Is the concept of somatoform pros-thesis intolerance still up to date?
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
32 RESEARCH ORIGINAL ARTICLE
Anne Wolowski
Is the concept of somatoform pros-
thesis intolerance still up to date?
Introduction: Until recently “somatoform prosthesis intolerance” covered a
wide range of patients with diffuse symptoms.
Material and Methods: Meanwhile, new dental conditions have been estab-
lished so that it is possible to differentiate among Burning Mouth Syndrome
(BMS), atypical odontalgia (persisting [idiopathic] dental alveolar pain), occlu-
sal dysesthesia, and somatoform prosthesis intolerance. These clinical pictures
can be categorized under diagnosis of “somatic symptom disorders”, which
was newly established in 2015. It is marked by a duration of symptoms of
more than 6 months, intense preoccupation with those symptoms, and a
significantly reduced capability to cope with everyday life. The formerly used
diagnosis “somatoform prosthesis intolerance” can likewise be understood as
a subcategory of specific dental somatic symptom disorder.
Conclusion: Based on available clinical experience it can be assumed that this
diagnosis will be particularly applicable for patients that are equipped with
objectively well-fitting fixed and/or removable dentures but experience dif-
ficulties with them and therefore attract attention with somatic stress symp-
toms. A structured approach is necessary for initial and basic treatment. This
is described by the S3-guideline “functional disorders”.
Keywords: somatoform prosthesis intolerance; burning mouth syndrome;
occlusal dysesthesia; atypical odontalgia; somatic stress disorder; functional
disorders
Poliklinik for Prosthetic Dental Medicine and Biomaterials, Westfälische Wilhelms-Universität, University hospital Münster – Center ZMK, Münster, Germany: PD Dr. Anne
Wolowski
Translation from German: Yasmin Schmidt-Park
Citation: Wolowski A: Is the concept of somatoform prosthesis intolerance still up to date? Dtsch Zahnärztl Z Int 2021; 3: 32–39
Peer-reviewed article: submitted: 10.07.2020, revised version accepted: 18.09.2020
DOI.org/10.3238/dzz-int.2021.0004
© Deutscher Ärzteverlag | DZZ International | Deutsche Zahnärztliche Zeitschrift International | 2021; 3 (1)WOLOWSKI:
Is the concept of somatoform prosthesis intolerance still up to date? 33
Review
Diagnostic criteria of a psychogenic prosthesis intolerance according
In 1921, Moral and Ahnemann [33] to Müller-Fahlbusch
described the course of disease of a
50-year old patient, who complained
1. Discrepancy between description of symptoms and anatomical limits
about tongue pain, in a paper on bor-
derline cases: “Her depiction appears
Discrepancy between chronology of symptoms and complaints and the
unclear and blurred ... if pain showed 2.
known development known to us by clinical experience
up on the right side of the tongue
once, it appeared on the other side at
3. Ex non juvantibus (a normally helpful treatment does not lead to success)
the next examination [...] suddenly
also here [...], so that the pain can
4. Unusual co-participation of the patient in the course of the disease
also be lead from one nerve region to
another [...]”. The authors found no
Coincidence of biographic-situational results and beginning of the
clinical abnormalities for the men- 5.
complaints
tioned complaints. They described
the prostheses as well-crafted and Table 1 Diagnostic criteria of a psychogenic prosthesis intolerance according to
occluded, the elimination test was Müller-Fahlbusch [34]
negative, meaning that the patient
was complaining about the same
amount of discomfort while not
wearing prostheses. The authors them are mostly unrecognizable. The alternating with different emphasis.
highlight the uselessness and specifi- clinical picture of “hysteria”, which In the meantime, the work of Briquet
cally the damage caused by countless according to Moral and Ahnemann is has been picked up by many authors.
treatment attempts, which usually based “... on a disorder of a normal Essentially, the attempt was made to
lead to chronification. They believe relationship between processes of our systematize his observations assisted
that the desire to help tormented pa- conscience and our physicality”, for by Guze [17–19]. With the introduc-
tients leads to therapeutic errors and which they determine a basic con- tion of the DSM-III in 1980 [3], the
mishaps. The authors are giving a lot dition “... that hysteria is an illness of Briquet-Syndrome was first incorpo-
of attention to a goal-oriented, pos- the soul and that a treatment should rated as a framework of the prototype
sibly interdisciplinary somatic diag- be used; ...”, which was described in of somatization disorder in its own
nosis of exclusion. They do not con- 1859 by the French physician Briquet category in a clinically binding clas-
sider it the dentist’s job to – accord- [5] in his work “Traité clinique et sification system. Müller-Fahlbusch
ing to them – treat hysteria, but thérapeutique de l´hystérie”. He also and Marxkors [30] shaped the term
rather to perform necessary dental shows a descriptive approach to ana- “psychogenic prostheses intoler-
treatment. The difficulties of making lyze the disease similarly to Moral ance”, which had already been used
the diagnosis in the manifold and and Ahnemann [33]. He lists a vari- by Peterhans in 1948 [36]. Based on
multifaceted clinical picture indicate, ety of physical and mental symp- an interdisciplinary research project
that for routine dental measures, toms, which appear in “hysteric” sick conducted in 1976 [39], Müller-
usually “... superficial recording of patients in the form of a protruding Fahlbusch and Marxkors understood
the anamnesis is sufficient”, and with leading symptoms or in combination this as “complaints that do not fit the
that the borderline cases depicted by with multiple complaints, possibly picture of the respective findings.
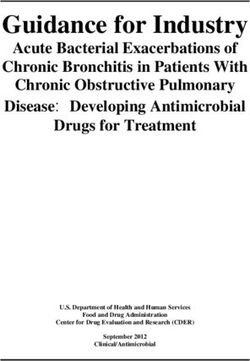
Somatic symptom(s)
Criterion A
are distressing
result in disruption of daily life
Psychological Characteristics regarding physical symptoms
Exaggerated and persisting thoughts on the seriousness of the present symptoms cognitive dimension
Criterion B
Persisting and pronounced high level of anxiety regarding health of symptoms emotional dimension
Excessive effort in time and energy that is expensed for the symptoms behavioral dimension
Kriterium C Burden of symptoms for longer than 6 months
Table 2 Somatic Symptom Disorder: For a diagnosis according to DSM-5 (Diagnostic and Statistical Manual of Mental Disorders)
criteria A, B (at least 1 of 3 psychological dimensions) and C must be met [11, 25].
© Deutscher Ärzteverlag | DZZ International | Deutsche Zahnärztliche Zeitschrift International | 2021; 3 (1)WOLOWSKI:
34 Is the concept of somatoform prosthesis intolerance still up to date?
List of symptoms In 2008, the term “psychogenic
prosthesis intolerance” was replaced
• Stomach pain or indigestion
by the term “somatoform prothesis
intolerance“ [13]. With this, the
• Back pain
necessary adjustment of the nomen-
clature in general medicine occurred
• Aching arms, legs or joints
[12]. Besides the Burning-Mouth-
Syndrome, the somatoform pain dis-
• Headache
order and body dysmorphic disorder
(as a special form), the somatoform
• Chest pain or shortness of breath
prosthesis intolerance presents a rel-
evant subdivision of somatoform dis-
• Dizzyness
order: “The characteristic of somato-
form disorder is the repeated presen-
• Fatigue or lack of energy
tation of physical symptoms in com-
bination with persistent demands
• Insomnia
after examinations, despite repeat-
edly negative results and reassur-
Severity of somatic burden ances by doctors, that the symptoms
are not based on any physicality. If
0–3 None to minimal
there is some organ pathology pres-
ent, it does not explain the nature
4–7 Low
and extent of the symptoms and the
pain and the internal investment of
8 – 11 Moderate
the patient”. With the classification
of the illness pattern of “somato-
12 – 15 High
form prosthesis intolerance”, the
first criterion according to Müller-
16 – 32 Very high
Fahlbusch takes on an extended di-
mension. While Müller-Fahlbusch
Table 3 Somatic symptoms scale to determine the somatic symptom burden (SSS 8) relates the discrepancy to anatomical
[28]. A sum score of 0 = “none” to 4 = “very high” is formed to answer the “how high structures – “medical psychology and
was the burden caused by the mentioned symptoms during the past week”. psychosomatics does not work with-
out anatomy” [34] –, demanded with
the inclusion of somatic findings,
that the complaints within context
The complaints are more general, less chosomatic conspicuous patients are evaluated of possible, also patho-
tangible and do not allow for direct (Tab. 1). logical findings, regarding their na-
conclusions about the prosthetic Müller-Fahlbusch attaches special ture, expansion and intensity in
work” [31, 34]. While Marxkors importance to the time of treatment order to detect an available discrep-
understood this term in the pros- of a possibly necessary somatic ther- ancy to the mentioned complaints.
thetic context, Müller-Fahlbusch ex- apy and depicts recommendations of
tended this viewpoint with psychi- how to deal with these patients. Just Characteristics of a
atric aspects. In an interdisciplinary like Haneke [20], he recommends “somatoform prosthesis
study he diagnosed 57 % of patients the regulation of psychiatric drugs, intolerance”
with psychogenic prosthesis intoler- usually antidepressants. Balters [4] Fundamentally, the question is
ance with phasic and chronic de- advises psychological care of the ill raised whether or not the term “so-
pression, 21 % of patients with ab- that is supposed to help turn the loss matoform prosthesis intolerance”
normal personality disorder and of their teeth into something posi- summarizes this group of patients
19 % of patients with an abnormal tive. Marxkors [31] warns against accurately enough today, or if
experience response. He classified overpowering when dealing with dif- further classifications exist by now
about 3 % of patients in the category ficult patients and to not expand that allow a more precise distinction
of schizophrenics. Only in the course treatments against the wishes of the and with that more targeted treat-
of further cooperation psychosomatic dentist, just because the patient ment options. There is hardly any
diagnostics developed, but further wishes or demands it. Other authors data on who is typically affected by
down the line, a viewpoint in psy- [8, 48] recommend to consider solid these symptoms. Studies [32, 39]
chosomatic diagnostics which was es- constrictions in “patients with psy- could show, that women aging be-
pecially expressed in the catalogue chosis”. All authors are in agreement tween 60 and 70 sought out a
compiled by Müller-Fahlbusch [34] of regarding a crucial and necessary in- specialized consultation 5-times
5 diagnostic criteria to recognize psy- terdisciplinary cooperation. more frequently. The main symp-
© Deutscher Ärzteverlag | DZZ International | Deutsche Zahnärztliche Zeitschrift International | 2021; 3 (1)WOLOWSKI:
Is the concept of somatoform prosthesis intolerance still up to date? 35
Burning-Mouth- Persisting idiopathic
Symptoms Syndrome facial pain Atypical odontalgia Occlusal dysesthesia
Diagnosis criteria – daily burning/burning – pain nearly all day – daytime pain, brief to – awareness only during
pain or feeling of – at most low impair- persisting waking state
dysesthesia ment of night’s sleep – unimpaired night‘s
– > 3 months sleep
– at least > 2 hours per – > 4 months
day – spontaneous beginn,
that can (often) be
delayed following the
trauma of a peripheral
trigeminal nerv (ex-
periencing pain during
such course of action
increases the risk)
– women, – fluctuating intensity – diffuse expansion ten- – “occlusally fixed”
– > 50 years old – at most just beginning dency model of illness
– reduced quality of life anatomically limiting – variable intensity – intensive occupation
– increasing intensity expansion – pain amplification with the disorder
during the course of – “peculiar” disease through peripheral – Chronification tenden-
the day causation modell stimuli cy with many unsuc-
– allodynia/hyperalgesia cessful changes in
– uncertain pain elimi- occlusion
nation – dismissive evaluation
– ex non iuvantibus of previous practi-
tioners
– glorification of the
current practitioner
– psychosocial burdens/
impairment at the
beginning and/or over
the course
– further physical ail-
ments usually without
objectifiable cause and
plausible course of
therapy
– no local/general medi- – no relevant pathologi- – missing adequate – no relevant malocclu-
cal and psychological cal results pathological results sion
causes
Screening/ Pain diary regarding – Chronification: GCS
documentation modulation factors, [43, 45].
forms (if avail- possibilities of relief and – anxiety, depression:
able) accompanying symp- HADS [21]; PHQ-4
toms [27]; DASS [20,34].
– emotional stress: SRRS
[1, 22];
– somatization: BL-R /
BL-R‘ [46]
– localisation of pain: full
body drawing [42] of
all existing pain
regions.
Table 4 Typical characteristics, screening options, differential diagnoses and supportive information in diseases appearing diffuse in
the orofacial
toms listed by affected patients are down)”. These symptoms can appear picture. Usually the symptoms last
pain, burning of oral mucosa and localized or radiate further into the longer than 6 months. The patient‘s
adaptation disorders (mostly related oral cavity and are solely associated path in search of relief is character-
to prostheses and often specifically with the oral cavity based on the pa- ized by countless diagnostic pro-
related to the “difficulty to bite tients’ understanding of the clinical cedures and therapy attempts (“doc-
© Deutscher Ärzteverlag | DZZ International | Deutsche Zahnärztliche Zeitschrift International | 2021; 3 (1)WOLOWSKI:
36 Is the concept of somatoform prosthesis intolerance still up to date?
Burning-Mouth- Persisting idiopathic
Symptoms Syndrome facial pain Atypical odontalgia Occlusal dysesthesia
Differential diag- secundary burning of neuropathological pain dental causes objectifiable malocclu-
noses (screening, the oral mucosa (possibly triggered by sion
if available) surgery in the specified craniomandibular dys-
pain region) function/bruxism
CMD screening
https://www.dgfdt.de/
documents/266840/
3732097/CMD-Screen-
ing+DGFDT/
cc704187-a983–4eed-8
93c-614ae3969bd1
bruxism screening
https://www.dgfdt.de/
documents/266840
/3732097/Bruxis
mus+Screening+02_20/
8039b42a-9640–47e9-
bd9f-0717a3c4d423
functional status
https://www.dgfdt.de/
documents/266840/
406693/Erfassungs
formular+Funktions
status+2012/1d692
d7a-bf94–4509–90
35-a091a82d58f7?
version=1.0)
Supporting https://www.zahnmed https://www.zahnmedi https://www.zahnmed
information izinische-patientenin zinische-patientenin izinische-patientenin
(if available, formationen.de/docu formationen.de/docu formationen.de/docu
retrievable from ments/10157/ ments/10157/1129556/ ments/10165/1430990/
DGZMK: 903264/Zungen- 268572_1567299_Chro PI+Bruxismus-final.pdf
https://www. und_Schleimhaut nischer+Kiefer-+und+
zahnmedizin brennen/ Gesichtsschmerz.pdf https://www.zahnmed
ische-patientenin izinische-patientenin
formationen.de/ formationen.de/docu
patientenin- ments/10157/1129556/
formationen) 268572_1567355_Kie
fergelenkschmerz.pdf/
Table 4 Typical characteristics, screening options, differential diagnoses and supportive information in diseases
appearing diffuse in the orofacial
tor hopping, doctor shopping”). It is of “somatic stress disorder”, which were triggered by a somatic and/or
not uncommon to observe that pa- can therefore be seen as a superordi- mental reason. In general medicine,
tients affected, as well as people nate category. the severity of the burden is deter-
close to them subject their entire mined by respective points on an
lives to these complaints and show a Somatic Symptom Disorder 8-symptom scale (SSS 8) [16, 28]
severely reduced quality of life. (SSD) (Tab. 3). Typical dental symptoms
These main symptoms are accom- SSD refers to a new classification in have not been recorded in the SSS 8.
panied by complaints about dry the Diagnostic and Statistical Manual In order to assess a potentially gen-
mouth or altered sense of taste. The of Mental Disorders (DSM-5) [7, 25, erally existing problem, this symp-
courses of complaints are individ- 26, 41]. This should diagnostically tom scale can be inquired within the
ually different and vary regarding record about 30 % of patients in context of general anamnesis in a
their intensity. These characteristics basic care, that are severely affected regular dentist appointment. This
regarding course and duration, by existing physical symptoms and offers the chance to recognize ten-
understanding of the disease or deal- restricted in their daily lives. In order dencies and risks of expansion into
ing with the complaints are key to make this diagnosis, it is irrelevant the jaw and face region with possibly
criteria of the newly added diagnosis if the characteristics listed in table 2 necessary dental measures. Depend-
© Deutscher Ärzteverlag | DZZ International | Deutsche Zahnärztliche Zeitschrift International | 2021; 3 (1)WOLOWSKI:
Is the concept of somatoform prosthesis intolerance still up to date? 37
Initial basic care Extended basic care
When visiting the doctor repeatedly and “doctor-hopping-
In the mild form
tendency”
Recognition Comprehensive anamnesis simulta- To emphasize the equality of physical and
– main symptoms neous diag- psychosocial influencing factors
– accompanying symptoms nosis – Attention: do not act on “pressure by the
– impairments patient” “slow down”
– patient behavior – Goal-oriented, clear setting
– initial recording of findings – No technical supplementary examinations
– demand preliminary findings to calm down the patient
– avoid redundancies – explain regular findings
– further examinations with reserved and – demonstrate prognosis/risks of a one-sided
strict indication somatic approach
Reassurance Evaluation of findings and risks Accomplish- – biopsychosocial explanation model orig-
– Announce “expectable” normal findings ment inating from subjective disease theory
– No downplaying model of disease in e.g. using individual amplifiers, modulation
order to expand psychosocial viewpoint factors as well as possibilities of relief
– clarify expectations and correct if necessary
– emphasize autonomy, develop “active”
coping strategies
– regular appointments independent of
discomfort
Advice – “take the patient seriously” Possibly – Transparent findings assessment
– emphasize credibility initiate inter- – Motivate patients to take up psychosocial
– work out positive resources disciplinary therapy options
cooperation – dental findings to avoid the polypragmatic
approach “monitoring”
Supporting https://www.awmf.org/uploads/tx_szleitlinien/051–001p3_S3_Funktionelle_Koerperbeschwerden_2020–01.pdf
information
Therapeutic wait and see: Patient monitoring and supervision while avoiding measures that are not strictly indicated
“support”
Table 5 Diagnostics and therapeutic approach [following 37]
(Tab. 1–5: A. Wolowski)
ing on the severity of the disorder, it mucosa, pain and occlusal “malfunc- tal factors arise following an (idio-
has to be decided if an explanation tions”. pathic) BMS. Different levels of
of risk by the dentist is sufficient or if Burning of the oral mucosa: Scala et anxiety are listed and in 20 % of BMS
an interdisciplinary approach has to al. [40] differentiate the secondary patients, the phobia of cancer can be
be pursued. It can be helpful for such burning of oral mucosa that can be observed. Depression and somati-
a decision to differentiate between diagnosed following an underlying zation disorder are named as further
relevant dental clinical pictures. The dental, general and mental disorder of diagnoses [2, 6, 14, 27, 29, 37] (Tab. 4).
necessity of this differentiation also idiopathic burning of the oral mucosa, Pain in the sense of persistent idio-
results from the fact that an interdis- which is classified as BMS [47]. Ac- pathic facial pain (PIFP)/ atypical odon-
ciplinary setting with treating “non- cording to the currently valid defini- talgia (persistent [idiopathic] dental
dentists” requires explicit details on tions [24], the diagnosis BMS is based pain): PIFP refers to the pain, that
dental context. on a diagnosis of exclusion. The differ- does not meet the criteria of a facial
ent current definitions regarding BMS neuralgia and is not associated with
Dental diseases with differ mainly in the specification of signs of an organic lesion. “The pain
symptoms seeming diffuse total duration and the daily course. is present, mostly continuous, one-
It can be differentiated between den- Because BMS has not been defined sided and difficult to locate. Sensitiv-
tal symptoms within the group of so- uniformly in literature, it cannot be ity symptoms or other deficiencies
matic stress disorders by using a com- differentiated regarding mental factors are not present. Further examinations
plaint-related classification. The lead- if this is the cause for a secondary including X-Ray diagnostics of the
ing symptoms are burning of the oral burning of the oral mucosa or if men- face and jaw are without pathological
© Deutscher Ärzteverlag | DZZ International | Deutsche Zahnärztliche Zeitschrift International | 2021; 3 (1)WOLOWSKI:
38 Is the concept of somatoform prosthesis intolerance still up to date?
findings. Either trauma, or an oper- into the always necessary basic care References
ation of face, jaw and teeth can cause and the extended care during longer 1. Ahlers MO, Jakstat HJ: Sozialanam-
the pain. However, there can be no hospital stays as well as multimodal nese: Fragebogen „Stressbelastung“. In:
current pathological local findings” therapy. It should be emphasized in Ahlers MO, Jakstat HJ (Hrsg): Klinische
[10], because that would categorize it this context that further dental treat- Funktionsanalyse. dentaconcept, Ham-
burg 2011, 170–179
as a diagnosis of exclusion [15]. ment support should be maintained
A localized form of the PIFP is de- and no either-/or-principle should be 2. Amenabar JM, Pawlowski J, Hilgert JB
et al.: Anxiety and salivary cortisol levels
scribed as atypical odontalgia, in initiated with the referral to other
in patients with burning mouth syn-
which a pathomechanism of a neuro- specialist disciplines. This issue is drome: case-control study. Oral Surg Oral
pathological persistent pain com- written out to supposedly lead to a Med Oral Pathol Oral Radiol Endod 2008;
parable to phantom pain is taken on better mutual understanding of co- 105: 460–465
[15, 44]. Based on missing pathologi- practitioner and patient. The basic 3. American Psychiatric Association
cal findings, this is also a diagnosis of principle here is maximum transpar- (APA): Diagnostic and statistical manual
exclusion. Endodontic procedures are ency. This requires a sustainable and of mental disorders, 3rd ed. revised. APA,
described as risk and trigger factors or with that resilient doctor-patient-rela- Washington DC, 1980
as an experienced painful dental tionship, which is supported by a 4. Balters W: Die Bedeutung von
treatment before a tooth extraction structured approach (Tab. 5). Zahnverlust und Zahnersatz für den Pa-
(Tab. 4). tienten – von der Psychologie her ge-
sehen. Dtsch Zahnärztl Z 1951; 11:
Occlusal dysesthesia: The symp- Which symptoms remain of 465–468
toms of occlusal dysesthesia (OD) de- the “somatoform prosthesis
5. Briquet P: Traité clinique et thérapeu-
scribes the phenomenon, that pa- intolerance”?
tique de l‘Hystérie. Baillière et fils, Paris
tients complain about pain origi- In conclusion, the question is raised 1859
nating from their occlusion, which is if the diagnosis “somatoform pros-
6. Browning S, Hislop S, Scully C, Path
clinically not objectifiable. Most pa- thesis intolerance” is justified today.
MRC, Shirlaw P: The association between
tients affected are burdened mentally This can be understood as a subgroup burning mouth syndrome and psycho-
and show characteristics of depres- of dental-specific disease in the sense social disorders. Oral Surg Oral Med Oral
sion and/or anxiety. They are often of a somatic stress disorder in pa- Pathol 1987; 64:171–174
solely focused on a somatic/occlusal tients whose leading symptom is 7. Budtz-Lilly A, Schröder A, Rask MT,
cause of their pain and every therapy burning of the oral mucosa, pain Fink P, Vestergaard M, Rosendal M:
attempt according to the rules with and/or occlusal difficulties to general Bodily distress syndrome: A new diag-
mostly rotating practitioners almost physically severely burdening symp- nosis for functional disorders in primary
care? BMC Fam Pract 2015; 16:1 80–190
always leads to intensification of toms. Based on the available clinical
the complaints. The median age de- experience one can assume that this 8. Costen JB: A syndrome of ear and
sinus symptoms dependent on disturbed
scribed for these symptoms in litera- diagnosis applies especially to pa-
function of the temporomandibular joint.
ture is 52 years (plus/minus 11 years), tients that are fitted with (fixed and/ Ann Otol Rhinol Laryngol 1934; 43: 1–15
which also goes along with clinical or removable) prostheses and experi-
9. DGZMK, DGFDT: S1-Leitlinie: Okklu-
experience in specialized consul- ence difficulties with them and show
sale Dysästhesie – Diagnostik und Man-
tation. Etiological factors discussed signs of somatic stress. The diagnosis agement, AWMF Registernummer
are psychopathological causes, neuro- “somatoform prosthesis intolerance” 083–037, 2019; https://www.awmf.org/
plasticity, phantom phenomenons should not be a diagnosis of exclu- leitlinien/detail/ll/083–037.html (last
and changes of proprioceptive stimu- sion, but rather it is more important access on 4. Juli 2020)
li and transmission [9] (Tab. 4). to detect indications of somatic and 10. Diener HC, Weimar C, Berlit P et al.:
psychosocial influences, if a differen- Anhaltender idiopathischer Gesichts-
schmerz in Kommission „Leitlinien“ der
Structured approach tial exclusion of the specific clinical
Deutschen Gesellschaft für Neurologie
Given the mostly complex and diffuse pictures follows. It is to be expected (DGN) (Hrsg.): Leitlinien für Diagnostik
ailments and also the psychological that the diagnosis “somatoform pros- und Therapie in der Neurologie. Thieme,
strain of the affected, it is the most thesis intolerance” can overlap with Stuttgart 2012, 562–566
important goal to identify influencing the described dental diseases. A valid 11. Dimsdale JE, Creed F, Escobar J et al.:
factors early and inform comprehen- and identical approach according to Somatic symptom disorder: an important
sively, so that affected people are ac- psychosomatic basic care for all dif- change in DSM. J Psychosom Res 2013;
tively included in the diagnostic and ferential diagnoses is helpful and cru- 75: 223–228
possibly therapeutic process. The cial for the practitioner. 12. Dilling H, Mombour W, Schmidt MH,
guideline on “functional disorders”, Schulte-Markwort E, Remschmidt H: In-
published in 2019 [37], which specifi- ternationale Klassifikation psychischer
Störungen: ICD-10 Kapitel V (F) klinisch-
cally included the clinical picture of
diagnostische Leitlinien. 10. Auflage,
somatic stress disorder on the spec- Conflicts of interest unter Berücksichtigung der Änderungen
trum of the summarized clinical pic- The author declares that there is no entsprechend ICD-10-GM 2015.
tures, presets a structured approach. conflict of interest as defined by the Hogrefe, Bern 2015
These are based on the severity of the guidelines of the International Com- 13. Doering S, Wolowski A: Psychoso-
course of the disease and are classified mittee of Medical Journal Editors. matik in der Zahn-, Mund- und Kiefer-
© Deutscher Ärzteverlag | DZZ International | Deutsche Zahnärztliche Zeitschrift International | 2021; 3 (1)WOLOWSKI:
Is the concept of somatoform prosthesis intolerance still up to date? 39
heilkunde. Wissenschaftliche Mitteilung Primary and Hospital Care – Allgemeine dener Fachdisziplinen. Dtsch Zahnärztl Z
der DGZMK 2008. https://secure.owidi. innere Medizin 2016; 16: 192–195 1976; 31: 5–7
de/documents/10165/2216111/Psycho
26. Lam TP, Goldberg DP, Dowell AC et 40. Scala A, Checchi L, Montevecchi M,
somatik_in_der_Zahn-_Mund-_und_Kie
al.: Proposed new diagnoses of anxious Marini I, Giamberardino MA: Update on
ferheilkunde_2008.pdf/0f0bbb
depression and bodily stress syndrome in burning mouth syndrome: overview and
61-d371–490d-b22d-65d6865976e4,
ICD-11-PHC: an international focus patient management. Crit Rev Oral Biol
(last access on 31. August 2020)
group study. Fam Pract 2013; 30: 76–87 Med 2003; 14: 275–291
14. Drage LA, Rogers RS: Clinical assess-
ment and outcome in 70 patients with 27. Lamey PJ, Lamb AB: Prospective
41. Sonnleitner J, Aigner M: Von den so-
complaints of burning or sore mouth study of aetiological factors in burning
matoformen Störungen zur somatischen
symptoms. Mayo Clin Proc 1999; 74: mouth syndrome. Br Med J (Clin Res Ed)
Belastungsstörung. Diagnoserichtlinien
223–228 1988; 296: 1243–1246
des DSM 5. psychopraxis.neuropraxis
15. Gaul C, Ettlin D, Pfau DB: Anhal- 28. Löwe B, Wahl I, Rose M et al.: A 2015; 18: 132–36
tender idiopathischer Gesichtsschmerz 4-item measure of depression and
anxiety: validation and standardization 42. Türp JC, Marinello C: Schmerzfrage-
und atypische Odontalgie. Persistent
of the Patient Health Questionnaire-4 bogen für Patienten mit chronischen
idiopathic facial pain and atypical odon-
(PHQ-4) in the general population. orofazialen Schmerzen. Quintessenz
talgia. Z Evid Fortbild Qual Gesundh
J Affect Disord 2010; 122: 86–95 2002; 53: 1333–1348
wesen (ZEFQ) 2013; 107: 309–313
16. Gierk B, Kohlmann S, Toussaint A et 29. Maina G, Albert U, Gandolfo S, Vita- 43. Türp JC, Nilges P: Diagnostik von
al.: Assessing somatic symptom burden: lucci A, Bogetto F: Personality disorders Patienten mit chronischen orofazialen
a psychometric comparison of the pa- in patients with burning mouth syn- Schmerzen. Die deutsche Version des
tient health questionnaire-15 (PHQ-15) drome. J Personal Disord 2005; 19: „Graded Chronic Pain Status“. Quintes-
and the somatic symptom scale-8 84–93 senz 2000; 51: 721–727
(SSS-8). J Psychosom Res 2015; 78: 30. Marxkors R, MüllerFahlbusch H: Psy-
352–355 44. Türp J: Die atypische Odontalgie.
chogene Prothesenunverträglichkeit – Ein Schweiz Monatsschr Zahnmed 2005;
17. Guze SB, Perley MJ: Observations on nervenärztliches Consilium für den 115: 1006–1011
the natural history of hysteria. Am J Psy- Zahnarzt. Hanser, München 1976
chiatry 1963; 119: 960–965 45. Von Korff M, Ormel J, Keefe F, Dwor-
31. Marxkors R: Ursachen und Therapie
von Prothesenintoleranz. Dtsch Zahnärztl kin SF: Grading the severity of chronic
18. Guze SB: The diagnosis of hysteria:
Z 1995; 50: 704–707 pain. Pain 1992; 50: 133–150
what are we trying to do? Am J Psy-
chiatry 1967; 124: 491–498 46. Von Zerssen D, Petermann F: Befind-
32. Marxkors R, Wolowski A: Unklare
19. Guze SB: The validity and signifi- Kiefer-Gesichtsbeschwerden. Abgrenzung lichkeitsskala – Revidierte Fassung.
cance of the clinical diagnosis of hysteria. zahnärztlich-somatischer von psy- Hogrefe, Göttingen 2011
(Briquet‘s syndrome). Am J Psychiatry chischen Ursachen. Hanser, München
1975; 132: 138–141 1999 47. Wolowski A, Runte C: Somatische
Reaktionen nach restaurativer Therapie –
20. Haneke E: Zungen- und Mund- 33. Moral H, Ahnemann W: Über Grenz- somatisches oder psychosomatisches
schleimhautbrennen – Klinik, Differen- fälle. Korrespondenzblatt für Zahnärzte Krankheitsbild? Dtsch Zahnärztl Z 2013,
tialdiagnose, Ätiologie, Therapie. Hanser, 1921; 47: 56–86 68: 471– 482
München 1980
34. Müller-Fahlbusch H: Ärztliche Psy-
48. Wupper H: Das psychische Trauma
21. Henry JD, Crawford JR: The short- chologie in der Zahnmedizin. Thieme,
beim Zahnverlust und die Psychose des
form version of the Depression Anxiety Stuttgart 1992, S 19
Zahnersatzes. Zahnärztl Welt 1971; 80:
Stress Scales (DASS-21): construct validity
35. Nilges P, Essau C: Depression, Angst 1056–1061
and normative data in a large non-clinical
sample. Br J Clin Psychol 2005; 44: und Stress: DASS – ein Screeninginstru-
227–239 ment nicht nur für Schmerzpatienten.
Schmerz 2015; 29: 649–657
22. Herrmann C, Buss U: Vorstellung und
Validierung einer deutschen Version der 36. Peterhans P: Zur Psychologie und
Psychohygiene in der Prothetik. Med
(Photo: A. Wolowski)
„Hospital Anxiety and Depression Scale“
(HAD-Skala). Ein Fragebogen zur Er- Diss, Zürich 1948
fassung des psychischen Befindens bei 37. Roenneberg C, Sattel H, Schaefert R,
Patienten mit körperlichen Beschwerden. Henningsen P, Hausteiner-Wiehle C: Kli-
Diagnostica 1994; 40: 143–154 nische Leitlinie: Funktionelle Körper-
23. Holmes TH, Rahe RH: The social beschwerden. Dtsch Arztebl 2019; 116:
readjustment rating scale. J Psychosom 553–560
Res 1967; 11: 213–218 PD DR. ANNE WOLOWSKI
38. Rojo L, Silvestre FJ, Bagan JV, De
Poliklinik for Prosthetic Dental
24. International Headache Society: Vicente T: Psychiatric morbidity in burn-
Medicine and Biomaterials
International Classification of Orofacial ing mouth syndrome. Psychiatric inter-
Westfälische Wilhelms-Universität
Pain, (ICOP). Cephalalgia 2020; 40: view versus depression and anxiety
University hospital Münster –
129–221 scales. Oral Surg Oral Med Oral Pathol
Center ZMK
1993; 75: 308–311
25. Känel v R, Georgi A, Egli D, Acker- Albert-Schweitzer-Campus 1 / W30
mann D: Die somatische Belastungsstö- 39. Sabinski, E: Prothesenunverträglich- D-48149 Münster
rung: Stress durch Körpersymptome. keit in der Betrachtungsweise verschie- wolowsk@uni-muenster.de
© Deutscher Ärzteverlag | DZZ International | Deutsche Zahnärztliche Zeitschrift International | 2021; 3 (1)You can also read