Hepatitis C (Acute, Chronic, Perinatal) - NJ.gov
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
Hepatitis C
(Acute, Chronic, Perinatal)
DISEASE REPORTABLE WITHIN 24 HOURS OF DIAGNOSIS
Per NJAC 8:57, laboratories and healthcare providers must report by telephone, confidential fax, over
the Internet using the confidential and secure Communicable Disease Reporting and Surveillance
System (CDRSS), or in writing, all suspected cases of newly diagnosed acute illness of hepatitis C and
newly diagnosed chronic cases of HCV within 24 hours of diagnosis to the NJDOH Infectious and
Zoonotic Diseases Program (IZDP) at 609.826.5964 or fax 609.826.5821.
May 2021Communicable Disease Service Manual
1 THE DISEASE AND ITS EPIDEMIOLOGY
A. Etiologic Agent
Hepatitis C is a liver infection caused by the blood-borne hepatitis C virus (HCV). HCV is an enveloped RNA
virus of the genus Hepacivirus in the Flaviviridae family, with seven distinct genotypes identified. Genotype 1
is the most common HCV genotype in the United States.
B. Clinical Description and Laboratory Diagnosis
Hepatitis C is a disease with varying rates of progression. In general, its course is slowly progressive. For
people with recent (acute) HCV infection, only about 20-30% will experience symptoms. Therefore, it is
uncommon for people to be diagnosed with hepatitis C infection in the acute stage. For people with acute
HCV infection, when symptoms do occur, they may include fatigue, fever, nausea, vomiting, jaundice,
abdominal pain, loss of appetite, dark urine, clay-colored stools, joint pain. The average time from exposure
to symptoms ranges from 2 to 12 weeks. https://www.cdc.gov/hepatitis/hcv/cfaq.htm#overview
Most people with chronic HCV do not have any symptoms or may have common symptoms such as chronic
fatigue and depression. Of those chronically infected, about 5-25% may eventually develop cirrhosis within
10-20 years. Cirrhosis can lead to liver failure or liver cancer. Factors related to developing cirrhosis include
alcohol consumption, being male, age 50 years and older, co-infection with hepatitis B virus, nonalcoholic
fatty liver disease or HIV, or receive immunosuppressive drugs. Approximately 50% of people who test anti-
HCV positive do not have current chronic infection which indicates that they may have experienced
spontaneous clearance after acute infection.
Perinatal hepatitis C in pediatric patients may range from asymptomatic to fulminant hepatitis. While there
are no measures currently recommended for prevention of HCV transmission by pregnant women to their
infants, HCV in pediatric populations can lead to significant illness.
https://wwwn.cdc.gov/nndss/conditions/hepatitis-c-perinatal-infection/case-definition/2018/
There is no one standard HCV screening recommendation for infants born to HCV infected mothers. Available
guidelines consistently recommend against antibody testing for children under 18 months of age, since anti-
HCV immunoglobulin crosses the placenta, confusing results for younger children. However, there are
multiple recommended timelines for HCV ribonucleic acid (RNA) screening of infants born to HCV-infected
mothers. These include not testing until at least 1-2 months of age and, in some cases, recommending repeat
serial testing of infants if the hepatitis C tests positive on one test, if done before 12 months of age. There is
concern that testing outside of recommended parameters may identify transient HCV RNA in infants that
may spontaneously clear the infection following perinatal exposure. The siblings of children with vertically
acquired chronic HCV should be tested for HCV infection, if born from the same mother.
https://www.hcvguidelines.org/unique-populations/children
Laboratory diagnosis is based upon several blood tests which include:
• Screening tests for antibody to HCV (anti-HCV): enzyme immunoassay (EIA), enhanced
chemiluminescence immunoassay (CIA)
• Qualitative tests to detect presence or absence of virus: HCV RNA polymerase chain reaction (PCR), HCV
Genotype
May 2021 1
Hepatitis CNew Jersey Department of Health
• Quantitative tests to detect amount (titer) of virus: HCV RNA PCR.
The Centers for Disease Control and Prevention (CDC) produced an algorithm that outlines the testing
process for HCV diagnosis https://www.cdc.gov/hepatitis/hcv/pdfs/hcv_flow.pdf as well as a table which
interprets the different tests for HCV infection https://www.cdc.gov/hepatitis/hcv/pdfs/hcv_graph.pdf.
HCV infection can be detected by anti-HCV on average 8–11 weeks after infection, but cases of
seroconversion may be delayed in people who are immunosuppressed. HCV RNA can be detected in blood as
early as 1–2 weeks after infection https://www.cdc.gov/hepatitis/hcv/cfaq.htm#overview .
False-positive anti-HCV test results may occur when people at low risk for HCV infection (e.g., blood donors)
are tested. All positive anti-HCV tests should be followed by an RNA test to establish current infection.
False-negative anti-HCV test results may occur in people with early HCV infection who have not yet
developed antibody levels high enough to be detectable with testing. Additionally, some people might not
mount a sufficient immune response to have detectable antibody levels. In these people, further testing with
an HCV RNA test is recommended.
Treatment
Over 90% of people infected with hepatitis C virus (HCV) can be cured of their infection, with 8–12 weeks of
oral therapy regardless of HCV genotype. https://www.cdc.gov/hepatitis/hcv/hcvfaq.htm#section .To
provide health-care professionals with timely guidance as new therapies are available and integrated into
hepatitis C treatment regimens, the Infectious Diseases Society of America (IDSA) and American Association
for the Study of Liver Diseases (AASLD), in collaboration with the International Antiviral Society–USA (IAS–
USA), developed evidence-based, expert-developed recommendations for hepatitis C management. These
recommendations are available at http://www.hcvguidelines.org/
C. Reservoirs
Infected humans are the only known source of this disease.
D. Modes of Transmission
HCV is predominantly spread person-to-person via parenteral exposure to contaminated blood or blood
products. Currently, the most prevalent mode of transmission is through the use of contaminated needles,
syringes and other instruments used for injections and other skin-piercing procedures
https://www.who.int/ith/diseases/hepatitisC/en/ .Before screening for HCV became available in 1992, it was
commonly spread through blood transfusions and organ transplants. Screening has significantly reduced
transmission via these sources.
Other potential risks for transmission include:
• Vertical transmission - infected mother to infant
• Other health-care procedures that involve invasive procedures, such as injections, hemodialysis
• Accidental needlestick injuries in health care settings
• Tattooing or body piercing with non-sterilized equipment
• Sharing straws for intranasal cocaine use
• Sharing personal items contaminated with infectious blood, such as razors or toothbrushes
• Household or sexual contacts with HCV-infected persons
2 Hepatitis C May 2021Communicable Disease Service Manual
HCV is not spread by casual contact, kissing, sneezing, hugging, sharing glasses or utensils, food, water, or
breast milk.
E. Incubation Period
The incubation period for HCV ranges from 2 weeks to 6 months, with an average of 14-84 days.
https://www.cdc.gov/hepatitis/resources/professionals/pdfs/abctable.pdf
F. Period of Communicability or Infectious Period
Persons newly infected with HCV are generally infectious 1 or more weeks before the onset of the first
symptoms; infectivity may persist indefinitely.
G. Epidemiology
Hepatitis C has a worldwide distribution. Globally, an estimated 71 million people have chronic hepatitis C
infection https://www.who.int/news-room/fact-sheets/detail/hepatitis-c .
In the United States an estimated 2.4 million people, 1 % percent of the adult population, were living with
hepatitis C from 2013–2016 https://www.cdc.gov/nchhstp/newsroom/2018/hepatitis-c-prevalence-
estimates-press-release.html . An estimated 50,300 acute hepatitis C cases occurred in 2018 with incidence
of acute HCV increasing over the years. In 2018 that rate was 1.2 reported cases per 100,000 population.
https://www.cdc.gov/hepatitis/statistics/2018surveillance/HepC.htm . HCV infection occurs among all
demographic groups. In 2018, rates of acute hepatitis C increased markedly among those aged 20-39 years
and among males. For acute cases with reported risk factors in 2018, 72% had a history of injection-drug use.
Other reported risk exposures included multiple sex partners, surgery, and needlestick injuries. More than
15,713 death certificates listed HCV as a cause of death in 2018. Perinatal transmission is estimated at about
4-8% of infants born to HCV positive mothers, with the rate being lower if the mother is HCV RNA-negative
but increases to 8-15% if the mother is co-infected with HIV. There is currently no prophylaxis available to
protect infants from infection.
In New Jersey, the estimated number of persons infected with HCV is roughly 680/100,000 people (2013-
2016) https://hepvu.org/local-data/new-jersey/ . In 2018, most of the newly diagnosed cases in New Jersey
were people with newly reported chronic HCV (7,148), rather than acute HCV infection (112). The highest
incidence of acute HCV occurred among persons aged 19 to 30 years (50%), among males (63%) and among
people who inject drugs (49%). Most of the chronic HCV cases reported in 2018 were 31 years and older
(79%).
2 CASE DEFINITIONS
New Jersey Department of Health (NJDOH) follows the CDC’s 2020 updated case definitions for acute and chronic
hepatitis C as well as the new 2018 perinatal HCV case definition.
A. Acute Hepatitis C
https://wwwn.cdc.gov/nndss/conditions/hepatitis-c-acute/case-definition/2020/
i. Clinical Criteria:
May 2021 3
Hepatitis CNew Jersey Department of Health
One or more of the following:
• Jaundice
OR
• Peak elevated total bilirubin levels ≥ 3.0 mg/dL
OR
• Peak elevated serum alanine aminotransferase (ALT) levels >200 IU/L
AND
The absence of a more likely diagnosis (which may include evidence of acute liver disease due to other
causes or advanced liver disease due to pre-existing chronic Hepatitis C virus (HCV) infection or other causes,
such as alcohol exposure, other viral hepatitis, hemochromatosis, etc.).
ii. Laboratory Criteria:
Probable laboratory evidence
• A positive test for antibodies to hepatitis C virus (anti-HCV)
Confirmatory laboratory evidence
• Positive hepatitis C virus detection test: Nucleic acid test (NAT) for HCV RNA positive (including
qualitative, quantitative or genotype testing);
OR
• A positive test indicating presence of hepatitis C viral antigen(s) when available 1.
iii. Epidemiologic Linkage
No epidemiologic linkage is required for case classification.
iv. Case Classification:
Probable
• A case that meets clinical criteria and has presumptive laboratory evidence,
AND
• Does not have a hepatitis C virus detection test reported,
AND
• Has no documentation of anti-HCV or HCV RNA test conversion within 12 months,
Confirmed
• A case that meets clinical criteria and has confirmatory laboratory evidence,
OR
• A documented negative HCV antibody followed within 12 months by a positive HCV antibody test
(anti-HCV test conversion) in the absence of a more likely diagnosis,
OR
• A documented negative HCV antibody OR negative hepatitis C virus detection test (in someone
without a prior diagnosis of HCV infection) followed within 12 months by a positive hepatitis C virus
detection test (HCV RNA test conversion) in the absence of a more likely diagnosis.
1
When and if a test for HCV antigen(s) is approved by the FDA and available.
4 Hepatitis C May 2021Communicable Disease Service Manual
Note: A new probable acute case may be re-classified as confirmed acute case if a positive NAT for HCV RNA or a
positive HCV antigen(s) test is reported within 12 months. A confirmed acute case may be classified as a confirmed
chronic case if a positive HCV RNA NAT or HCV antigen is reported one year or more after acute case onset. A confirmed
acute case may not be reported as a probable chronic case (i.e., anti-HCV positive, but with an unknown HCV RNA NAT
or antigen status), because of previous HCV RNA NAT reported. Report acute cases by date of diagnosis and chronic
cases by year of diagnosis. All hepatitis C virus cases in each classification category should be > 36 months of age, unless
known to have been exposed non-perinatally.
B. Chronic Hepatitis C
https://wwwn.cdc.gov/nndss/conditions/hepatitis-c-chronic/case-definition/2020/
i. Clinical Criteria
No available evidence of clinical and relevant laboratory information indicative of acute infection. Most HCV
infected persons are asymptomatic; however, many have chronic liver disease, which can range from mild to
severe.
ii. Laboratory Criteria for Diagnosis
Probable laboratory evidence
• A positive test for antibodies to hepatitis C virus (anti-HCV)
Confirmatory laboratory evidence
• Positive hepatitis C virus detection test: Nucleic acid test (NAT) for HCV RNA positive (including
qualitative, quantitative, or genotype testing),
OR
• A positive test indicating presence of hepatitis C viral antigen(s) (HCV antigen).
iii. Epidemiologic Linkage
No epidemiologic linkage is required for case classification.
iv. Case Classification
Probable
• A case that does not meet the clinical criteria or has no report of clinical criteria.
AND
• Does not have a documented negative HCV antibody, HCV antigen or NAT laboratory test result
followed within 12 months by a positive result of any of these tests (test conversion) or has no report
of test conversion.
AND
• Has a positive anti-HCV antibody test, but no report of a positive HCV NAT or positive HCV antigen
test.
May 2021 5
Hepatitis CNew Jersey Department of Health
Confirmed
• A case that does not meet the clinical criteria or has no report of clinical criteria.
AND
• Does not have a documented negative HCV antibody, HCV antigen or NAT laboratory test result
followed within 12 months by a positive result of any of these tests (test conversion) or has not
report of test conversion.
AND
• Has a positive HCV NAT or HCV antigen test (may have any anti-HCV antibody test result).
C. Perinatal Hepatitis C
https://wwwn.cdc.gov/nndss/conditions/hepatitis-c-perinatal-infection/case-definition/2018/
i. Clinical Criteria
Perinatal hepatitis C in pediatric patients may range from asymptomatic to fulminant hepatitis.
ii. Laboratory criteria for diagnosis
• HCV RNA positive test results for infants between 2 to 36 months of age.
OR
• HCV genotype test results for infants between 2 to 36 months of age.
OR
• HCV antigen1 test results for infants between 2 to 36 months of age.
iii. Epidemiologic Linkage
Maternal infection with HCV of any duration, if known. Not known to have been exposed to HCV via a
mechanism other than perinatal (e.g. not acquired via healthcare).
iv. Case Classification
Confirmed
Infant who has a positive test for HCV RNA nucleic acid test (NAT), HCV antigen, or detectable HCV genotype
at ≥ 2 months and ≤ 36 months of age and is not known to have been exposed to HCV via a mechanism other
than perinatal.
Note: Test results prior to 2 months of age should not be used for classification. Test results after 36 months of age
should be reported under the 2016 Acute and Chronic HCV Infection case classification and not as perinatal HCV
infection. Cases in the specified age range that are known to have been exposed to HCV via healthcare and not
perinatally should be reported under the 2016 position statement. Event date should be based on earliest relevant
laboratory test date within the 2-36-month window. All hepatitis C virus cases in each classification category should be >
36 months of age, unless known to have been exposed non-perinatally.
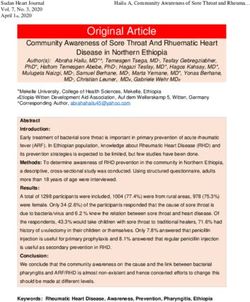
D. Case Classification Summary
After investigation of a reported Hepatitis C case has been completed the case should be assigned a Disease
Group and Case Status as shown in Table 1.
6 Hepatitis C May 2021Communicable Disease Service Manual
v. Table 1. HCV Case Classification Assignments
Disease Subgroup Case Status Evidence of Jaundice or HCV RNA NAT / Positive HCV
Bili > 3 or Alt > 200 AND Genotype Antibody only
absence of a more likely
diagnosis OR
documentation of
negative HCV Antibody or
NAT test within the past
12 months
Chronic Confirmed No Positive No
Chronic Probable No Unknown/Not reported Yes
Acute Confirmed Yes Positive No
Acute Probable Yes Unknown/Not reported Yes
Perinatal Confirmed Not Applicable Positive No
Pending Not a Case No Negative No
3 LABORATORY TESTING
The NJDOH Public Health and Environmental Laboratories (PHEL) do not provide routine HCV antibody
testing. Testing is widely available at clinical and commercial laboratories. Molecular sequencing (genetic
typing) may be performed in response to an outbreak after consultation with NJDOH Communicable Disease
Service (CDS) staff.
4 PURPOSE OF SURVEILLANCE AND REPORTING REQUIREMENTS
A. Purpose of Surveillance and Reporting
1. To identify persons infected with HCV to ensure that they are educated on the need for medical
evaluation to reduce disease progression and to provide referrals to support services.
2. To identify cases and determine the incidence and prevalence of HCV in specific populations and
geographic locations to better inform HCV prevention and service activities.
3. To provide information to persons infected with HCV on how to prevent exposing others.
4. To identify outbreaks.
5. To identify new risk factors for transmission of HCV.
B. Laboratory and Healthcare Provider Reporting Requirements
NJAC 8:57-1 et seq. stipulates that laboratories and healthcare providers must report by telephone,
confidential fax, over the Internet using the confidential and secure Communicable Disease Reporting and
Surveillance System (CDRSS), or in writing, all suspected cases of newly diagnosed acute illness of hepatitis C
and newly diagnosed chronic cases of HCV within 24 hours of diagnosis to the NJDOH Infectious and Zoonotic
Diseases Program (IZDP) at 609.826.5964 or fax 609.826.5821.
May 2021 7
Hepatitis CNew Jersey Department of Health
https://njlmn2.njlincs.net/sites/default/files/NJAC-8-57-CommunicableDiseases.pdf
Mailing address:
New Jersey Department of Health
Communicable Disease Service
Infectious and Zoonotic Disease Program
PO Box 369
Trenton, NJ 08625-0369
The report shall contain the reporting laboratory's name, address, and telephone number; the first name, last
name, age, date of birth, sex, race, ethnicity, home address and telephone number of the person tested; the
test performed; the source or type of specimen tested, the date the specimen was collected, and the date of
testing; the test results; and the healthcare provider's name, address, and telephone number.
Note: If a healthcare provider is reporting, ask him or her to inform the patient that someone from the local
health department will be contacting the patient for follow-up.
C. Local Department of Health Reporting Requirements
NJAC 8:57-1 et seq. stipulates that each local health officer must report the occurrence of any suspected case
of HCV. Case reports received by a local health department should be reported to NJDOH, IZDP electronically
via the Internet using CDRSS. Most HCV reports will go directly to NJDOH from labs/healthcare providers, but
some may continue to go to the local health department.
5 CASE INVESTIGATION
A. Forms and Laboratory Reports
A positive hepatitis C test (HCV antibody; HCV RNA NAT, including genotype) reported electronically into
CDRSS or directly to the local health department (LHD) is the primary trigger for investigation of a new case
The LHD should utilize the NJDOH CDS-17 Form to collect case information. The LHD’s initial goal is to
determine if the case is Acute or Chronic hepatitis C. To guide this case classification, the following steps
should be taken on all HCV disease reports received. Note: if the case has been previously reported to CDRSS
and closed as a confirmed case no further investigation is required. To merge a new case to a confirmed
chronic case, reference NJDOH’s case merge document (17). To reduce the investigation load for the
jurisdictions which receive a huge number of HCV disease reports NJDOH classifies cases into priority and
non-priority groups.
The NJDOH identified priority groups are as follows:
• All cases 40 years of age and younger.
• All cases suspected to be acute: that is, with evidence of jaundice, Bili >3 mg/dl, ALT > 200U/L, and
absence of more likely diagnosis.
• All cases suspected to be a seroconversion: that is, positive HCV test within 12 months of a documented
negative HCV test.
8 Hepatitis C May 2021Communicable Disease Service Manual
• All cases with a healthcare associated risk factor: hemodialysis, invasive medical procedures, healthcare
worker, blood, organ, or tissue transplant.
• All pregnant woman and perinatal cases
The LHD should make two attempts to collect information on the CDS- 17 form from the provider who
ordered the hepatitis C test(s). This attempt can be made via phone, fax, email, or letter and should be
documented in the comments section of CDRSS. Information returned on the form should be entered in
CDRSS, as well. Ideally these two attempts should be at least a week apart and within the first 30 days after
the case was reported.
If the attempt to reach the provider is not successful, LHD should make two attempts to collect information
directly from the patient. These attempts can be done via phone or letter. These attempts should also be
documented in CDRSS. Ideally attempts to reach the patient should be done at least a week after provider
contact. Each contact to the patient should be at least a week apart and conducted no later than 60 days
after the case was initially reported. Reassure the patient that all information is kept strictly confidential.
If a response is not received from the physician or patient after all attempts, a final letter should be sent to
the patient asking him/her to contact the health department with the requested information. Reference the
NJDOH HCV letter template. This letter may not be feasible for those located within an institution. In these
cases, LHD can skip this step and proceed with case classification per the HCV Case Classification Algorithm or
Hepatitis C Perinatal Case Classification Algorithm for perinatal cases.
Contact the referring medical facility for additional information if the case is suspected to be acute as
additional information is needed to confirm classification.
Cases determined to have a reported positive hepatitis C serology test within 12 months of a documented
negative HCV test (i.e., seroconversion) and/or has a health care associated risk factor will need additional
investigation and follow up. See below under Healthcare Associated Infection (HAI).
If no response to any attempt is received within 30 days of sending this final letter, the case should be closed
based on existing information in CDRSS per the HCV Case Classification Algorithm or Hepatitis C Perinatal
Case Classification Algorithm for perinatal cases.
The NJDOH identified non-priority cases are as follows:
Cases older than 40 years of age that do not meet the criteria for acute illness or seroconversion, are not
healthcare associated, and are not associated with a pregnancy
The LHD should make a single attempt to collect information on the CDS-17 from the provider who ordered
the testing. This attempt can be made via phone, fax, email, or letter and should be documented in the
comments section of CDRSS. Information returned on the form should be entered in CDRSS. Based on
information received the case should be classified appropriately in CDRSS per the HCV Case Classification
Algorithm. The case should be classified appropriately in CDRSS, based on the information received.
Contact the referring medical facility for additional information if the case is suspected to be acute (i.e.,
determined to have either signs and symptoms, or ALT>200 IU/L) as additional information is needed to
confirm classification.
May 2021 9
Hepatitis CNew Jersey Department of Health
Cases determined to have a reported positive hepatitis C serology test within 12 months of a documented
negative HCV test (i.e., seroconversion) and/or has a health care associated risk factor (hemodialysis, invasive
medical procedures, healthcare worker, blood, organ or tissue transplant) will need additional investigation
and follow up. See below under Healthcare Associated Infection (HAI).
A. Entry into CDRSS
The mandatory fields to be populated in CDRSS include disease, first name, last name, birth date, county,
municipality, gender, race, ethnicity, case status, and report status.
The following table can be used as a reference guide to determine which fields need to be completed for
accurate and complete reporting of HCV. The “Tab” column includes the tabs that appear along the top of
the CDRSS screen. The “Required Information” column provides detailed explanations of what data should be
entered.
CDRSS Fields Required Information
Disease Information (a): • Select the appropriate SUBGROUP based on the appropriate
Disease, Subgroup, classification after investigation is complete. Reference section 2A
Report/Illness Onset Date above.
• Select “Pending” for all new reports for persons >36
months old and “Perinatal” for personsCommunicable Disease Service Manual
can be added to the text box. If the text box is used, check FREE-
TEXT INPUT.
B. Other Reporting/Investigation Issues
1. Case report forms DO NOT need to be mailed to NJDOH as long as mandatory fields in CDRSS indicated
in section 5B are completed.
2. Once an LHD completes its investigation and assigns a report status of “LHD CLOSED,” NJDOH will review
the case. NJDOH will approve the case by changing the report status to “DHSS APPROVED.” At this time,
the case will be submitted to the CDC and the case will be locked for editing. If additional information is
received after a case has been placed in “DHSS APPROVED,” LHDs will need to contact NJDOH to reopen
the case. This should be done only if the additional information changes the case status of the report
3. Every effort should be made to complete the investigation within three months of opening a case.
6 CONTROLLING FURTHER SPREAD
A. Isolation and Quarantine
i. Minimum Period of Isolation of Patient
No restrictions except for exclusion from blood donation and counseling to modify activities to prevent
transmission.
With the large disparity between patients in need of organ transplantation and available donor organs, some
transplant programs are turning to use of organs from HCV infectious donors. In the past, organs from HCV
infectious donors were primarily used in recipients with chronic hepatitis C or discarded. With the advent of
safe and effective HCV direct acting antiviral (DAA) regimens, however, organs from HCV infectious donors
may be considered for use in recipients without HCV infection. https://www.hcvguidelines.org/unique-
populations/organs-from-hcv-viremic-donors
ii. Minimum Period of Quarantine of Contacts
None.
B. Protection of Contacts of a Case
Standard precautions for cases are recommended to prevent exposing others to blood and body fluids.
Immunoglobulin prophylaxis is not effective and is not recommended for contacts of persons who are
infected with HCV.
C. Managing Special Situations
There are no specific regulations regarding HCV infection in daycare, school, or community residential
programs. HCV is not spread via casual contact or through food or water. Provided standard precautions are
maintained, HCV will not be spread to others in these settings. No person who is infected with HCV should be
excluded from attending or working in any of these settings based on his/her HCV infection.
May 2021 11
Hepatitis CNew Jersey Department of Health
Correctional Facility Investigations
The institutions in New Jersey which house confined inmates are mainly Federal, State and County facilities.
HCV disease reports are frequently received from these institutions.
Per NJAC 8:57 regulation, state institutions are required to report communicable diseases directly to NJDOH.
State Correctional Facility cases are investigated by the contracted care group for state facilities. Prison and
jail facilities have procedures in place to notify LHDs when a prisoner is released into their jurisdiction with a
communicable disease. Once an inmate is released and has been relocated into the LHD’s jurisdiction, the
LHD now has an obligation to conduct additional investigations, if necessary.
The LHD is responsible for investigating all non-state prison and jail facilities cases. Investigate as per priority
or non-priority group as explained above.
Hemodialysis
Patients requiring hemodialysis are at high risk for infection because the process of hemodialysis requires
frequent use of catheters or insertion of needles to access the bloodstream
https://www.cdc.gov/dialysis/index.html .In an environment where multiple patients receive dialysis
concurrently, repeated opportunities exist for person-to-person transmission of infectious agents, directly or
indirectly via contaminated devices, equipment and supplies, environmental surfaces, or hands of personnel.
Furthermore, hemodialysis patients have weakened immune systems, which increase their risk for infection,
and they require frequent hospitalizations and surgery which increases their opportunities for exposure to
healthcare associated infections. To reduce transmission of infectious agents, dialysis center in New Jersey
routinely test patients undergoing chronic dialysis and have been proactive about reporting seroconversion
and working with public health officials to determine where breeches may have occurred.
If an HCV case investigation reveals the patient is a current or past recipient of dialysis, this should be
documented in the CDRSS record. Investigation should include date of admission to dialysis facility and HCV
status upon admission. LHD should contact NJDOH to determine if a more in-depth investigation is required.
Injection Safety/Breaches
Injected medicines are commonly used in healthcare settings for the prevention, diagnosis, and treatment of
various illnesses. Unsafe injection practices put patients and healthcare providers at risk of infectious and
non-infectious adverse events and have been associated with a wide variety of procedures and settings.
If an HCV case investigation reveals the patient has had significant medical procedures with no traditional
HCV risk factors, this should be documented in the CDRSS record. LHD should contact NJDOH to determine if
a more in-depth investigation is required.
D. Preventive Measures
The role of the local health department in managing HCV largely is educating persons who are infected on
how to care for themselves and avoid spreading infection to others. Prevention and education include
information on how the disease is transmitted, how to avoid transmitting to others, and how infected
persons can protect themselves from other potential sources of liver damage.
Offer the following information and support to HCV infected persons/cases:
• Provide basic instruction on transmission of HCV and emphasize the need for ongoing medical evaluation.
The person should be referred to their healthcare provider for treatment options.
12 Hepatitis C May 2021Communicable Disease Service Manual
• Educate on the need to completely abstain from alcohol to help protect the liver. If the person needs or
wants support to stop drinking, provide referrals to appropriate treatment or support services.
• Discuss medications that should be avoided (e.g. acetaminophen) as high doses of these can damage the
liver. Infected persons should discuss any medications (including over-the-counter medications) and
dietary supplements and herbs with a healthcare provider before taking them to be certain the
medications will not impair liver function.
• Provide information on the importance of hepatitis A and B immunization. Refer to the NJDOH Hepatitis A
and Hepatitis B Chapters https://www.state.nj.us/health/cd/topics/hepatitis_viral.shtml .
• Discuss sexual transmission of HCV. Indicate that HCV may be transmitted during sex, but that the risk is
low. All contact with blood during sex should be avoided. Emphasize latex barrier protection to prevent the
spread of HCV, as well to prevent the exposure to, and transmission of other pathogens.
• Discuss household transmission of HCV. Household transmission is rare, but to ensure that it does not
happen, the person should not share razors, toothbrushes, nail clippers, or any other item that could be
contaminated with blood.
• Inform the person that they should not be restricted from working, preparing food, or taking part in their
daily activities unless they have specific symptoms that make it difficult to do so.
• There are no recommendations suggesting that persons who are infected with HCV change their exercise
routines or have any dietary restrictions other than avoidance of alcohol.
7 ADDITIONAL INFORMATION
Supporting Hepatitis C documents and resources can be obtained from the New Jersey Department of Health
website Hepatitis C page https://www.state.nj.us/health/cd/topics/hepatitisc.shtml .
REFERENCES
American Association for the Study of Liver Diseases. (2020, August 27). HCV in Children. Retrieved from HCV
Guidance: Recommendations for Testing, Managing, and Treating Hepatitis C:
https://www.hcvguidelines.org/unique-populations/children
American Association for the Study of Liver Diseases. (2020, August 27). Treatment of HCV-Uninfected
Transplant Recipients Receiving Organs From HCV-Viremic Donors. Retrieved from Unique & Key
Populations: https://www.hcvguidelines.org/unique-populations/organs-from-hcv-viremic-donors
Centers for Disease Control and Prevention. (2013). HCV Algorithm. Retrieved January 20, 2021, from
Recommended Testing Sequence for Identifying: https://www.cdc.gov/hepatitis/hcv/pdfs/hcv_flow.pdf
Centers for Disease Control and Prevention. (2013). HCV Graph. Retrieved January 20, 2021, from
Interpretation of Results of Tests for Hepatitis C: https://www.cdc.gov/hepatitis/hcv/pdfs/hcv_graph.pdf
May 2021 13
Hepatitis CNew Jersey Department of Health
Centers for Disease Control and Prevention. (2018, November 6). CDC Estimates Nearly 2.4 Million Americans
Living with Hepatitis C. Retrieved from NCHHSTP Newsroom:
https://www.cdc.gov/nchhstp/newsroom/2018/hepatitis-c-prevalence-estimates-press-release.html
Centers for Disease Control and Prevention. (2018). Hepatitis C, Perinatal Infection. Retrieved January 13,
2021, from National Notifiable Diseases Surveillance System (NNDSS):
https://wwwn.cdc.gov/nndss/conditions/hepatitis-c-perinatal-infection/case-definition/2018/
Centers for Disease Control and Prevention. (2019, April 9). Hepatitis C Questions and Answers for Health
Professionals. Retrieved from Viral Hepatitis: https://www.cdc.gov/hepatitis/hcv/hcvfaq.htm
Centers for Disease Control and Prevention. (2019, May 2). The ABCs of Hepatitis Fact Sheet. Retrieved from
Viral Hepatitis: https://www.cdc.gov/hepatitis/resources/professionals/pdfs/abctable.pdf
Centers for Disease Control and Prevention. (2020, January 27). Dialysis Safety. Retrieved from
https://www.cdc.gov/dialysis/index.html
Centers for Disease Control and Prevention. (2020, July 28). Hepatitis C Questions and Answers for the Public.
Retrieved January 20, 2021, from Viral Hepatitis: https://www.cdc.gov/hepatitis/hcv/cfaq.htm#overview
Centers for Disease Control and Prevention. (2020). Hepatitis C, Acute. Retrieved January 13, 2021, from
National Notifiable Diseases Surveillance System (NNDSS):
https://wwwn.cdc.gov/nndss/conditions/hepatitis-c-acute/case-definition/2020/
Centers for Disease Control and Prevention. (2020). Hepatitis C, Chronic. Retrieved Janaury 13, 2021, from
National Notifiable Diseases Surveillance System (NNDSS):
https://wwwn.cdc.gov/nndss/conditions/hepatitis-c-chronic/case-definition/2020/
Centers for Disease Control and Prevention. (2020, August 28). Viral Hepatitis Surveillance Report 2018 —
Hepatitis C. Retrieved January 20, 2021, from Viral Hepatitis:
https://www.cdc.gov/hepatitis/statistics/2018surveillance/HepC.htm
David L. Heymann, M. (2008). Control of Communicable Disease Manual, 19th Edition. Washington, D.C:
American Public Health Association.
HepVu. (2021). New Jersey. Retrieved from Local Data: https://hepvu.org/local-data/new-jersey/
New Jersey Department of Health. (2018, December 19). Hepatitis C. Retrieved January 15, 2020, from
Communicable Disease Service: https://www.state.nj.us/health/cd/topics/hepatitisc.shtml
New Jersey Department of Health. (2018, July 10). Viral Hepatitis. Retrieved from Communicable Disease
Service: https://www.state.nj.us/health/cd/topics/hepatitis_viral.shtml
New Jersey Learning Management Network. (2019, June 3). Document: N.J.A.C 8:57-1.5. Retrieved January
20, 2021, from Communicable Diseases: https://njlmn2.njlincs.net/sites/default/files/NJAC-8-57-
CommunicableDiseases.pdf
World Health Organization. (2019). Hepatitis C. Retrieved from International travel and health:
https://www.who.int/ith/diseases/hepatitisC/en/
14 Hepatitis C May 2021Communicable Disease Service Manual
World Health Organization. (2021). Hepatitis C. Retrieved from Fact Sheets Detail:
https://www.who.int/news-room/fact-sheets/detail/hepatitis-c
May 2021 15
Hepatitis CNew Jersey Department of Health
8 APPENDICES
A. HCV Case Classification Algorithm
16 Hepatitis C May 2021Communicable Disease Service Manual
*When and if a test for HCV antigen(s) is approved by the FDA and available
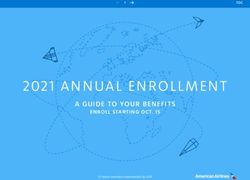
B. Perinatal Hepatitis C Case Classification Algorithm
May 2021 17
Hepatitis CNew Jersey Department of Health
C. Interpretation of Laboratory Test Names in CDRSS
CDRSS Test Name Test Type
Hepatitis C Virus Antibody (Anti-HCV) Antibody test
Hepatitis C Virus Antibody Signal to Cut Off Ratio Antibody test
(S/CO)
Hepatitis C Virus Genotype Nucleic Acid Test (NAT)
Hepatitis C Virus RNA (PCR – Qualitative) Nucleic Acid Test (NAT)
Hepatitis C Virus RNA (PCR – Quantitative) Nucleic Acid Test (NAT)
Alanine Aminotransferase (ALT) Liver function
Serum glutamic pyruvic transaminase (SGPT)
Alkaline Phosphatase (Alk Phos) Liver function
Aspartate Aminotransferase (AST) Liver function
Serum glutamic-oxaloacetic transaminase (SGOT)
Bilirubin Total – Bili (total) Liver function
D. Local Health Department Letter Template
HCV Letter
{Local Health Department Letter}
Date
Patient Name
Patient Address
Dear Mr./Ms. X,
The _____________Health Department has made several attempts to contact you regarding a positive laboratory result that
was received. New Jersey Administrative Code (NJAC 8:57) requires physicians, laboratories, and institutions (e.g., prisons,
long term care, rehabilitation) to report certain communicable diseases to state and local health departments for follow up
and investigation. Please contact our office at the phone number below so we may discuss this matter with you. If you are
not aware of recent positive laboratory result, you may want to contact your healthcare provider prior to contacting our
office.
Thank you,
________Health Department
Phone:
Fax:
Email:
18 Hepatitis C May 2021You can also read