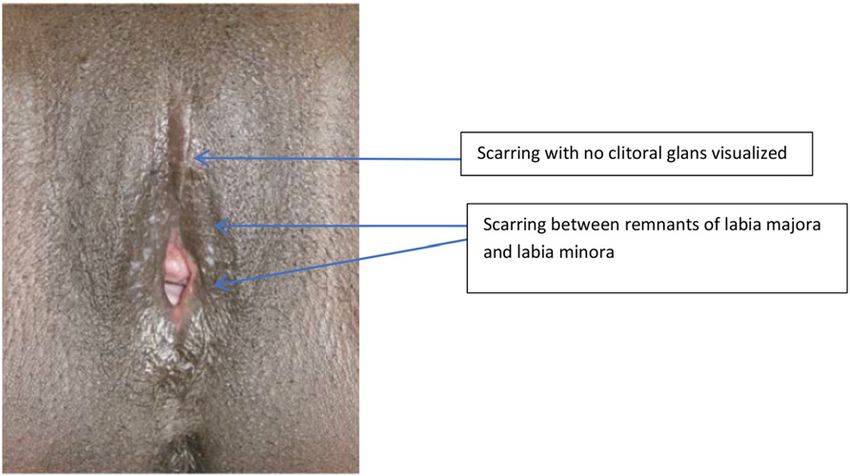
Urinary Issues
The narrow neo-introitus and scar in
type III FGM/C create a dark, moist,
and unventilated area surrounding
the urethra. Urine can stagnate
beneath the scar and promote
abnormal bacterial growth. As
a result, girls who are infibulated can
experience chronic urinary tract
infections. With recurrence of UTI,
suppressive antimicrobial medication
is an option, although defibulation is
preferable; however, currently there
are no known systematic studies
evaluating the efficacy of prophylactic
FIGURE 11
Type IIIb FGM/C in a Tanner stage 5 17-year-old with severe dysmenorrhea preventing her from going antibiotic treatment or defibulation in
to school during menstrual flow (photo courtesy of N.N.). preventing recurrent UTIs associated
with FGM/C.53
health care systems contribute to very rare cases, hematocolpos and In general, clinical experience
such complications (Tables 6 hematometra have been documented. indicates that girls who are
and 7).45 infibulated may describe their
Other painful complications arise urinary stream as being slow and
Secondary analysis of cesarean when remnant foreign bodies are left having a dripping quality. As the urine
delivery rates has revealed that in the scar during the initial exits the urethra, it trickles under the
health care provider unfamiliarity procedure. These can produce sharp scar and then drips past the neo-
with defibulation and/or other pains when sitting and walking. Cut introitus. Patients also may complain
management options for FGM/C may or trapped nerve fibers have also of overactive bladder on the one hand
increase the risk of cesarean been documented, creating very or straining and urinary retention on
deliveries in some cases.46,47 painful neuromas. In both of these the other. These issues may be
situations, defibulation and removal attributable to injury of the
Long-term complications can be
of the foreign body or neuroma are urethra, resulting in urinary
placed into 7 major categories: pain,
recommended.51 strictures and stenosis and
urinary issues, infections, scarring,
requiring cystoscopy or urethral
infertility, sexual dysfunction,42,48 Dyspareunia in sexually active dilation. It is also possible for the
mental health issues,49,50 and other teenagers with type III FGM/C has obstructing scar to enable urinary
(Table 5).
been seen (see Future Infertility) and crystals to deposit and, as a result,
treatment includes defibulation.52 form urinary stones.54 These patients
Pain routinely experience sharp pains and
Pain is a common long-term One study followed 40 Somali women require defibulation for stone
complication after type III FGM/C and whose primary indications for removal.
can also be present in patients with defibulation were pregnancy (30%),
type I and II FGM/C. In type III FGM/ dysmenorrhea (30%), apareunia Scarring and Other Postinflammatory
C, the narrow neo-introitus creates (20%), or dyspareunia (15%). Of the Reactions
a closed environment that can 32 patients surveyed, 94% stated Keloid formation is rare, although not
obstruct urinary and menstrual flow. they would highly recommend unknown in FGM/C cases. The main
Because of the scarring that obstructs defibulation to others; 100% of problem with the infibulated scar is
the introitus, the menstrual flow of patients were pleased with the its obstructive nature. However, other
women and teenagers with results, felt their appearance had complications in type II FGM/C
infibulation can last longer than improved, and were sexually satisfied, include unintended labial fusions and
usual, rendering them unable go to suggesting that the symptoms of cysts (fluid-filled, sebaceous, or
school during this time (see Fig 11). teenagers who have undergone FGM/ inclusion cysts or abscesses). There
Menstruation may be painful and may C and are experiencing dysmenorrhea are multiple case reports
become dark and foul smelling will also be improved by documenting epidermal cysts
because of the retention of blood. In defibulation.52 associated with all types of FGM/C.
Downloaded from www.aappublications.org/news by guest on September 21, 2021
10 FROM THE AMERICAN ACADEMY OF PEDIATRICSOf note, large epidemiologic studies
conducted in low- or middle-income
countries where both FGM/C and HIV
and/or hepatitis B are prevalent have
not revealed an association between
FGM/C and HIV and/or hepatitis B
infections.44,58,59 The authors of these
studies did not evaluate risk around
the time of cutting but months to
years after the cutting occurred. To
our knowledge, no studies have
specifically addressed hepatitis C
infection risks. However, given that
FGM/C is often performed with
unsterile equipment that may be
shared between patients, some
experts recommend testing girls with
FGM/C for these blood-borne
infections.
Future Infertility
Infertility for women with type III
FGM/C is influenced by anatomic and
psychological barriers as well as from
possible recurrent gynecologic
infections. In a Sudanese case-control
hospital-based study of 99 women
without hormonal, iatrogenic, or
male-partner risk factors for
infertility a diagnostic laparoscopy
was performed, and it was found that
FIGURE 12 primary infertility was associated
WHO FGM/C subtype diagrams. A, Female genital mutilation (FGM) type 1. B, FGM type 2. World Health
Organization. Copyright © World Health Organization 2016. Also published in Abdulcadir J, Catania L, with the increased anatomic damage
Hindin MJ, Say L, Petignat P, Abdulcadir O. Female genital mutilation: a visual reference and learning inflicted by FGM/C.60 Repeated
tool for health care professionals. Obstet Gynecol. 2016;128(5):959–960. attempts at penetration through the
infibulated scar may be painful and
Some cysts have been documented to suppositories, this is an alternative difficult, and stretching of the
grow up to 12 cm in size and are not treatment. For girls and teenagers infibulated introitus may take
only extremely painful but also with chronic infections, defibulation months. The learned association
become problematic for ambulation by an adolescent or general between sexuality and pain may
and sitting.55,56 Dissecting the cyst gynecologist experienced with a have significant negative effect on
and defibulating the patient is managing FGM/C is recommended. the woman’s willingness to have
necessary in these cases (see Fig 17). intercourse and, thereby, on fertility.
A study in rural Gambia of teenagers In general, if there are any issues
Other Infections and women (15–54 years) with related to FGM/C that negatively
Given the infibulated scar, this clinically diagnosed type I or II FGM/C affect sexual health, referral to
enclosed environment fosters (N = 671) also revealed a higher appropriate mental health supports is
bacterial and fungal growth and prevalence of bacterial vaginosis and advisable for both women and their
predisposes girls to chronic or herpes simplex virus 2 compared partners.
recurrent vaginal infections. In these with teenagers and women without
cases, oral antifungal and FGM/C but did not reveal an Sexuality
antimicrobial medications are increased risk for perineal or anal There are currently no studies that
recommended. If the patient’s neo- damage, vulvar tumors, dyspareunia, have been specifically focused on
introitus is not too small and she is infertility, organ prolapse, or other sexuality in teenagers with FGM/C.
comfortable with introducing vaginal reproductive tract infections.57 The impact of FGM/C on female
Downloaded from www.aappublications.org/news by guest on September 21, 2021
PEDIATRICS Volume 145, number 6, June 2020 11small cross-sectional study of
Egyptian women and girls (N = 204,
ages 14–19 years), those with and
without FGM/C were compared, and
a significantly higher prevalence of
somatization, depression, and anxiety
was found in those with FGM/C.49
Defibulation
Defibulation, also known as
deinfibulation, is the procedure that
opens the infibulated scar in type III
FGM/C and exposes the vaginal
introitus and urethral opening. In
general, in some regions of the world,
including Djibouti, defibulation is
most often performed in newly
married teenagers by a traditional
birth attendant or midwife so that
sexual intercourse may occur. In other
regions, including North Sudan,
Somalia, and areas in southern Egypt,
the husband opens the neo-introitus
over time through ongoing attempts
at penetration. However, some
teenagers and women who have
access to medical care may have
defibulation performed by a medical
professional at marriage or after their
official engagement.
FIGURE 12 Teenagers who are infibulated may
Continued.
present to health care providers
requesting defibulation. Given the
sexuality has been evaluated in a few date, there are no conclusive results significant morbidity associated with
studies in adult women. However, the revealing long-term benefits. If type III FGM/C, experts believe that
lack of standardization of FGM/C teenagers inquire about the option of defibulation should be recommended
subtype studied and the use of reconstructive surgical repair, it is for all girls and teenagers with type
nonvalidated questionnaires make important to review the fact that III FGM/C, particularly when
interpretation of results difficult. there is still inadequate data that complications are currently present.
Some studies reveal that women with assure successful outcomes, including Similarly, teenagers who are pregnant
FGM/C have reported less sexual a decrease in pain and increased should also be counseled regarding
desire, arousal, orgasms, and sexual pleasure.65,66 risks during and after pregnancy and
satisfaction compared with women should be strongly encouraged to
without FGM/C61 as well as increased
Mental Health
undergo defibulation.
rates of dyspareunia.62 Other There has been limited high-quality
research has revealed no association research on the effects of FGM/C on Of note, given that girls and teenagers
between FGM/C and sexual the mental health of girls and women. who are infibulated have varying
intercourse frequency and that One 2010 systematic review of the degrees of obstruction of urinary or
women with FGM/C also initiated literature included 17 studies of menstrual flow, have varying degrees
sexual intercourse more than women women with and without FGM/C (N = of pain, and/or have risks for normal
without FGM/C.63,64 12 755) and revealed insufficient vaginal delivery, such signs and
evidence to support or refute the link symptoms should underscore the
Surgical clitoral reconstruction is an of FGM/C to specific mental health medical necessity for treatment.
emerging area of study. However, to diagnoses.48 In a more recent 2017 Given the medical necessity of
Downloaded from www.aappublications.org/news by guest on September 21, 2021
12 FROM THE AMERICAN ACADEMY OF PEDIATRICSFIGURE 13
Female genital anatomic structures. Clitoral excision refers to the cutting of the glans (which is the
distal part of the body of the clitoris) or the glans and part of the body. In all cases, part of the
clitoral body remains intact, with scarring overlying the remaining body. The bulbs and crura, two
other sexual erectile structures, have not been noted to be affected in FGM/C cases. Reprinted with
permission from Abdulcadir J, Botsikas D, Bolmont M, et al. Sexual anatomy and function in women
with and without genital mutilation: a cross-sectional study. J Sex Med. 2016;13(2):227–237 and Pauls
RN. Anatomy of the clitoris and the female sexual response. Clin Anat. 2015;28(3):376–384.
treatment in these cases, Medicaid is that there are currently few trained
should cover the defibulation. specialists with experience in
managing FGM/C, particularly in FIGURE 16
In all cases of defibulation, it is young children. Similarly, it may be Clinical approach to external female genital
advised that an experienced pediatric difficult to refer a girl or teenager to examination. (Reprinted with permission from
American Academy of Pediatrics. Visual Di-
gynecologist (for young children), a male provider, and much discussion agnosis of Child Abuse on CD-ROM. 3rd ed. Elk
gynecologist (for older children and and support will need to be provided Grove Village, IL: American Academy of Pediat-
teenagers), urologist, or to facilitate successful care. rics; 2008.)
urogynecologist be identified to Counseling patients who do not want
perform the procedure. One challenge to be defibulated, despite current visits, and it may be necessary to
complications, may be challenging dispel fears of loss of virginity in
given social and cultural pressures. cases of defibulation.67 Mental health
This counseling may take multiple and social issues may arise and need
to be addressed through counseling
and support. Multiple legal and
ethical issues may also arise in cases
in which a teenager desires
defibulation but she does not
want her parents to know because
of fear of stigma and/or refusal by
her parents (see The Law and FGM/C
in Minors in the United States, Ethical
Analysis, and Case 2 in the Appendix
FIGURE 14 for further information).
Normal prepubertal female anatomy. Labia
minora is often less well-developed than pic- For young children who are
tured in prepubertal girls.110 (Reprinted with FIGURE 15
permission from Graham EA. Ritual female Prepubertal female introitus. (Reprinted with defibulated, general anesthesia is
genital cutting [RFGC] PowerPoint slides. 2014. permission from American Academy of Pediat- recommended in all cases.
Available at: https://ethnomed.org/resource/ rics. Visual Diagnosis of Child Abuse on CD-
ritual-female-genital-cutting-rfgc-powerpoint- ROM. 3rd ed. Elk Grove Village, IL: American If a teenager is pregnant, defibulating
slides/. Accessed April 30, 2020.) Academy of Pediatrics; 2008.) her under spinal anesthesia during
Downloaded from www.aappublications.org/news by guest on September 21, 2021
PEDIATRICS Volume 145, number 6, June 2020 13TABLE 4 Resources
Title or Description Source
Care of Girls and Women Living with Female Genital Mutilation: A Clinical Handbook. WHO111
To find a regional FGM/C expert, please go to the US End FGM/C Network Web site https://endfgmnetwork.org/
Female Genital Mutilation/Cutting: Existing Federal Efforts to Increase Awareness Should Be US Government Accountability Office112
Improved
WHO Guidelines on the Management of Health Complications From Female Genital Mutilation WHO113
Eliminating Female Genital Mutilation: An Interagency Statement: OHCHR, UNAIDS, UNDP, UNECA, WHO2
UNESCO, UNFPA, UNHCR, UNIFEM, WHO
Female Genital Mutilation/cutting: A Statistical Overview and Exploration of the Dynamics of United Nations Children’s Fund16
Change
Female Genital Mutilation (FGM) Frequently Asked Questions United Nations Population Fund114
Background information and educational pamphlets in Amharic, Arabic, French, Somali, Swahili, US Citizenship and Immigration Services115
and Tigrinya
Guidelines for the US Domestic Medical Examination for Newly Arriving Refugees Centers for Disease Control and Prevention116
Immigrant Child Health Toolkit American Academy of Pediatrics117
Female Genital Mutilation. A Visual Reference and Learning Tool for Health Care Professionals Abdulcadir et al118; video available at https://www.youtube.
com/watch?v=XRid7jIUzMY
Defibulation: A Visual Reference and Learning Tool Abdulcadir et al68
Female Genital Mutilation/Cutting and Violence Against Women and Girls: Strengthening the Policy United Nations Entity for Gender Equality and the
Linkages Between Different Forms of Violence Empowerment of Women12
Overview: Female Genital Mutilation (FGM) National Health Service119
Female genital mutilation (FGM): Resources for Healthcare Staff National Health Service, Department of Health and Social
Care120
FGM: Mandatory Reporting in Healthcare National Health Service, Department of Health and Social
Care121
Canadian FGM/C statement Canadian Paediatric Society122
Australian FGM/C statement The Royal Australasian College of Physicians123,124
New Zealand FGM/C statement The FGM Education Programme124
the second trimester is advised. In WHO recommends local anesthesia as COMMUNITY ENGAGEMENT
countries where spinal anesthesia best practice, this recommendation is Within the United States, emerging
may not available, local anesthesia not based on strong evidence. Local evidence indicates
may be used, if necessary. This allows anesthesia is not recommended a misunderstanding and distrust
ample time for healing and will (unless in a country where spinal and among immigrant communities with
facilitate providing care during labor. general anesthesia may not be fears of deportation, criminalization,
However, some teenagers may available),68 because women may raids by Immigration and Customs
present late in the third trimester. report flashback memories from the Enforcement, and fear of being
They can still be defibulated up to 34 day when they were cut, as noted in reported to Child Protective Services
weeks’ gestation, which will allow for one case report.69 (CPS).70–74 Some health care and
the neo-vulva to heal adequately social service providers may also not
before labor. Otherwise, defibulating For type III FGM/C, timing and
understand the long-term physical
the patient preferably in the first complications of defibulation have
and mental health-related morbidity
stage of labor or when the baby is not been systematically studied in
associated with the practice of FGM/
crowning are options and are the prepubertal girls. For prepubertal
C.75 In addition, language barriers
routine approaches in some girls with complications, including
may complicate patient-provider
African countries, although these pain, obstruction of urinary stream,
communication and have been
approaches have not been and recurrent urinary tract infections,
demonstrated to negatively affect
systematically studied. Defibulation and teenagers with dysmenorrhea
health-seeking behavior and health
in the first stage of labor does related to FGM/C, it is important that
services use.30,76,77
facilitate pelvic examinations, the health care provider begin
catheterization, and general conversations with the parents and/ A grassroots community-based and
monitoring during labor while also or child regarding the need for community-led approach is essential
allowing for procedures on less defibulation to treat these medical when working with affected
edematous tissues and quicker complications and associated populations to ensure that policies,
delivery. If a teenager is not pregnant, morbidity as well as whether the girl preventive interventions, and
she can be defibulated under regional would benefit from mental health advocacy are all informed by the
or general anesthesia. Although the counseling. perspectives, experiences, and needs
Downloaded from www.aappublications.org/news by guest on September 21, 2021
14 FROM THE AMERICAN ACADEMY OF PEDIATRICSTABLE 5 FGM/C Immediate and Long-Term Complications
Immediate Complications Long-term Complications
Category Description Category Description
41
Bleeding Hemorrhage Urinary Urethral strictures41
Anemia — Meatal obstruction41
Hypotension — Chronic urinary tract infection125
Hypovolemic shock — Pyelonephritis
Death41 — Meatitis
— — Urinary crystals
Infection Cellulitis Infection Chronic yeast infections
Abscess41 — Chronic bacterial vaginitis41
Fever41 — Herpes simplex virus
Pelvic inflammatory disease — Vulvar or periclitoral abscess41
Tetanus — No definitive data on risks for hepatitis B, hepatitis C, or HIV44,126
Gangrene — —
Septic shock — —
Poor healing41 — —
Oliguria Dehydration Scarring Fibrosis41
Urethral injury41 — Keloids41
Urethral edema41 — Partial fusion
Urinary retention41 — Complete fusion
— — Hematocolpos41
— — Inclusion or sebaceous cyst41
Fractures Clavicle Pain Neuromas
Femur — Chronic vaginal infections41
Humerus — Dyspareunia41
— — Vaginismus
— — Dysmenorrhea41
— Infertility Vaginal stenosis
— — Infibulated scar
— — Dyspareunia41
— — Apareunia
— Mental health Anxiety disordersa
— — Depressiona
— — Posttraumatic stress disordera
— — Somatisationa
—, not applicable.
a Large systematic studies are lacking. Some small studies have revealed an association between FGM/C and mental health diagnoses.49
of those directly affected by FGM/C.78 personnel. It is important to assess need to be explored and created. It is
There are varying approaches to whether local efforts already exist recommended that pediatric health
engage FGM/C-affected communities because it will be much easier to care professionals nurture
that need to be culturally and build and/or expand on these meaningful partnerships with FGM/
linguistically tailored on the basis of partnerships. If there are no C-affected communities to foster
availability of local expertise, preexisting relationships, new greater trust, open dialogue,
resources, infrastructure, and community-based partnerships may counseling, education, and
community outreach to enhance
culturally sensitive care for affected
TABLE 6 Obstetric Difficulties in Type III FGM/C populations and to prevent FGM/C
Obstetric Difficulties among female minors. In the past, the
Prolonged labor focus of outreach efforts has
Increased risk of perineal tears or episiotomy principally targeted women, who
Perineal wound infection have been at the forefront of the
Difficult episiotomy repairs perpetuation of FGM/C. However
Postpartum hemorrhage
men, as husbands, fathers, brothers,
Sepsis
Difficulty placing fetal scalp electrode, Foley catheter, or intrauterine pressure catheter sons, community leaders, and
Difficulty performing fetal scalp pH religious figures, also play a critical
Adapted from Nour NM. Female genital cutting: clinical and cultural guidelines. Obstet Gynecol Surv. 2004; role in changing social norms;
59(4):272–279. encouraging greater dialogue with
Downloaded from www.aappublications.org/news by guest on September 21, 2021
PEDIATRICS Volume 145, number 6, June 2020 15You can also read