Electrolyte Disorders - Jai Radhakrishnan, MD
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
Electrolyte Disorders
Jai Radhakrishnan, MD
1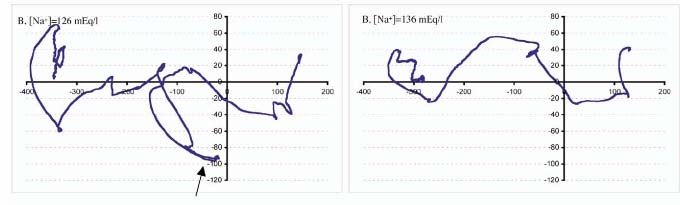
Objectives
Diagnostic and therapeutic principles of
Disorders of osmolarity (Hypo/hypernatremia)
Potassium
Magnesium
2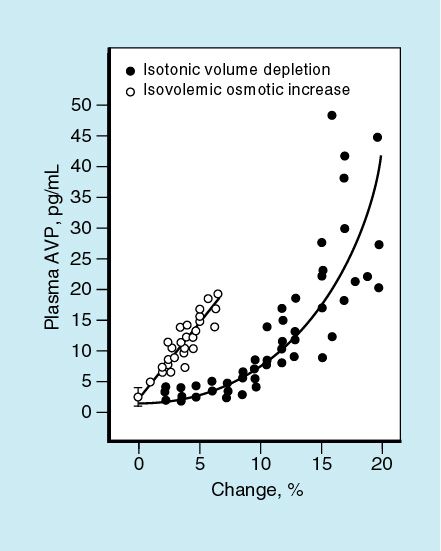
Disorders of Osmolarity
Na Ξ Osmolality
Free Water Intake
Hyperosmolarity (Hypernatremia)
Hypoosmolarity (Hyponatremia)
P. Na
Free Water Loss
3
Generation of Disorders of Osmolarity
Hypernatremia
If water intake is less than
Free Water Intake output
Hyponatremia
If free water intake is
P. Na greater than output
Free Water Loss
4Hyponatremia
Hypo-osmolar
Iso-osmolar
lipid/protein
Hyper-osmolar
Osmotically active subs
5Case
27 year old male alcoholic is admitted with altered mental
status after a recent drinking spree.
P.E.: BP 100/70 HR=130 RR=40
Labs: 116|66|56 109
5.0|15 |2.8
A.G.=35 Ketones=neg
Measured Osm= 350
Calculated Osm=156
Urine= +++ oxalate crystals
6Hyperosmolar Hyponatremia:
Osmolar Gap
Calculate:
2Na + Glucose/18 + BUN/2.8
Measure:
Freezing point depression (lab)
Gap: (Measured)-(Calculated) 10 presence of an osmotic substance that is not
Na, glucose or BUN
7Case: Hyperosmolar Hyponatremia
27 year old male alcoholic is admitted Endogenous:
with altered mental status after a recent
Acetone
drinking spree.
Renal failure
P.E.: BP 100/70 HR=130 RR=40 Lactate
Labs: 116|66|56 109 Exogenous:
5.0|15 |2.8 Methanol
Ethylene Glycol
A.G.=35 Ketones=neg
Ethanol
Measured Osm= 350 Glycine
Calculated Osm=156 Mannitol
Urine= +++ oxalate crystals 8Hypoosmolar Hyponatremia
Increased free water
supply
Free Water Intake
Decreased free water
excretion
P. Na
Free Water Loss
9Hyponatremia:
1. Increased free water supply
Psychogenic polydipsia is the
only situation where this
Free Water Intake
mechanism is solely responsible
Uosm low;"Drink at least eight glasses of water a day." Really?
Is there scientific evidence for "8 × 8"?
Valtin H… Am J Physiol Regul Integr Comp 11
Physiol 283: R993-R1004, 200212 Sumit Kumar & Tomas Berl
Hyponatremia-
2. Impaired free water excretion by kidney
Too few nephrons
Free Water Intake
renal failure
Too much ADH
Volume depletion
Real
P. Na Effective (edema states)
Endocrine
Thyroid
Adrenal
Free Water Loss
INAPPROPRIATE ADH
13Evaluation of Hyponatremia
Iso/hyperosmolar states
Measure plasma osmolarity (calculate osmolar gap)
Check Lipids/proteins
Free Water Intake Psychogenic polydipsia?
Urine OsmCauses of SIADH
z Tumours: bronchogenic carcinoma, lymphoma,
pancreatic cancer, mesothelioma
z Pulmonary: pneumonia, TB, lung abscess, COPD
pneumothorax, HIV infection
z CNS: head injury, meningitis, subdural
haematoma, subarachnoid hge,
neurosurgery
z Drugs: carbamazepine, chlorpropamide,
cyclophosphamide, ‘ecstasy’, NSAID,
tricyclic antidepressants,
phenothiazines, SSRI
15Case
71 year old woman presented with fatigue and
forgetfulness. PMHx: HTN on thiazides.
Physical exam: Systolic BP drop of 20mmHg
Plasma: 119|75| 4 UNa+=13
3.1|29|1.8 Uosm=422
Hyperosmolar?
Psychogenic polydipsia?
Too few nephrons?
Too much ADH?
Volume depletion
Edematous states
Thyroid/Cortisol
SIADH (by exclusion) 16Hyponatremia
Clinical Effects
460
Brain water g/100g dry weight
440
420
400
PNa+=139:
380
Baseline
360
340
320
PNa+=119 in 2h 139 139-119 140-122 139-99
(2h) (3.5d) (16d)
PNa+=122 (3.5 days)
PNa+=140:
PNa+= 99 (16 days)
Day 5
Correction 1718 Sumit Kumar & Tomas Berl
Clinical Course of Treated
Hyponatremia
Arieff A.. NEJM 1986;314(24):1529-35 1920 Am J Med. 2006 Jan;119(1):71.e1-8
Hyponatremia-
Principles of Treatment
Treat vigorously if symptomatic/acute to
reach a “safe” level
If vigorous treatment planned do not increase
PNa+ by >0.5meq/h.
Use frequent monitoring of PNa+ to guide
therapy.
21Treatment Modalities
All forms of hyponatremia will respond to water restriction.
Primary polydipsia
Free Water Intake Renal failure: Dialysis
True Volume depletion: Normal saline
Effective volume depletion: treat cause, loop diuretics.
Thyroid, cortisol: replacement
SIADH
P. Na Asymptomatic/chronic:
Water restrict
Salt tablets, high protein diet
Furosemide in divided doses
ADH Antagonists
Free Water Loss
Acute/Mental status change
Hypertonic saline until M.S. adequate (.5meq/hour)
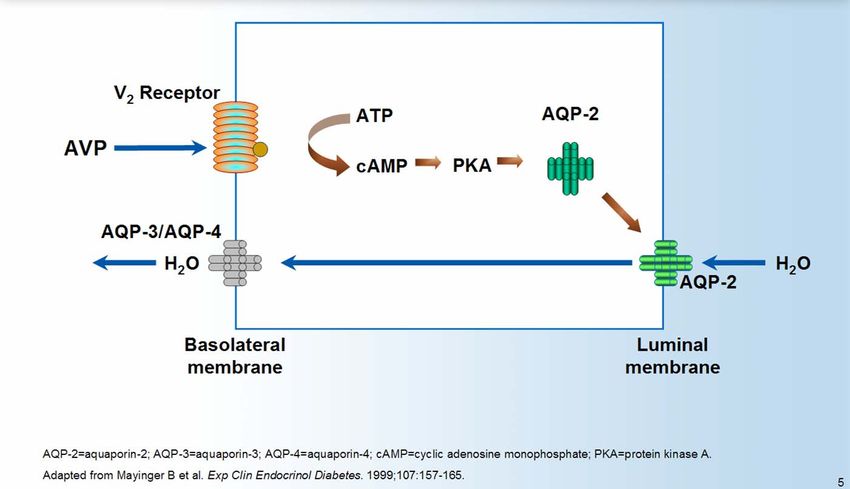
22Arginine Vasopressin
23Tolvaptan (SALT-1 & SALT-2)
24IV Conivaptan 40mg/d in
Hypervolemic Hyponatremia
25Vasopressin v2-receptor blockade with tolvaptan in
patients with chronic heart failure
Circulation. 2003 Jun 3;107(21):2690-6. 26Case
65 year old woman with no PMHx is admitted with
unresponsiveness. Physical exam is normal.
PNa+ = 115, Posm=240, Uosm=700, UNa+=70. Normal sugar/urea.
Hyperosmolar?
Psychogenic polydipsia?
Too few nephrons?
Too much ADH?
Volume depletion
Edematous states
Thyroid/Cortisol
SIADH (by exclusion)
How would you treat this
patient? 27Hypertonic saline-
dose calculation
Current PNa+ = 115 Target PNa+ = 120
Na+deficit = 5 meq/liter
Total body Na+ deficit= 5 x total body water
= 5 x 0.5 x body wt (50kgs)
= 125meq
Amount of 3% NaCl needed (Na=513meq/L) =
125/513= 240ml
Rate of infusion=0.5meq/hour=10 hours
=24ml/hour
28HYPERNATREMIA
29Case
60 year old male with ARDS/intubated/pressors/TPN
PNa= 150. Urine output 150ml/hr. Normal hemodynamics.
Uosm=504 UNa=40meq
Urine dip=2+ glucose
Serum glucose 400.
What is the cause of hypernatremia ?
How would you treat him?
30Pathogenesis of Hypernatremia
Free Water Intake Decreased free water supply
Water loss
Osmotic diuresis, D.I.
Osmotic diarrhea
P. Na
Insensible
Solute load
Free Water Loss
31Workup of Hypernatremia
Why is the patient not drinking??
Is there increased free water loss:
?Polyuria
Uosm: if 300 – solute diuresis
? GI (osmotic diarrhea)
Is the patient getting too much solute?
32Treatment of Hypernatremia Provide free water Oral is optimal Rate of correction
Case
60 year old male with
Why is the patient not drinking??
ARDS/intubated/pressors/TPN Is there increased free water loss:
PNa= 150. Urine output 150ml/hr. ?Polyuria
Uosm: if 300 – solute diuresis
Uosm=504 UNa=40meq ? GI (osmotic diarrhea)
Is the patient getting too much
Urine dip=2+ glucose solute?
Serum glucose 400.
What is the cause of
hypernatremia ?
How would you treat him?
34Calculation of water deficit
Calculate Amount of Water
0.4 x body weight x (PNa/140 – 1)
0.4 x 50 x (150/140 – 1) = 1.4 liters
Insensible losses= + 1 liter/24h
Total volume= 2.4 liters
Rate (0.5meq/hour)
For Na to go from 150->140=20 hours
Prescription: Rate of water repletion
= 2400/20=120ml/hr.
35Hyper- and
Hypokalemia
36Hyperkalemia- Etiology
Intake (never alone)
Shift (Acute)
Acidosis
ICF ECF Insulin lack
Tissue Lysis
Beta blockade
Digitalis o.d.
Succinylcholine
Excretion (Chronic)
Advanced renal failure
Hypoaldosteronism
Volume depletion
37Hyperkalemia: Case
50 year old male with NIDDM/ CRI has been prescribed a low Na
diet for HTN. He presents to the ER with marked weakness.
Labs: 130|98|50 280
8.0 |17| 2.7
Is this pseudohyperkalemia ?
What is causing the hyperkalemia?
How would you treat ?
38Treatment of Hyperkalemia
Antagonism of membrane action
Intravenous calcium
Shift
Insulin (Dextrose)
NaHCO3
ß-2 agonists
Removal
Diuretics
Cation exchange resin
Dialysis
39Hypokalemia- Etiology
Intake (never alone)
Shift
Treatment with insulin
Alkalosis
ICF ECF ß-2 stimulation
Periodic paralysis
Treatment of anemia
Increased Excretion
GI
Renal
Hyperaldosteronism
Diuresis
Ampho-B
Hypomagnesemia
40Hypokalemia-
Clinical Consequences
Cardiac arrhythmias
Muscle weakness
Rhabdomyolysis
Renal dysfunction
Glucose intolerance
41Hypokalemia-Treatment
Estimate of deficit is difficult
~100-200 meq for 1 meq/liter
PO therapy usually adequate
IV therapy if severe/symptomatic
Max conc. 40meq/liter
Max rate 20meq/hour
Use in saline (not dextrose)
42Hypokalemia-case
58 yr old cirrhotic is admitted with worsening ascites
Meds: Lasix 40mg bid, Lactulose
EKG: Unifocal VPC’s, prominent U waves
Admission labs: 125|87|32 80
2.2 |20|2.0
How would you treat her hypokalemia ?
43Disorders of
Magnesium
44Hypomagnesemia:Etiology
Intake
Malnutrition
GI malabsorption
Shift
Pancreatitis
Insulin administration
ICF ECF Post-parathyroidectomy (hungry bone syndrome)
Excretion (Renal)
Post-obstructive, Post ATN
Post-renal transplant
Bartter’s/Gitelman’s syndromes
Drugs: Diuretics, aminoglycosides, cisplatinum,
amphotericin
Alcohol (decreased intake contributing)
45Hypomagnesemia:Clinical Effects
Cardiovascular
Arrhythmia (prolonged QT)
Metabolic
Hypocalcemia
Hypokalemia
Neurological
Tetany
Seizures
46Hypomagnesemia: Treatment
Oral
MgO
Mg-containing antacids
Milk of Magnesia
Mg citrate, sulfate, lactate
Intravenous (avoid IM)
Bolus
Infusion
47Hypermagnesemia:Etiology
INTAKE
Mg-containing
antacids/laxatives
ICF ECF IV magnesium replacement
SHIFT
DKA
Tissue injury
EXCRETION
48Hypermagnesemia:
Clinical Consequences
>4mEq/L
Inhibition of neuromuscular transmission
Inhibition of cardiac conduction
> 7 mEq/L
Lethargy
PR, QT and QRS prolongation
>10mEq/L
Respiratory failure/voluntary muscle paralysis
CHB/Asystole
49Hypermagnesemia
Treatment
IV calcium
Dialysis
50END
51You can also read