FEMALE REPRODUCTIVE PHYSIOLOGY - DR RAELIA LEW CREI, FRANZCOG, PHD, MMED, MBBS FERTILITY SPECIALIST, MELBOURNE IVF - FERTILITY SOCIETY OF AUSTRALIA
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
Female Reproductive Physiology
Dr Raelia Lew
CREI, FRANZCOG, PhD, MMed, MBBS
Fertility Specialist, Melbourne IVF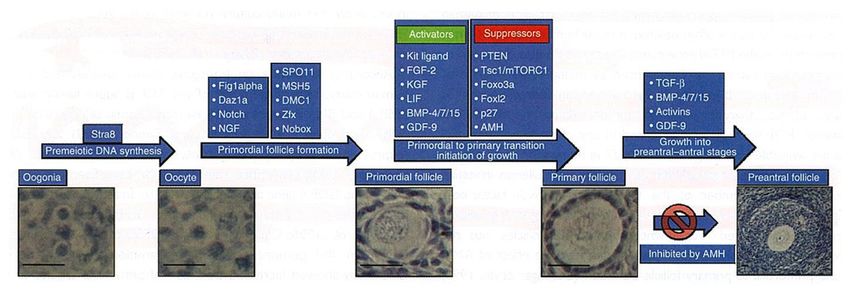
REFERENCE
Lew, R, ‘Natural History of ovarian function
including assessment of ovarian reserve and
premature ovarian failure”
Best Practice & Research Clinical Obstetrics and Gynaecology, July 2018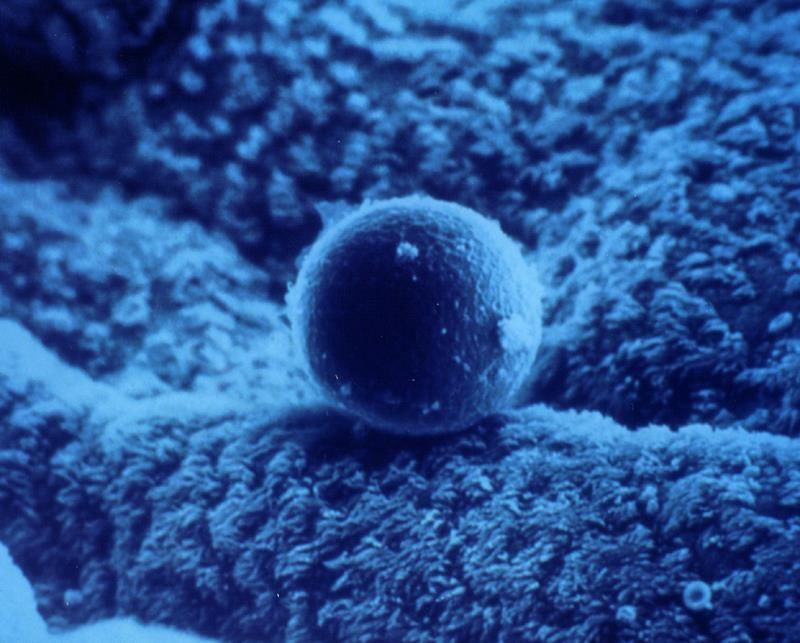
1 in 6 couples are affected by infertility Infertility is a W.H.O. medical condition, it is not a choice!!

Normal Time to Conceive
Advice to couples:
100% Cumulative
Pregnancy Rate Seek advice after 12
(%)
months trying to conceive
80% 11%
Seek advice earlier if:
14%
60% • Maternal age is >35
20% • Known fertility
40% concerns:
• STIs
20% • Anovulation
• Sexual problems
40%
• Endometriosis
0%
• Known male factors
0-3 3-6 6-9 9 - 12
Months or cycles of
treatment
Physical Structures of Female
Reproductive System
Fallopian tube Ovary
Sigmoid colon
Uterus
Bladder
Pubic bone Cervix
Rectum
Anus
Urethra
Vagina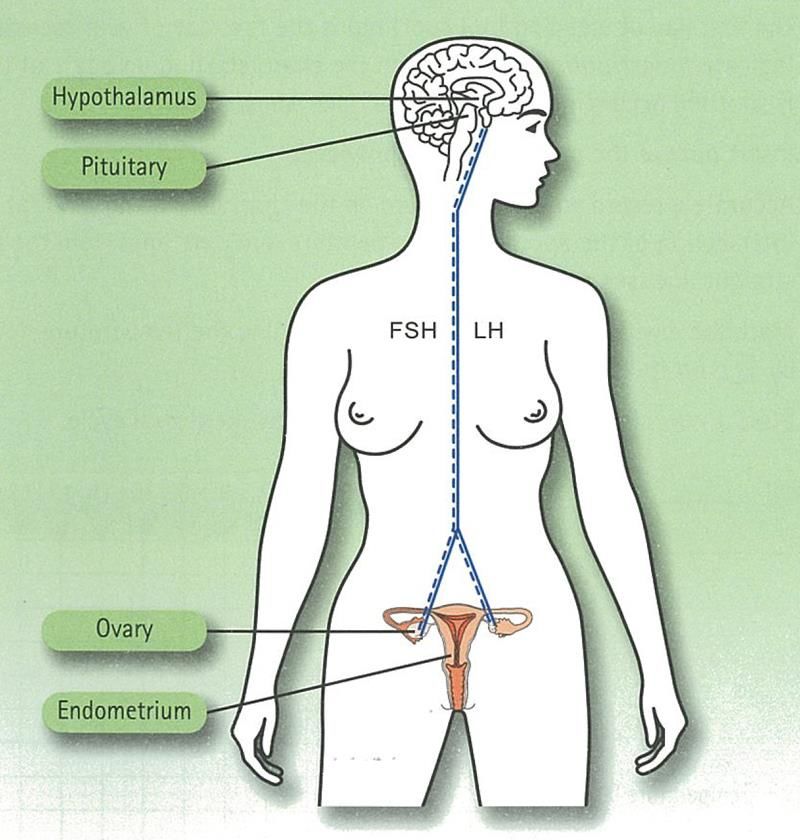
Uterine lining - endometrium
Ovulated oocyte in the oviduct
Sperm swimming through cervical mucous
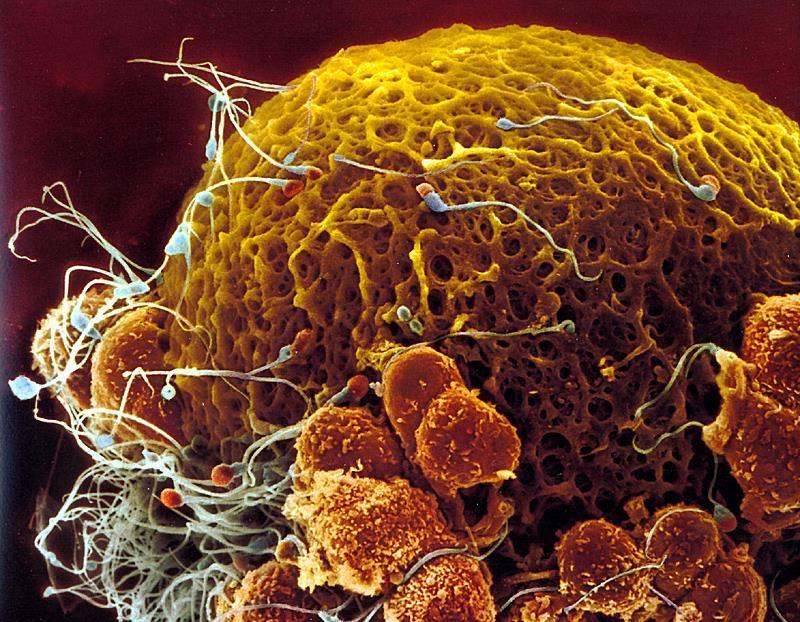
A lot goes on inside an ovarian
follicle as an oocyte matures ……
•To produce a mature
oocyte
•To assist the sperm to
reach the egg
•To prepare and support
the lining of the uterus
• To allow an embryo to
hatch out and implant
•To support the luteal
phase until placental
transition
Fertility & Sterility Cover; July 2009, Vol. 92, No.1.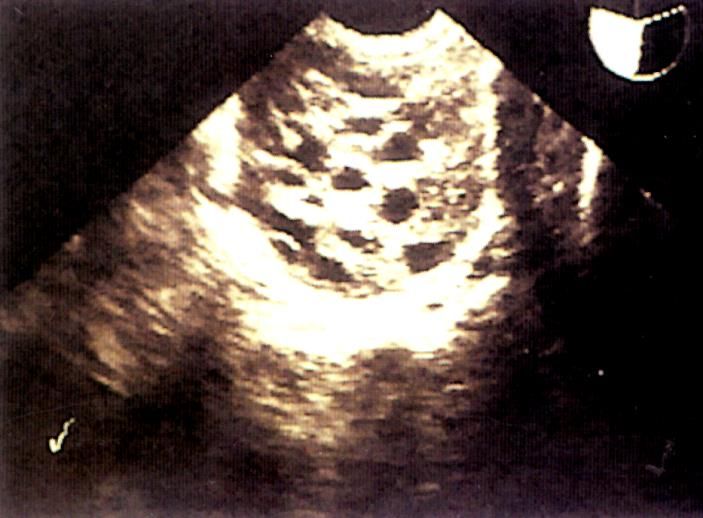
A lot goes on inside an ovarian
follicle as an oocyte matures
……
Achieves this by:
Oogenesis: to produce
female gametes
Secretion of hormones
A pregnancy is
dependent on the
corpus luteum until 8 to
9 weeks gestation
Fertility & Sterility Cover; July 2009, Vol. 92, No.1.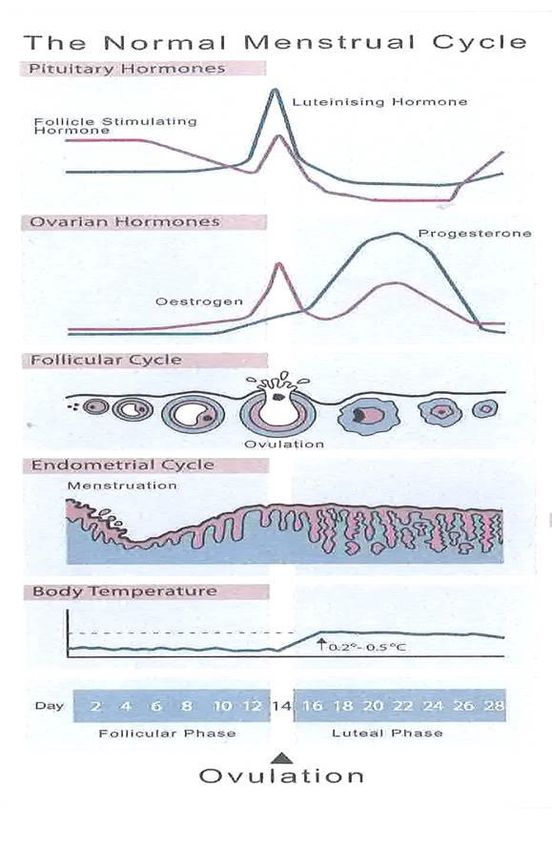
Early Folliculogenesis: the factors involved This process starts between 8 and 13 weeks of gestation
Oocyte Development
At birth: Primary oocytes
Oocytes arrest in prophase I of
meiosis I
• Diploid (46 chromosomes)
After puberty:
Cyclic recruitment
• Text goes here
Developing oocytes complete
meiosis I • Text goes here
• Haploid (23 chromosomes)
• secondary oocyte • Text goes
• Extrusion of 1st polar body • here
Around ovulation: • Text goes here
Meiosis II begins
Metaphase II oocyte
• Text goes here
• Text goes here
Around fertilization:
• Meiosis II completed • Text goes here
• Extrusion of 2nd polar body
The LH surge is critical
for final oocyte maturation
HCG can be used in ARTConnection between the Brain and the Female Reproductive System A feedback system of hormones secreted by the ovary, hypothalamus and pituitary
FSH and LH production in an orderly fashion is key to the development of a mature oocyte that can become a baby
FSH and LH only act in the final weeks of the
development of a mature surviving oocyte
Folliculogenesis occurrs independently of gonadotrophin stimulation
McGee and Hsueh (2000).Antral Follicle
Thecal Cells
Granulosa Cells
Cumulus Cells
Egg - OocyteFSH and LH • Granulosa cells are the only cells in women to possess FSH receptors • Antral formation becomes FSH dependent, when follicles reach about 0.25mm antrim in diameter • Granulosa cells develop LH receptors when the follicle is >11mm in diameter ~ day 8 or 9 of follicular phase • The pre-ovulatory surge of gonadotropins (FSH and LH) is essential to induce the resumption of meiosis
Ovarian
steroidogenesis
is LH dependent
• LH receptors are present in
ovarian theca and
granulosa cells.
antrim
• Theca cells produce
androgens in response to
LH
• FSH induces aromatisation
of androgens to estrogens
in granulosa cells.‘Two cell, two gonadotrophin’ theory
FSH alone is
required for
follicular growth
Some LH is
essential:
• achieves
steroidogenesis
• develops the
capacity of a
follicle to ovulate
and luteinise
• Inhibin B secreted by
granulosa cells in response to
FSH, directly suppresses
pituitary secretion.
• Activin originating in both
pituitary and granulosa,
augments FSH secretion and
action.‘Two cell, two gonadotrophin’ theory
The
maturing
follicle
reduces its
dependence
on FSH by
acquiring LH
receptorsLH Surge >20IU/l required for
Ovulation
• Continuation of meiosis in the oocyte
• Frees oocyte from follicular attachments
• luteinisation of the granulosa synthesis
OVULATION of progesterone
• Progesterone + proteolytic enzymes +
prostaglandins rupture of the follicular
wall
• Early progesterone rise premature
luteinisation adversely affects
E2 LH pregnancy potentialEndocrine Testing Follicular phase: LH and FSH Follicle growth Oestrogen Timing Ovulation LH, Progesterone Luteal phase Progesterone
Maternal Age and Oocyte Numbers A woman has her maximal quota of eggs when her mother is 6 months pregnant
Assessing a
Woman’s Fertility
Potential
Antral follicle count
normal 6 to 12
Antral FollicleAssessing a Woman’s Fertility Potential Early Follicular phase FSH Normal
Assessing a Woman’s treatment options:
Anti Mullerian Hormone
Text goes here …..
Antral
Follicle Anti-mullerian hormone is
secreted by granulosa cellsAnti-Müllerian Hormone (AMH)
Testing in WomenWhat is the role of Anti-Müllerian
Hormone (AMH) in Women?
• Inhibition on follicle recruitment into the antral cohort
• Reduces the sensitivity of growing follicles to FSH.Why test Anti-Müllerian Hormone
(AMH) in Women?
• Simple blood test
• Estimates “ovarian reserve”
• Estimates ART fertility potential
• Predicts response to controlled ovarian hyperstimulationAMH: Pitfalls • Patient and cyclic variation • Assay variation • COCP suppresses • Does not reflect egg quality • Does not influence spontaneous fecundity as a stand alone measure
Anti-Müllerian Hormone Age Relationship
AMH levels pM
100
Probable PCOS
Upper
Median
10 Lower
1
Diminishing Ovarian
Reserve
Guideline only. Statistical analysis on data from Natural Conception Patients
20 25 30 35 40 45 50 Age
Values of AMH below the optimal range indicate a low antral
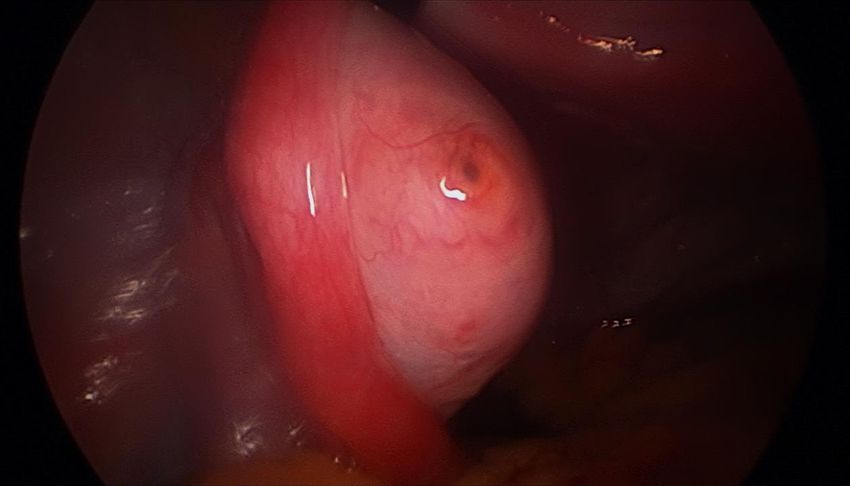
follicle count and therefore reduced reproductive capacity.Very high levels AMH Unilateral pleural effusion What is this??
AMH Usefulness as a Predictor of
Live Birth
• 88 women, aged 25 to 40 years, TTC with AMH levelsTo Conclude … What to Believe • AMH is a useful screening tool for measuring a woman’s ovarian reserve. • AMH testing can be done at any time in the menstrual cycle. However … • AMH it is not an absolute indicator of ovarian reserve, just a guideline. • AMH is not a measure of a woman’s chance of actually conceiving in the immediate future. • Therefore, a woman should never be advised she is unable to have a child or treatment on the basis of an AMH level alone!
Effect of Maternal Age Fertility and
Miscarriage Rates
Fertility Rate Miscarriage Rate
(per 100 women) (percentage)
500 100
Fertility
450 90
As a woman’s age
400 80 increases her fertility
350 70 decreases and her risk
300 60
of miscarriage
increases.
250 50
200 40
150 30
100 20
50 10
Miscarriage
0 0
20-24 25-29 30-34 35-39 40-44 >45
Maternal Age (Years)Effect of Maternal Age on Live Birth Rates
after IVF Using a Woman’s Own Oocytes
Live Births
(percentage)
40
35
30
25
20
15
10
5
0
23 24 25 26 27 28 29 30 31 32 33 34 35 36 37 38 39 40 41 42 43 44 45 46
Woman’s Age (years)A woman is only half the baby… ‘It takes two to tango’ A male factor is present in 50% of infertile couples In 30%, a male factor is the main issue
Time to Conception for a 25 year old
Woman vs. Male Partners Age
Time to Pregnancy
(months)
25
4x longer
20
15
2x longer
10
5
0
40
Hassan et al, F&S 2003, 2006 Male Partner’s Age (Years)
Likelihood of conception following IVF is halved for women
38 to 40 years if their partner is aged 40 years or older.An egg and sperm contribute an equal amount of genetic material to a pregnancy. The placenta is largely dependent on the expression of genes from the paternal chromosomes. Miozzo and Simoni, 2002, Biol. Neonate; 81:217-228
Questions?
Fertilised egg in fallopian tubeYou can also read