Insulin resistance syndrome as a feature of cardiological syndrome X in non-obese men
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
Downloaded from http://heart.bmj.com/ on October 11, 2015 - Published by group.bmj.com
Br Heart3' 1994;71:41-44 41
Insulin resistance syndrome as a feature of
cardiological syndrome X in non-obese men
Jonathan W Swan, Christopher Walton, Ian F Godsland, David Crook, Michael F Oliver,
John C Stevenson
Abstract abnormalities within the blood or myo-
Objective-To assess the features of the cardium resulting in ischaemia,' and reduced
insulin resistance syndrome in patients blood flow secondary to either microvascular
presenting with cardiological syndrome disease45 or alterations in vasomotor tone.6
X, who experience angina despite angio- Recently, the combination of insulin resis-
graphically normal coronary arteries. tance, hyperinsulinaemia, high plasma triglyc-
Patients and methods-14 Non-obese eride concentration, low high density
male patients with syndrome X and 38 lipoprotein (HDL) cholesterol concentration,
symptom free, apparently healthy, male and raised blood pressure has also, confus-
volunteers were studied. Insulin sensi- ingly, been labelled syndrome X.7 Insulin
tivity (inversely related to insulin resis- resistance seems to underlie these related
tance) was measured by minimal disturbances in risk factors for coronary
modelling analysis of glucose and insulin heart disease and the term insulin resistance
concentrations during an intravenous syndrome may be more appropriate.
glucose tolerance test. Serum lipids, As hyperinsulinaemia has also been impli-
lipoproteins, and apolipoproteins were cated in the pathogenesis of cardiological syn-
also measured. drome X,8 we investigated a group of patients
Results-Insulin sensitivity was 31% with syndrome X angina to see if they had the
lower in the men with syndrome X insulin resistance syndrome.
(p < 0.05) and fasting insulin concentra-
tion was 30% higher (p < 0.05). The
patient group also had 64% higher mean Patients and methods
triglycerides (p < 0.001) and 20% lower PATIENTS
mean high density lipoprotein choles- Fourteen non-obese, white, male patients of
terol concentration (p < 0.01). Systolic mean age 46-6 (range 31-59) years were
blood pressure was also 10% higher in selected after review of cardiac catheterisation
the syndrome X group (p < 0.01). There and case records. All patients reported a his-
were no differences in total cholesterol, tory of chest pain typical of angina pectoris,
low density lipoprotein cholesterol or with electrocardiographic evidence of
lipoprotein (a). ischaemia on exercise but normal coronary
Conclusion-These findings show that arteries at angiography. Coronary arteri-
non-obese male patients with anginal ograms were considered normal if there were
chest pain but normal coronary arteries no stenoses on visual inspection by two expe-
(syndrome X) are insulin resistant, rienced observers. An exercise test was per-
hyperinsulinaemic, and have higher con- formed to the Bruce protocol and considered
centrations of triglycerides and lower positive for ischaemia if ST segment depres-
high density lipoprotein cholesterol than sion > 1 mm developed in any leads at peak
healthy men. The insulin resistance syn- exercise. Patients were excluded if they had
drome may predispose to a spectrum of taken any drugs known to affect lipid or
arterial disease capable of causing carbohydrate metabolism in the previous 6
myocardial ischaemia. months, if there was any evidence of struc-
tural heart disease, or if they deviated by
(Br Heart _j 1994;71:41-44) more than 20% from their ideal body weight
(Metropolitan Life tables9).
Cardiologists use the term syndrome X to CONTROLS
Wynn Institute for refer to patients who present with anginal Thirty eight apparently healthy and clinically
Metabolic Research,
London chest pain, are found to have a positive exer- normal, male, white, volunteers of mean age
J W Swan cise electrocardiogram suggestive of myocar- 47-3 (range 30-60) years were also studied.
C Walton dial ischaemia, but no angiographic evidence They were seen as part of a medical health
I F Godsland
D Crook of atherosclerotic coronary artery disease.' screening programme and none had any
M F Oliver The pathological mechanisms responsible for symptoms suggestive of heart disease.
J C Stevenson
the chest pain in this condition, which was Physical examination and resting electrocar-
Correspondence
Dr J W Swan, Wynn
to:
originally described by Kemp,2 remain diogram were normal in each case. They were
Institute for Metabolic obscure. In the absence of stenoses of a also selected to be within 20% of their ideal
Research, 21 Wellington
Road, London NW8 9SQ.
coronary artery, various theories have been body weight and were taking no medication
proposed to explain the origin of the known to affect lipid or carbohydrate metab-
Accepted for publication
23 August 1993. symptoms. These include biochemical olism.Downloaded from http://heart.bmj.com/ on October 11, 2015 - Published by group.bmj.com
42 Swan, Walton, Godsland, Crook, Stevenson
Table 1 Population characteristics then the HDL, subfraction was measured
Syndrome X Controls after further precipitation with dextran
Age (yr) 46-6 (2 4) 47-3 (1-5)
sulphate.12 The HDL, subfraction was
Height (m) 179 (2.5) 176 (1-2) calculated as the difference between HDL
Weight (kg) 80-0 (2.5) 76-4 (1-4) and HDL,. Low density lipoprotein (LDL)
Body mass index (kg/M2) 24-8 (0.6) 24-5 (0-3)
Systolic blood pressure (mm Hg) 130 (4-0) 118 (2 2) cholesterol was calculated from the
Diastolic blood pressure (mm Hg) 78 (3-0) 75 (1-5) Friedewald formula."3 Apolipoproteins AI and
Current smokers (%) 7 27
Previous smokers (%) 64 60 B were measured by immunoturbidimetry"4
Values are mean (SEM).
and lipoprotein (a) by an enzyme linked
immunosorbent assay (ELISA) method
(Biopool, Sweden).
Table 2 Lipids and lipoproteins
Syndrome X Controls p Value ANALYSIS DATA
Incremental glucose, insulin, and C-peptide
Total cholesterol (mmoIl/) 5-17 (0 26) 5-14 (0-13) NS areas (the area between the fasting concentra-
Triglyceride (mmoll)* 1-56 (+0 26,-0 23) 0-95 (+0-08,-0 07)Downloaded from http://heart.bmj.com/ on October 11, 2015 - Published by group.bmj.com
Insulin resistance syndrome as a feature of cardiological syndrome X in non-obese men 43
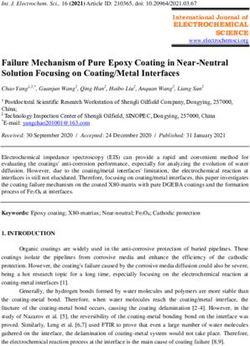
Figure 1 Mean plasma and raised blood pressure compared with
concentration profiles for healthy men. Earlier work has shown that
blood glucose, insulin, and
C-peptide before and after insulin resistance and hyperinsulinaemia are
a 05 glkg intravenous associated with increased plasma triglycerides
glucose load. 20 * Syndrome)
O Controls K]0
E and low plasma HDL cholesterol.'7 18
E
Similarly, a close relation between blood
0
en pressure and insulin resistance has been
10 described in both hypertensive and nor-
FDI motensive persons.'719 It has been suggested
i----ji that the insulin resistance syndrome may be
0
associated with the development of athero-
sclerosis and coronary heart disease.7
600
A recent study has also shown insulin resis-
tance, by the euglycaemic clamp method, in
11 patients with syndrome X compared with
nine controls with non-cardiac chest pain.20
o 400 By contrast with our findings, these authors
E
a failed to show significant differences in serum
cholesterol, triglycerides, HDL cholesterol, or
blood pressure. Mean serum HDL choles-
200
terol concentration was, however, 12% lower
and mean serum triglycerides 14% greater in
the syndrome X group, findings consistent
with the insulin resistance syndrome.
In our study we excluded those with hyper-
2 tension, diabetes, obesity, and other known
insulin resistant states.'9 21 22 Furthermore, the
groups were closely matched for body mass
E index and age, both of which have been
0 reported to affect sensitivity to insulin.23 24
E
-L 1
Smoking has been reported to increase
insulin resistance25 but cannot be responsible
C)
for our findings as there was a similar propor-
tion of previous smokers in each group, with
QL I more current smokers in the control group.
The difference in previous and current smok-
n I II Il .i.., .j
..., ing habits probably reflects clinical advice
30 60 90 120 150 180 given to patients with chest pain. The differ-
Time (min) ence found in insulin resistance is likely to
relate to the diagnosis of syndrome X.
Although our study could not find a causative
role for the insulin resistance syndrome in
of total cholesterol, LDL cholesterol, syndrome X, the similarity of metabolic
apolipoprotein B, or lipoprotein (ax) (table 2). profile between syndrome X and atheroscle-
Fasting plasma glucose coIncentrations rotic coronary heart disease suggests a com-
were similar in both groups despite a mon aetiology or common underlying
significantly higher fasting insulin concentra- pathology.
tion in the syndrome X group (p < 005, The insulin resistance found in these men
table 3). Figure 1 shows plasma concentra- with syndrome X was associated with both
tion profiles for glucose, insuliin, and C- fasting and stimulated hyperinsulinaemia
peptide during the IVGTT. A greater despite a normal fasting blood glucose con-
insulin response was seen in men with centration and normal glucose tolerance. We
syndrome X, but plasma gllucose and divided the hyperinsulinaemic response to
C-peptide responses were similai r. A greater glucose into first phase, representing mainly
second phase response was resrponsible for secretion of stored insulin, and second phase,
TP _
6- - pI- 2
lower in the syndrome X giroup (3 40
C (+O061,-0-56) v 4 95 (+040,-O 38) x 10-5 were no significant differences in either first
min-'/(pmol/l), p < 005, fig 2). or second phase C-peptide response suggest-
ing that increased pancreatic secretion alone
e+ 4o' does not account for the increased insulin
Discussion response in these patients and that altered
These men with cardiological s yndrome X insulin elimination may be contributory.
Figure 2 Insulin have all the characteristic featLares of the Myocardial ischaemia is thought to be a
sensitivity derivedfrom the insulin resistance syndrome: hLyperinsulin- feature of cardiological syndrome X and has
minimal model in men been shown by a number of alternative meth-
with syndrome X and aemia, increased triglyceride conicentrations,
controls. decreased HDL cholesterol conicentrations, ods as well as the exercise electrocardiogramDownloaded from http://heart.bmj.com/ on October 11, 2015 - Published by group.bmj.com
44 Swan, Walton, Godsland, Crook, Stevenson
used in our study. These have included angina ("syndrome X"). Lancet 1991;i:456-7.
9 Metropolitan Life Insurance Company. New weight stan-
reduced coronary perfusion2627 and inducible dards for men and women. Statistical Bulletins and Tables
ischaemia as assessed by production of coro- of the Metropolitan Life Insurance Company 1959;40:1-4.
10 Trinder P. Determination of glucose in blood using glu-
nary sinus lactate.2628 At present, obstructive cose oxidase with an alternative oxygen acceptor. Ann
atheromatous disease has not been shown in Clin Biochem 1969;6:24-7.
11 Warnick GR, Albers JJ. A comprehensive evaluation of the
the coronary arteries of patients with syn- heparin-manganese precipitation procedure for estimat-
drome X. The larger epicardial vessels have, ing high density lipoprotein cholesterol. J Lipid Res
1978;19:65-76.
by definition, been shown to be clear at coro- 12 Gidez LI, Miller GJ, Burnstein M, Slagle S, Eder HA.
nary angiography, and myocardial biopsy has Separation and quantitation of subclasses of human
plasma high density lipoproteins by a simple precipita-
excluded atherosclerosis in the very small tion procedure. J Lipid Res 1982;23: 1206-23.
myocardial vessels.26 29 Neither angiography 13 Friedewald WT, Levy RI, Fredrickson DS. Estimation of
the concentration of low density lipoprotein cholesterol
nor biopsy, however, allows visualisation of in plasma without the use of the preparative ultracen-
the important intermediate size vessels (about trifuge. Clin Chem 1972;18:499-502.
14 Mount JN, Kearney EM, Rosseneu M, Slavin BM.
45-150,um in diameter). These arteries could Immunoturbidimetric assays for serum apolipoproteins
conceivably be the site of atherosclerosis AI and B using Cobas Bio centrifugal analyser. J Clin
Pathol 1988;41:471-4.
responsible for ischaemia and angina in syn- 15 Bergman RN, Ider YZ, Bowden CR, Cobelli C.
drome X. Quantitative estimation of insulin senstivity. Am J
Physiol 1979;236:E667-77.
The finding of myocardial ischaemia in 16 Walton C, Godsland IF, Proudler AJ, Felton C, Wynn V.
syndrome X does not necessarily mean that Evaluation of four mathematical models of glucose and
insulin dynamics with analysis of effects of age and
the chest pain must be caused by obstructive obesity. Am J Physiol 1992;262:E755-62.
coronary atheroma. The most likely cause of 17 Godsland IF, Crook D, Walton C, Wynn V, Oliver MF.
Influence of insulin resistance, secretion, and clearance
ischaemia without coronary atherosclerosis on serum cholesterol, triglycerides, lipoprotein choles-
would be a functional impairment of coro- terol, and blood pressure in healthy men. Arteriosclerosis
Thromb 1992;12: 1030-5.
nary vasodilatation. Insulin resistant states, 18 Modan M, Halkin H, Lusky A, Segal F, Fuchs Z, Chetrit
such as diabetes and hypertension, have been A. Hyperinsulinaemia is characterized by jointly dis-
turbed plasma VLDL, LDL, and HDL levels. A popula-
linked with reduced activity of endothelium tion-based study. Arteriosclerosis 1988;8:227-36.
dependent relaxing factor.3' Insulin has also 19 Swislocki ALM, Hoffman BB, Reaven GM. Insulin resis-
tance, glucose intolerance and hyperinsulinaemia in
been shown to stimulate smooth muscle cell patients with hypertension. Am J Hypertens 1989;2:
proliferation in humans.'2 Such mechanisms 419-23.
20 Botker HE, Moller N, Ovesen P, et al.. Insulin resistance
may contribute to an abnormal vasoconstric- in microvascular angina (syndrome X). Lancet 1993;
tive response in syndrome X leading to 342:136-40.
21 Olefsky JM, Kolterman OG, Scarlett JA. Insulin action
ischaemia. and resistance in obesity and non-insulin dependent
Our data show that syndrome X is an type II diabetes mellitus. Am J Physiol 1982;243:
El 5-30.
insulin resistant state, exhibiting all the fea- 22 Kolterman OG, Insel J, Saekow M, Olefsky JM.
tures of the insulin resistance syndrome. To Mechanisms of insulin resistance in human obesity: evi-
dence for receptor and postreceptor defects. J Clin
what extent these abnormalities relate to the Invest 1980;65:1272-84.
cause of the symptoms remains unknown and 23 Walton C, Godsland IF, Proudler AJ, Felton C, Wynn V.
Effect of body mass index and fat distribution on insulin
is an important area for further investigation. sensitivity, secretion, and clearance in nonobese healthy
men. J Clin Endocrinol Metab 1992;75:170-5.
24 Fink RI, Revers RR, Kolterman OG, Olefsky JM.
JWS is supported by a Bristol-Myers Squibb Cardiovascular Mechanisms of insulin resistance in aging. J Clin Invest
Research Fellowship. We thank Dr Christopher Ley for help 1983;71:1523-35.
with patient recruitment, Mary Miller and Lee Rogers for 25 Facchini FS, Hollenbeck CB, Jeppesen J, Ida Chen Y-D,
assistance with clinical procedures, and Anthony Proudler, Reaven GM. Insulin resistance and cigarette smoking.
Carl Felton, and Melek Worthington for insulin, C-peptide, Lancet 1992;339:1128-30.
and lipoprotein assays. 26 Opherk D, Zebe H, Weihe E, Mall G, Durr C, Gravert B,
et al. Reduced coronary dilatory capacity and ultra-
structural changes of the myocardium in patients with
angina pectoris but normal coronary arteriograms.
1 Anon. Syndrome X. Lancet 1987;ii: 1247-8. Circulation 1981;63:817-25.
2 Kemp HG. Left ventricular function in patients with the 27 Cannon RO, Bonow RO, Bacharach SL, Green MV,
anginal syndrome and normal coronary arteriograms. Rosing DR, Leon MB, et al. Left ventricular dysfunc-
Am J Cardiol 1973;32:375-6. tion in patients with angina pectoris, normal epicardial
3 Mammohanasingh P, Parker JO. Angina pectoris with coronary arteries, and abnormal vasodilator reserve.
normal coronary arteriograms. Haemodynamic and Circulation 1985;71:218-26.
metabolic response to atrial pacing. Am Heart Jf 1975; 28 Boudoulas H, Cobb TC, Leighton RF, Wilt SM.
90:555-61. Myocardial lactate production in patients with angina-
4 Korhola 0, Valle M, Frick MH, Wiljasalo M, Riihimaki like chest pain and angiographically normal coronary
E. Regional myocardial perfusion abnormalities on arteries and left ventricle. Am J Cardiol 1974;34:501-5.
xenon-133 imaging in patients with angina pectoris and 29 Richardson PJ, Livesley B, Oram S, Olsen EG, Armstrong
normal coronary arteries. Am J Cardiol 1977;39:355-9. P. Angina pectoris with normal coronary arteries.
5 Kaul S, Newell JB, Chesler JB, Pohost GM, Okada RD, Transvenous myocardial biopsy in diagnosis. Lancet
Boucher CA. Quantitative thallium imaging findings in 1974;ii:677-80.
patients with normal coronary angiographic findings 30 De Tejada IS, Goldstein I, Azadzoi K, Krane RJ, Cohen
and in clinically normal subjects. Am J Cardiol 1986; RA. Impaired neurogenic and endothelium-mediated
57:509-12. relaxation of penile smooth muscle from diabetic men
6 Sax FL, Cannon RO, Hanson C, Epstein SE. Impaired with impotence. N EnglJ Med 1989;320: 1025-30.
forearm vasodilator reserve in patients with microvascu- 31 Panze JA, Quyyumi AA, Brush JE, Epstein SE. Abnormal
lar angina: evidence of a generalised disorder of vascular endothelium-dependent vascular relaxation in patients
function. N EnglJ Med 1987;317:1366-70. with essential hypertension. N Engl J Med 1990;323:
7 Reaven GM. Banting lecture 1988. Role of insulin resis- 22-6.
tance in human disease. Diabetes 1988;37:1595-607. 32 Pfeifle B, Ditschuneit H. Effect of insulin on growth
8 Dean JD, Jones CJH, Hutchinson SJ, Peters JR, of cultured human arterial smooth muscle cells.
Henderson AH. Hyperinsulinaemia and microvascular Diabetologia 1981;20:155-8.Downloaded from http://heart.bmj.com/ on October 11, 2015 - Published by group.bmj.com
Insulin resistance syndrome as a feature of
cardiological syndrome X in non-obese men.
J. W. Swan, C. Walton, I. F. Godsland, D. Crook, M. F. Oliver and J. C.
Stevenson
Br Heart J 1994 71: 41-44
doi: 10.1136/hrt.71.1.41
Updated information and services can be found at:
http://heart.bmj.com/content/71/1/41
These include:
Email alerting Receive free email alerts when new articles cite this article. Sign up in the
service box at the top right corner of the online article.
Notes
To request permissions go to:
http://group.bmj.com/group/rights-licensing/permissions
To order reprints go to:
http://journals.bmj.com/cgi/reprintform
To subscribe to BMJ go to:
http://group.bmj.com/subscribe/You can also read