Gynaecology & Obstetrics - Italian Journal of (SIGO) The Official Journal of the Società Italiana di Ginecologia e Ostetricia
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below

Italian Journal
of
Gynaecology
& Obstetrics
The Official Journal of the
Società Italiana di Ginecologia e Ostetricia
(SIGO)
September 2016 - Vol. 28 - N. 4 - Quarterly - ISSN 2385 - 0868
Quarterly
Partner-Graf 1

Italian Journal
of
Gynaecology
& Obstetrics
The Official Journal of the
Società Italiana di Ginecologia e Ostetricia
(SIGO)
Quarterly
Partner-Graf
Editor in Chief Paolo Scollo, Catania Editors Herbert Valensise, Roma Enrico Vizza, Roma Editorial Board Cervigni Mauro, Roma Chiantera Vito, Napoli Costa Mauro, Genova De Stefano Cristofaro, Avellino De Vita Davide, Salerno La Sala Giovanni Battista, Reggio Emilia Locci Maria Vittoria, Napoli Marci Roberto, Roma Monni Giovanni, Cagliari Ragusa Antonio Franco, Milano Sirimarco Fabio, Napoli Trojano Vito, Bari Viora Elsa, Torino Editorial Staff Roberto Zerbinati Serena Zerbinati Management, Administrative office Partner-Graf Srl - Via F. Ferrucci, 73 - 59100 Prato Tel 0574 527949 - Fax 0574 636250 E-mail: info@partnergraf.it The Italian Journal of Gynaecology & Obstetrics is a digital magazine. You can download it freely from www.italianjournalofgynaecologyandobstetrics.com or www.italianjog.com

It. J. Gynaecol. Obstet.
2016, 28: N.2
Table of contents 5
Editorial 6
Benign Peritoneal Melanosis associated with atypical leiomyom 7
Madhuri Alwani, Ishan Shrivastava, Amit Varma, Ratna Thakur
Intrauterine transfusion versus Corticosteroids for treatment of immune fetal 11
hydrops secondary to Rh incompatibility with 6 months postnatal follow-up:
Case series with review of literature
Tamer Mamdouh Abdeldayem, ElSayed El Badawy Mohamed, Ahmed El Habashy, Sherif Gaafar,
Ashraf Han, Aly Alaa Youssef
Improving prescription of physical exercise in prophylaxis/therapy of 15
gestational diabetes: a survey from evidence to current recommendation
Cristina Bianchi, Michele Aragona, Alessandra Bertolotto, Pietro Bottone, Maria Calabrese, Ilaria
Cuccuru, Alessandra De Bellis, Anna Leopardi, Cristina Lencioni, Roberto Miccoli, Mary Liana
Mori, Serena Ottanelli, Matilde Romano, Gigliola Sabbatini, Maria Giovanna Salerno, Giuseppe
Trojano, Stefano Del Prato, Lorella Battini
Aggressive late Sezary syndrome with pregnancy: A case presented with 23
generalized erythroderma and dyspnea
Ahmed Samy El-Agwany
One Case of Severe Preeclampsia Who Died from Postpartum Complications Ten 31
Days after Caesarian Delivery
Myrvete Pacarada, Astrit M. Gashi, Albiona Beha, Bujar Obertinca
Polyglandular Autoimmune Syndrome in pregnancy: case report. 35
Basilio Pecorino, Maria Cristina Teodoro, Paolo Scollo
Centiles of weight of spontaneous and medically induced preterm births 41
in Lombardy
Fabio Parazzini, Sonia Cipriani, Stefania Noli, Ilaria Baini, Paola Agnesi Mauri, Mauro Busacca,
Michele Vignali, Giuseppe Trojano
5
It. J. Gynaecol. Obstet.
2016, 28: N. 4 Editorial
Dear Friends,
Dear SIGO members,
in the last two year, since september 2014 to september 2016, Italian Journal of Obstertrics &
Gynaecology has been renewed and became an on-line magazine. Since then, 53 original articles were
published, reviews and case reports has been published. Two issues on 2014, four on 2015 and five on
2016. The site of the Italian Journal of Obstertrics & Gynaecology counted 16200 users, 18.550 sessions,
24.000 views. 72% of the users were italian, 10% from Europe and Asia, 7% from USA.
The present data clearly shows the growth of Italian Journal during the last years and how much is
changed trasforming from a national magazine to an international one.
Therefore, I would like to thank all the Italian Journal staff member and the editorial board for the
results achieved.
During the next National SIGO Congress that will be helded in Rome, a new council board of SIGO
will be elected and I ma sure that new projects will be done in order to improve our Journal.
Prof. Paolo Scollo
S.I.G.O. President
6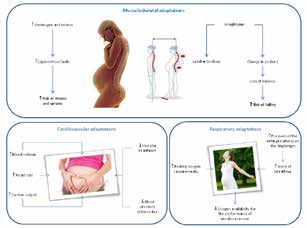
Italian Journal of
Gynaecology & Obstetrics
September 2016 - Vol. 28 - N. 4 - Quarterly - ISSN 2385 - 0868
Benign Peritoneal Melanosis associated with atypical leiomyoma
Madhuri Alwani1, Ishan Shrivastava1, Amit Varma2, Ratna Thakur1
1
Department of Obstetrics and Gynaecology, Sri Aurobindo Medical College and PG Institute, Indore
Ujjain Highway, Indore, Madhya Pradesh, India
2
Department of Pathology, Sri Aurobindo Medical College and PG Institute, Indore Ujjain Highway,
Indore, Madhya Pradesh, India
ABSTRACT SOMMARIO
Benign Peritoneal Melanosis is an extremely rare La Melanosi Peritoneale Benigna è una condizione
condition with only a handful cases in the literature. It estremamente rara con pochi casi riportati in letteratura.
is characterized by melanin pigment deposition in the È caratterizzata da deposizione di melanina nel
peritoneum. The pathogenesis of Peritoneal Melanosis peritoneo. La patogenesi della melanosi peritoneale
in particular, the origin of the pigment producing cells, ed in particolare, l’origine della produzione delle
is unclear. We describe a case of Benign Peritoneal cellule pigmentate, è non-chiara. In questo articolo
Melanosis associated with atypical leiomyomya of the descriviamo un caso di melanosi peritoneale benigna
uterus in a 40 year old woman. She presented with associata a leiomyomya uterino atipico in una donna
increased blood loss during menses and recurrent di 40 anni La paziente ha presentato un aumento
pain in abdomen since last 3 years. On USG Pelvis, della perdita di sangue durante le mestruazioni e
she was diagnosed as a case of fibroid uterus and was dolore ricorrente addominale negli ultimi 3 anni. Con
posted for hysterectomy. During surgical procedure, USG della Pelvi, è stata diagnosticata come un caso
India ink colored (Black) pigmentation was seen in the di fibroma dell’utero ed è stata eseguita l’isterectomia.
peritoneum and the complete lining peritoneum of the Durante la procedura chirurgica, con la colorazione di
pelvis was seen black. Only the body of the uterus, the inchiostro di china (nero) il peritoneo e il rivestimento
fallopian tubes and ovaries were spared. Biopsies of the del bacino è diventato nero. Solo il corpo dell’utero, le
peritoneum showed pigment in the stroma and pigment tube di Falloppio e le ovaie sono stati risparmiati. Le
laden histiocytic aggregation and ultra structural study biopsie del peritoneo hanno mostrato pigmentazione
found melanosomes in the cytoplasm of histiocytes. dello stroma e aggregazione istiocitaria pigmentata e
lo studio ultra-strutturale ha trovato melanosomi nel
Keywords: Benign Peritoneal Melanosis, Hysterectomy, citoplasma degli istiociti.
Melanosomes
INTRODUCTION CASE REPORT
Benign Peritoneal Melanosis, a diffuse black A 40 yr old female para 4 living 4, all full term
pigmentation of peritoneum, is a condition normal vaginal deliveries came to the OPD with
characterized by melanin pigment deposition chief complaints of increased blood loss during
in the peritoneum, mesentry, appendix surface, menses since last 1 year and pain in lower abdomen
pelvic peritoneum and surface of ovary [Kim et al and backache since 1 year. Her LMP was 20 days
2002, Jaworski 2003]. It is of unknown origin and back and during her present cycles she had a
it is an extremely rare condition with only handful heavy flow of menstrual blood for 6 to 7 days with
of cases in the literature. an interval of every 30 days. This was since last one
year. Previous cycles were regular with average
blood loss. She was married for 19 years and was
using barrier method of contraception. Her last
child birth was 15 years. There was no history of
any surgery in the past and no relevant medical
Correspondence to: drmadhuri_2007@rediffmail.com history. On general examination, all parameters
Copyright 2015, Partner-Graf srl, Prato were within normal limits. Per abdomen nothing
DOI: 10.14660/2385-0868-47 abnormal was found. Cervix and vagina appeared 7
It. J. Gynaecol. Obstet. Benign Peritoneal Melanosis associated with atypical leiomyoma
2016, 28: N. 4
healthy; Pap smear was taken which was reported
as inflammatory. On p/v examination cervix was
downwards backwards, uterus anteverted, 6-8
weeks in size and firm in consistency. Both fornices
were free. USG pelvis showed a submucosal to
intramural fibroid in anterior wall of the body of
uterus measuring 5.2 X 6.0 cms. Pap smear was
inflammatory. OT profile was done and decision
of hysterectomy was taken in view of symptomatic
fibroid uterus.
On opening the abdomen, when we reached
the peritoneum, we could see dark picture
through the peritoneum as if there was collection
of clotted blood. That gave us the suspicion of
ruptured chronic ectopic pregnancy or ruptured
hemorrhagic ovarian cyst that we might have Figure 1.
missed. After opening the parietal peritoneum Surgical Picture of abdomen showing black colored
peritoneum(A&B),Hematoxylin and Eosins(10X) showing fibro
we could see complete dark black peritoneum adipose tissue with brown black colored melanin pigment(C)
covering the inner lining of pelvis. Body of the Hematoxylin and Eosins(40X) stained section of peritoneal biopsy
uterus, ovaries, fallopian tubes were spared uptil revealed fibrous connective tissue with deposition of brown black
uterovesical fold anteriorly and posteriorly till colored pigment in the peritoneum. The pigment stained positive
with Masson Fontana stain and negative with Perls stain proving
rectovaginal fold of peritoneum. Biopsy was taken the pigment to be Melanin (D).
from peritoneum and subtotal hysterectomy with
bilateral salpingo ophrectomy was done. Decision
of subtotal hysterectomy was taken as there was
dark pigmentation below the utero vesical fold of
peritoneum (shown in Figure 1). Bilateral salpingo DISCUSSION
ophrectomy was also considered keeping in view Peritoneal melanosis, a diffuse black
of again any pathology developing in ovaries in pigmentation of peritoneum is a very rare
future for which laparotomy may be required, condition characterized by melanin pigment
as this operative finding was a very rare and deposition in the peritoneum, mesentery, appendix
unknown entity. Laparotomy was performed over surface, pelvic peritoneum and surface of ovary. It
laparoscopy because patient was not affording is an extremely rare condition with only handful
for laparoscopy and she wanted abdominal of cases in the literature. Benign peritoneal
hysterectomy. A sample of peritoneum was taken melanosis is of unknown origin. Confirmation of
and the specimen was sent for HPR. Patient stood the condition is done with peritoneal biopsies.
the procedure well and the post op was uneventful. There are handful case reports showing
presentation of Peritoneal Melanosis.
Angelopoulos et al in 2013 reported a case of
Benign Peritoneal Melanosis in 35 year old
women with symptoms of abdominal and pelvic
MACROSCOPIC FINDINGS OF THE pain. Diagnosis was done by laparoscopy and
SPECIMEN confirmed by extensive peritoneal biopsies. Kim et
There was a flap like structure black in color al in 2010 reported a case of peritoneal melanosis
measuring 2.2X1.3X0.8 cms. Another specimen associated with mucinous cystadenoma of ovary
was of uterus with both adnexa. H & E pictures and adenocarcinoma of colon. In that patient
of peritoneum and underlying connective tissue India-ink-colored pigmentation was seen in the
showed deposition of fine granular black material peritoneum, in the omentum, and on the surface
in the submesothelial fibrous tissue (Figure 1C of the ovary during the surgery. Pigment in the
&D). This material stains black with Masson stroma and pigment-laden histiocytic aggregation
Fontana stain (A Stain for Melanin). On the basis of were seen in biopsies of omentum and peritonium.
surgical and histopathological findings, diagnosis Likewise, another case of peritoneal melanosis
of Benign Peritoneal Melanosis was made. combined with serous cystdenoma of ovary was
Histopathological findings of uterus showed as reported by Kim et al 2002. Follow up of these
8 Atypical Leiomyoma of uterus. cases were not reported.
Benign Peritoneal Melanosis associated with atypical leiomyoma M. Alwani et al.
It has been described along with cystic peritoneal biopsies and further investigation
abnormalities of the ovary (serous, mucinous), to exclude sinister pathology. This case was
cystic teratomas of the ovary (Dermoid cysts), chosen for publication because of its rarity, scary
colonic tumors, malignant melanomas and rarely presentation and it could be of research interest
with genetic disorders (eg enteric duplication,
gastric triplication) [De la Torre 1997, Nada et
al 2000, Kim et al 2002, Hefaiedh et al 2009]. Our
patient had no GIT Symptoms. She did not report ACKOWLEDGEMENTT
any ovarian cyst or cyst “accident”. Authors would like to thank chairman, Sri
There is no protocol yet mentioned for the Aurobindo Medical College and PG Institute,
follow up of this clinical entity so we decided to Indore for providing Infrastructure facilities to
give the patient first follow up in 1 month, 2nd carry out this research
follow up in 3 months and then every 6 months.
Prognosis of this condition is quite uncertain.
History and pattern of disease is unclear due to DECLARATION OF INTEREST
scarcity of cases. Given associations with ovarian ACKOWLEDGEMENT
pathology and gastrointestinal malignancies None
we suggest confirmation of the condition with
REFERENCES
1) Angelopoulos G, Smith J H F, Farag K. Benign 5) Kim NR, Suh YL, Song SY, Ahn G. Peritoneal
Peritoneal Melanosis; a rare case report. BJOG. melanosis combined with serous cystadenoma of the
2013;120(S1):406 ovary: a case report and literature review. Pathol Int.
2) De la Torre Mondragón L, Daza DC, Bustamante 2002; 52(11):724-9.
AP, Fascinetto GV. Gastric triplication and peritoneal 6) Kim SS, Nam JH, Kim SM, Choi YD, Lee JH.
melanosis. J Pediatr Surg. 1997; 32(12):1773-5. Peritoneal melanosis associated with mucinous
3) Hefaiedh R, Fekih M, Kacem IH, Matri S, Boubaker cystadenoma of the ovary and adenocarcinoma of the
J, Filali A. [Peritoneal melanosis: a rare localization colon. Int J Gynecol Pathol. 2010;29(2):113-6.
of the melanoma: a case report]. Tunis Med. 7) Nada R, Vaiphei K, Rao KL. Enteric duplication
2009;87(10):719-20[French] cyst associated with melanosisperitonei. Indian J
4) Jaworski RC. Peritoneal “Melanosis”. Int J Gastroenterol. 2000;19(3):140-1.
GynecolPathol. 2003; 22(1):104.
9SIGO 2016
91° congresso
nazionale SIGO
56° congresso
nazionale AOGOI
23° congresso
nazionale AGUI
ROMA
Ergife Palace Hotel
16/19 Ottobre 2016 Segreteria organizzativa:
presidenti
Giovanni Scambia
Enrico Vizza
LA SALUTE AL FEMMINILE
TRA SOSTENIBILITA’
E SOCIETA’ MULTIETNICA
Associazione Ginecologi
Universitari ItalianiItalian Journal of
Gynaecology & Obstetrics
September 2016 - Vol. 28 - N. 4 - Quarterly - ISSN 2385 - 0868
Intrauterine transfusion versus Corticosteroids for treatment of immune
fetal hydrops secondary to Rh incompatibility with 6 months postnatal
follow-up: Case series with review of literature
Tamer Mamdouh Abdeldayem1, ElSayed El Badawy Mohamed1, Ahmed El Habashy1, Sherif
Gaafar1, Ashraf Han1, Aly Alaa Youssef2
1
Department of Obstetrics and Gynecology, Faculty of Medicine, Alexandria University, Egypt.
2
Department of Obstetrics and Gynecology, Sant’Orsola Malpighi University Hospital, University of Bologna, Italy
ABSTRACT SOMMARIO
Introduction: Immune hydrops fetalis is still a L’idrope fetale immunomediata in medicina fetale
challenging condition in fetal medicine. Corticosteroids è ancora una condizione clinica indaginosa. I
are established for immune suppression in auto-immune corticosteroidi sono somministrati nei disordini
disorders. Their use in cases of Rh isoimmunization is not immuno mediati come terapia immuno soppressiva.
fully studied so the aim of our study was to evaluate its Il loro uso in caso di isomimmunizzazione Rh non
role in fetal hydrops. è ancora stato studiato a fondo, quindi lo scopo del
Methods: This study included six patients recruited from nostro studio è quello di valutarne il possibile ruolo nel
January 2015 to December 2015 at fetal medicine center- trattametno dell’idrope fetale.
Alexandria, Egypt. Patients were multiparous women Questo studio include sei pazienti che sono state
with Rh negative blood group and history of successful full reclutate da gennaio 2015 a dicembre 2015 nel centro
term delivery once before. They had clinical history of fetal di medicina fetale di Alessandria, in Egitto. Le pazienti
hydrops and subsequent intrauterine fetal death at 26-28 erano pluripare con gruppo sanguigno Rh negativo ed
weeks of gestation in the subsequent pregnancies. Patients in anamnesi una gravidanza portata fino al termine
were referred to the center at gestational age 22-32weeks con successo. Le pazienti incluse hanno avuto una
gestation. Three cases were treated by Cordocentesis and gravidanza con feto affetto da idrope fetale e successiva
transfusion of irradiated O negative red blood cells, Three morte intrauterina tra 26-28 settimane e sono giunte al
cases were treated by administration of prednisolone 20 nostro centro tra le 22 e le 32 settimane di gestazione. Tre
mg tab twice a day for suppression of maternal anti-Rh dei casi inclusi nello studio sono stati trattati mediante
antibodies production. Ultrasonographic examination was cordocentesi e trasfusione di globuli rossi irradiati O
repeated every week. For cases whose fetuses survived negativo. Tre sono stati trattati con somministrazione
till 34 weeks gestation, 4 doses of Dexamethasone 6 mg orale di prednisolone 20 mg per due volte al giorno
were given intramuscularly and cases were delivered by ai fini della soppressione della produzione materna di
elective caesarian section. anticorpi anti Rh. Gli esami ecografici sono stati ripetuti
Results: Three progressed into sudden intrauterine fetal ogni settimana. Le pazienti i cui feti sono sopravvissuti
death; two of them treated with transfusion and one with oltre le 34 settimane di gestazione sono state trattate
corticosteroids. One, treated by transfusion, improved mediante 4 dosi da 6 mg di desametasone per via
and was delivered at 33 weeks gestation after full course intramuscolo ed in questi casi è stato eseguito un taglio
of dexamethasone administration to the mother. For the cesareo elettivo.
other two cases treated by corticosteroids, both were Tre pazienti hanno avuto morte intrauterina fetale;
delivered at 34 weeks gestation, none developed hydrops due di queste erano state trattate con trasfusione e una
fetalis. Follow-up of the three surviving neonates was con corticosteroidi. Una paziente trattata mediante
done till 6 months after birth showed normal growth and trasfusione è andata incontro a miglioramento e ha
neurological development. partorito a 33 settimane dopo aver concluso la terapia
Conclusions: Corticosteroids could be of benefit in con desametasone. Per i due casi che sono stati trattati
treating fetal hydrops but this needs to be evaluated more con corticosteroidi, entrambi hanno partorito a 34
in a large studies. settimane senza sviluppare idrope fetale. I neonati
Keywords: Steroids, Hydrops, Ultrasound, Anemia, sopravvissuti sono stati sottoposti a follow up fino ai
Pregnancy 6 mesi di vita e hanno mostrato un normale sviluppo
Correspondence to: tmdaeim@gmail.com fisico e neurologico.
Copyright 2015, Partner-Graf srl, Prato I corticosteroidi potrebbero essere di beneficio nel
DOI: 10.14660/2385-0868-48 trattare l’idrope fetale ma sono necessari studi con una
più ampia coorte di pazienti. 11It. J. Gynaecol. Obstet. Use of corticosteroids for treatment of immune hydrops fetalis
2016, 28: N. 4
INTRODUCTION RESULTS
Immune hydrops fetalis is still a challenging All cases were Rh negative, with indirect
condition in fetal medicine. Incidence has Coomb’s test showing anti-Rh antibodies titer
decreased dramatically in last decades after above 1/32.Gestational ages were 22-26 weeks
introduction of the use of anti D immunoglobulins in the recruited cases. Middle cerebral artery
after delivery, at 28-30 weeks gestation and peak systolic velocity was above 1.5 MoM for
after any bleeding incidence during gestation(1). the gestational age in all three recruited cases.
Screening for Rh isoimmunization is through Four cases showed fetal ascites at the time of
anti-Rh antibodies, using indirect Coomb’s recruitment. Three of them were treated with
test. Screening for fetal anemia is feasible using serial cordocentesis and O negative red blood cell
values of peak systolic velocity in middle transfusion, guided by Peak systolic velocities in
cerebral artery(2). Established treatment is serial middle cerebral artery. Of these four cases, three
intrauterine transfusion of irradiated O negative progressed into sudden intrauterine fetal death;
red blood cells, whether into the umbilical vein two of them treated with transfusion and one
or intraperitoneal. These routes carry the risk of with corticosteroids. One, treated by transfusion,
intrauterine infection, preterm birth, intrauterine improved and was delivered at 33 weeks gestation
fetal death and others(3-5). after full course of dexamethasone administration
Corticosteroids are established for immune to the mother. Fetal weight was 1800 gms, severe
suppression in auto-immune disorders. Their use neonatal jaundice developed and was promptly
in cases of Rh isoimmunization is not fully studied treated by exchange transfusion and phototherapy.
so the aim of our study was to evaluate its role in Neonate was discharged after 16 days. For the
fetal hydrops. other two cases treated by corticosteroids, both
were delivered at 34 weeks gestation, none
developed hydrops fetalis. Birth weights were 1900
and 1950 grams. Newborns developed hemolytic
METHODS anemia and jaundice at day one, necessitating
This study included six patients recruited exchange transfusion, which was repeated three
from January 2015 to December 2015 at fetal times together with phototherapy. Fetuses were
medicine center-Alexandria, Egypt. Patients were discharged 12 and 14 days after delivery. Follow-
multiparous women with Rh negative blood group up of the three surviving neonates was done till
and history of successful full term delivery once 6 months after birth showed normal growth and
before. They had clinical history of fetal hydrops neurological development.
and subsequent intrauterine fetal death at 26-28
weeks of gestation in the subsequent pregnancies.
Patients were referred to the center at gestational
age 22-32 weeks gestation. DISCUSSION
At recruitment, they were subjected to: Alloanti-D that is acquired during pregnancy
Assessment of ABO and Rh blood grouping, or by transfusion is a major cause of severe and
Measurement of hemoglobin, postprandial sometimes fatal haemolytic disease of newborns
blood sugar and anti-Rh antibody titer and and haemolytic transfusion reactions, respectively.
Ultra-sonographic examination including: Isoimmunized mothers are destined to have
Fetal biometry, anomaly scan including fetal immune hydrops in all future pregnancies with
echocardiography and Peak systolic velocity in Rh positive fetuses. Treatment of these fetuses
middle cerebral artery. is currently through repeated intrauterine
Three cases were treated by Cordocentesis and transfusion, Other modes of treatment include
transfusion o irradiated O negative red blood cells, plasmapheresis to dilute the anti-Rh antibodies
Three cases were treated by administration of in maternal blood, with large volumes of plasma
prednisolone 20 mg tab twice a day for suppression needed for this procedure. Pharmaceutical
of maternal anti-Rh antibodies production. treatment is currently of limited use. In our case
Ultrasonographic examination was repeated series we proposed the use of relatively high
every week. For cases whose fetuses survived till doses of corticosteroids for immune suppression
34 weeks gestation, 4 doses of Dexamethasone 6 versus the established transfusion therapy. The
mg were given intramuscularly and cases were underlying principle is suppression of maternal
delivered by elective caesarian section. Anti-Rh antibodies which cross the placenta and
12 cause fetal hemolysis(3-6).Use of corticosteroids for treatment of immune hydrops fetalis T. M. Abdeldayem et al.
Early use of this mode of treatment was immunoglobulin therapy. Prednisolone therapy is
successful to suppress antibodies, allowing the cheap, it proved helpful on its own for obtaining
bone marrow and reticuloendothelial system of good outcome, and in combination with other
two fetuses to maintain adequate cardiovascular therapies prognosis could be more favorable.
function and tissue oxygenation. Liver affection
was not documented and no evidence of ascites,
pleural effusion nor subcutaneous oedema was
found in the two cases surviving on prednisolone CONCLUSIONS
therapy. Second case showed hepatomegaly Corticosteroids could be of benefit in treating
at 33 weeks, 4 days, prompting the decision of fetal hydrops but this needs to be evaluated more
caeserian delivery after 4 doses of corticosteroids. in a large studies.
Conservative treatment till this age allowed
shorter period of admission at neonatal intensive
care unit and helped improve the outcome for
fetuses of both cases. Treatment with 40 mg AUTHORS CONTRIBUTION:
oral prednisolone helped save two fetuses of All the authors contributed to protocol
isoimmunized mothers. It could be used alone or development, data collection and management,
in conjunction with other modes of treatment(3-6). Data analysis and Manuscript writing/editing.
On the other hand, cases already presenting Ethical disclosure
with evidence of fetal ascites mostly agreed to Protection of human and animal subjects. The
the transfusion therapy, with only one having authors declare that the procedures followed were
successful outcome. This method is more effective in accordance with the regulations of the relevant
in replacing hemolysis fetal red blood cells, clinical research ethics committee and with
without slowing down the rate of hemolysis(6). those of the Code of Ethics of the World Medical
Isojima et al(7) reported the successful use Association (Declaration of Helsinki).
of plasmapheresis and high doses of gamma Confidentiality of data. The authors declare
globulins for dilution and neutralization of anti- that they have followed the protocols of their work
Rh antibodies in one case. center on the publication of patient data.
Houston et al(8) reported another cases case Right to privacy and informed consent. The
managed with the same combination, none of authors have obtained the written informed
them added corticosteroids. consent of the patients or subjects mentioned in the
In conclusion, we propose the addition of article. The corresponding author is in possession
40 mg oral prednisolone therapy to preganant of this document.
females, in addition to other modes of therapy, Conflict of interest. The authors declare no
whether transfusion or plasmapheresis and conflict of interest.
REFERENCES
1) McBain RD, Crowther CA, Middleton P. Anti-D 5) Moise KJ Jr. Management of rhesus alloimmunization
administration in pregnancy for preventing Rhesus in pregnancy. Obstet Gynecol. 2008 Jul;112(1):164-76.
alloimmunisation. Cochrane Database Syst Rev. 2015 6) Aitken SL, Tichy EM. Rh(O)D immune globulin
Sep 3;9. products for prevention of alloimmunization
2) Mari G, Norton ME, Stone J. Society for Maternal- during pregnancy. Am J Health Syst Pharm. 2015 Feb
Fetal Medicine (SMFM) Clinical Guideline #8: the 15;72(4):267-76.
fetus at risk for anemia--diagnosis and management. 7) Isojima S, Hisano M, Suzuki T. Early plasmapheresis
Am J Obstet Gynecol. 2015 Jun;212(6):697-710 followed by high-dose γ-globulin treatment saved a
3) Bigelow CA, Cinelli CM, Little SE. Percutaneous severely Rho-incompatible pregnancy. J Clin Apher.
umbilical blood sampling: current trends and 2011;26(4):216-8
outcomes. Eur J Obstet Gynecol Reprod Biol. 2016 8) Houston BL, Govia R, Abou-Setta AM. Severe
May;200:98-101. Rh alloimmunization and hemolytic disease of the
4) Aitken SL, Tichy EM. Rh(O)D immune globulin fetus managed with plasmapheresis, intravenous
products for prevention of alloimmunization immunoglobulin and intrauterine transfusion: A case
during pregnancy. Am J Health Syst Pharm. 2015 Feb report. Transfus Apher Sci. 2015 Dec;53(3):399-402.
15;72(4):267-76. 13M E V
U T ICA
A C E O G IA
FARM INECOL
IN G LA NATURA CHE AIUTA
ClimaMEV
IncontinenzaMEV
VenaMEV
FARMACEUTICA MEV - Strada Cassia Sud, 175 - 53100 Siena (SI)
Tel. 0577 378091/ Fax 0577 379970 - www.farmaceutica-mev.itItalian Journal of
Gynaecology & Obstetrics
September 2016 - Vol. 28 - N. 4 - Quarterly - ISSN 2385 - 0868
Improving prescription of physical exercise in prophylaxis/therapy of
gestational diabetes: a survey from evidence to current recommendations
Cristina Bianchi1, Michele Aragona1, Alessandra Bertolotto1, Pietro Bottone11, Maria
Calabrese4, Ilaria Cuccuru5, Alessandra De Bellis6, Anna Leopardi8, Cristina Lencioni2,
Roberto Miccoli10, Mary Liana Mori7, Serena Ottanelli3, Matilde Romano11, Gigliola Sabbatini9,
Maria Giovanna Salerno11, Giuseppe Trojano11, Stefano Del Prato10, Lorella Battini11 on behalf
of Tuscany working group on “Diabetes, Pregnancy and Exercise”*
1
U.O. Malattie Metaboliche e Diabetologia, Azienda Ospedaliero-Universitaria Pisana, Pisa
2
U.O.C. Diabetologia e Malattie Metaboliche, Ospedale di Livorno
3
U.O. Ostetricia e Ginecologia, Ospedale di Arezzo
4
U.O. Diabetologia, Ospedale di Prato
5
U.O.S. Diabetologia, Ospedale di Lucca
6
U.O.C. Diabetologia, Ospedale di Pistoia
7
U.O.S. Diabetologia, Ospedale di Carrara
8
U.O.C Diabetologia e Malattie Metaboliche, Ospedale San Giovanni di Dio - Firenze
9
U.O. Diabetologia, Ospedale di Grosseto
10
Dipartimento di Medicina Clinica e Sperimentale, Università di Pisa
11
U.O. Ginecologia ed Ostetricia, Azienda Ospedaliero-Universitaria Pisana, Pisa
ABSTRACT SOMMARIO
Exercise has been proved to be safe during pregnancy Numerose evidenze suggeriscono che l’attività fisica è
and to offer benefits for both mother and fetus; sicura in gravidanza e offre benefici sia per la madre che
moreover, physical activity may represent a useful per il feto; inoltre, l’esercizio fisico può rappresentare
tool for gestational diabetes prevention and treatment. un utile strumento per la prevenzione e il trattamento
Therefore, all women in uncomplicated pregnancy del diabete gestazionale. Pertanto, tutte le donne
should be encouraged to engage in physical activity in gravidanza non complicata dovrebbero essere
as part of a healthy lifestyle. However, exercise in incoraggiate ad impegnarsi in attività fisica come parte
pregnancy needs a careful medical evaluation to exclude integrante di uno stile di vita sano. Tuttavia, l’esercizio
medical or obstetric contraindications to exercise, and fisico in gravidanza necessita di una attenta valutazione
an appropriate prescription considering frequency, medica per escludere controindicazioni mediche od
intensity, type and duration of exercise, to carefully ostetriche, e una prescrizione appropriata che tenga
balance between potential benefits and potential conto della frequenza, dell’intensità, del tipo e della
harmful effects. Moreover, some precautions related to durata dell’esercizio, per bilanciare con attenzione i
anatomical and functional adaptations observed during benefici e gli effetti indesiderati potenziali. Inoltre,
pregnancy should be taken into consideration. This dovrebbero essere prese in considerazione alcune
survey summarized the suggested recommendations precauzioni relative ai fisiologici adattamenti anatomici
for physical activity among pregnant women with focus e funzionali che si osservano durante la gravidanza.
on gestational diabetes. Questa survey riassume le raccomandazioni attualmente
suggerite per l’attività fisica nelle donne in gravidanza
Keywords: Guidelines, Physical Activity, Gestational con particolare attenzione al diabete gestazionale.
Diabetes, Pregnancy.
INTRODUCTION
Gestational Diabetes Mellitus (GDM) is the most prevalence is increasing worldwide accordingly
common metabolic complication of pregnancy. Its with increasing of obesity and the number of
obese pregnant women(1). Significant evidences
Correspondence to: lorella.battini@gmail.com suggest that physical activity may represent a
Copyright 2015, Partner-Graf srl, Prato simple, inexpensive and useful tool for GDM
DOI: 10.14660/2385-0868-49 prevention and treatment(2). However, exercise 15It. J. Gynaecol. Obstet. Gestational diabetes and exercis
2016, 28: N. 4
in pregnancy needs a careful evaluation and includes: maternal education, diet modifications,
appropriate prescription. To implement a proper exercise, drug treatment and fetal surveillance
prescription of exercise during pregnancy, we (Figure 1).
examined the published international guidelines The initial management of GDM involves diet
for exercise in pregnancy(3-9) complicated or not modifications and implementation of regular
by diabetes and summarize in this survey the physical activity. If adequate glycemic control is not
suggested recommendations for physical activity been achieved, drug treatment is prescribed with
among pregnant women with focus on GDM. the aim to reach the target maternal blood glucose
levels and hence indirectly for the fetus (17-19).
GESTATIONAL DIABETES:
SCREENING, DIAGNOSIS AND
MANAGEMENT
Briefly, GDM is defined as a carbohydrate
intolerance of varying degree of severity with
first diagnosis during pregnancy and a natural
dispelling of the hyperglycemic condition
after child birth(4). GDM, when undiagnosed
or inadequately treated, has many detrimental
consequences for the woman, the fetus and the
child(10-15).
Since 2011, the Italian National Health System Figure 1. Key elements in the management of gestational diabetes.
guidelines recommend a selective screening for
GDM based on risk factors. According to national
guidelines, high risk women are those with A PHYSICAL ACTIVITY DURING
previous GDM, obesity (pre-gestational BMI≥30 PREGNANCY: BENEFITS AND RISKS
kg/m2), fasting plasma glucose between 100 and Exercise has been proved to be a beneficial
125 mg/dl, in the first trimester of pregnancy; therapeutic tool during pregnancy (Table 2).
while at medium risk are women aged 35 years Recent studies showed that exercise was safe and
or older, overweight (pre-gestational BMI 25-29.9 advantageous for glucose control for women with
kg/m2), with family history of type 2 diabetes, GDM, improved cardiovascular functions (fitness,
previous fetal macrosomia, ethnic group at GDM blood pressure, peripheral edema), preeclampsia
high risk. Based on this stratification, in high prophylaxis, varicose veins and deep vein
risk women an early screening between 16th- thrombosis, decreased lower back pain and had
18th gestational week was recommended, to be benefits on mood and psychological wellbeing;
repeated later (24th-28th gestational week) in case decreased risk of preterm delivery, length of labor
of normal glucose tolerance, while in medium and delivery complications; furthermore exercise
risk women the screening was scheduled between has an important role in limitation of weight gain
24th-28th gestational week. Diagnosis of GDM is and fat retention after delivery, also improving self
based on IADPSG/WHO 2013 criteria. (Table 1). image(20-21). Maternal exercise has also been shown
Table 1. Diagnostic criteria for GDM (IADPSG/WHO 2013) 16.
to provide significant benefits to the fetus health:
increased amniotic fluid, increased in placenta
Glucose viability and volume, increased vascular function,
2 hours -75 g OGTT concentration threshold*
faster placenta growth and greater villous tissue,
Fasting plasma glucose ≥ 5.1 mmol/l (92 mg/dl) more adequate birth weight and lower risk of
1-h plasma glucose ≥ 10.0 mmol/l (180 mg/dl)
2-h plasma glucose ≥ 8.5 mmol/l (153 mg/dl)
preterm birth, improved neurodevelopment and
lower fetal body fat percentage(22-25). Therefore,
*One or more of these values from a 75-g OGTT must be equaled or considering the benefits of exercise during
exceeded for the diagnosis of GDM 16. pregnancy, it’s necessary that it becomes an
integral part of treatment strategies in women
The primary aim of GDM treatment is blood during pregnancy and particularly in case of
glucose control in order to reduce the elevated pregnancy complicated by GDM.
risk for short and long term complications for both Exercise prescription requires knowledge
16 mother and offspring. The approach for GDM of the potential risks and assessment of theGestational diabetes and exercise L. Battini et al.
Table 2. Benefits of maternal exercise
Benefits to the mother Benefits to the foetus Benefits to the child
• Improved glucose control • Lower heart rate response to acute • Infants have higher behaviour regulatory
• Decreased lower back pain maternal exercise ability and orientation
• Improve cardiovascular functions • Increased amniotic fluids • At the age of five children have less body
• Decreased preeclampsia • Increase in placenta viability and volume fat, higher general language intelligence
• Improved muscle tone • Increase in vascular function and oral language
• Reduced lenght of labour • Faster placental growth and greater
• On mood and psychological wellbeing villous tissue
• Improved self image • Higher tolerance to labour
• Control in weight gain • Lower birth weights
• Facilitating post partum weight loss • Lower risk of preterm birth
• Reduced costipation and bloating, • Improved neurodevelopment and lower
fatigue and insomnia body fat percentage
physical ability to engage in various activities. Women with complicated pregnancy have
As with any clinical population, there are some been discouraged from the practice of physical
contraindications to exercise also in pregnancy. activity to avoid a worsening of the underlying
Moreover, some anatomical and physiological disease or negative impacting both maternal and
change occurring during pregnancy should fetal outcomes. The absolute contraindications
be taken into account in prescribing exercise. represent conditions where exercise is not
Therefore, clinical evaluation of each pregnant recommended, while relative contraindications
woman should be conducted before physical are conditions where the risks may outweigh
activity is recommended and exercise programs the benefits of regular physical activity and
should be tailored by appropriately trained and should be individually evaluated (Table 3).
qualified practitioners. Therefore, clinical evaluation of each pregnant
Pregnant women with GDM don’t need woman should be performed before physical
suggestions or special precautions for physical activity is recommended. [Level of evidence V,
activity other than those recommended in women Recommendation B]
with normal glucose tolerance but, considering
the presence of hyperglycemia, they need to
take into account the recommendations for the STARTING A NEW EXERCISE
physical activity outlined for the pre-gestational PROGRAM DURING PREGNANCY
diabetes too, especially when GDM requires Starting a new exercise program should be
a pharmacological treatment that could cause considered already in the pre-conceptional period,
hypoglycemia. Considering the lack of large cohort especially in women who are overweight-obese
studies implementing exercise as treatment of and/or have other risk factors for GDM (previous
GDM, the suggested recommendations have been gestational diabetes, age > 35 years, family history
derived from exercise guidelines in pregnancy for diabetes, high-risk ethnic group) in order to
and exercise in type 2 diabetes guidelines(26-31). avoid excessive weight gain during pregnancy
Although currently there is only a GDM specific and prevent GDM (33) [Level of evidence III,
exercise prescription guideline published(32), we Recommendation B].
suggest to develop italian recommendations to Previously active women can continue the
allow proper application of physical activity regular practice of physical exercise, as long as
practice as an effective tool in glucose control to the pregnancy is uncomplicated, and the activity
prevent, delay or treat GDM. practiced meets the safety criteria in terms of
type, intensity and frequency of exercise as
suggested below-Table 4 (34). [Level of evidence III,
I N D I C A T I O N A N D Recommendation B].
CONTRAINDICATIONS TO In sedentary women, especially those in
which the gestational diabetes is diagnosed, an
PHYSICAL ACTIVITY DURING
exercise program could be initiated in the second
PREGNANCY trimester, when the nausea, vomiting, and fatigue
All women in uncomplicated pregnancy (sometimes intense in the first trimester) have
should be encouraged to engage in physical passed and before the physical limitations of
activity as part of a healthy lifestyle. [Level of the third trimester occur. [Level of evidence VI,
evidence II, Recommendation B] Recommendation C]. 17It. J. Gynaecol. Obstet. Gestational diabetes and exercis
2016, 28: N. 4
Table 3. Relative and absolute contraindications for the practice of physical activity during pregnancy.
Absolute Relative
Obstetric complications Obstetric complications
• Ruptured membranes • History of spontaneous abortion or premature labour in previous
• Preeclampsia pregnancies
• Pregnancy-induced hypertension • Twin pregnancy after 28th week
• Premature labour during current pregnancy • Intrauterine growth restriction in current pregnancy
• Persistent bleeding (second or third trimester) • Previous spontaneous abortion
• Incomplete cervix or cerclage • Anaemia (Hb >10 g/dL)
• Placenta previa (placental implanting into lower uterus) after 26 • Twin pregnancy after 28 wk
wk of gestation Behaviour habits and medical complications
• High order multiple gestation (≥ triplets) • Heavy smoking
Medical complications • History of extremely sedentary lifestyle
• Restrictive lung disease • Orthopaedic limitations
• Hemodynamically significant heart disease • Poorly controlled hypertension
• Severe anaemia (Hb 40 kg/m2)
• Poorly controlled hyperthyroidism
• Poorly controlled type 1 diabetes
EXERCISE PRESCRIPTION DURING
PREGNANCY
Consideration should be given to frequency appropriate heart rate) (36). [Level of evidence IV,
of exercise sessions, intensity of exercise, type Recommendation C]. To optimize the metabolic
of exercise and its duration, to carefully balance benefits of physical activity, due to the transient
between potential benefits and potential improvement of insulin action and passive glucose
harmful effects. We identified in the FITT model uptake for up to 48 hours, exercise should be
(Frequency, Intensity, Time/duration and Type - conducted with no more than two consecutive
Table 4) a valid tool to prescribe physical activity days between sessions.
during pregnancy in order to prevent and treat Aerobic activity should be preceded by a
GDM (35). short (10-15 min.) warming up and followed by
a short (10-15 min.) cool-down phase that include
Table 4. FITT
(Frequency, Intensity, Time / duration and Type) model. stretching and relaxation exercises. [Level of
evidence VI, Recommendation C].
F FREQUENCY Begin at 3 times per week and progress to 4
times per week Intensity
The best way to prescribe and monitor the
I INTENSITY Exercise to not excessively increase the heart
rate. The proper intensity is one that lets you
intensity of physical activity is evaluating the
continue the conversation while exercising heart rate based on age and the rating of perceived
(Talk Test) exertion (RPE), simultaneously.
T TIME Start from a minimum of 15 minutes per Heart rate: In pregnancy, at rest, there is a
session, 3 times a week (according to an physiological increase in heart rate from 10 to
appropriate target heart rate) to a maximum of
about 30 minutes per session, 4 times a week 15 beats/minute(37). The target heart rate during
(to the appropriate heart rate). exercise, depending on the age of the woman
T TYPE Preferably use large muscle groups (such
(Table 5), representing about 60-80% of peak
as those that are put in motion for walking, aerobic capacity for a pregnant woman (38) [Level
stationary bike, swimming, aquatic exercise, of evidence VI, Recommendation C].
low impact aerobics). Avoid the exercises
with use of weights or resistance; those that
can cause falls; sports at high altitude and
Table 5. Heart Rate Intervals useful for pregnant women.
underwater.
Maternal age Fitness level Heart rate range
(years) (beats/minute)
FREQUENCY AND DURATION
Aerobic exercise should go on for a minimum < 20 - 140-155
of 15 minutes per session, 3 times a week Low 129-144
(according to an appropriate target heart rate), and 20-29 Active 135-150
Fit 145-160
should be increased gradually during the second Low 128-144
trimester up to a maximum of approximately 30-39 Active 130-145
18 30 minutes per session, 4 times to week (to the Fit 140-156Gestational diabetes and exercise L. Battini et al.
Classification of perceived physical activity: Precautions for exercise during pregnancy
Choosing carefully the desirable heart rate, it is Although it is useful to exercise all muscle
useful to compare it with the scale that assesses the groups, precautions shall be taken, in part related
individual’s perception of physical activity (Borg’s to anatomical and functional adaptations that are
scale, Table 6) (39). An interval between 12 and observed during pregnancy (Figure 2).
14 is appropriate for most of pregnant women.
[Level of evidence VI, Recommendation C].
Table 6. Borg’s scale of perceived physical activity
6 7 8 9 10 11 12 13 14 15 16 17 18 19 20
Very Somewhat Light Somewhat Hard Very Very
very light light hard hard very hard
Talk Test: A simple, alternative or complement
system for assessing the adequacy of physical
exercise intensity is represented by the “talk test”:
if a woman is able to maintain a conversation
during exercise means that the intensity of
exercise is adequate; It should be reduced if the
conversation is not possible. [Level of evidence
VI, Recommendation C]. Figure 2. Anatomical and physiological adaptation during
pregnancy and related potential risks during exercise.
Musculo-skeletal adaptation: The increase in
weight can increase the pressure on all the joints,
TYPE especially hips and knees, causing discomfort
Exercise for the development and the for normal joints and increase in damage in
maintenance of adequate physical fit in pregnant previously unstable joints. Furthermore, due to the
women consists of activities that improve both the increase of weight and abdomen, pregnant women
cardio-respiratory (aerobic exercise, consisting of any usually develop lumbar lordosis, which leads to
activity that uses large muscle groups rhythmically changes in posture, predisposing them to loss of
and continuously) and musculoskeletal status balance and increased risk of falls. Finally, during
(strength and flexibility exercises) [Level of evidence pregnancy there is an increase of the laxity of the
VI, Recommendation C]. ligaments, due to the higher levels of estrogen and
However, some elements should be considered relaxin. This could predispose pregnant women to
when prescribing physical activity during a higher risk of tearing and distortions.
pregnancy. Cardiovascular adaptation: Pregnancy induces
A wide range of recreational activities appears an increase in blood volume, frequency and cardiac
to be safe for pregnant women. The safety of output, and a reduction in systemic vascular
each sport is largely determined by the specific resistance (40). These hemodynamic changes seem
movements required by the exercise. Activities to establish a circulatory reserve, necessary to
with a high risk of falling or abdominal trauma provide nutrients and oxygen to the mother
should be discouraged. Activity with a high and fetus at rest and during moderate physical
potential for physical contact (such as ice hockey, activity(41). After the first trimester, the supine
football, and basketball) or falls (horseback riding, position results in relative obstruction of venous
downhill skiing, ...) can cause severe trauma to return and therefore decreased cardiac output. For
both mother and fetus and therefore should be this reason, the supine position should be avoided
discouraged. Scuba diving should be avoided as much as possible during both rest and exercise.
during pregnancy, because the fetus is at risk [Level of evidence VI, Recommendation C].
for decompression sickness. Caution should Furthermore, the maintenance of the motionless
be also in the practice of physical exercise at standing should be avoided because it is associated
high altitude (> 2500 m). [Level of evidence VI, with a significant decrease in cardiac output.
Recommendation C]. Respiratory adaptation: Pregnancy is
The most popular form of aerobic activity associated with increase of about 50% of the
during pregnancy is walking, however, also water ventilation, increase in arterial oxygen tension,
exercise may be an excellent choice of exercise especially in the first trimester, increased uptake of
during pregnancy. oxygen and its baseline consumption(42). Because 19It. J. Gynaecol. Obstet. Gestational diabetes and exercis
2016, 28: N. 4
of the increased requirement of oxygen at rest insulin-treated, it is necessary to minimize the risk
and increased work of breathing caused by the of an episode, however rare, of hypoglycemia.
pressure exerted on the diaphragm by increased Therefore, glucose self-monitoring should be
uterine volume, the availability of oxygen for the recommended before and after physical exercise.
execution of aerobic exercise during pregnancy If exercise is particularly prolonged, glucose
decreases. monitoring should be performed also during
Thermoregulation: During pregnancy, the physical activity. Moreover, if glycemia before
basal metabolic rate, and thus heat production, has exercise is ≤ 70 mg/dl, it is useful to posticipate
increased. The dissipation of excess heat generated the exercise after the intake of glucose and the
during exercise can be a potential problem, since restoration of an adequate blood glucose level.
some studies suggest that hyperthermia (body Finally, it may be important to perform physical
temperature > 39°C) during the first 45-60 days activity after at least one hour of rapid acting
of gestation can also be teratogenic in humans (43). insulin administration, in order to further reduce
The increase in body temperature during exercise the risk of hypoglycemia.
is directly related to the intensity of exercise (44). If Indication to the interruption of physical activity
the production of heat exceeds the heat dissipation Pregnant women should be asked to stop
capacity, for example during exercise in hot, humid physical activity in case of occurrence of:
conditions or during very high intensity exercise, •Excessive shortness of breath, feeling short of
the temperature may further rise. The exercise breath or rapid heartbeat
should, therefore, be preferably performed in a •Chest pain
thermo-neutral environment or under controlled •Painful uterine contractions
environmental conditions (conditioning). [Level (more than 6-8 per hour)
of evidence VI, Recommendation C]. Moreover, •Vaginal bleeding
since during prolonged exercise the loss of fluid •Any “gush” of fluid from the vagina
through sweat can impair the dissipation of heat, (suggesting premature rupture of membranes)
it must be maintained a proper hydration. •Dizziness or weakness
In women with gestational diabetes, especially [Level of evidence VI, Recommendation C].
REFERENCES
1) IDF Diabetes Atlas. Seventh edition, 2015. 8) Sports Medicine Australia. SMA statement: the
2) Carolan-OIah MC. Educational and intervention benefits and risks of exercise during pregnancy. J Sci
programs for gestational diabetes mellitus (GDM) Med Sport 2002; 5(1):11–19.
management: An integrative review. Collegian 9) Metzger BE, Coustan DR. Summary and
2016;23(1):103-14. recommendations of the Fourth International
3) U.S. Department of Health and Human Services. 2008 Workshop-Conference on Gestational Diabetes
Physical Activity Guidelines for Americans. ODPHP Mellitus. The Organizing Committee. Diabetes Care
Publication No. U0036. Washington, D.C: 2008. at 1998; 21 Suppl 2: B161-B167
http://www.health.gov/paguidelines 10) Coustan DR, Imarah J. Prophylactic insulin
4) ACOG. Exercise during pregnancy and the treatment of gestational diabetes reduces the incidence
postpartum period. ACOG Committee Opinion No. of macrosomia, operative delivery,and birth trauma.
267. Obstet Gynecol. 2002; 99(1):171–173. Am J Obstet Gynecol 1984; 150: 836-842
5) Davies G, Wolfe L, Mottola M, MacKinnon C. Joint 11) Hod M, Merlob P, Friedman S, Schoenfeld A, Ovadia
SOGC/CSEP clinical practice guideline: Exercise in J. Gestational diabetes mellitus. A survey of perinatal
pregnancy and the postpartum period. Can J Appl complications in the 1980s.Diabetes 1991; 40 Suppl 2:
Physiol 2003; 28(3):330–341. 74-78
6) Wolfe L, Davies G. Canadian guidelines for exercise 12) Crowther CA, Hiller JE, Moss JR, et al. Australian
in pregnancy. Clin Obstet Gynecol 2003; 46(2):488–495. Carbohydrate Intolerance Study in Pregnant Women
7) Royal College of Obstetricians and (ACHOIS) Trial Group. Effect of treatment of
Gynaecologists. Exercise in pregnancy. RCOG gestational diabetes mellitus on pregnancy outcomes.
Statement No. 4 - January 2006 at http://www. N Engl J Med 2005;352:2477-86
rcog.org.uk/files/rcog-corp/uploaded-files/ 13) Landon MB, Spong CY, Thom E, et al. A multicenter,
20 RCOGStatement4ExercisePregnancy2006.pdf randomized trial of treatment for mild gestationalGestational diabetes and exercise L. Battini et al. Diabetes. N Engl J Med 2009;361:1339-48 physical fitness and HbA1(c) in type 2 diabetes mellitus. 14) Bellamy L, Casas JP, Hingorani AD, et al. Type Diabetologia 2011; 54:93-102. 2 diabetes mellitus after gestational Diabetes: 29) Zanuso S, Jimenez A, Pugliese G, et al. Exercise for a systematic review and meta-analysis. Lancet the management of type 2 diabetes: a review of the 2009;373:1773-1779 evidence. Acta Diabetol 2010; 47:15-22. 15) Pettit D, Bennett PH, Knowler WC, Baird HR, Aleck 30) Sigal RJ, Kenny GP. New evidence for the value KA. Gestational diabetes mellitus and impaired of supervised exercise training in type 2 diabetes glucose tolerance during pregnancy: long-term effects mellitus. Arch Intern Med 2010; 170:1790-1791. on obesity and glucose intolerance in the offspring. 31) Madden KM. Evidence for the benefit of exercise Diabetes Care 1985; 34: 119-122 therapy in patients with type 2 diabetes. Diabetes, 16) Linea-guida Gravidanza fisiologica. Aggiornamento Metab Syndr Obes 2013; 6: 233-239. 2011. Diagnosi del diabete gestazionale, pag 169- 32) Padayachee C, Coombes JS. Exercise guidelines for 173. Accessibile al: www.salute.gov.it/imgs/C_17_ gestational diabetes mellitus. World J Diabetes 2015, pubblicazioni_1436_allegato.pdf (visitato il 28/10/2013) 6(8): 1033-1044. 17) Crowther CA, Hiller JE, Moss JR, McPhee AJ, Jeffries 33) Institute of Medicine IOM(US) and National WS, Robinson JS. Effect of treatment of gestational Research Council (US) Committee to Reexamine IOM diabetes mellitus on pregnancy outcomes. N Engl J Pregnancy Weight Guidelines. Weight gain during Med 2005; 352: 2477-2486 pregnancy: reexamining the guidelines. National 18) Horvath K, Koch K, Jeitler K, et al. Effects of Academy Press, Washington, 2009). treatment in women with gestational diabetes 34) Hale RW, Milne L. The elite athlete and exercise in mellitus: systematic review and meta-analysis. BMJ pregnancy. Semin Perinatol 1996;20:277–84. 2010;340,1395 35) Evenson KR, Barakat R, Brown WJ, Dargent-Molina 19) Poolsup N, Suksomboon N, Amin M. Effect of P, Haruna M, Mikkelsen EM, Mottola MF, Owe KM, treatment of gestational diabetes mellitus: a systematic Rousham EK, Yeo SA. Guidelines for Physical Activity review and meta-analysis. PLoS One 2014; 9: e92485 during Pregnancy: Comparisons From Around the 20) Prather H, Spitznagle T, Hunt D. Benefits of exercise World. Am J Lifestyle Med 2014 ; 8(2): 102–121. during pregnancy. PM R 2012; 4: 845-850 36) Wolfe LA, Hall P,Webb KA, Goodman L, Monga M, 21) Rankin J. The effects of Antenatal Exercise on McGrath MJ. Prescription of aerobic exercise during Psychological Well-being, Pregnancy and Birth pregnancy. Sports Med 1989;8:273–301. Outcomes. Philadelphia: Whurr Publishers, 2002 37) Avery ND,Wolfe LA, Amara CE, Davies GAL, 22) Briend A. Maternal physical activity, birth weight McGrath MJ. Effects of human pregnancy on cardiac and perinatal mortality. Med Hypotheses 1980; 6: autonomic function above and below the ventilatory 1157-1170 threshold. J Appl Physiol 2001;90:321–8. 23) Clapp JF, Capeless EL. Neonatal morphometrics 38) Mottola MF, Davenport MH, Brun CR, Inglis SD, after endurance exercise during pregnancy. Am J Charlesworth S, Sopper MM. VO2peak prediction and Obstet Gynecol 1990; 163:1805-1811 exercise prescription for pregnant women. Med Sci 24) Clapp JF. Exercise during pregnancy. A clinical Sports Exerc 2006 38(8):1389-95. update. Clin Sports Med 2000; 19: 273-286 39) Borg GAV. Psychophysical bases of perceived 25) Kalisiak B, Spitznagle T. What effect does an exertion. Med Sci Sports Exerc 1982;14:377–81. exercise program for healthy pregnant women have 40) Clark SL, Cotton DB, Lee W, et al. Central on the mother, fetus, and child? PM R 2009; 1: 261-266 hemodynamic assessment of normal term pregnancy. 26) Sigal RJ, Kenny GP, Wasserman DH, Castaneda- Am J Obstet Gynecol 1989;161:1439–42. Sceppa C, White RD. Physical activity/exercise and type 41) Wolfe LA, Ohtake PJ, Mottola MF, et al. 2 diabetes: a consensus statement from the American Physiological interactions between pregnancy and Diabetes Association. Diabetes Care 2006, 29(6):1433-8. aerobic exercise. Exerc Sport Sci Rev 1989;17:295–351. 27) Balducci S, Zanuso S, Nicolucci A, et al.; for the 42) Prowse CM, Gaensler EA. Respiratory and acid- Italian Diabetes Exercise Study (IDES) Investigators. base changes during pregnancy. Anesthesiology 1965; Effect of an intensive exercise intervention strategy on 26:381–92. modifiable cardiovascular risk factors in subjects with 43) Milunsky A, Ulcickas M, Rothman KJ, et al. Maternal type 2 diabetes mellitus - A randomized controlled heat exposure and neural tube defects. JAMA 1992; trial: The Italian diabetes and Exercise Study (IDES). 268:882–5. Arch Intern Med 2010;170:1794-1803 . 44) Soultanakis HN, Artal R, Wiswell RA. Prolonged 28) Larose J, Sigal RJ, Khandwala F, Prud’homme exercise in pregnancy: glucose homeostasis, D, et al.; Diabetes Aerobic and Resistance Exercise ventilatory and cardiovascular responses. Semin (DARE) trial investigators. Associations between Perinatol 1996; 20:315–27. 21
You can also read