Patient Accessibility and Budget Impact of Orphan Drugs in South Korea: Long-Term and Real-World Data Analysis (2007-2019) - MDPI
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
International Journal of
Environmental Research
and Public Health
Article
Patient Accessibility and Budget Impact of Orphan
Drugs in South Korea: Long-Term and Real-World
Data Analysis (2007–2019)
Se Hee Lee 1,† , Seung-Lai Yoo 2,† , Joon Seok Bang 1, * and Jong Hyuk Lee 3, *
1 College of Pharmacy, Sookmyung Women’s University, Seoul 04310, Korea
2 Department of Insurance Benefits, National Health Insurance, Wonju 26464, Korea
3 Department of Pharmaceutical Engineering, Hoseo University, Asan 32499, Korea
* Correspondence: jsbang@sookmyung.ac.kr (J.S.B.); jhyuk@hoseo.edu (J.H.L.); Tel.: +82-2-2077-7526 (J.S.B.);
+82-41-540-9814 (J.H.L.)
† These authors contributed equally to this work.
Received: 6 April 2020; Accepted: 24 April 2020; Published: 26 April 2020
Abstract: This study aimed to identify orphan drug accessibility and impact on pharmaceutical
budgets in South Korea by analyzing the status of orphan drug designation, approval, reimbursement,
and pharmaceutical expenditure. We analyzed the dataset on orphan drugs designated, approved,
and reimbursed from 2007 to 2019 based on long-term real-world data. The designated and
approved orphan drugs were 165 and 156, respectively, and 88 out of 156 approved products were
reimbursed. Total expenditure on orphan drugs increased annually to account for about 1.44% of
total pharmaceutical expenditure in 2018. Orphan drug expenditure per patient increased on average
by 8.7% per year. The average annual cost of orphan drugs was USD 27,000–USD 47,000, with the
maximum value of USD 260,000–USD 560,000. As there are a number of orphan drugs that have not
yet been reimbursable after approval, a reimbursement policy should be established that considers the
characteristics of orphan drugs. Since the rapid increase in orphan drug expenditure can be a potential
threat to the insurance budget, budget management should also be considered. In conclusion, it
is necessary to take preemptive measures to manage the health insurance budget efficiently while
improving patient accessibility to orphan drugs.
Keywords: Orphan drug; rare disease; pharmaceutical expenditure; reimbursement; budget impact;
budget controls; patient accessibility; health services accessibility
1. Introduction
With improvements in medical and diagnostic technology, approximately 6000 to 8000 rare
diseases have been identified, and the number of patients diagnosed with rare diseases has rapidly
increased [1,2]. In addition, unmet needs for therapeutics are increasing as most rare diseases shorten
the patient’s life expectancy by damaging the body and reducing the quality of life (QOL) [2,3]. Since the
Orphan Drug Act was introduced in the United States (US) in 1983, most developed countries, including
countries in the European Union (EU) and Japan, have enacted orphan drug (OD) legislation, which
includes orphan drug designation, marketing approval, post-marketing monitoring, and financial
incentives [1,4–6]. Moreover, the identification of many rare diseases and development of biotechnology
promote research and development (R&D) and marketing approval of ODs [2,4,7,8]. Most rare diseases
are characterized by high severity, low prevalence, and no alternative treatments, making it difficult
to prove the safety and efficacy of ODs as it requires a longer time and higher R&D cost for clinical
trials [9]. Due to high price and the small number of patients, pharmaceutical expenditure per patient
is very high, and the total budget impact of individual ODs is relatively low [5,6,10,11]. However,
Int. J. Environ. Res. Public Health 2020, 17, 2991; doi:10.3390/ijerph17092991 www.mdpi.com/journal/ijerphInt. J. Environ. Res. Public Health 2020, 17, 2991 2 of 8
as the number of OD products increases and their impact is gradually increasing, policy makers are
facing difficulties in decisions concerning reimbursement and pricing [1,5,6,10]. Due to the high price
and uncertainty of clinical outcomes, in countries where a health technology assessment (HTA) system
is applied, patients may not be treated with ODs at a suitable time because reimbursement is not
available without proof of cost-effectiveness [2,7]. This means that even if marketing approval is
successful by making a lot of effort, failure of reimbursement can result in social losses, as patients
lose treatment opportunities and pharmaceutical companies fail to retrieve R&D costs. Therefore,
stakeholders, including policy decision makers, should continuously monitor the impact of ODs on
the overall budget to manage patient accessibility and financial risk related to ODs appropriately.
The situation of OD-related legislation and reimbursement in South Korea is similar to that of
other countries. In South Korea, financial incentives are provided for R&D activation of OD, and
various benefits are provided in terms of marketing authorization and reimbursement to improve
patient accessibility [12]. However, the South Korean government is also struggling with the budget
impact from the gradually increasing high-priced ODs. In 2007, South Korea introduced the HTA
system to thoroughly manage pharmaceutical expenditure while remaining sensitive to the budget
impact of high-priced ODs [13–15].
Although many studies related to OD availability and budget impact have been released in
countries such as the United States and EU countries, studies based on long-term and real-world
data have not been conducted in South Korea. This study aimed to identify patient accessibility and
pharmaceutical budget impact of ODs in South Korea by analyzing the status of OD designation,
approval, reimbursement, and pharmaceutical expenditure from 2007 (the year HTA was implemented)
to 2019.
2. Methods
The study was conducted on medicinal products designated, approved, and reimbursed as ODs
in South Korea from 2007 to 2019. Since the data before 2007 were inaccessible, the datasets used in this
study included the data from 2007, with the introduction of the HTA system in South Korea, to 2019.
2.1. Patient Accessibility of ODs
The study analyzed OD designation, approval, and reimbursement from 2007 to 2019, and
calculated the ratio of the number of reimbursed products as of 1 April 2020 to approved products for
each year. The data on the designation and approval status of ODs were retrieved from the website
of Korea Ministry of Food and Drug Safety (KMFDS) [16]. Reimbursement status of approved ODs
was identified on the website of Health Insurance Review and Assessment Service, South Korea
(HIRA) [17].
2.2. Budget Impact of ODs
The study analyzed the budget impact of 88 OD products that were approved and reimbursed
between 2007 and 2018. The reimbursement for the listed drugs started in 2009 and the budget impact
in 2009 was insignificant. Thus, the period from 2007 to 2009 was excluded from the analysis. From
2010 to 2018, the study analyzed total pharmaceutical expenditure and OD expenditure by year,
annual growth rate in expenditure, and the percentage of OD expenditure to total pharmaceutical
expenditure. In addition, the annual cost of patients treated with ODs (annual per patient costs) and
annual expenditure of individual ODs were analyzed. For the cost analysis, the dataset was collected
using publicly available materials from sources such as websites (HIRA and National Health Insurance
Service (NHIS), South Korea) and claims data from NHIS.Int. J. Environ. Res. Public Health 2020, 17, 2991 3 of 8
3. Results
3.1. Current Status of Patient Accessibility of ODs in South Korea
As of 31 December 2019, 290 ingredients were designated for orphan drugs in South Korea. From
2007 to 2019, designated ODs and approved ODs were 165 and 156, respectively, and 88 out of 156
approved products (56.4%) were reimbursed (Table 1). Of the 165 designated products, there may have
been products that had not applied for a New Drug Application (NDA), and some products that were
designated before 2007 may have been approved afterwards. In addition, some of the 156 approved
products may have not applied for reimbursement. Since the lead time until reimbursement from
approval might be about 1 to 3 years, the rate of reimbursement has dropped to 45% over the past 5
years (2015–2019).
Table 1. Current designation, approval, and reimbursement status of orphan drugs in South Korea
(2007–2019).
Year 2007 2008 2009 2010 2011 2012 2013 2014 2015 2016 2017 2018 2019 Total
Designation * 12 5 8 1 7 10 14 17 27 18 3 16 27 165
Approval ** 8 14 5 14 15 15 10 15 23 14 8 6 9 156
Reimbursed *** 6 6 2 11 9 11 7 9 14 6 3 1 3 88
Reimbursed
75.0 42.9 40.0 78.6 60.0 73.3 70.0 60.0 60.9 42.9 37.5 16.7 33.3 56.4
Ratio (%)
* As all designated products are not approved in the same year, designation year and approval year may differ. **
The number of approved products in a specific year may be greater than the number of products designated. ***
Reimbursed is the number of reimbursed orphan drugs (ODs) as of 1 April 2020 among approved ODs in the year.
3.2. Total Pharmaceutical and Orphan Drug Expenditure
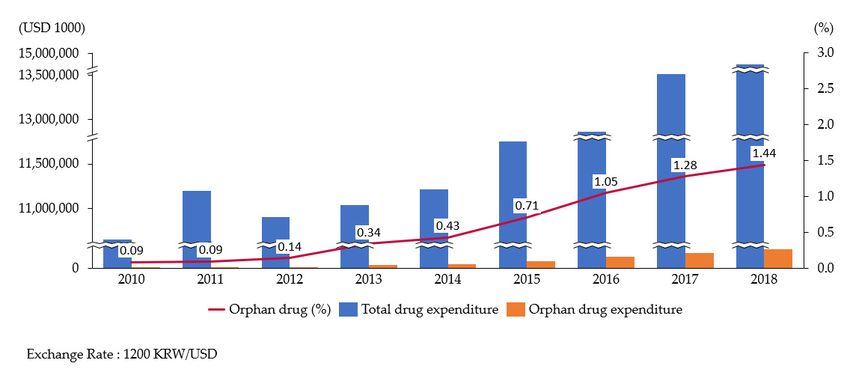
As a result of analyzing the total annual pharmaceutical expenditure and the total number of
ODs (88) reimbursed during the period 2010 to 2018, the expenditure on ODs gradually increased to
USD 213,553,000 in 2018, which accounted for about 1.44% out of total pharmaceutical expenditure
(USD 14,872,013,000; Figure 1). On the other hand, the compound annual growth rate (CAGR) of ODs
was 47.8%, which was around 11 times higher compared to the growth rate of total pharmaceutical
expenditure of 4.3% during the same period (Table 2).
3.3. Number of Patients Treated with ODs and Expenditure Per Patient of OD Products
The number of patients treated with ODs significantly increased each year, reaching 62,413 in 2018,
with an average annual increase of 36.0%. The annual OD expenditure per patient annually increased
to USD 4041 in 2017, but decreased to USD 3422 in 2018, showing an average increase of 8.7%. The
main reason for a decrease in OD expenditure per patient in 2018 was that the patient number growth
was mainly driven by products with lower cost and the average price of the newly listed products
in 2018 was relatively lower than one of previous years. As a result of analyzing annual treatment
costs of 88 ODs products, the average was USD 27,000–USD 47,000, with the maximum value of USD
260,000–USD 560,000 (Table 3).Reimbursed Ratio
75.0 42.9 40.0 78.6 60.0 73.3 70.0 60.0 60.9 42.9 37.5 16.7 33.3 56.4
(%)
* As all designated products are not approved in the same year, designation year and approval year may differ. ** The number of approved products in a specific
year may be greater than the number of products designated. *** Reimbursed is the number of reimbursed orphan drugs (ODs) as of 1 April 2020 among approved
Int. J. ODs
Environ. Res.year.
in the Public Health 2020, 17, 2991 4 of 8
Figure 1. Trend of orphan drug (OD) expenditure ratio out of total pharma expenditure (2010–2018). The expenditure ratio on ODs gradually increased and accounted
for about 1.44% out of total pharmaceutical expenditure in 2018. Source: Korea National Health Insurance Service, Health Insurance Claims Data.
Table 2. Annual
Figure 1. Trend of orphan drug (OD) expenditure expenditure
ratio out on pharmaceutical
of total pharma expenditureand orphan drugs
(2010–2018). The(2010–2018).
expenditure ratio on ODs gradually increased and
accounted for about 1.44% out of total pharmaceutical expenditure in 2018. Source: Korea National Health Insurance Service, Health Insurance Claims Data.
Year 2010 2011 2012 2013 2014 2015 2016 2017 2018 CAGR (%)
Total pharma expenditure 10,641,174 11,190,798 10,895,323 11,034,395 11,207,612 11,748,808 12,857,228 13,508,153 14,872,013 4.3
OD expenditure * 9383 10,365 15,371 37,515 48,054 83,722 135,263 172,295 213,553 47.8
OD ratio (%) 0.09 0.09 0.14 0.34 0.43 0.71 1.05 1.28 1.44 NA
Source: Korea National Health Insurance Service, Health Insurance Claims Data; Expenditure unit: USD 1000. Exchange Rate: 1200 KRW/USD. CAGR: Compound annual growth rate,
2010–2018. * OD expenditure: Total expenditure of orphan drugs reimbursed since 2006.Int. J. Environ. Res. Public Health 2020, 17, 2991 5 of 8
Table 3. Annual number of patients treated with ODs and OD expenditure (2010–2018).
Year 2010 2011 2012 2013 2014 2015 2016 2017 2018 CAGR (%)
Patients no. 5348 6408 10,650 16,040 18,405 26,220 34,460 42,633 62,413 36.0
Annual total OD
1754 1618 1443 2339 2611 3193 3925 4041 3422 8.7
expenditure/patient
Mean 46,812 31,812 31,136 44,405 46,473 43,114 27,275 41,682 36,629 NA
Annual cost
of each OD Min. 336 22 77 22 80 22 44 70 62 NA
product
Max. 366,777 363,151 402,911 452,042 464,557 513,546 265,701 553,703 554,308 NA
Median 3463 2187 2297 2076 2000 2161 2254 3808 4735 AN
Source: Korea National Health Insurance Service, Health Insurance Claims Data. Expenditure unit: USD; Exchange
rate = 1200 KRW/USD. CAGR: Compound annual growth rate, 2010–2018.
4. Discussion
The most difficult policy hurdles on availability and accessibility of ODs relate to registration
and reimbursement issues [1,2,7,18,19]. As the number of patients with rare diseases has increased,
patient access to ODs has emerged as an important issue, increasing the number of designated and
approved products. However, due to the high price of OD, there are still many OD products that are
not included in the reimbursement after marketing authorization, which has a negative impact on
patient accessibility [5,6,18,20]. In particular, countries that implement public health insurance, such
as South Korea, may have an unfavorable view on spending a huge amount of money on a small
number of patients. In other words, stakeholders related to reimbursement are struggling to adequately
accept the conflict issues on efficient allocation of limited resources along with social obligations and
ethical issues on patients in need of proper treatment [2,7,18,21–23]. As a result, some countries have
introduced systems such as exemption of cost-effectiveness assessment, conditional reimbursement,
flexible level of Incrementally Cost-Effectiveness Ratio threshold (ICER), and Risk Sharing Agreement
(RSA) in HTA to enhance patient accessibility to ODs [1,17,24].
In South Korea, with the development of diagnostic technology, the number of patients with
rare diseases has also been increasing every year: 2589 in 2002; 238,687 in 2008; 314,681 in 2010; and
520,970 in 2016 [12]. The Korean government enacted the Rare Disease Management Act in 2016 to
comprehensively manage the tasks and treatments of patients with rare diseases [25]. In addition,
OD-related regulations were introduced, such as tax favors for R&D, accelerated approval, exemption
of data submission, and extension of market exclusivity period [12]. Moreover, various benefits for ODs
are also provided in the HTA system. For instance, when the drug is designated as a medically essential
drug, the drug can be reimbursed without proof of cost-effectiveness [26]. To increase OD accessibility,
even if the drug, based on social needs and clinical values, is not designated as a medically essential
drug, the value of the ICER threshold might be adjusted flexibly through a pharmaco-economic (PE)
study assessment [26]. In addition, systems including RSA and PE study exemption are currently
implemented to improve patient accessibility [26]. As a result of such legislation, OD availability
and accessibility have improved significantly, but the accompanying budget impact has gradually
increased as well. In South Korea, the proportion of pharmaceutical expenditure in national health
insurance finance exceeds 20%, which is higher than the average pharmaceutical expenditure of 16%
in Organization for Economic Cooperation and Development (OECD) countries, making stakeholders
sensitive to increasing pharmaceutical costs [27].
In other words, the South Korean government is struggling to resolve OD accessibility and the
efficient distribution of limited financial resources. Especially in South Korea, stakeholders may be
sensitive to patient accessibility issues because of a number of high-profile cases (e.g., Novoseven RT,
Presista, Myozyme, Elaprase, and Soliris). These ODs could either not make an agreement on price and
budget limit in the final negotiation of reimbursement or had been refused supply by pharmaceutical
companies due to low listing prices [28].Int. J. Environ. Res. Public Health 2020, 17, 2991 6 of 8
This study aimed to identify the progress of OD accessibility and budget impact in South Korea
by analyzing the status of OD designation, approval, and reimbursement from 2007 (the year in
which HTA was implemented) to 2019. Following growing trends in other countries, OD designation,
approval, and reimbursement have been considerably improved in Korea under the influence of
OD-related legislation. Since 2012, the number of designated, approved, and reimbursed products has
increased, which can be explained by the effects of OD-related legislation applied to provide benefits
for regulation and legislation of OD. However, the number of products is still less than that of other
developed countries, such as the United States and countries in Europe, and many OD products are
not approved after designation or are not reimbursable after marketing authorization [1,2,6,29].
As a result of analyzing the annual budget impact of 88 ODs approved and reimbursed during
the same period, the number of patients treated with ODs continuously increased as expected, and the
growth in OD expenditure was 11 times higher than total pharmaceutical expenditure. The reason for
the excessive growth in total OD expenditure is due to the fact that the total amount is very small. As
higher-priced ODs continue to be reimbursed, the number of patients and the amount of expenditure
looks not reaching the steady state yet.
The OD expenditure rate of total pharmaceutical expenditure in South Korea is not as high as in
the United States, Canada, and European countries, where the rate of expenditure reached 2.5%~8.9%
in early 2010, although the methods and data sources are different [4,5,10,11,30,31].
On the other hand, the number of patients treated with ODs each year has increased with CAGR
36% (2010–2019), resulting in higher OD expenditure. The annual cost of individual OD products was
up to USD 260,000–USD 560,000, which indicates that some specific products have very high annual
expenditures and a very large proportion of the budget is spent on some patients treated with those
OD. If only very few patients are treated with high-priced OD, this has a significant financial impact; if
the number of patients increases for any reason, budget risk is inevitable, therefore the impact of ODs
must be monitored continuously.
Although this study was based on long-term (2009–2018) real-world data on OD expenditure
in South Korea, there are some limitations. Patient accessibility to ODs in South Korea should be
compared with other countries to make it a more valuable study, but the scope was too wide to cover
in this study. In addition, the datasets used in this study included data from 2007, the year of the
introduction of the HTA system in South Korea, and thus the products designated before 2007 were not
included. Therefore, the budget impact result in this study does not include all ODs that are currently
being reimbursed. Moreover, for ODs with multiple indications, each orphan indication must be
extracted and analyzed to obtain the exact budget impact of the OD, but currently there is no system in
South Korea to extract budget data for each orphan indication. Despite these limitations, this study is
the latest research on the availability, accessibility, and budget impact on ODs in South Korea, and can
be used as an important reference for further research.
5. Conclusions
The South Korean government tried to improve the patient accessibility of ODs through various
OD support policies, leading to an increase in the number of OD designations, approvals, and
reimbursements. However, as there are a number of ODs that have not yet been approved or are not
reimbursable after approval; a reimbursement policy should be established considering the disease
characteristics of the ODs. Meanwhile, due to the increase in patients treated with ODs and high-priced
OD products, the growth rate in OD expenditure was found to be very large, but the share in total
pharmaceutical expenditure was not as large as that of major developed countries. However, as the
rapid increase in OD expenditure can be a potential threat to the national insurance budget, budget
management such as post-reimbursement monitoring of OD expenditure should be included. In other
words, it is necessary to take preemptive measures to manage the health insurance budget efficiently
while improving patient accessibility to OD.Int. J. Environ. Res. Public Health 2020, 17, 2991 7 of 8
Author Contributions: S.H.L. and S.-L.Y. contributed equally to the study design, data analysis, and manuscript
development under the guidance of J.S.B. and J.H.L. S.H.L. participated in data collection, data analysis, and
manuscript review. S.-L.Y. participated in collecting data and revising the manuscript. J.S.B. and J.H.L. supervised
the entirety of the study right from study designing, data collection and analysis, and manuscript editing to
manuscript submission. All the authors have read and approved the final version of the manuscript. All authors
have read and agreed to the published version of the manuscript.
Funding: This research received no external funding.
Conflicts of Interest: The authors declare no conflict of interest.
References
1. Czech, M.; Baran-Kooiker, A.; Atikeler, K.; Demirtshyan, M.; Gaitova, K.; Holownia-Voloskova, M.;
Turcu-Stiolica, A.; Kooiker, C.; Piniazhko, O.; Konstandyan, N.; et al. A Review of Rare Disease Policies and
Orphan Drug Reimbursement Systems in 12 Eurasian Countries. Front. Public Health 2020, 7, 416. [CrossRef]
[PubMed]
2. Rodriguez-Monguio, R.; Spargo, T.; Seoane-Vazquez, E. Ethical imperatives of timely access to orphan drugs:
Is possible to reconcile economic incentives and patients’ health needs? Orphanet J. Rare Dis. 2017, 12, 1.
[CrossRef]
3. Dunoyer, M. Accelerating access to treatments for rare diseases. Nat. Rev. Drug Discov. 2011, 10, 475–476.
[CrossRef] [PubMed]
4. Divino, V.; DeKoven, M.; Kleinrock, M.; Wade, R.L.; Kim, T.; Kaura, S. Pharmaceutical expenditure on drugs
for rare diseases in Canada: A historical (2007-13) and prospective (2014-18) MIDAS sales data analysis.
Orphanet J. Rare Dis. 2016, 11, 68. [CrossRef] [PubMed]
5. Hughes-Wilson, W.; Palma, A.; Schuurman, A.; Simoens, S. Paying for the Orphan Drug System: Break
or bend? Is it time for a new evaluation system for payers in Europe to take account of new rare disease
treatments? Orphanet J. Rare Dis. 2012, 7, 74. [CrossRef] [PubMed]
6. Hall, A.K.; Carlson, M.R. The current status of orphan drug development in Europe and the US. Intractable
Rare Dis. Res. 2014, 3, 1–7. [CrossRef] [PubMed]
7. Davies, E.H.; Fulton, E.; Brook, D.; Hughes, D.A. Affordable orphan drugs: A role for not-for-profit
organizations. Br. J. Clin. Pharmacol. 2017, 83, 1595–1601. [CrossRef]
8. Kumar Kakkar, A.; Dahiya, N. The evolving drug development landscape: From blockbusters to niche
busters in the orphan drug space. Drug Dev. Res. 2014, 75, 231–234. [CrossRef]
9. Jayasundara, K.; Hollis, A.; Krahn, M.; Mamdani, M.; Hoch, J.S.; Grootendorst, P. Estimating the clinical cost
of drug development for orphan versus non-orphan drugs. Orphanet J. Rare Dis. 2019, 14, 12. [CrossRef]
10. Logviss, K.; Krievins, D.; Purvina, S. Impact of orphan drugs on Latvian budget. Orphanet J. Rare Dis. 2016,
11, 59. [CrossRef]
11. Kanters, T.A.; Steenhoek, A.; Hakkaart, L. Orphan drugs expenditure in the Netherlands in the period
2006–2012. Orphanet J. Rare Dis. 2014, 9, 154. [CrossRef] [PubMed]
12. Gachon University Industry-Academic Collaboration. Policy Report: Foundation Analyzing the Status
of Rare Diseases and Ways to Improve Support for Rare Diseases Patients in Korea; Gachon University
Industry-Academic Collaboration: Incheon, Korea, 2018; Available online: http://www.prism.go.kr/
homepage/lately/retrieveLatelyDetail.do;jsessionid=3A49CCBE15518DC57FEF2ABB66D9ED6F.node02?
research_id=1351000-201800313 (accessed on 29 March 2020).
13. Ministry of Health and Welfare. Press Release: Policy Measures to Optimize Drug Expenditure; Ministry of
Health and Welfare: Sejong, Korea, 2006. Available online: http://www.mohw.go.kr/react/al/sal0301vw.jsp?
PAR_MENU_ID=04&MENU_ID=0403&page=1&CONT_SEQ=39921 (accessed on 29 March 2020).
14. Park, S.E.; Lim, S.H.; Choi, H.W.; Lee, S.-M.; Kim, D.W.; Yim, E.Y.; Kim, K.H.; Yi, S.Y. Evaluation on the first 2
years of the positive list system in South Korea. Health Policy 2012, 104, 32–39. [CrossRef] [PubMed]
15. Bae, E.-Y.; Hong, J.-M.; Kwon, H.-Y.; Jang, S.; Lee, H.-J.; Bae, S.; Yang, B.-M. Eight-year experience of using
HTA in drug reimbursement: South Korea. Health Policy 2016, 120, 612–620. [CrossRef] [PubMed]
16. Korea Ministry of Food and Drug Safety. Available online: https://nedrug.mfds.go.kr/pbp/CCBAD01
(accessed on 16 April 2020).
17. Korea Health Insurance Review and Assessment Service. Available online: http://www.hira.or.kr/rf/medicine/
getHistoryList.do?pgmid=HIRAA030035020000 (accessed on 16 April 2020).Int. J. Environ. Res. Public Health 2020, 17, 2991 8 of 8
18. Gammie, T.; Lu, C.Y.; Babar, Z.U. Access to Orphan Drugs: A Comprehensive Review of Legislations,
Regulations and Policies in 35 Countries. PLoS ONE 2015, 10, e0140002. [CrossRef] [PubMed]
19. Bourdoncle, M.; Juillard-Condat, B.; Taboulet, F. Patient access to orphan drugs in France. Orphanet J. Rare
Dis. 2019, 14, 47. [CrossRef]
20. Picavet, E.; Morel, T.; Cassiman, D.; Simoens, S. Shining a light in the black box of orphan drug pricing.
Orphanet J. Rare Dis. 2014, 9, 62. [CrossRef]
21. Franco, P. Orphan Drugs: The regulatory environment. Drug Discov. Today 2013, 18, 163–172. [CrossRef]
22. Blankart, A.; Rudolf, C.; Stargardt, T.; Schreyogg, J. Availability of and access to orphan drugs.
Pharmacoeconomics 2011, 29, 63–82. [CrossRef]
23. Barrera, L.A.; Galindo, G.C. Ethical aspects on rare diseases. Adv. Exp. Med. Biol. 2010, 686, 493–511.
24. Kawalec, P.; Sagan, A.; Pilc, A. The correlation between HTA recommendations and reimbursement status of
orphan drugs in Europe. Orphanet J. Rare Dis. 2016, 11, 122. [CrossRef]
25. Ministry of Health and Welfare. Act: Act on the Management of Rare Desease; Ministry of Health and Welfare:
Sejong, Korea, 2019. Available online: http://www.law.go.kr/lsSc.do?tabMenuId=tab18&query=%ED%9D%
AC%EA%B7%80%EC%A7%88%ED%99%98%EA%B4%80%EB%A6%AC%EB%B2%95#undefined (accessed
on 30 March 2020).
26. Yoo, S.L.; Kim, D.J.; Lee, S.M.; Kang, W.G.; Kim, S.Y.; Lee, J.H.; Suh, D.C. Improving Patient Access to New
Drugs in South Korea: Evaluation of the National Drug Formulary System. Int. J. Environ. Res. Public Health
2019, 16, 288. [CrossRef] [PubMed]
27. OECD. Statics: OECD Health Statics 2018; OECD: Paris, France, 2018; Available online: http://www.oecd.org/
health (accessed on 30 March 2020).
28. Kwon, H.Y.; Yang, B.M. Issues with Orphan Drug Pricing in South Korea. Korean J. Health Econ. Policy 2010,
16, 17–37.
29. European Medicines Agency. Annual Report: Annual Report on the Use of the Special Contribution for
Orphan Medicinal Products; European Medicines Agency: Amsterdam, The Netherlands, 2018; Available
online: https://www.ema.europa.eu/en/documents/report/annual-report-use-special-contribution-orphan-
medicinal-products-2018_en.pdf (accessed on 29 March 2020).
30. Hutchings, A.; Schey, C.; Dutton, R.; Achana, F.; Antonov, K. Estimating the budget impact of orphan drugs
in Sweden and France 2013–2020. Orphanet J. Rare Dis. 2014, 9, 22. [CrossRef] [PubMed]
31. Denis, A.; Mergaert, L.; Fostier, C.; Cleemput, I.; Simoens, S. Budget impact analysis of orphan drugs in
Belgium: Estimates from 2008 to 2013. J. Med. Econ. 2010, 13, 295–301. [CrossRef]
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access
article distributed under the terms and conditions of the Creative Commons Attribution
(CC BY) license (http://creativecommons.org/licenses/by/4.0/).You can also read