Gender-Inequity in Eyecare: Variation by Service Level and Location in North India - Open Journal Systems
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
784 Indian Journal of Public Health Research & Development, July 2020, Vol. 11, No. 7
Gender-Inequity in Eyecare: Variation by Service Level and
Location in North India
Shalinder Sabherwal1, Ishaana Sood2, Gaurav Kumar Garg3, Shantanu DasGupta4, Sathish Nagappan5,
Priya Adhisesha Reddy6, Ken Bassett7
1
Head-Community Ophthalmology, 2Officer-Community Ophthalmology, 3Officer-Community Outreach, 4General
Manager-Community Outreach, 5Manager-Community Outreach, Dr Shroff’s Charity Eye Hospital 5027,
Kedarnath Road, Daryaganj, New Delhi, India, 6Researcher-Centre for Public Health, Queen’s University Belfast,
7Professor-University of British Columbia, Seva Canada, Seva Foundation
Abstract
Background: In the South Asian sub-continent, more than 87% of distance visual impairment is due to
avoidable causes. Women bear a disproportionately large burden of the problem.
Objectives: To perform an eyecare program wide analysis of utilization data, disaggregated by sex, age and
presenting visual acuity, in order to investigate if utilization varied with gender, and if so at what level of
services.
Methods: Retrospective one-year data (July 2016-June 2017), collected as part of a north-Indian eyecare
program was analyzed for sex-based differences. It consisted of rural and urban attendance at vision centers and
camps at primary level, plus walk-in access and cataract operations at rural secondary, and urban tertiary levels.
Results: At primary and secondary levels in rural areas, significantly fewer women than men accessed
vision centers and camps, and received cataract surgery at the secondary hospital, respectively. This trend
was reversed in urban areas, both at primary level, and at tertiary hospital. Cataract surgical patients were
further stratified by pre-operative visual acuity in better eye, and at both levels significantly more women
than men were blind at time of surgery.
Conclusions: Service utilization by women varies significantly and unpredictably within a single eyecare
program. Collection and analysis of sex-disaggregated data is needed at all locations and levels of care, to
determine inequity and plan interventions.
Keywords: Cataract; Primary; Rural; Secondary; Tertiary; Urban
Introduction is particularly pronounced in India,6 and other low and
middle-income countries.7
Women access formal healthcare less frequently,1
and at much later stages than men, for most conditions. Universal eye health cannot be achieved without
A rural south Indian study showed similar delays in substantial investment in primary and secondary level
accessing services for eye conditions, with 89% of services. Over the past decade, our organization has
women not accessing treatment, despite noticing poor invested heavily in developing a system consisting of a
vision, as compared to 29% of men.2 tertiary hospital, secondary hospitals and vision centers
(VCs,) as well as in conducting transient screening
Women have been shown to bear a disproportionately
camps. In last five years, number of people screened at
larger share of global visual impairment (VI)3 and
primary level through rural camps and VCs, increased
blindness.3-4 Almost two-thirds of people blind from
from 35,008 to 92,080 per year, and patients examined
cataract are women and yet cataract surgical coverage
at secondary hospitals increased from 45,838 to 94,966
(CSC) is higher in men.5 This gender-inequity in CSC
per year. In same time period, surgeries performed at all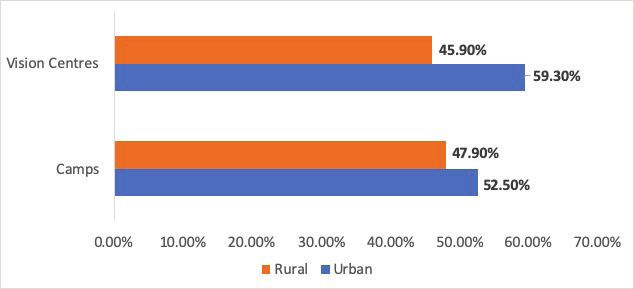
Indian Journal of Public Health Research & Development, July 2020, Vol. 11, No. 7 785
secondary hospitals increased from 4,947 to 13,751 per public transport.
year.
Tertiary facility is located in Delhi and provides all
Factors reportedly influencing service uptake sub-specialty services, as well as training and research
by women are lack of awareness, distance, cost, activities. For hospitals, sex-specific data was extracted
ease of access and dependence on an escort.8 While from routine administrative software, the Integrated
many programs report overall gender-inequity, few Hospital Management System (IHMS). Participants
publications examine gender-inequity at different levels were selected using the gender code identified through
of an established eyecare program. camp reports, VCMS and IHMS .
The purpose of this study was to perform a program Comparisons were made between proportions of
wide analysis of utilization data, disaggregated by male and female patients at all ages, over the age of 50
sex, age and presenting visual acuity (VA), in order to years (where most eye diseases are concentrated), and
investigate if utilization varied with gender and if so at at each level and location of care. Comparisons were
what level of services. This would also have practical also made on proportions of male and female patients
implications for design of future service-based programs undergoing cataract surgery with blindness (Snellen
for eyecare, in similar regions. VA of less than 3/60 in better eye).10 This was used as a
proxy indicator for delay in accessing services.
Method
Data were analyzed using R software version 3.1.1
Retrospective cross-sectional study of sex-specific
and Excel 2013. Proportions were compared using Z-test,
service utilization data collected between July 2016 and
and p-value of less than 0.05 was considered statistically
June 2017, at different levels of an eyecare system, of a
significant. The study adheres to the recommendations
north Indian community-based organization.
made in the Declaration of Helsinki.
Primary eyecare in the system includes outreach
Results
camps (camps) and VCs, in both urban and rural settings.
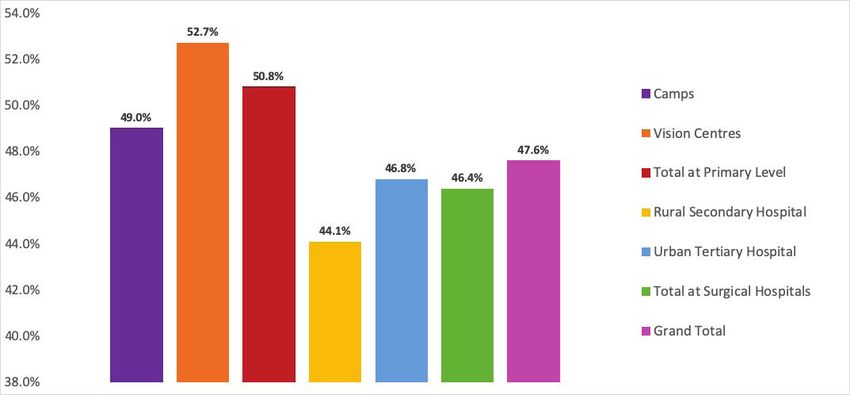
Camps are scheduled activities in community where More women than men attended VCs, but fewer
patients are screened and provided with glasses. Patients attended camps. Overall, outpatient service utilization
requiring surgery are transported to the nearest surgical by women at primary level (both VCs and camps) was
secondary or tertiary hospital for free. Sex-specific camp 50.8% (39,235 of 77,236 total patients examined) and
data was extracted from camp reports prepared after hospital outpatient service utilization (both secondary
each camp. and tertiary level) by women was 46.4% (94,607 of
203,824 patients) (Figure 1).
VCs9 are permanent facilities that provide primary
level eyecare to a population of around 50,000 people. In rural areas, significantly fewer women than men
They are based in rural10 areas at the block headquarters’ accessed outreach camps (14,327 of total 29,933; 47.9%
level and in urban slums, making them accessible by [95% CI:47.3%-48.4%; p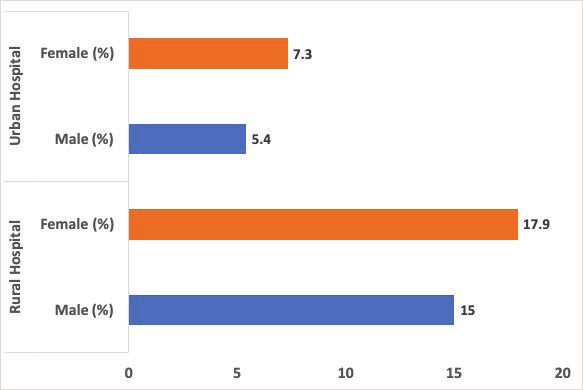
786 Indian Journal of Public Health Research & Development, July 2020, Vol. 11, No. 7
At rural secondary hospital, significantly fewer In rural hospital, significantly fewer women than
women than men were paying walk-in patients (13,844 men underwent cataract surgery (1,975 out of 4,350;
of 31,353; 44.1% [95% CI:43.6%-44.7%; pIndian Journal of Public Health Research & Development, July 2020, Vol. 11, No. 7 787
Figure 3: Percentage of men and women operated at urban tertiary and rural secondary hospitals (Column Width), belonging
to blind category. [Original]
Discussion 5% less able to get a maternal tetanus vaccination than
women in urban areas.11
In the past decade, our organization has substantially
increased footfall of people treated through its’ eyecare Several studies report similar gender-inequity in
program and has improved access for marginalized rural eyecare services. A study in rural south India, from
people in urban slums and rural areas. 1999, showed that men were twice as likely as women
to attend eye camps.12 A Nigerian study showed that
Analysis of overall service utilization at primary
men were more likely to access primary eyecare than
level (camps and VCs) in both urban and rural settings of
women13 while a Ghanaian study reported that a lower
the organizational network showed equity for outpatient
proportion of women than men had ever had their eyes
visits by sex (50.8% women). Similarly, cataract
examined at any level of care.14
operations performed at urban and rural hospitals
combined showed equity (49.8% women). However, Organization provisioned services are standard pan-
disaggregation by location showed that, in rural primary system. Both urban and rural camps provide all services
level camps and VCs, a significantly lower proportion free of cost, while VCs charge only a minimal fee of
of women than men were served. In addition, in rural around Indian Rupees 30 for an examination. Thus, in
secondary hospital significantly fewer women than men this context, barriers other than cost and services become
above the age of 50 years attended, and significantly relevant.
fewer women than men were operated for cataract.
Outreach camps and VCs are two very different
Lower utilization of services by women in rural areas models of primary eyecare service delivery. VCs are
is seen for a range of health conditions. Women from fixed facilities providing flexible times for access, while
rural areas in India are 31% less able to access antenatal camps deliver transient services at a pre-decided date
care, 53% less able to have an institutional delivery and and time. In our study, proportion of women attending788 Indian Journal of Public Health Research & Development, July 2020, Vol. 11, No. 7
was greater in VCs than camps, presumably due to in rural hospital, and will require additional focus for
flexible hours offered. A similar trend has been reported future interventions, to increase CSC for women.
almost a decade earlier from a high-volume rural Indian
Pre-operative VA in the better eye was used as a
eyecare institute.15
measure of delay in uptake of surgery. In both the rural
Distance from hospital, loss in wages, transportation secondary and urban tertiary hospital, a higher proportion
and cost2 are oft cited barriers to utilization in eyecare. of operated women than men had blindness, indicating
Our network employed strategies to overcome these later presentation of women. This is consistent with
barriers of distance and cost, including mobile cataract related blindness being higher amongst women
campaigns,16 to distant rural communities and no-cost than men in a national survey.24 Delay in seeking
VCs for people too poor to pay. However, in rural surgery needs to be targeted in both the rural and urban
households, women’s total workload is much higher than settings in our context as later presentation by women
that of men, including farm activities over and above was associated with poorer outcome after surgery, as
domestic work, further constraining time for personal reported in RAAB from many countries.25
chores.17 In rural areas served by our network, female
A limitation of our study would be its’ basis in
and male literacy was 57% and 77% respectively, with
retrospective data sourced from a single service provider.
83% women and 52% men not employed in organized
As data were extracted from software, we don’t expect
sectors.18 Lack of autonomy and low literacy have been
any observer bias Data from more service providers
shown to negatively influence health-seeking behavior
needs to be collated if regional, sex-specific service
in a neighboring Indian state.19
utilization trends are to be observed, to enable planning
Considerable research has examined the cost- of interventions.
effectiveness of different strategies increasing uptake
of eyecare services by women. Systematic review of Conclusions
randomized controlled trials undertaken in Bangladesh, Our results show that while the provision of primary
India, Malawi, and Nepal recommended women’s and secondary level of services in rural areas reduces
groups practicing participatory learning and action as overall population-level inequity, it doesn’t ensure
a cost-effective strategy in low-resource settings.20 A gender-equity. Our study highlights the importance of
similar study from 2018 has recommended sensitizing in-depth, system wide, analysis of sex-specific utilization
family members, community mobilization, and data by service providers as a first step for ensuring
capacity building of frontline health functionaries. It gender equity. Prospective studies to understand
also highlighted that community-based interventions reasons for inequity in uptake of services at different
by eyecare personnel may be required to improve level of eyecare delivery within a network and relevant
awareness regarding access to care in rural areas.21 interventions are recommended as next steps.
Lower utilization of cataract services by women in Ethical Clearance: Taken from Institutional
our study’s rural hospital is similar to multiple meta- Review Board of Dr Shroff’s Charity Eye Hospital
analyses from studies around the world.22 In a rapid (IRB/2018/MAY/17).
assessment of avoidable blindness (RAAB) conducted
in rural setting in the same state as the secondary References
hospital, CSC at vision less than 3/60, was found to be 1. Shaikh BT, Hatcher J. Health seeking
lower among women. In contrast, RAAB carried out in behaviour and health service utilization in
an urban location in the same state showed similar CSC Pakistan: challenging the policy makers.
amongst men and women.23 J Public Health (Oxf). 2005;27(1):49-54.
The highest proportion of cataract, and cataract
related blindness and VI is in patients over 50 years of 2. Kovai V, Krishnaiah S, Shamanna BR, Thomas R,
Rao GN. Barriers to accessing eye care services
age.3 Among the walk-in patients over the age of 50
among visually impaired populations in rural
years, there were more women. This trend was reversedIndian Journal of Public Health Research & Development, July 2020, Vol. 11, No. 7 789
Andhra Pradesh, South India. Indian J Ophthalmol. care services in a rural adult population of a
2007;55(5):365-371. developing country. Middle East Afr J Ophthalmol.
3. Flaxman SR, Bourne RRA, Resnikoff S, et al. Global 2016;23(1):96-103.
causes of blindness and distance vision impairment 14. Ocansey S, Kumi-Kyereme A, Awusabo-Asare
1990-2020: a systematic review and meta-analysis. K, Ilechie AA, Boadi-Kusi SB, Abraham CH.
Lancet Glob Health. 2017;5(12):e1221-e1234. Utilization of eye care services among Ghanaian
4. Abou-Gareeb I, Lewallen S, Bassett K, elderly population: Evidence from a peri-urban
Courtright P. Gender and blindness: a meta- community. Ophthalmol Research. 2013;1(2):89-
analysis of population-based prevalence surveys. 101.
Ophthalmic Epidemiol. 2001;8(1):39-56. 15. Sudhan KA, Jain PK, Pandey KP, Singh V. Gender
5. Lewallen S, Courtright P. Gender and use of and eyecare services in central India. Community
cataract surgical services in developing countries. Eye Health. 2009;22(70):s123-s126.
Bull World Health Organ. 2002;80(4):300-303. 16. Ellwein LB, Lepkowski JM, Thulasiraj RD,
6. Patil S, Gogate P, Vora S, et al. Prevalence, causes Brilliant GE, Group TOR. The cost effectiveness of
of blindness, visual impairment and cataract strategies to reduce barriers to cataract surgery. Int
surgical services in Sindhudurg district on the Ophthalmol. 1991;15(3):175-183.
western coastal strip of India. Indian J Ophthalmol. 17. Baliyan K. Unequal sharing of domestic work: A
2014;62(2):240-245. time use study of farm households in western Uttar
7. Lewallen S, Mousa A, Bassett K, Courtright Pradesh. Indian J Gend Stud. 2017;24(3):341-359.
P. Cataract surgical coverage remains lower in 18. Office of the Registrar General & Census
women. Br J Ophthalmol. 2009;93(3):295-298. Commissioner India. [Internet] Primary Census
Abstract. http://censusindia.gov.in/pca/. Accessed
8. Marmamula S, Khanna RC, Shekhar K, Rao GN. A
August 21, 2019.
population-based cross-sectional study of barriers
to uptake of eye care services in South India: the 19. Pandey KK, Singh RD. Womens status, household
structure and the utilization of maternal health
Rapid Assessment of Visual Impairment (RAVI)
services in Haryana. J Stat Appl Pro Lett.
project. BMJ Open. 2014;4(6):e005125-e005125.
2017;1(4):1-10.
9. Rao GN, Khanna RC, Athota SM, Rajshekar
20. Prost A, Colbourn T, Seward N, et al. Women’s
V, Rani PK. Integrated model of primary and
groups practising participatory learning and action
secondary eye care for underserved rural areas:
to improve maternal and newborn health in low-
The L V Prasad Eye Institute experience. Indian J
resource settings: a systematic review and meta-
Ophthalmol. 2012;60(5):396-400.
analysis. Lancet. 2013;381(9879):1736-1746.
10. World Health Organization. [Internet] Blindness
21. Reddy PA, Kishiki EA, Thapa HB, Demers L,
and vision impairment. https://www.who.int/news-
Geneau R, Bassett K. Interventions to improve
room/fact-sheets/detail/blindness-and-visual-
utilization of cataract surgical services by girls:
impairment. Accessed February 14, 2019.
Case studies from Asia and Africa. Ophthalmic
11. Namasivayam A, Osuorah DC, Syed R, Antai D. Epidemiol. 2018;25(3):199-206.
The role of gender inequities in women’s access to
22. Ramke J, Zwi AB, Palagyi A, Blignault I, Gilbert
reproductive health care: a population-level study
CE. Equity and blindness: Closing evidence gaps
of Namibia, Kenya, Nepal, and India. Int J Womens
to support Universal Eye Health. Ophthalmic
Health. 2012;4:351-364.
Epidemiol. 2015;22(5):297-307.
12. Fletcher AE, Donoghue M, Devavaram J, et al.
23. RAAB Repository. [Internet] http://raabdata.
Low uptake of eye services in rural India: A
info/repository. Accessed January, 10th 2019.
challenge for programs of blindness prevention.
JAMA Ophthalmol. 1999;117(10):1393-1399.
24. Pant HB, Bandyopadhyay S, John N, Chandran A,
13. Olusanya B, Ashaye A, Owoaje E, Baiyeroju
Gudlavalleti MVS. Differential cataract blindness
A, Ajayi, B. Determinants of utilization of eye790 Indian Journal of Public Health Research & Development, July 2020, Vol. 11, No. 7
by sex in India: Evidence from two large national An indicator for measuring quality-of-care in the
surveys. Indian J Ophthalmol. 2017;65(2):160-164. context of Universal Health Coverage. PloS One.
25. Ramke J, Gilbert CE, Lee AC, Ackland P, Limburg 2017;12(3):e0172342.
H, Foster A. Effective cataract surgical coverage:You can also read