Idiopathic Left Ventricular Apical Aneurysm in a Sailor With Moderate Transient Chest Pain: A Unique Perspective on an Atypical Presentation in ...
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
MILITARY MEDICINE, 00, 0/0:1, 2023
Idiopathic Left Ventricular Apical Aneurysm in a Sailor With
Moderate Transient Chest Pain: A Unique Perspective on an
Atypical Presentation in the Military Population
LT Michael S. Wilinski, MC, USN; LCDR Ian M. Porter, MC, USN
Downloaded from https://academic.oup.com/milmed/advance-article/doi/10.1093/milmed/usac416/7099420 by guest on 13 April 2023
ABSTRACT Left ventricular (LV) apical aneurysm is a rare condition that carries a high risk of fatal cardiac rupture.
Wall ruptures are an uncommon catastrophic complication after acute transmural myocardial infarction. Rarely is the
rupture only contained by an adherent pericardium or hematoma creating a pseudoaneurysm. This clinical finding calls
for emergent surgical intervention. If no ruptures are detectable and myocardium wall integrity is verified, the diagnosis
of a true aneurysm can be made to be repaired via elective surgery. The etiological differential for a patient with an
LV aneurysm in the setting of normal coronaries and in the absence of prior cardiac surgery remains broad, including
traumatic, infectious, and infiltrative causes. In this case report, we demonstrate an atypical and rare presentation of an
idiopathic LV apical aneurysm in a physically fit, active duty male in the U.S. Navy.
INTRODUCTION CASE REPORT
Left ventricular (LV) aneurysms occur most often as com- The patient is a 25-year-old active duty male U.S. Navy ser-
plications of myocardial infarction, ventricular arrhythmia, vice member of Jamaican descent with a history of migraines
and cardiac arrest.1,2 Other documented etiologies of LV and GERD. He presented to Aviation Medicine sick call clinic
aneurysms include hypertrophic cardiomyopathy, trauma, with an acute complaint of stabbing and left-sided chest pain
Chagas disease,3 myocarditis,4 or sarcoidosis.5 They rarely which awoke him from sleep. He noted that he works days
can be congenital.1 LV aneurysm was first reported in 1951 as an aviation structural mechanic in an environment that
by angiographic evidence.6 Cardiac aneurysm applies to the exposes him daily to high heat and humidity in the hangar
anatomical bulging or outpouching of the weakened myocar- and on flight line duties. Because of a lack of comprehensive
dial wall. The formation of a ventricular aneurysm occurs cardiac evaluation resources at the Aviation Medicine clinic,
when fibrous tissues largely replace a region of infarcted he was directed to the nearest hospital with an emergency
myocardium. Mechanically, the replaced region cannot syn- department, cardiology, and surgical capabilities.
chronize during contraction and herniates outward during The history of the present illness revealed chest pain that
systole6 in a motion abnormality called dyskinesis. The localized to the anterior left lower chest with a 5/10 inten-
dynamic ebb and flow of hydrostatic pressure with the cardiac sity, lasting for 3-4 hours, associated with radiation into the
cycles expands the dyskinetic area and forms a broad-necked, left upper extremity, including tingling in the hands and fin-
thin, circumscribed, fibrous, and noncontractile outpouch- gers. The pain was made worse by deep inspiration and
ing6 ; these patients are at risk of demise because of ventricular cough. Symptoms initially worsened reporting dyspnea at
arrhythmia. Conversely, a pseudoaneurysm is a consequence rest; however, no differences in symptoms were observed
of full-thickness rupture of the myocardial ventricular wall, with positional change. Upon exertion, a burning sensation in
but the defect remains contained by the pericardium and sur- the chest was experienced. Current maintenance medications
rounding hematoma. The hematoma then becomes organized included amitriptyline 50 mg once nightly and as needed and
into fibrous tissue involving no cardiac tissue. This con- sumatriptan 50 mg to prevent and treat migraines. Approxi-
formation predisposes to a high likelihood of fatal rupture mately 1 month prior, he underwent a bilateral mastectomy
completion and thus requires emergent surgery, as opposed for gynecomastia, complicated by recurrent but now resolved
to elective surgery for a true aneurysm. hematoma formation.
He admitted to experiencing similar symptoms of chest
pain approximately 1 year prior but was not evaluated by a
medical professional after symptoms remitted on their own.
Department of Aviation Medicine, Naval Branch Health Clinic Mayport,
Jacksonville, FL 32228, USA
The service member was also stationed onboard a ship pre-
The views expressed in this material are solely those of the authors and do venting him from pursuing evaluation previously. His family
not reflect the official policy or position of the U.S. Army, the U.S. Navy, the history was notable only for his father having cerebral infarc-
U.S. Air Force, the DoD, or the U.S. Government. We are military service tion in his 60s. He endorsed occasional alcohol use—denied
members. This work was prepared as part of our official duties. Title 17 the use of tobacco or illicit drugs.
U.S.C. 105 provides copyright protection.
Vital signs demonstrated that he was non-tachycardic but
Published by Oxford University Press on behalf of the Association of
was also mildly hypertensive with a measured blood pressure
Military Surgeons of the United States 2022. This work is written by (a) US of 167/68. A workup for an acute cardiac syndrome was per-
Government employee(s) and is in the public domain in the US. formed. Physical examination revealed that the patient’s lungs
MILITARY MEDICINE, Vol. 00, Month/Month 2023 1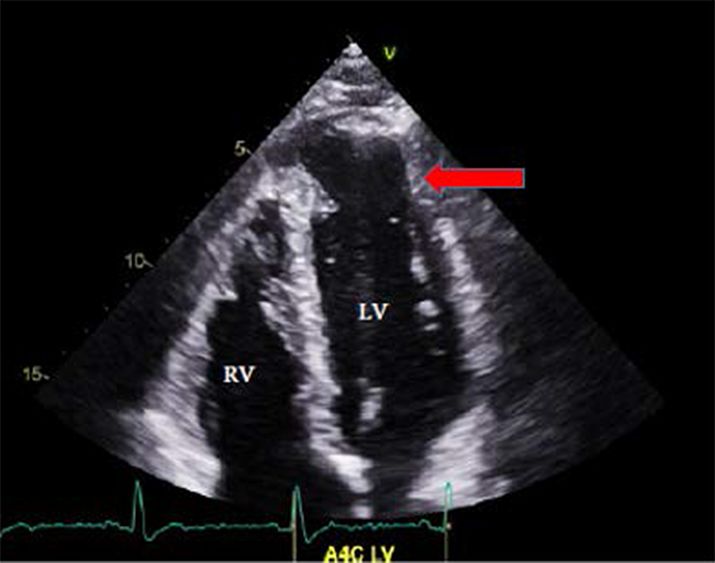
Left Ventricular Aneurysm in Sailor
Downloaded from https://academic.oup.com/milmed/advance-article/doi/10.1093/milmed/usac416/7099420 by guest on 13 April 2023
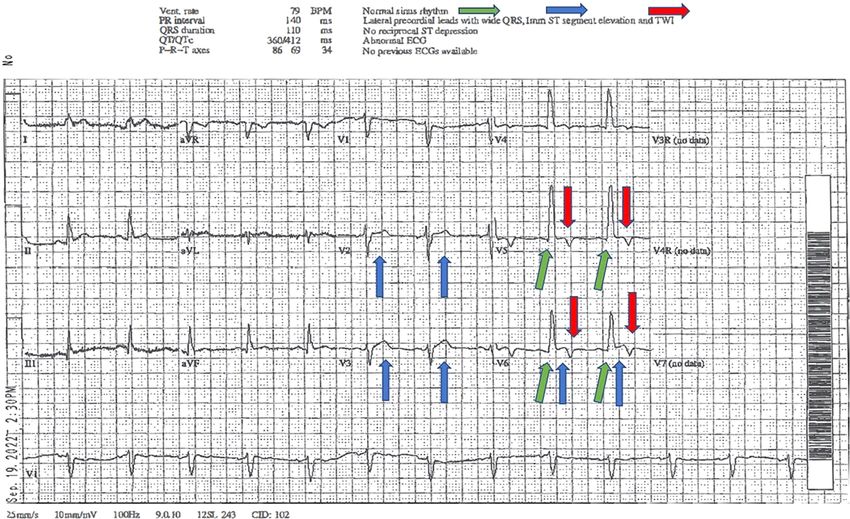
FIGURE 1. Electrocardiogram.
were clear to auscultation bilaterally. Heart sounds demon-
strated a grade 2/6 systolic murmur most consistent with
tricuspid regurgitation. Routine laboratory studies, includ-
ing serial cardiac enzyme, coagulation panel, and D-dimer,
were normal. Portable plain films of the chest revealed the
heart size within normal limits, no focal airspace disease, and
no pneumothorax. An electrocardiogram demonstrated nor-
mal sinus rhythm with mild ST elevation in the anterior lead,
T-wave inversion in the lateral leads, and a widening QRS
complex in the precordial leads (Fig. 1 [Electrocardiogram
(EKG)]). At the bedside, a transthoracic echocardiogram per-
formed by cardiology revealed normal LV size, moderately
reduced LV ejection fraction, estimated at an EF of 40%-45%,
and moderately sized apical aneurysm with a neck of 3.3 cm,
with inability rule out pseudoaneurysm (Fig. 2 [transthoracic
echocardiogram]). This examination also demonstrated addi-
tional findings consisting of mild mitral regurgitation and mild FIGURE 2. Transthoracic Echocardiogram.
anterior akinesis with dyskinesis of the apex.
The sailor was emergently airlifted to a tertiary health care
facility, in the heart of downtown Jacksonville, FL, USA, for and 29.1 mm at the neck of the aneurysm (Fig. 3 [cardiac CT]).
left heart catheterization because of the concern for active Impression described a true aneurysm, not a pseudoaneurysm.
ST-elevation myocardial infarction. Left heart catheterization The thinnest portion of the LV apex was 2 mm. There was no
was completed, with normal coronary arteries found, and the thrombus present within the aneurysm.
patient was admitted to the floor. Following this, a computed Cardiothoracic surgery was promptly consulted, who cor-
tomography angiogram of the heart and lungs was completed, roborated the diagnosis of an LV apical aneurysm. Approx-
confirming normal coronary arteries. This study demonstrated imately 7 days after the admission, the sailor underwent an
a left apical ventricular aneurysm measuring 37.3 mm in depth elective thoracotomy for the performance of plication of the
2 MILITARY MEDICINE, Vol. 00, Month/Month 2023
Left Ventricular Aneurysm in Sailor
Both devices were available to this service member in the local
emergency facility. In the military, particularly in austere set-
tings such as onboard ships and submarines, it is important to
recognize the utility and application of these devices to help
take care of chest pain cases as they arise.
Differentiation between ventricular aneurysms and pseu-
doaneurysms is challenging, requiring a combination of com-
prehensive clinical skill and high-resolution imaging to deter-
Downloaded from https://academic.oup.com/milmed/advance-article/doi/10.1093/milmed/usac416/7099420 by guest on 13 April 2023
mine the proper diagnosis and disposition. In either case, if
any of those diagnoses are suspected, medevac or escalation
of care is warranted.
CONCLUSION
This case demonstrates an atypical and rare presentation of
FIGURE 3. Cardiac CT scan. an idiopathic left apical ventricular aneurysm within the third
decade of life in a relatively healthy active duty male of
Jamaican descent. Heightened clinical suspicion coupled with
LV apical aneurysm. The patient was discharged 6 days after concerning EKG and echocardiogram findings allowed for
surgery without complications. He was immediately started timely transfer, evaluation, and care of this sailor, likely pre-
on 60 days of convalescent leave and has been placed on venting early demise because of this severe acquired cardiac
limited duty to allow for at least 6 months of recovery, malady. We recommend the continued use and availability
postoperatively. of EKG and ultrasound for chest pain and trauma evaluation
patients in the military acute care setting.
DISCUSSION
A review of published military medicine literature revealed
that ventricular aneurysm is a rarely documented topic in ACKNOWLEDGMENTS
active duty service members. This is to be expected in the gen- None declared.
erally young, fit, and relatively good health of this military
population, especially given that the most common associa-
FUNDING
tion of this diagnosis is myocardial infarction. Although there None declared.
are reports describing the onset of LV aneurysm by penetrat-
ing trauma,7 this case rules out active myocardial infarction
and likely represents an otherwise idiopathic etiology because CONFLICT OF INTEREST STATEMENT
of a relatively benign medical history, normal serial troponin None declared.
laboratories upon initial evaluation in the emergency room,
and confirmation by cardiac catheterization. DATA AVAILABILITY
Considering the atypical presentation of this patient’s The data that support the findings of this study are available on request from
case, it is fortuitous that escalation of care in recognition the corresponding author. All data are freely accessible. (A sample list of data
of significant abnormalities in bedside EKG and the ensu- availability statements from Oxford University Press can be found here.)
ing echocardiogram likely captured a condition that would
have portended an early demise. This case demonstrates key
competencies of interpretation of EKG and the value of ultra- CLINICAL TRIAL REGISTRATION
Not applicable.
sound. Serial troponin panels remained within normal limits
but did not dissuade the emergency department from specialist
referral and elevation to higher level care, including an air-lift INSTITUTIONAL REVIEW BOARD (HUMAN
to the catheterization laboratory downtown. SUBJECTS)
The patient’s symptoms of chest pain may have been dis- Not applicable. Consent was obtained from the service member.
missed as GERD-related and transient given his medical his-
tory. His eventual medical disposition to the emergency room
and emergency surgery underscores the importance of taking INSTITUTIONAL ANIMAL CARE AND USE
chest pain complaints in the acute care setting seriously. COMMITTEE (IACUC)
Not applicable.
Additionally, this case illustrates the importance of proper
screening, referral, and access to ancillary testing, such as
EKG and ultrasound as adjuncts in recognizing cardiac dysk- INDIVIDUAL AUTHOR CONTRIBUTION STATEMENT
inesia apparent in both aneurysms and pseudoaneurysms. All authors contributed to the creation and editing of this manuscript.
MILITARY MEDICINE, Vol. 00, Month/Month 2023 3Left Ventricular Aneurysm in Sailor
INSTITUTIONAL CLEARANCE 4. Frustaci A, Chimenti C, Pieroni M: Prognostic significance of
Institutional clearance approved. left ventricular aneurysm with normal global function caused by
myocarditis. Chest 2000; 118(6): 1696–702. 10.1378/chest.118.6.
REFERENCES 1696.
̈
1. Paul M, Schafers M, Grude M, et al: Idiopathic left ventricular aneurysm 5. Kosuge H, Noda M, Kakuta T, Kishi Y, Isobe M, Numano F: Left ven-
and sudden cardiac death in young adults. Europace 2006; 8(8): 607–12. tricular apical aneurysm in cardiac sarcoidosis. Jpn Heart J 2001; 42(2):
10.1093/europace/eul074. 265–9. 10.1536/jhj.42.265.
2. Singh A, Katkov H, Zavoral JH, Sane SM, McLeod JD: Congeni- 6. Sattar Y, and Alraies MC: Ventricular Aneurysm. Treasure Island, FL,
tal aneurysms of the left ventricle. Am Heart J 1980; 99(1): 25–32. StatPearls Publishing; 2022. Available at https://www.ncbi.nlm.nih.gov/
10.1016/0002-8703(80)90311-7. books/NBK555955/; accessed September 25, 2022.
Downloaded from https://academic.oup.com/milmed/advance-article/doi/10.1093/milmed/usac416/7099420 by guest on 13 April 2023
3. Babb DE, Vera-Arroyo A, Rodriquez-Blanco Y, Fabbro M: An unusual 7. Crane AP: Traumatic rupture of the myocardium: report of three
suspect in a case of left ventricular aneurysm. J Cardiothorac Vasc cases. Mil Surg 1952; 110(5): 346–9. 10.1093/milmed/110.
Anesth 2019; 33(8): 2344–8. 10.1053/j.jvca.2019.01.016. 5.346.
4 MILITARY MEDICINE, Vol. 00, Month/Month 2023You can also read