HERE AND NOW: CLINICAL PRACTICE - Hiatal and Paraesophageal Hernias - USA Health System
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
HERE AND NOW: CLINICAL PRACTICE
Charles J. Kahi, Section Editor
Hiatal and Paraesophageal Hernias
James P. Callaway* and Michael F. Vaezi‡
*Division of Gastroenterology and Hepatology, University of Alabama at Birmingham, Birmingham, Alabama; and ‡Division of
Gastroenterology, Hepatology, and Nutrition, Vanderbilt University Medical Center, Nashville, Tennessee
natomically, one of the primary defense mecha- instance, no clinical action other than noting presence of
A nisms to prevent gastroesophageal reflux (GER) is
an intact gastroesophageal junction (GEJ) that is
hernia is indicated. However, the hiatal hernia may lead
to symptoms of GERD, including heartburn, regurgita-
composed of an overlapping lower esophageal sphincter tion, and dysphagia. Hiatal hernias disrupt the normal
and diaphragmatic crus (Figure 1). This barrier, if dis- GEJ reflux barrier, leading to delayed esophageal clear-
rupted, can lead to increased GER and symptoms of ance and increases in acid exposure times3 and persis-
gastroesophageal reflux disease (GERD) including tently abnormal pH/impedance monitoring despite
heartburn, chest pain, regurgitation, and extraesophageal proton pump inhibitor (PPI) therapy.4 This is especially
symptoms of cough or throat soreness. Prolonged or true in those whose heartburn may be resolved on PPI
frequent GER can lead to complications including erosive therapy but continue to have regurgitation as a sign of
esophagitis, Barrett’s esophagus, or stricture formation. mechanical barrier dysfunction. Paraesophageal hernias
The anatomic alignment of the lower esophageal may be asymptomatic but often present with symptoms
sphincter and diaphragmatic crus is believed to of postprandial fullness, nausea, dysphagia, epigastric
contribute to reflux prevention primarily during dynamic pain, and symptoms of GER. Iron deficiency anemia,
situations such as post-deglutition or at times of caused by Cameron lesions or superficial linear ulcers
increased intra-abdominal pressure.1 The principal related to sheer forces from the fundus moving in and
mechanism behind the development of a diaphragmatic out through the diaphragmatic hiatus, is a well-known
hernia, either hiatal or paraesophageal, is a lax diaphrag- presentation for paraesophageal hernias. Less well-
matic hiatus and phrenoesophageal membrane. These known complications include exertional dyspnea from
defects allow for migration of the stomach cranially reduction of thoracic volume or compression on the left
either in an anatomic (hiatal) or non-anatomic (paraeso- atrium.5 An ominous complication of paraesophageal
phageal) fashion and lead to disruption of the typical hernias is its potential to become strangulated and lead
GER barrier. Hiatal hernias account for the majority of to volvulus, ischemia, and potentially gangrene. This is an
diaphragmatic hernias, whereas paraesophageal hernias important clinical consideration in those with large
account for approximately 5%–10%.2 The overall U.S. hernias for whom surgical correction may be recom-
prevalence varies widely from 14% to 84%, depending mended to reduce the likelihood of this complication.
on the detection methods.2 The presence of a hernia should be sought if the appro-
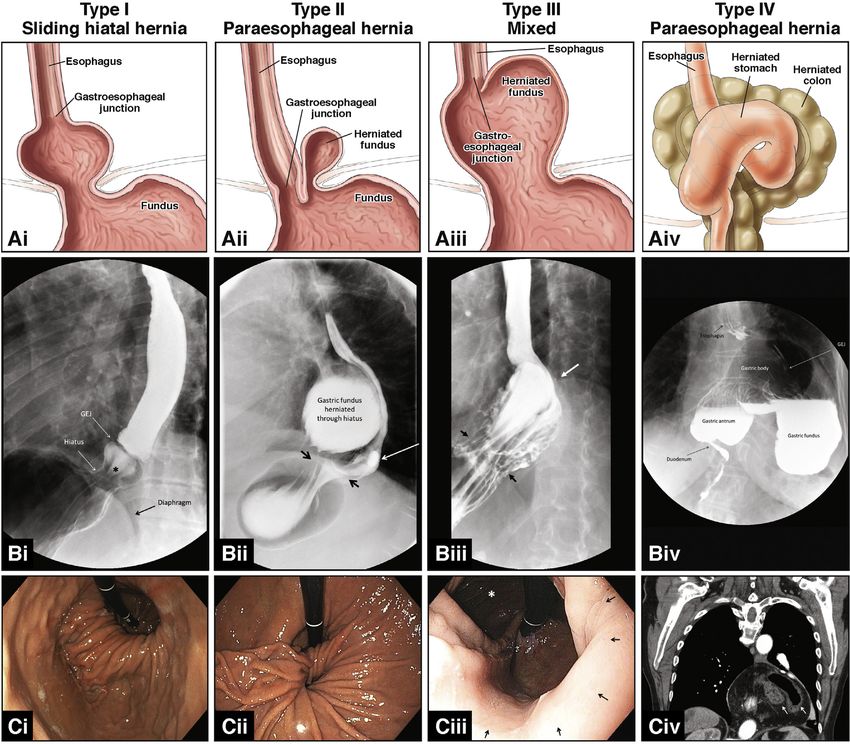
Diaphragmatic hernias are classified as hiatal (type I or priate clinical symptoms are present, especially if typical
“sliding-type”), where the GEJ is displaced cranially above medical therapy for GERD does not resolve the pre-
the diaphragmatic hiatus with a portion of the gastric senting symptoms. A diagnosis can be made with
cardia, or as paraesophageal (types II–IV), where defects numerous modalities, including upper endoscopy, con-
in the phrenoesophageal membrane allow for migration of trasted fluoroscopy, computed tomography, and esoph-
the stomach or other structures adjacent to the GEJ ageal manometry. Each method has advantages and
(Figure 2). In a type II hernia, the GEJ remains at the level disadvantages. Barium esophagography has the advan-
of the diaphragm, but a portion of the gastric fundus tage of providing bolus transit and anatomic information
migrates through the phrenoesophageal membrane into of the hernia, whereas endoscopy can better assess for
the mediastinum. Type III paraesophageal hernias, often mucosal changes including esophagitis, Barrett’s esoph-
referred to as “mixed-type”, have elements of both type I agus, and Cameron lesions. Computed tomography is
and type II where the GEJ is displaced cranially, but there useful in the assessment of type IV paraesophageal
also is a defect in the phrenoesophageal membrane with
accompanying fundic displacement adjacent to the lower
esophageal sphincter. A type IV paraesophageal hernia is Abbreviations used in this paper: GEJ, gastroesophageal junction; GER,
gastroesophageal reflux; GERD, gastroesophageal reflux disease; PPI,
diagnosed when non-gastric structures herniate through proton pump inhibitor.
the phrenoesophageal membrane, including the spleen,
Most current article
colon, small bowel, or pancreas.
© 2018 by the AGA Institute
Clinically, hiatal hernias are often asymptomatic and 1542-3565/$36.00
are frequently encountered on routine endoscopy. In this https://doi.org/10.1016/j.cgh.2017.12.045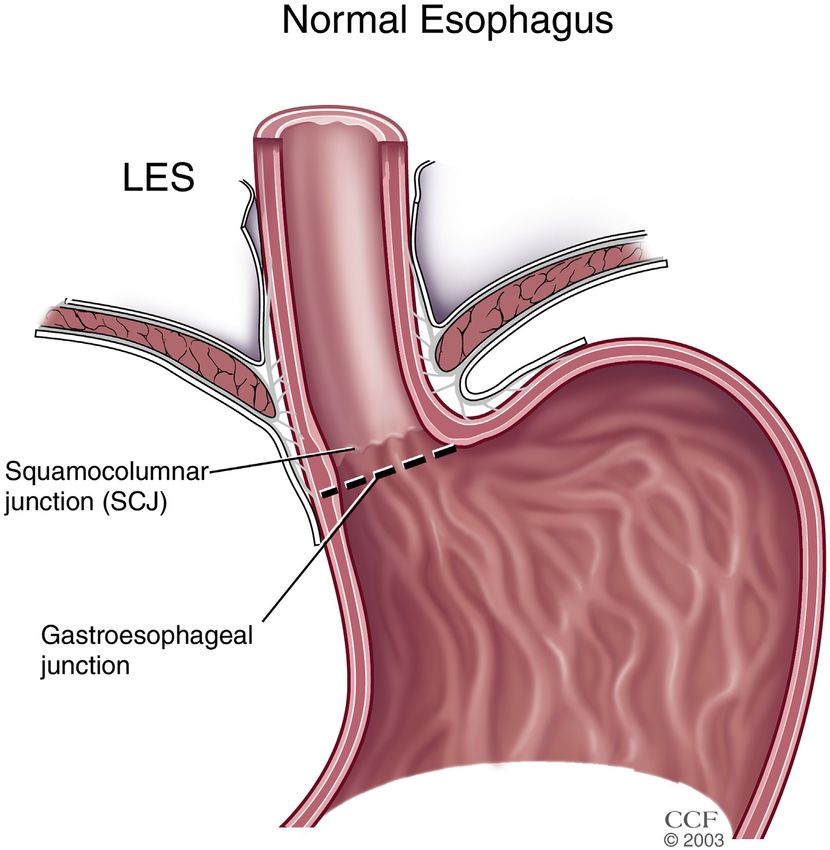
June 2018 Hiatal and Paraesophageal Hernias 811
Figure 1. Normal anatomy.
GEJ within 1 cm of dia-
phragmatic hiatus. LES,
lower esophageal sphincter.
Reprinted with permission
from Vaezi MF. Esophageal
Diseases: An Atlas of
Investigation and Manage-
ment. © Clinical Publishing
Oxford, 2006.
hernias and should be obtained in suspected cases of catheter-based or wireless modalities to document
volvulus or obstruction. Esophageal manometry provides pathologic GER.7 If surgical repair is undertaken, an
a real-time assessment of the anatomic relationship anti-reflux operation (fundoplication) should be offered
between the esophagogastric junction and the dia- by the performing surgeon because dissection of the
phragmatic hiatus and can precisely characterize this phrenoesophageal membrane during hernia repair al-
relationship throughout the dynamic swallow. The clin- lows for hernia recurrence.7 For paraesophageal her-
ical usefulness of this characterization continues to be nias, surgical repair has been historically advocated to
investigated; however, if surgical intervention is consid- potentially prevent the acute, emergent complications of
ered, manometry should be performed in all patients to volvulus and obstruction. As surgical technique has
assess esophageal motility pattern. transitioned from open to laparoscopic approaches and
The fundamental treatment of hiatal hernias with the morbidity and mortality associated with emergent
GER symptoms is acid suppression therapy with PPIs. operations have decreased, routine elective repair of
PPIs are effective at controlling GER symptoms of completely asymptomatic paraesophageal hernia is no
heartburn and chest pain; however, PPIs are less effec- longer the standard.5,7 A watchful waiting approach for
tive for symptoms of regurgitation, especially when asymptomatic patients is more likely to result in greater
provoked by bending/stooping over or with increases in health outcomes compared with elective repair per 2
intra-abdominal pressure. Baclofen, a GABAB receptor separate microsimulation models.8,9 Surgical repair is
agonist and inhibitor of transient lower esophageal re- recommended for type IV hernias and all symptomatic
laxations, is shown to be effective in patients with GERD type II or III paraesophageal hernias, including persis-
and hiatal hernias6; however, common side effects tent iron deficiency anemia or pulmonary symptoms
preclude its widespread utility. Surgical repair of a type that are likely underappreciated.5 Recurrent hiatal
I hernia in the absence of reflux disease is not necessary, hernia after surgical repair is common, occurring in up
and before any consideration for repair, an ambulatory to 48% of patients with a large (>5 cm) initial hernia
pH assessment should be performed with either size.10 Hernias812 Callaway and Vaezi Clinical Gastroenterology and Hepatology Vol. 16, No. 6 Figure 2. Representative images of anatomy (Row A), barium swallow (Row B) and endoscopic views (Row C) of features of Type I or sliding hiatal hernia (Column 1), Type II PEH (Column 2), Type III PEH (Column 3) and Type IV PEH (Column 4). Pane Bi: asterisk – sliding hiatal hernia. Pane Bii: True paraesophageal hernia adjacent to GEJ. Separation between GEJ and dia- phragm noted, consistent with a small adjacent hiatal hernia. (White arrow) Barium tablet present. (Black arrows) Widened hiatus. Pane Biii: White Arrow: Gastroesophageal junction; Black arrows: Widened diaphragmatic hiatus. Pane Biv: Herniated, intrathoracic stomach with herniation of duodenum. This stomach is flipped in an organoaxial rotation. Pane Ci: Sliding hiatal hernia. Pane Cii: Separate PEH present, herniated through laxity in phrenoesophageal membrane. Lax diaphragmatic hiatus also present. Pane Ciii: Image taken from the diaphragmatic hiatus (black arrows). Herniation of GEJ noted with large adjacent fundus/PEH (white asterisk). Pane Civ: Coronal computed tomography (CT) image of an intra-thoracic stomach with herniated loops of colon (white arrows). GEJ, gastroesophageal junction. PEH, paraesophageal hernia. associated with less than 25% chance of recurrence at not respond to typical therapy, especially if regurgitation 3 years.10 The majority of hiatal hernia recurrences or dysphagia is the predominant presentation, surgical are asymptomatic and found incidentally; however, repair should be considered. Paraesophageal hernias are recurrent symptoms can require repeat operation, less common but can also cause symptoms and have the depending on their severity. potential for volvulus or obstruction. Symptomatic type Although the presence of a hiatal hernia predisposes II and III hernias unresponsive to medical therapy should patients to GERD, it can also result in delayed acid be repaired surgically as well as all type IV hernias. A clearance and thus complicated reflux disease in the watchful waiting approach can be considered for form of persistent GER symptoms, stricture formation, asymptomatic paraesophageal hernias. Recurrence of and Barrett’s esophagus. Treatment should be focused on hiatal hernias is common after surgical repair, occurring symptom management with PPIs, and if symptoms do in up to 50%, depending on the initial hernia size; thus,
June 2018 Hiatal and Paraesophageal Hernias 813
the choice for surgical intervention must be approached 6. Beaumont H, Boeckxstaens GE. Does the presence of a hi-
cautiously, with special attention to ensure likelihood of atal hernia affect the efficacy of the reflux inhibitor baclofen
surgical success for the refractory symptoms. during add-on therapy? Am J Gastroenterol 2009;104:
1764–1771.
References 7. Kohn GP, Price RR, De Meester SR, et al. Guidelines for the
management of hiatal hernia. Surg Endosc 2013;27:4409–4428.
1. Kahrilas P. The role of hiatus hernia in GERD. Yale J Biol Med
1999;72:101. 8. Jung JJ, Naimark DM, Behman R, et al. Approach to
asymptomatic paraesophageal hernia: watchful waiting or
2. Dunbar K, Rohan Jeyarajah D. Abdominal hernias and gastric
elective laparoscopic hernia repair? Surg Endosc 2017;32:
volvulus. In: Feldman M, Friedman LS, Brandt LJ, eds.
864–871.
Sleisenger and Fordtran’s gastrointestinal and liver disease.
10th ed. Philadelphia: E Saunders, 2016;407–425. 9. Stylopoulos N, Gazelle GF, Rattner DW. Paraesophageal
hernias: operation or observation? Ann Surg 2002;236:492.
3. Kayaoglu HA. Correlation of the gastroesophageal flap valve
grade with the surgery rate in patients with gastroesophageal 10. Simorov A, Ranade A, Jones R, et al. Long-term patient out-
reflux disease. Surg Endosc 2013;27:801–807. comes after laparoscopic anti-reflux procedures. J Gastrointest
Surg 2014;18:157–163.
4. Becker V, Bajbouj M, Waller K, et al. Clinical trial: persistent
gastro-oesophageal reflux symptoms despite standard therapy
with proton pump inhibitors—a follow-up study of intraluminal-
Reprint requests
impedance guided therapy. Aliment Pharmacol Ther 2007; Address requests for reprints to: James P. Callaway, MD, University of
26:1355–1360. Alabama at Birmingham, BDB 380, 1720 2nd Avenue South, Birmingham, AL
35294. e-mail: jcallaway@uabmc.edu; fax: (205) 975–6201.
5. Lebenthal A, Waterford SD, Fisichella PM. Treatment and con-
troversies in paraesophageal hernia repair. Front Surg 2015; Conflicts of interest
2:13. The authors disclose no conflicts.GASTROENTEROLOGY ARTICLE OF THE WEEK
August 23, 2018
Callaway JP, Vaezi MF. Hiatal and paraesophageal hernias. Clin Gastroenterol Hepatil 2018;16:810‐
813
1. After surgical repair, hiatal hernia recurrence (with or without symptoms) occurs in:
a.You can also read