Highlights of Your UCC Medical and Dental Benefits Plan - For individuals who are not eligible for medicare
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
Highlights of Your UCC Medical and Dental Benefits Plan For individuals who are not eligible for medicare Health Coverage Dental Coverage Vision Coverage
WHERE FAITH & FINANCE INTERSECT Operating at the intersection of faith and finance, we are caring professionals partnering with those engaged in the life of the Church to provide valued services leading to greater financial security and wellness. HEALTH PLAN MISSION To provide the highest standard of service, access to care, and options to active, inactive, and retired UCC clergy and lay employees.

January 2018
Dear UCC Colleague,
We are pleased to provide you with this copy of Highlights of Your UCC Medical and Dental Benefits Plan
(for individuals who are not eligible for Medicare).
The UCC Plans offer a schedule of comprehensive benefits to assist participants in maintaining healthy
lifestyles with an emphasis on preventive care, including immunizations, wellness programs, and chronic
condition management.
Your UCC Plan offers flexibility and choice, including:
• three Health Plan options through Blue Cross Blue Shield that offer various levels of premiums, deductibles,
copays, and benefits;
• a robust schedule of benefits to include all federally-mandated preventive health and essential health benefits
and services;
• Healthy Stewards Wellness Rewards and Member Assistance Programs to help promote physical and mental
health and well-being;
• physician and hospitalization coverage while traveling overseas;
• a pharmacy benefit offering a comprehensive nationwide formulary, low copays, and retail and mail-order
services through Express Scripts, Inc.;
• two Dental Plan options, including a stand-alone entry-level Plan for those not previously enrolled in UCC
dental coverage;
• an optional, stand-alone Vision Plan that does not require participation in the UCC Medical Plan; and
• access to nationwide Preferred Provider Organizations (PPOs) for cost-effective health, dental, and vision
care, as well as the flexibility to use in-network and out-of-network providers.
The Plan continues to benefit from the collective purchasing power made possible by our partnerships with
other denominational health plans through the Church Benefits Association. Participants’ use of in-network
providers, generic medications, and the no-cost preventive care services offered as a way to prevent more
serious health conditions, have a significant impact on Plan-wide basis.
We hope that you continue to be pleased with the benefits available to UCC Plan participants, and covenant
to work with you to provide the best possible benefits at the most effective cost.
May you enjoy good health and abundant blessings.
Best regards,
Brian R. Bodager
President and Chief Executive Officer
Benefits Plan Highlights: Non-Medicare 1CONTENTS
AVAILABLE PLANS 6 HOW THE MEDICAL PLAN WORKS 10
Health Plans 6 Preferred Provider Organization
Dental Plans 6 (PPO)-BlueCard 10
Vision Plan 6 Preexisting Medical Conditions 10
Precertification 10
ELIGIBILITY FOR BENEFITS 7 Centers of Excellence 11
Eligible Employee 7 Blues on Call 11
Eligible Dependents 7 Medical Referrals 12
Applying for Coverage 7 International Medical Care 12
Evidence of Good Health 8 Case Management Services 12
Waiving or Terminating Coverage 8 Maternity Benefits, Education and
When Coverage Starts 8 Support Services 12
When Coverage Ends 8 Women’s Health and Cancer Rights Act 14
Seminary Students 8 Wellness Benefits 15
Coverage While Living Abroad 8 Summary of Benefits: Medical
Military Service 8 Plans Through Highmark
Blue Cross Blue Shield 16
CONTINUATION OF COVERAGE 9 Adult Preventive Schedule 19
Children’s Preventive Schedule 21
What the Medical Plan Does Not Cover 24
2 Benefits Plan Highlights: Non-MedicareHOW THE PRESCRIPTION DRUG PLAN WORKS 27 COORDINATION OF BENEFITS 36
Prescription Drug Benefits-Express Scripts 27 Subrogation 36
Pharmacy Benefit Management 28 Participant’s Cooperation 36
Summary of Benefits: Prescription Drug
Benefits Through Express Scripts 28 YOUR RIGHTS TO APPEAL 37
What the Prescription Plan Does Not Cover 29 First Level 37
Second Level 37
HOW THE DENTAL PLAN WORKS 30
Preferred Provider Organization DEFINITIONS AND RELATED INFORMATION 38
(PPO)–Advantage Plus 2.0 30
Summary of Benefits: Dental Benefits CONTACTS 40
Through United Concordia
Companies, Inc. 32 PRIVACY PRACTICES INSIDE BACK COVER
What the Dental Plan Does Not Cover 33
HOW THE VISION PLAN WORKS 34
Preferred Provider Organization
(PPO)–VSP 34
Summary of Benefits: Vision Benefits
Through VSP 35
Benefits Plan Highlights: Non-Medicare 3ABOUT THIS BOOKLET
The Pension Boards–United Church of Christ, Inc. is pleased to provide you and your family with a
comprehensive health benefits program, offering flexibility and choice. This booklet contains information
about the UCC Medical and Dental Benefits Plan (“the Plan”) and applies to you if you meet the eligibility
requirements stated on p. 7.
In the event of any conflict between this booklet and the UCC Medical and Dental Benefits Plan Document,
the UCC Medical and Dental Benefits Plan Document shall govern.
The UCC Medical and Dental Benefits Plan is designed to support employees of the UCC and UCC-
affiliated entities in performing their ministries. The Plan is self-insured and administered by The Pension
Boards–United Church of Christ, Inc. on behalf of all participants.
This Plan is intended to meet the requirements of a “church plan” within the meaning of Section 414(e) of
the Internal Revenue Code of 1986 (the “Code”), as amended, and Section 3(33) of the Employee Retirement
Income Security Act of 1974 (“ERISA”), as amended. The Plan qualifies as a Section 125 Plan under the
Code. The Plan is exempt from the requirements of Title I of ERISA.
The UCC Medical and Dental Benefits Plan is a “grandfathered health plan” under The Patient Protection
and Affordable Care Act (the “Affordable Care Act”). As permitted by the Affordable Care Act, a
grandfathered health plan can preserve certain basic health coverage that was already in effect when that law
was enacted. Being a grandfathered health plan means that the Plan is not legally required to adopt certain
consumer protections of the Affordable Care Act that apply to other plans; however, the Pension Boards
has voluntarily adopted some, but not all, of these consumer protections. Grandfathered health plans must
comply with certain other consumer protections in the Affordable Care Act; for example, the elimination of
lifetime limits on benefits.
PLAN ADMINISTRATION
The UCC Medical and Dental Benefits Plans are self-funded plans administered by The Pension Boards–
United Church of Christ, Inc., an affiliated ministry of the United Church of Christ. The Pension Boards has
engaged Highmark Blue Cross Blue Shield, Express Scripts, United Concordia Companies, Inc., and VSP to
provide claims administration services. Claims administration services do not insure benefits under the Plan.
Final interpretation of any and all Plan provisions is the responsibility of the Pension Boards. The Pension
Boards is solely responsible for determination of, entitlements to, and payments of any amount due under this
Plan. The Pension Boards retains the right to modify or terminate the Plan at any time.
4 Benefits Plan Highlights: Non-MedicareAbout This Book
YOUR UCC MEDICAL AND DENTAL BENEFITS PLAN COORDINATES ACCESS TO HEALTH CARE
SERVICES THROUGH THE FOLLOWING PREFERRED PROVIDER ORGANIZATIONS
MEDICAL SERVICES
(INCLUDING MENTAL HEALTH AND PHARMACY SERVICES
SUBSTANCE ABUSE SERVICES)
Access through BlueCard, a nationwide Access through Express Scripts, a
network of physicians, hospitals, and ancillary nationwide network of retail pharmacies and
care providers managed by Highmark Blue Mail Order Pharmacy
Cross Blue Shield
DENTAL SERVICES VISION SERVICES
Access through Advantage Plus 2.0, a Access through VSP, a nationwide network of
nationwide network of dental providers vision care providers managed by VSP
managed by United Concordia Companies, Inc.
MEMBER ASSISTANCE PROGRAM
Access through Health Advocate, a leading
clinical health advocacy company to a Licensed
Professional Counselor or Work/Life Specialist
for help with personal, family, and work issues.
Benefits Plan Highlights: Non-Medicare 5Available Plans
AVAILABLE PLANS
You are eligible to participate in the following UCC Plans if you meet the eligibility requirements listed
on p. 7 and are not eligible for Medicare. Information contained in this booklet is also available on our
website at www.pbucc.org.
HEALTH PLANS DENTAL PLANS VISION PLANS
Plan A: A comprehensive Dental 1800: A comprehensive A stand-alone plan available
health plan with the lowest dental plan available to all to eligible employees and
out-of-pocket (deductible and eligible employees and their their eligible dependents to
coinsurance) cost. eligible dependents. The provide coverage for vision
annual benefit maximum is care services.
Plan B: A comprehensive
$1,800 per person.
health plan with mid-level
out-of-pocket (deductible and Dental 750: A comprehensive
coinsurance) cost. dental plan available to
eligible employees and their
Plan C: A comprehensive
eligible dependents who
health plan with the highest
were not covered by the
out-of-pocket (deductible and
UCC Dental Plan when first
coinsurance) cost.
eligible to participate. The
Plan M: This plan is available to annual benefit maximum is
individuals whose eligibility will $750 per person. Participants
be determined by Wider Church in the Dental 750 Plan will
Ministries. transition to the Dental 1800
Plan after one year.
6 Benefits Plan Highlights: Non-MedicareEligibility For Benefits
ELIGIBILITY FOR BENEFITS
You are eligible to participate in the UCC Health Plan if you are a citizen or reside in the United States,
are not eligible for Medicare,* and you are one of the following:
ELIGIBLE EMPLOYEE Your coverage will be transferred to the UCC
• A full-time or part-time minister or lay Medicare Supplement Plan with Rx. If you do
employee who meets the eligibility requirements not enroll for Medicare benefits, you will no
of a church or other UCC-related entity. longer be eligible for benefits through the UCC
Plan. The booklet, Highlights of Your UCC
– I n the event your church does not cover the
Medicare Supplement Plan, is available online at
cost of your coverage, you may do so on a self-
www.pbucc.org or by calling the Pension Boards
pay basis; or
toll-free at 1.800.642.6543.
• Attending a seminary or other institution of
higher education pursuing a degree in theology ELIGIBLE DEPENDENTS
or related discipline; or You may also enroll eligible dependents in the Plan.
Eligible dependents include your:
• A Member in Discernment of a UCC Association
or Conference acting as an Association; or • Spouse
• A non-UCC minister working for a UCC • Same-gender domestic partner
church or UCC-related entity; or
• Opposite-gender domestic partner
• A self-employed UCC minister who may be
• Children
working for a non-UCC employer; or
– Y our natural child(ren) or stepchild(ren) under
• A UCC minister working for another
age 26;
denomination; or
– Natural child(ren) or stepchild(ren) under age
• An Intentional UCC Interim Minister working 26 of your domestic partner, provided your
for a UCC-related entity or a non-UCC employer. domestic partner is enrolled in the Plan;
– Permanently disabled unmarried and
*SPECIAL CONSIDERATION FOR MEDICARE-
unemancipated children age 26 and over if
ELIGIBLE EMPLOYEES WHO ARE ACTIVELY WORKING
the disability began prior to their reaching
• If you continue UCC employment after age 65
age 26, and for whom you provide at least half
and your employer has more than 20 employees,
their support;
the Pension Boards recommends that you do not
– Children under age 26 for whom you can
sign up for Medicare Part B at this time; however
provide documentation of adoption or
you must enroll in Medicare Part A. The UCC
guardianship (including a child for whom legal
(Non-Medicare) Plan will remain the primary
adoption proceedings have been started);
insurer until you retire, terminate employment
– Children for whom you are required to provide
with the UCC, or terminate your medical benefit
medical care through a Qualified Medical
coverage through the UCC Health Plan.
Child Support Order (QMCSO).
• I f you continue UCC employment after age
65 and your employer has fewer than 20 APPLYING FOR COVERAGE
employees, you will be required to enroll in You may apply for coverage for yourself and your
Medicare Parts A and B in order to maintain eligible dependent(s) by filing a Medical Benefits
eligibility for benefits under the UCC Plan. Enrollment Application with the Pension Boards
Benefits Plan Highlights: Non-Medicare 7Eligibility For Benefits
within 90 days of your initial eligibility to WHEN COVERAGE ENDS
participate in the UCC Medical and Dental Coverage for you and your dependent(s) will end
Benefits Plan. You must apply for employee when contributions are no longer paid, or on
coverage in order to apply for dependent coverage. the last day of the month in which you or your
dependent(s) are no longer eligible for coverage.
If you do not have a dependent when you are first
enrolled in the Plan, you must apply for dependent Coverage for your spouse or domestic partner will
coverage within 90 days of the birth, adoption, or end when your coverage ends or when they no
placement of child in your care, or within 90 days longer qualify as your eligible dependent.
of your marriage. You must apply for coverage for
Your adult children cease to be eligible for coverage
your domestic partner within 90 days of the six-
at the end of the month they turn 26.
month anniversary of the commencement of your
domestic partnership.
SEMINARY STUDENTS
You may apply for such coverage at a later date, Plan participation for seminary students is
but satisfactory evidence of good health must be permitted for up to four years while you are a
provided before coverage can begin. full-time student pursuing your first ministerial
degree or for up to three years as a full-time student
EVIDENCE OF GOOD HEALTH seeking an advanced degree. At the end of the
Evidence of good health must be provided if you stated time limit, you may continue coverage under
and/or your dependent(s) are not enrolled in the this Plan if you begin employment with a UCC
Plan within the first 90 days of initial eligibility. church or UCC-related entity.
Plan participation may be denied on health status
Once a year (during the Fall semester), seminary
after the first 90 days of eligibility.
students may enroll in the Plan without having to
provide evidence of good health.
WAIVING OR TERMINATING COVERAGE
If you choose to waive or terminate your coverage
COVERAGE WHILE LIVING ABROAD
(or coverage is terminated or waived by your
Your coverage may be continued if you live outside
employer), you and your dependent(s) will not be
the United States while on sabbatical, church
eligible for future coverage under this Plan without
business, or business for a UCC entity. Dependents
first providing evidence of good health.
who normally live with you in the United States and
move to another part of the world will be eligible for
WHEN COVERAGE STARTS
Plan coverage for up to one year. This does not apply
UCC Health Plan coverage for you and your eligible
to participants in Plan M, whose eligibility will be
dependent(s) begins on the first day of the month
determined by Wider Church Ministries.
following receipt of your enrollment application if you
apply for coverage within the 90-day eligibility period.
MILITARY SERVICE
Newborn children are covered on the date of birth If you are called to military service while enrolled
if you have properly notified the Pension Boards. in the Plan, you will be eligible for coverage upon
You must notify the Pension Boards within 90 days return to your UCC-related employment. You must
following the birth; otherwise evidence of good re-enroll within 90 days of your return. You may
health will be required in order to add your child to re-apply for coverage at a later date but satisfactory
your coverage. evidence of good health must be provided before
coverage can begin.
8 Benefits Plan Highlights: Non-MedicareContinuation of Coverage
CONTINUATION OF COVERAGE
If your coverage ends because you are no longer If you divorce or dissolve your domestic partnership,
employed, you may continue Plan coverage for up to your spouse or domestic partner may continue their
24 months by making contributions directly to the coverage by making contributions directly to the
Plan. Should you gain employment of 20 or more Plan. The duration of this coverage is limited to 24
hours per week prior to the 24-month limit, you months or, if earlier, until 90 days after they become
may continue Plan coverage for up to 90 days after employed for 20 or more hours per week.
such employment begins. However, the 90 days may
For all other events that cause a loss of coverage,
not extend beyond the 24-month overall limit.
dependent children will continue to be covered for
If you retire while participating in the Plan, you up to 24 months.
may continue your coverage as long as you make
If you, your spouse or domestic partner, or dependent
contributions directly to the Plan.
child is or becomes totally disabled (as defined by the
In the event of your death, your spouse or domestic Social Security Act) at any time during the first 60
partner, and dependent child(ren), may continue days of coverage, the continuation of coverage will be
Plan coverage by making contributions directly to extended from 24 months to 29 months.
the Plan.
Benefits Plan Highlights: Non-Medicare 9How the Medical Plan Works
HOW THE MEDICAL PLAN WORKS
To provide participants with quality, cost-effective health benefits, the Pension Boards
has contracted for the following services:
PREFERRED PROVIDER ORGANIZATION (PPO) – If you receive services from an out-of-network
BLUECARD provider, you may be required to submit your claim
A PPO is a network of physicians, hospitals, to Highmark. Contact Highmark at 1.866.763.9471
laboratories, and other ancillary practitioners that to request a claim form. Complete the form, make a
have agreed to provide services at discounted rates. copy for your records, and mail it to the address on
Use of in-network services is highly encouraged to the form along with your itemized receipt. You may
receive the highest level of coverage. In-network also visit www.pbucc.org to obtain a claim form.
providers are not permitted to bill Plan participants
If your physician or other health care provider is not
for charges in excess of network-allowable fees.
in the BlueCard network, they can contact the local
PPO network access information can be found on
Blue Cross Blue Shield plan serving their area to join.
your identification card.
PREEXISTING MEDICAL CONDITIONS
HEALTH CARE SERVICES – BLUECARD
There are no restricitions for preexisting conditions
PPO THROUGH HIGHMARK BLUE CROSS
for participants in the Plan.
BLUE SHIELD
The Pension Boards–United Church of Christ,
PRECERTIFICATION
Inc. has partnered with Highmark Blue Cross Blue
All inpatient hospital services must be precertified
Shield to ensure that you get the medically necessary
through Highmark Healthcare Management
and appropriate care you need from the provider you
Services by calling 1.800.452.8507. If precertification
select. When you or a covered family member needs
is not obtained as required, you will be subject to a
medical care, you can choose between two levels of
$300 penalty that will not be applied toward your
medical care services: in-network or out-of-network.
Plan Year out-of-pocket maximum.
In-network care is care you receive from providers
in the PPO network. Out-of-network care is care
Non-Emergency Admissions–You must notify
you receive from providers who are not in the PPO
Highmark Blue Cross Blue Shield at least 24 hours
network. When you receive services from an out-of-
prior to a non-emergency hospital admission.
network provider, you may be responsible for paying
the difference between the provider’s actual charge
Emergency Hospital Admissions–You must notify
and the Plan’s allowable amount.
Highmark Blue Cross Blue Shield within 48 hours
of an emergency admission.
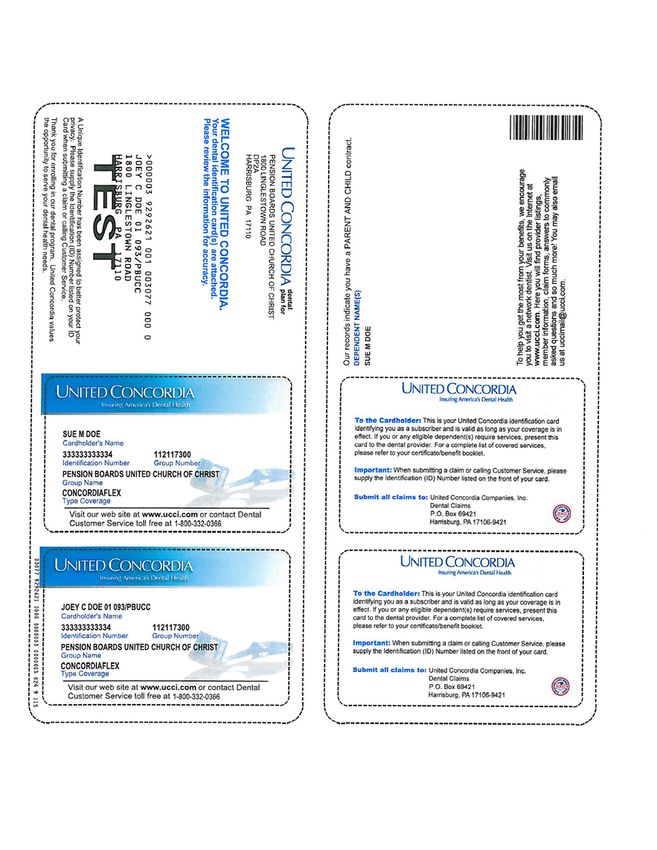
CLAIMS PROCESSING SERVICES
When you use a BlueCard PPO provider, your
You will receive a medical identification card
medical care provider will submit claims directly to
from Highmark Blue Cross Blue Shield for each
their local Blue Cross Blue Shield plan.
member of your family who is enrolled in the
Medical Plan. You may also access an electronic
To find a Highmark Blue Cross Blue Shield
ID card for your smartphone by visiting
BlueCard PPO network provider:
www.highmarkbcbs.com. Log in to your
call 1.866.763.9471
Highmark account for more information.
or
visit www.highmarkbcbs.com
10 Benefits Plan Highlights: Non-MedicareHow the Medical Plan Works
An Explanation of Benefits (EOB) will be mailed to you when claims are processed. An EOB is a summary
of the benefits paid by Highmark to your medical care provider. It lists the date of service, the service
performed, the charges submitted, and the total you may owe the provider according to the Medical Plan
guidelines. You may also visit the Highmark Blue Cross Blue Shield website (www.highmarkbcbs.com) for
more information about receiving electronic EOBs via email.
CENTERS OF EXCELLENCE
Centers of Excellence are part of an overall Blue to access the provider site or determine eligibility,
Cross Blue Shield initiative called Blue Distinction. contact the Highmark Blue Cross Blue Shield
Blue Distinction includes centers for transplant, Customer Service Center at 1.866.763.9471.
bariatric, and cardiac care, and represents
significant enhancements to quality critical care. BLUES ON CALL
Blues on Call is a nurse helpline made available
To obtain precertification for these services, contact
to all Plan participants to answer your medical
Highmark Healthcare Management Services at
care questions. You can reach them by calling
1.800.452.8507. For more information about how
1.888.258.3428.
Benefits Plan Highlights: Non-Medicare 11How the Medical Plan Works
MEDICAL REFERRALS Case managers, physicians, and institutional
No physician referrals are required except in limited providers collaborate to assess your needs and to
instances. If you are unsure whether your procedure plan and coordinate appropriate care options and
will require a referral, call Highmark Blue Cross services. For those with chronic conditions, health
Blue Shield at 1.866.763.9471. coaches offer customized interventions and support,
help you understand your condition and treatment
INTERNATIONAL MEDICAL CARE plan, and address adherence issues and barriers to
The Blue Cross Blue Shield Global Core program care. For those with complex needs related to major
enables you to receive inpatient and outpatient and/or multiple medical issues, Highmark Blue
hospital care and physician services while outside Cross Blue Shield offers case management services
the United States. It includes medical assistance to ensure the most appropriate care is received in the
services and an expanded network of health care most appropriate setting. You may contact Blues on
providers throughout the world. Call at 1.888.258.3428.
If you need assistance finding a foreign provider, CONDITION/DISEASE MANAGEMENT
call 1.800.810.2583. If you are unable to use The Plan provides chronic condition management
the toll-free number, you can call collect at services at no cost through Highmark Blue Cross
1.804.673.1177. A medical coordinator will Blue Shield. The program:
arrange hospitalization if necessary, or make an
• assists in the management of individuals’
appointment with a physician. In an emergency,
total health;
you should go directly to the nearest hospital.
• offers educational resources and materials on a
These services are available 24 hours a day, 365
wide range of diseases or chronic conditions,
days a year, anywhere in the world. There is no
along with access to a personal health coach; and
charge for any referral or coordination help you
need, and any medical services you receive will • identifies individuals for participation based on
be covered in accordance with the Plan limits. To medical and pharmacy claims received from
learn more about Blue Cross Blue Shield Global their providers.
Core, or to access an international claim form,
visit www.bcbsglobalcore.com. See the Summary MATERNITY BENEFITS, EDUCATION, AND
of Benefits (p. 16) for additional information SUPPORT SERVICES
regarding covered medical services. Use Participating Network Providers: Please use
the services of Highmark Blue Cross Blue Shield
Medical evacuation and repatriation of remains are
participating network providers to receive maximum
not covered under this Plan. The Pension Boards
benefits under your health plan. To locate a Blue
recommends you purchase a separate travel policy
Cross Blue Shield participating provider, call
to cover these services.
1.866.763.9471, or visit www.highmarkbcbs.com
and click on Find a Provider. Please have your
CASE MANAGEMENT SERVICES
provider confirm benefit coverage by contacting
The Plan includes case management services
Highmark Blue Cross Blue Shield at 1.866.763.9471.
provided by Blues on Call. These services
provide assistance with chronic or complex Present Your Identification Card: Please
medical care services. remember to present your Blue Cross Blue Shield
Identification card on your first visit to your
12 Benefits Plan Highlights: Non-MedicareHow the Medical Plan Works
provider. Also, please know that your pharmacy • Inpatient maternity services, including labor
benefits are provided under Express Scripts for and delivery room, etc., are covered at 100%
which there is a separate ID card. (after deductible).
Benefits Provided: Listed below are the benefits, • The Plan covers at least 48 hours of
education, and support services included in your hospitalization for a vaginal delivery, and at
Maternity Benefit under the UCC Non-Medicare least 96 hours of hospitalization for a Caesarean
Health Plan. section for both the mother and child.
PREVENTIVE CARE FOR PREGNANT WOMEN – ANTEPARTUM SERVICES
BENEFITS COVERED AT NO COST The Plan covers the following services to determine the
• Gestational diabetes screening health of the baby or if you have a high-risk pregnancy:
• Hepatitis B screening and immunization, if needed • Amniocentesis
• HIV screening • Cordocentesis
• Syphilis screening • Chorionic villi sampling
• Smoking/alcohol cessation counseling • Fetal stress test
• One depression screening for pregnant women • Electronic fetal monitoring
and one for postpartum women
LABOR AND DELIVERY
• Rh typing at first visit The Plan covers medically-necessary services during
your labor and delivery, including anesthesia, fetal
• Rh antibody testing for Rh-negative women
monitoring, and other services required for your care
• Tdap (Tetanus, Diphtheria, Pertussis) vaccine during your stay.
with every pregnancy
The Plan will cover Caesarean section when needed.
• Urine culture and sensitivity at first visit If you choose to have a Caesarean section instead
of vaginal delivery for personal reasons, you may be
• Breastfeeding education
responsible for some of the costs.
MATERNITY BENEFITS
MATERNITY EDUCATION AND SUPPORT
• Prenatal care, including labs, labor and delivery,
Participants who become pregnant can take
hospital stay, postnatal care, and the treatment
advantage of programs available through Highmark
of any pregnancy-related complications are
Blue Cross Blue Shield.
covered.
To enroll in the Baby BluePrints program, call
• Deductibles will vary, depending upon the Plan
1.866.918.5267 for access to the following services:
(A, B, or C) you are enrolled in.
• A welcome package containing a comprehensive
• Prenatal maternity office visits are covered at
maternity guide
100% (copay and deductible do not apply).
• Discounts on important classes and services
• Outpatient maternity services, including labs,
diagnostic services, etc., are covered at 100% • Support/assistance from a health coach
(after deductible).
• Free online classes and educational information
Benefits Plan Highlights: Non-Medicare 13How the Medical Plan Works
• Free gifts throughout the pregnancy, including Q. Can my newborn grandchild be added to my
a pregnancy book of your choice, baby photo health plan coverage?
album, baby dish and cup set, and a book on child A. No. Your grandchild does not qualify as
emergency first aid care a dependent under your coverage unless
he/she has been adopted, or you have begun
BENEFITS NOT PROVIDED
adoption proceedings.
• Non-medically required ultrasounds, including
ultrasounds to determine gender Q. How do I ensure my baby is added to my UCC
Health Plan?
• Private rooms at hospitals where there are shared
A. Please visit our website, www.pbucc.org, to
rooms available
download a copy of the Medical Benefits
• Umbilical cord collection and storage Enrollment Application. You may also obtain
a copy by calling 1.800.642.6543. Return
• Non-medical support during labor and
the completed application with your church
childbirth, such as a doula
or employer’s signature. This should be done
Upon discharge of the mother, future services are as soon as possible, and no later than 90 days
covered at standard Plan benefit levels. Services after the birth. Please also provide the Pension
received by the newborn while the mother remains in Boards with a copy of your child’s birth
the hospital are covered under the maternity benefit. certificate and Social Security card as soon as
they become available.
In the event the newborn remains in the hospital
after the discharge of the mother, services are For additional questions, contact:
covered at standard Plan benefit levels.
Highmark Blue Cross Blue Shield Member Service:
FREQUENTLY ASKED QUESTIONS 1.866.763.9471
Q. In the event of miscarriage, what is the
Pension Boards Health Services Representative:
coverage for a Dilation and Curettage (D&C)
1.800.642.6543, ext. 2870
procedure?
A. A D&C procedure is covered under “Global
WOMEN’S HEALTH AND CANCER RIGHTS ACT
Maternity Benefits.” (Deductible may apply.)
The Women’s Health and Cancer Rights Act of
Q. What coverage is available for abortions? 1998 mandates that all group health plans providing
A. Abortion is a covered benefit as of May 15, coverage for mastectomies also cover:
2017:
• all stages of reconstruction of the breast on which
– A ll elective and voluntary services received the mastectomy was performed;
are covered per Plan policies
• surgery and reconstruction of the other breast to
– Deductibles, copays, and co-insurance may
produce a symmetrical appearance; and
apply
• prostheses and treatment of physical
Q. What if a claim has not been processed per my
complications for all stages of a mastectomy,
Plan benefits?
including lymphedema.
A. Contact a Pension Boards Health Plan
Representative at 1.800.642.6543, or contact The Plan covers mastectomies and, therefore,
Highmark Blue Cross Blue Shield covers the services in the paragraphs above as well.
at 1.866.763.9471. A consultation with your attending physician is
necessary to determine the level of covered services.
14 Benefits Plan Highlights: Non-MedicareHow the Medical Plan Works
WELLNESS BENEFITS After completing the online Wellness Profile and blood
HEALTHY STEWARDS screening, participants will receive a personal score and
Healthy Stewards is the UCC Medical Plan’s health report. All information is kept confidential.
well-being philosophy, rooted in the biblical
PREVENTIVE SERVICES
understanding that we are called to be stewards of
The Plan provides coverage according to the
all our resources, including our health.
schedule recommended by the U.S. Preventive
The Plan offers a well-being improvement program Services Task Force, the Centers for Disease Control
through Highmark Blue Cross Blue Shield that and Prevention, and the American College of
provides participants with free information and tools Obstetricians and Gynecologists. The Plan covers
needed to make positive lifestyle choices. 100% of the cost when in-network providers are
used. When out-of-network providers are used,
The program consists of three components:
the Plan will pay 100% of the Reasonable and
• an online Wellness Profile; Customary (R&C) limit. The participant pays
any charges in excess of the R&C limit. See the
• setting a health goal with a health and wellness
Preventive Schedule (p. 19-23) for more information.
coach or online via WebMD My Health
Assistant; and
• a blood screening test via a home test kit, a
LabCorp voucher, or a physician’s results form.
SUMMARY OF BENEFITS: MENTAL HEALTH AND SUBSTANCE USE CARE THROUGH HIGHMARK
BLUE CROSS BLUE SHIELD
A PPO, or Preferred Provider Organization, offers two levels of benefits. If you receive services from a provider
who is in the PPO network, you’ll receive the higher level of benefits. If you receive services from a provider who
is not in the PPO network, you’ll receive the lower level of benefits. In either case, you coordinate your own care.
Below are specific benefit levels.
Plans A, B, and C Plan M1
Benefit: Mental Health and
Comprehensive
Substance Abuse Treatment Services In-Network Out-of-Network2
Coverage3
Inpatient
Including residential treatment center services 80% after deductible 60% after deductible 85% after deductible
Outpatient
Including office visits, partial hospitalization, and 100% after $25 copayment 60% after deductible 100% after $25 copayment
intensive outpatient services
MENTAL HEALTH AND SUBSTANCE ABUSE CARE FOOTNOTES:
1. Eligibility for Plan M will be determined by Wider Church Ministries.
2. Benefit payments are based on Reasonable and Customary (R&C) limits.
3. Under the comprehensive benefits program, health care benefits are provided as one integrated
program. These benefits include coverage for hospital services, physician services, and many other
covered services. Most benefits are subject to deductible and coinsurance provisions, which require you
to share a portion of the medical costs.
Benefits Plan Highlights: Non-Medicare 15How the Medical Plan Works
SUMMARY OF BENEFITS: MEDICAL PLANS THROUGH HIGHMARK BLUE CROSS BLUE SHIELD
A PPO, or Preferred Provider Organization, offers two levels of benefits. If you receive services from a
provider who is in the PPO network, you’ll receive the higher level of benefits.
Plan A Plan B
Benefit
In-Network Out-of-Network 2 In-Network Out-of-Netw
Deductible 1
Individual $300 $600 $500 $1,500
Family $600 $1,200 $1,500 $4,500
80% after deductible until out-of- 60% after deductible until out-of- 80% after deductible until out-of- 60% after deductible u
Payment Level/Coinsurance 3 pocket maximum is met; then 100% pocket maximum is met; then 100% pocket maximum is met; then 100% pocket maximum is me
$2,000 Individual $4,000 Individual $5,000 Individual $15,000 Individ
Out-of-Pocket Maximums $4,000 Family $8,000 Family $15,000 Family $45,000 Fami
Annual Maximum 4 No Limit No Limit No Limit No Limit
Physician Office Visits 100% after $25 copayment 5 60% after deductible 80% after deductible 60% after deduc
Preventive Care
Follows Preventive Care Schedule
Adult
Routine physical exams 100% - deductible does not apply 100% - deductible does not apply 100% - deductible does not apply 100% - deductible doe
Eye exam $40 after deductible $40 after deductible $40 after deductible $40 after deduc
Routine gynecological exams,
100% - deductible does not apply 100% - deductible does not apply 100% - deductible does not apply 100% - deductible doe
including a Pap Test
Mammograms, as required 100% - deductible does not apply 100% - deductible does not apply 100% - deductible does not apply 100% - deductible doe
Child
100% - deductible does not apply 100% - deductible does not apply 100% - deductible does not apply 100% - deductible doe
Routine physical exams
Pediatric immunizations 100% - deductible does not apply 100% - deductible does not apply 100% - deductible does not apply 100% - deductible doe
Emergency Room Services 80% after in-network deductible 80% after in-network deductible 80% after in-network deductible 80% after in-network
Ambulance 80% after in-network deductible 80% after in-network deductible 80% after in-network deductible 80% after in-network
Hospital Expenses
80% after deductible 60% after deductible 80% after deductible 60% after deduc
Inpatient 6
Outpatient 80% after deductible 60% after deductible 80% after deductible 60% after deduc
Maternity 100% - copay and deductible 100% - copay and deductible
60% after deductible 60% after deduc
Office Visits do not apply do not apply
Outpatient
100% after deductible 60% after deductible 100% after deductible 60% after deduc
(Labs, diagnostic services, etc.)
Inpatient
100% after deductible 60% after deductible 100% after deductible 60% after deduc
(Labor and delivery room, etc.)
Infertility Counseling, Testing, and
80% after deductible 60% after deductible 80% after deductible 60% after deduc
Treatment 7
Autism Spectrum Disorder 80% after deductible 60% after deductible 80% after deductible 60% after deduc
Medical/Surgical Expenses
80% after deductible 60% after deductible 80% after deductible 60% after deduc
(Except Office Visits)
Gender Identity Services
80% after deductible 60% after deductible 80% after deductible 60% after deduc
Inpatient
Outpatient 100% after $25 copayment 5 60% after deductible 80% after deductible 60% after deduc
Spinal Manipulation/Chiropractic 80% after deductible 60% after deductible 80% after deductible 60% after deduc
Services Limit: $2,000 per person/year Limit: $2,000 per person/year Limit: $2,000 per person/year Limit: $2,000 per per
Diagnostic Services
80% after deductible 60% after deductible 80% after deductible 60% after deduc
(Lab, X-Ray and other tests)
Physical, Speech, Occupational
80% after deductible 60% after deductible 80% after deductible 60% after deduc
Therapy
80% after deductible 60% after deductible 80% after deductible 60% after deduc
Acupuncture 8 Limit: $2,000 per person/year Limit: $2,000 per person/year Limit: $2,000 per person/year Limit: $2,000 per per
80% after deductible 60% after deductible 80% after deductible 60% after deduc
Allergy Testing Limit: 60 tests per person/year Limit: 60 tests per person/year Limit: 60 tests per person/year Limit: 60 tests per pe
Durable Medical Equipment,
80% after deductible 60% after deductible 80% after deductible 60% after deduc
Orthotics, and Prosthetics
100% 100% 100% 100%
Hearing Aids Limit: $3,000 per person/every 3 years Limit: $3,000 per person/every 3 years Limit: $3,000 per person/every 3 years Limit: $3,000 per person
Skilled Nursing Facility Care 80% after deductible 60% after deductible 80% after deductible 60% after deduc
Home Health Care 80% after deductible 60% after deductible 80% after deductible 60% after deduc
Private Duty Nursing 80% after deductible 60% after deductible 80% after deductible 60% after deduc
Hospice 9 80% after deductible 60% after deductible 80% after deductible 60% after deduc
Precertification Requirements 10 Performed by Participant Performed by Participant Performed by Participant Performed by Part
16 Benefits Plan Highlights: Non-MedicareHow the Medical Plan Works
If you receive services from a provider who is not in the PPO network, you’ll receive the lower level of benefits.
In either case, you coordinate your own care. There is no requirement to select a Primary Care Physician
(PCP) to coordinate your care. Below are specific benefit levels. Footnote explanations are located on p. 18.
Plan C Plan M 11
-Network Out-of-Network In-Network Out-of-Network Comprehensive Coverage 12
$500 $1,500 $1,000 $3,000 $200
$1,500 $4,500 $3,000 $9,000 $400
ductible until out-of- 60% after deductible until out-of- 70% after deductible until out-of- 50% after deductible until out-of- 85% after deductible until out-of-pocket
mum is met; then 100% pocket maximum is met; then 100% pocket maximum is met; then 100% pocket maximum is met; then 100% maximum is met; then 100%
00 Individual $15,000 Individual $6,000 Individual $18,000 Individual $2,000 Individual
,000 Family $45,000 Family $18,000 Family $54,000 Family $4,000 Family
No Limit No Limit No Limit No Limit No Limit
fter deductible 60% after deductible 70% after deductible 50% after deductible 100% after $25 copayment
uctible does not apply 100% - deductible does not apply 100% - deductible does not apply 100% - deductible does not apply 100% - deductible does not apply
fter deductible $40 after deductible $40 after deductible $40 after deductible $40 after deductible
uctible does not apply 100% - deductible does not apply 100% - deductible does not apply 100% - deductible does not apply 100% - deductible does not apply
uctible does not apply 100% - deductible does not apply 100% - deductible does not apply 100% - deductible does not apply 100% - deductible does not apply
uctible does not apply 100% - deductible does not apply 100% - deductible does not apply 100% - deductible does not apply 100% - deductible does not apply
uctible does not apply 100% - deductible does not apply 100% - deductible does not apply 100% - deductible does not apply 100% - deductible does not apply
n-network deductible 80% after in-network deductible 70% after in-network deductible 70% after in-network deductible 85% after deductible
n-network deductible 80% after in-network deductible 70% after in-network deductible 70% after in-network deductible 85% after deductible
fter deductible 60% after deductible 70% after deductible 50% after deductible 85% after deductible
fter deductible 60% after deductible 70% after deductible 50% after deductible 85% after deductible
pay and deductible 100% - copay and deductible
60% after deductible 50% after deductible 100% - after copayment
o not apply do not apply
after deductible 60% after deductible 100% after deductible 50% after deductible 85% after deductible
after deductible 60% after deductible 100% after deductible 50% after deductible 85% after deductible
fter deductible 60% after deductible 70% after deductible 50% after deductible 85% after deductible
fter deductible 60% after deductible 70% after deductible 50% after deductible 85% after deductible
fter deductible 60% after deductible 70% after deductible 50% after deductible 85% after deductible
fter deductible 60% after deductible 70% after deductible 50% after deductible 85% after deductible
fter deductible 60% after deductible 70% after deductible 50% after deductible 85% after deductible
fter deductible 60% after deductible 70% after deductible 50% after deductible 85% after deductible
000 per person/year Limit: $2,000 per person/year Limit: $2,000 per person/year Limit: $2,000 per person/year Limit: $2,000 per person/year
fter deductible 60% after deductible 70% after deductible 50% after deductible 85% after deductible
fter deductible 60% after deductible 70% after deductible 50% after deductible 85% after deductible
fter deductible 60% after deductible 70% after deductible 50% after deductible 85% after deductible
000 per person/year Limit: $2,000 per person/year Limit: $2,000 per person/year Limit: $2,000 per person/year Limit: $2,000 per person/year
fter deductible 60% after deductible 70% after deductible 50% after deductible 85% after deductible
ests per person/year Limit: 60 tests per person/year Limit: 60 tests per person/year Limit: 60 tests per person/year Limit: 60 tests per person/year
fter deductible 60% after deductible 70% after deductible 50% after deductible 85% after deductible
100% 100% 100% 100% 100%
per person/every 3 years Limit: $3,000 per person/every 3 years Limit: $3,000 per person/every 3 years Limit: $3,000 per person/every 3 years Limit: $3,000 per person/every 3 years
fter deductible 60% after deductible 70% after deductible 50% after deductible 85% after deductible
fter deductible 60% after deductible 70% after deductible 50% after deductible 85% after deductible
fter deductible 60% after deductible 70% after deductible 50% after deductible 85% after deductible
fter deductible 60% after deductible 70% after deductible 50% after deductible 85% after deductible
ed by Participant Performed by Participant Performed by Participant Performed by Participant Performed by Participant
Benefits Plan Highlights: Non-Medicare 17How the Medical Plan Works
MEDICAL PLAN FOOTNOTES:
1. In-network and out-of-network deductibles cross-accumulate. Excludes prescription drug copayments,
physician office visit copayments, difference paid for brand-name drugs in lieu of available generics,
penalty for failure to precertify hospital admissions, and payments over Reasonable and Customary
(R&C) limits.
2. Benefit payments are based on Reasonable and Customary (R&C) limits.
3. In-network and out-of-network out-of-pocket maximums cross-accumulate. Excludes prescription drug
copayments, physician office visit copayments, difference paid for brand-name drugs in lieu of available
generics, penalty for failure to precertify hospital admissions, and payments over Reasonable and
Customary (R&C) limits.
4. The annual maximum is the total paid in “essential health benefits” from January through December of
each Plan Year.
5. Not subject to deductible.
6. Room and board charges for a semi-private or private room when medically necessary.
7. Treatment includes coverage for the correction of a physical or medical problem associated with infertility.
8. Acupuncture services are covered if medically necessary to treat a diagnosed medical condition and are
provided by a physician (MD, DO), or Doctor of Chiropractic, or a licensed acupuncturist.
9. Hospice services are covered only when under the supervision of a physician.
10. Participant is required to contact Highmark Healthcare Management Services prior to a planned
inpatient admission or within 48 hours of an emergency or maternity-related admission. If this does
not occur and it is later determined that all or part of the inpatient stay was not medically necessary
or appropriate, the patient will be responsible for payment of any costs not covered, plus an additional
$300 penalty.
11. Eligibility for Plan M will be determined by Wider Church Ministries.
12. Under the comprehensive benefits program, health care benefits are provided as one integrated
program. These benefits include coverage for hospital services, physician services, and many other
covered services. Most benefits are subject to deductible and coinsurance provisions, which require you
to share a portion of the medical costs.
18 Benefits Plan Highlights: Non-MedicareHow the Medical Plan Works
2018 Preventive Schedule
ADULT (AGE 19+) PREVENTIVE SCHEDULE
PLAN YOUR CARE: KNOW WHAT YOU NEED AND WHEN TO GET IT
QUESTIONS?
Preventive
PLANorYOURroutine
CARE:care
KNOWhelps us stay
WHAT YOUwell
NEED or AND
findsWHEN
problems
TO GETearly,
IT when they are easier to treat. The preventive
guidelines on this schedule depend on your age, gender, health, and family history. As a part of your health plan,
Call Member
you may be eligible
guidelines on this to receive
schedule some
depend on of these
your preventive
age, gender, benefits
health and with little
family history. toofno
As a part cost
your sharing when usingService
health in-network
providers. Make sure you know what is covered by your health plan and any requirements before you receive any of
in-network providers. Make sure you know what is covered by your health plan and any requirements before you Ask your
these services.
receive any of these services. doctor
Some Some
services andand
services their
theirfrequency
frequency maymay depend
depend ondoctor’s
on your your doctor’s advice.
advice. That’s That’s
why it’s whytoit’s
important talkimportant
with to talk with your
doctoryour
about theabout
doctor services that are
the services right
that are for
right foryou.
you. Log in to your
account
Adults: Ages 19+ Male Female
General Health Care
Routine Checkup* (This exam is not the • Ages 19 to 49: Every 1 to 2 years
work- or school-related physical) • Ages 50 and older: Once a year
Pelvic, Breast Exam Once a year
Screenings/Procedures
Abdominal Aortic Aneurysm Screening Ages 65 to 75 who have ever smoked: One-time screening
Ambulatory Blood Pressure Monitoring
Breast Cancer Genetic (BRCA) Screening
(Requires prior authorization) ovarian cancer risk
Cholesterol (Lipid) Screening • Ages 20 and older: Once every 5 years
• High-risk: More often
Colon Cancer Screening • Ages 50 and older: Every 1 to 10 years, depending on screening test
(Including Colonoscopy) • High-risk: Earlier or more frequently
Certain Colonoscopy Preps • Ages 50 and older: Once every 10 years
With Prescription • High-risk: Earlier or more frequently
Diabetes Screening High-risk: Ages 40 and older, once every 3 years
Hepatitis B Screening High-risk
Hepatitis C Screening High-risk
Latent Tuberculosis Screening High-risk
Lung Cancer Screening Ages 55 to 80 with 30-pack per year history: Once a year for current smokers, or once a
(Requires use of authorized facility) year if currently smoking or quit within past 15 years
Mammogram Ages 40 and older: Once a year including 3-D
Adults: Ages 19+
Osteoporosis (Bone Mineral Density) Ages 60 and older: Once every 2 years
Screenings/Procedures
Screening
Pap Test • Ages 21 to 65: Every 3 years, or annually, per doctor’s advice
• Ages 30 to 65: Every 5 years if combined Pap and HPV are negative
* Routine checkup could include health history; physical; height, weight• and
Ages 65pressure
blood and older: Per doctor’s
measures; body massadvice
index (BMI) assessment; counseling for obesity, fall prevention,
skin cancer and safety; depression screening; alcohol and drug abuse, and tobacco use assessment; and age-appropriate guidance.
Sexually Transmitted Disease (STD) Sexually active males and females
Screenings and Counseling (Chlamydia,
Gonorrhea, HIV and Syphilis)
Immunizations
Chicken Pox (Varicella) Adults with no history of chicken pox: One 2-dose series
* Routine checkup could include health history; physical; height, weight and blood
pressure measures; body
Diphtheria, mass(Td/Tdap)
Tetanus index (BMI) assessment; counseling
• One-time Tdap for obesity, fall
• Td booster every 10 years
prevention, skin cancer, and safety; depression screening; alcohol and drug abuse,
and tobacco use assessment; and age-appropriatecall
guidance.
Member Service to verify that your vaccination provider is in the Highmark network)
For adults with certain medical conditions
Benefits to prevent
Plan meningitis,
Highlights: pneumonia and
Non-Medicare 19
Hepatitis A At-risk or per doctor’s advice: One 2-dose seriesPreventive or routine care helps us stay well or finds problems early, when they are easier to treat. The
Call Member
preventive guidelines on this schedule depend on your age, gender, health and family history. As a part
Service
of your health
How the Medical Plan plan,
Worksyou may be eligible to receive some of these preventive benefits with little to no cost
Adults: Ages 19+
sharing when using in-network providers. Make sure you know what is covered by your health plan and
Ask your
any requirements before you receive any of these services.
Screenings/Procedures doctor
Some services and their frequency may depend on• your
Pap Test doctor’s
Ages 21 advice.
to 65: Every That’s
3 years, why it’sper
or annually, important to
doctor’s advice
talk with your doctor about the services that are right for30you.
• Ages to 65: Every 5 years if combined Pap and HPV are negative Log in to your
• Ages 65 and older: Per doctor’s advice account
Sexually Transmitted Disease (STD) Sexually active males and females
Adults: Ages
Screenings and 19+
Male
Counseling (Chlamydia,
Female
Gonorrhea, HIV and Syphilis)
General Health Care
Immunizations
Routine Checkup* (This exam is not the • Ages 19 to 49: Every 1 to 2 years
Chicken
work- Pox (Varicella)physical)
or school-related •Adults with
Ages 50 andnoolder:
history of chicken
Once a year pox: One 2-dose series
Pelvic, Breast Exam Once a year
Diphtheria, Tetanus (Td/Tdap) • One-time Tdap
• Td booster every 10 years
Screenings/Procedures
Abdominal Aortic Aneurysm Screening Ages 65 to 75Service
call Member who have ever smoked:
to verify that your One-time screening
vaccination provider is in the Highmark network)
For adults with certain medical conditions to prevent meningitis, pneumonia and
Ambulatory Blood Pressure Monitoring To confirm new diagnosis of high blood pressure before starting treatment
Hepatitis
Breast A Genetic (BRCA) Screening
Cancer At-riskmeeting
Those or per doctor’s
specificadvice: One
high-risk 2-doseOne-time
criteria: series genetic assessment for breast and
(Requires prior authorization) ovarian cancer risk
Adults: Ages
Hepatitis
Cholesterol 19+
B (Lipid) Screening •At-risk
Ages 20or per
anddoctor’s advice:
older: Once One
every 3-dose series
5 years
• High-risk: More often
Screenings/Procedures
Human
Colon Papillomavirus
Cancer Screening (HPV)
and Certain •To age50
Ages 26:and
Oneolder:
3-dose series
Once a year
Pap Test • Ages 21 to 65: Every 3 years, or annually, per doctor’s advice
Colonoscopy Preps With Prescription • High-risk: Earlier or more frequently
• Ages 30 to 65: Every 5 years if combined Pap and HPV are negative
Measles, Mumps, Rubella (MMR) One or two doses
Diabetes Screening • Ages 65Ages
High-risk: and older:
40 andPer doctor’s
older, once advice
every 3 years
Sexually Transmitted Disease (STD) Sexually active males and females
Meningitis*and Counseling (Chlamydia,
Screenings At-risk or per doctor’s advice
Hepatitis B Screening High-risk
Gonorrhea, HIV and Syphilis)
Pneumonia High-risk or ages 65 and older: One or two doses, per lifetime
Immunizations
Hepatitis C Screening High-risk
Chicken Pox (Varicella) Adults with no history of chicken pox: One 2-dose series
Shingles (Zoster) Ages 60 and older: One dose
Lung Cancer Screening Ages 55 to 80 with 30-pack per year history: Once a year for current smokers, or once a
(Requires useTetanus
Diphtheria, of authorized facility)
(Td/Tdap) year if currently
• One-time Tdapsmoking or quit within past 15 years
Preventive Drug Measures That Require a Doctor’s Prescription
• Td booster every 10 years
Mammogram Ages 40 and older: Once a year including 3-D (If you have/had cancer or your
Aspirin • Ages 50 to 59
mammogram to reduceannual
is positive, the risk of stroke
MRIs followand heart
your attack benefits)
diagnostic
• Pregnant
call Memberwomen
Service at
to risk forthat
verify preeclampsia
your vaccination provider is in the Highmark network)
Osteoporosis (Bone Mineral Density) Ages 60 and older: Once every 2 years
Folic Acid
Screening Women
For adults planning or capable
with certain medical of conditions
pregnancy:toDaily supplement
prevent containing
meningitis, pneumonia and
.4 to .8 mg of folic acid
Pap Test
Raloxifene Tamoxifen •At-risk
Ages 21forto 65: Every
breast 3 years,
cancer, withoutor annually, per doctor’s
a cancer diagnosis, advice
ages 35 and older
• Ages 30 to 65: Every 5 years if combined Pap and HPV are negative
Hepatitis A At-risk or per doctor’s advice: One 2-dose series
• Ages 65 and older: Per doctor’s advice
Tobacco Cessation Adults who use tobacco products
Sexually
HepatitisTransmitted
(Counseling Disease (STD)
B and medication) Sexually
At-risk oractive males and
per doctor’s females
advice: One 3-dose series
Screenings (Chlamydia, Gonorrhea,
Vitamin D Supplements Ages 65 and older who are at risk for falls
HIV and Syphilis)
Human Papillomavirus (HPV) To age 26: One 3-dose series
* Routine checkup could include health history; physical; height, weight and blood pressure measures; body mass index (BMI) assessment; counseling for obesity, fall prevention,
Low
skin cancer and to depression
safety; Moderate Dose Select
screening; alcohol Generic
and drug abuse, and Ages 40 to
tobacco use75 years with
assessment; and1age-appropriate
or more CVDguidance.
risk factors (such as dyslipidemia, diabetes,
Statin Drugs
Measles, For Prevention
Mumps, of
Rubella (MMR) hypertension,
One or smoking) and have calculated 10-year risk of a cardiovascular event
or two doses
Cardiovascular Disease (CVD) of 10% or greater.
Preventive Care for Pregnant Women
PREV/SCH/G-W-1
Meningitis* At-risk or per doctor’s advice
Screenings and Procedures • Gestational diabetes screening •
Pneumonia • Hepatitis
High-risk orBages
screening
65 andand immunization,
older: • Rhper
One or two doses, antibody
lifetimetesting for
if needed Rh-negative women
• HIV screening • Tdap with every pregnancy
Shingles
* Meningococcal (Zoster)
B vaccine per doctor’s advice. Ages 60 and older: One dose
• Syphilis screening • Urine culture and sensitivity
• Smoking cessation counseling
Preventive Drug Measures That Require a Doctor’s
• DepressionPrescription
screening during pregnancy
Aspirin and postpartum
• Ages 50 to 59 to reduce the risk of stroke and heart attack
Prevention of Obesity, Heart Disease and Diabetes
• Pregnant women at risk for preeclampsia
Folic
AdultsAcid
With BMI 25 to 29.9 (Overweight) Women
• planning or capable of pregnancy: Daily supplement containing
• Recommended lab tests:
and 30 to 39.9 (Obese) Are Eligible For: .4 to .8 mg of folic acid – ALT
Raloxifene Tamoxifen blood
At-risk forpressure measurement
breast cancer, – AST
without a cancer diagnosis, ages 35 and older
• Additional nutritional counseling – Hemoglobin A1c or fasting glucose
Tobacco Cessation Adults who use tobacco products – Cholesterol screening
Adult Diabetes
(CounselingPrevention Program (DPP)
and medication)
Vitamin D Supplements
Applies to Adults Ages 65 andinolder
Enrollment who
certain are atCDC
select riskrecognized
for falls lifestyle change DPP programs for
• Without a diagnosis of Diabetes (does
Low
nottoinclude
Moderate Dose Select
a history Generic
of Gestational Ages 40 to 75 years with 1 or more CVD risk factors (such as dyslipidemia, diabetes,
Statin Drugsand
Diabetes) For Prevention of hypertension, or smoking) and have calculated 10-year risk of a cardiovascular event
Cardiovascular
• Overweight orDisease (CVD)
obese (determined by of 10% or greater.
BMI) and
• Fasting Blood Glucose of 100-125 mg/
dl or HGBA1c of 5.7 to 6.4 percent or
Impaired Glucose Tolerance Test of
140-199mg/dl.
* Meningococcal B vaccine per doctor’s advice.
20 Benefits Plan Highlights: Non-MedicareYou can also read