KANSAS UNINTENTIONAL INJURY PREVENTION PLAN 2021-2025 - Department of Health and Environment
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
Department of Health
KANSAS
and Environment
UNINTENTIONAL
INJURY
PREVENTION
PLAN
2021-2025
MISSION
To build solid infrastructure
to improve the health of
Kansans by increasing
awareness and action to
reduce unintentional
injuries.
Kansas Unintentional Injury Prevention Plan 2021-2025
Kansas Department of Health and Environment
Lee A. Norman, M.D., Secretary
Ashley Goss, Deputy Secretary of Public Health
Alix Guerrero, Equity Manager
Bureau of Epidemiology and Public Health Informatics
Farah Ahmed, State Epidemiologist & Environmental Health Officer
Yidan Pei, Epidemiologist, Injury & Violence Prevention Programs
Danielle Sass, Senior Epidemiologist, Kansas Trauma Program
Bureau of Health Promotion
Ryan Lester, MPH, Director
Stefanie Olson, Program Coordinator, Sexual Violence Prevention & Education
Cherie Sage, State Director, Safe Kids Kansas
Daina Zolck, Director, Injury & Violence Prevention Programs
For additional information, please contact:
Daina Zolck, Section Director
Injury & Violence Prevention Programs
Bureau of Health Promotion,
Kansas Department of Health and Environment
1000 SW Jackson, Ste 230, Topeka, KS 66612
or call 785-925-1018, or email Daina.Zolck@ks.gov.
Kansas Department of Health and Environment’s Mission:
To protect and improve the health and environment for all Kansans.
Funding
This plan is supported by funding from the Preventive Health and Health Services Block Grant, Centers
for Disease Control and Prevention, Atlanta, GA. Its contents are solely the responsibility of the authors
and do not necessarily represent the official views of the Centers for Disease Control and Prevention.
Recognition
Sincere appreciation to DCCCA, Inc. for its role and dedication in the development, organization, and
production of this plan.
December 2020
1
To protect and improve the health and environment for all Kansans.
Plan Preparation
Kansas Unintentional Injury Prevention State Plan Steering Committee
Acknowledgements
The following individuals participated in development of the Kansas Unintentional Injury
Prevention State Plan:
*Steering Committee Member
Jean Akuhlman Crystal Dalmasso*
Lindsborg Hospital DCCCA
Krista Alanis Candace Davidson
Northwest Kansas Ambulance Service Reno County Health Department
Deanne Armstrong* Olivia Desmarais
DCCCA University of Kansas Health System
Stefanie Baines* Kelli Devine
Kansas Poison Control Center Republic County Hospital
Rynekah Barbour Jennifer Donnelly*
Johnson County Health Department Kansas Board of Pharmacy
Ashlee Barkley* Tanya Ewert
Kansas Department of Health and Environment Anderson County Hospital
Julia Baughman* Sarah Finch
Kansas Department of Health and Environment McPherson Center for Health
Kayzy Bigler* Stuart Funk
Kansas Department of Health and Environment Butler County EMS
Sadie Birchard Lydia Fuqua*
YMCA of Greater Kansas City DCCCA
Danielle Bohl Alix Guerrero*
Phillips County Hospital Kansas Department of Health and Environment
Misti Bond Leslie Hale
Labette Health Kansas Department of Health and Environment
Candice Breshears Jean Hall
Kansas Highway Patrol University of Kansas
David Caudill Lisa Harper
Gove County Medical Center DCCCA
2
To protect and improve the health and environment for all Kansans.
Jill Cavender Adrienne Hearrell*
Kansas Department of Health and Environment Kansas Department of Health and Environment
Pam Chaffee Paula Hofmeister
US Coast Guard Auxiliary Clara Barton Hospital
Sara Hortenstine* Stefanie Olson*
Child Death Review Board Kansas Department of Health and Environment
Kelly Ingold* Yidan Pei*
Kansas Fire Marshal’s Office Kansas Department of Health and Environment
Tenille Kimberlin* Gustavo Ramirez*
DCCCA/Kansas Traffic Safety Resource Office Kansas Highway Patrol
Kelsey King Melissa Rau
Labette Health Kansas Department of Transportation
Allison Koonce Cherie Sage*
Lawrence Memorial Hospital Health Kansas Department of Health and Environment
Phyllis Larimore* Danielle Sass*
Children's Mercy Hospital Kansas Department of Health and Environment
Karl Leech Christy Schunn
Minneapolis Ambulance Service KIDS Network
Ryan Lester Julie Sergeant
Kansas Department of Health and Environment Kansas Department of Health and Environment
Krista Machado* Rachel Sisson*
DCCCA Kansas Department of Health and Environment
Chrissy Mayer* Courtney Strathman
DCCCA Nemaha Valley Community Hospital
Dot Nary Teresa Taylor*
Kansas Disability and Health Program Stormont Vail Health/Kansas Emergency Nurses
Association
Britney Nichols Darlene Whitlock*
Kansas Department of Health and Environment Kansas Emergency Nurses Association
Wendy O'Hare* Jeffrey Wilhelm*
Kansas Department of Health and Environment Kansas Department of Health and Environment
3
To protect and improve the health and environment for all Kansans.
Table of Contents
Executive Summary..................................................................................................................................... 5
KDHE Injury & Violence Prevention Programs............................................................................................ 6
Introduction ................................................................................................................................................ 8
Kansas Unintentional Injury Prevention Plan ............................................................................................. 9
Healthy Equity and Shared Risk and Protective Factors ........................................................................... 13
State Plan Indicators ................................................................................................................................. 16
Poisoning ................................................................................................................................................... 18
Motor Vehicle Crashes .............................................................................................................................. 23
Falls ........................................................................................................................................................... 28
Suffocation ................................................................................................................................................ 32
Fire/burn ................................................................................................................................................... 36
Drowning................................................................................................................................................... 41
4
To protect and improve the health and environment for all Kansans.
Executive Summary
Unintentional injuries are the leading cause of death among people ages 1-4 and 10-44 years old in
Kansas in 2016-2019. The following statistics highlight the burden of unintentional injuries among
Kansas residents from 2016 to 2019:
• 5,915 deaths (Death rate = 46.7 every 100,000 Kansans)
• 53,247 hospitalization (Rate = 403.7 every 100,000 Kansans)
• 763,793 emergency department visits (EDVs) (Rate = 6,583.5 every 100,000 Kansans)
• Nearly 119 thousand years of potential life lost (YPLL) before age 75 due to the fatal injuries
• The three most common specified causes of deaths consist of 77% of total unintentional injury
deaths:
o falls (29%, n=1,727)
o motor vehicle traffic (MVT) accidents (27%, n=1,609)
o poisoning (21%, n=1,230)
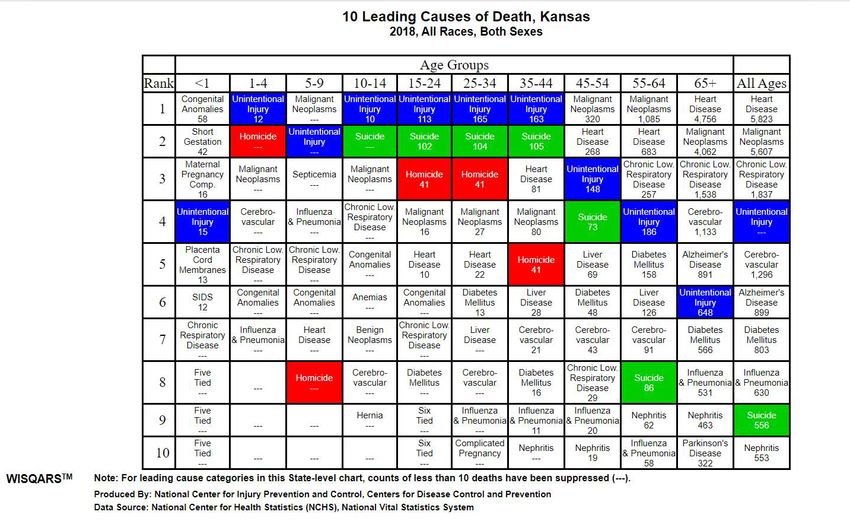
The table below shows the 10 leading causes of death in Kansas in 2018. Unintentional injury, shown in
blue, highlights the burden of unintentional injuries across the lifespan. An individual’s risk of injury
may be impacted by social, personal, economic, and environmental factors. Understanding the
determinants of health and identifying risk and protective factors are key to improving the safety of
Kansans.
It is common to consider unintentional injuries as accidents or random events. However, this implies
outcomes are inevitable. We know that unintentional injuries are both predictable AND preventable,
and there is a need to raise awareness of unintentional injury as a leading public health issue and
educate communities on effective interventions.
5
To protect and improve the health and environment for all Kansans.
KDHE Injury & Violence Prevention Programs
Mission
To build solid infrastructure to improve the health of Kansans by increasing awareness and action to
reduce injuries and violence.
Vision
To provide technical assistance to local and state partners to assess the burden of injury and violence,
assure interventions, and facilitate policy development.
Data collection
Data is critical to informing public health priorities and needs. It can be used to determine how often
unintentional injuries occur, where they occur, trends, and who is affected. At KDHE, the Bureau of
Epidemiology and Public Health Informatics is responsible for collecting, analyzing, and interpreting
data that provide information on a variety of conditions of public health importance, including
unintentional injuries, and on health status of the population.
Programs
The Office of Injury Prevention and Disability Programs was established in 1993 within the Bureau of
Health Promotion at the Kansas Department of Health and Environment (KDHE). A disability grant and
the Preventive Health and Health Services Block Grant (PHHSBG) from the Centers for Disease Control
and Prevention (CDC) provided initial funding for the office. The office has evolved into KDHE Injury &
Violence Prevention Programs and currently includes Safe Kids Kansas, the Kansas Sexual Violence
Prevention and Education Program, Kansas Violent Death Reporting System, Kansas Essentials for
Childhood Initiative and Implementation of Zero Suicide in Health Systems in Kansas.
The Safe Kids Kansas Coalition, established in 1993, is a nonprofit coalition of statewide and regional
organizations and businesses with the mission to prevent unintentional childhood injury to Kansas
children ages 0-19. The coalition network includes 30 local coalitions covering 36 counties and 74.8
percent of the Kansas child population. In addition to CDC funding through PHHSBG, Safe Kids also
receives funding from private sources to support work in the primary prevention of injury.
Safe Kids Kansas has received several awards for their work including the following:
• Outstanding Safe Kids Day Event, Safe Kids Worldwide, 2015
• Excellence in Communications, Safe Kids Worldwide, 2013
• The first Dr. Robert Sanders Award for Outstanding Public Policy Achievement in Child
Passenger Safety, Safe Kids Worldwide, 2006
• Coalition of the Year, Safe Kids Worldwide, 2004
For more information about Safe Kids Kansas, please visit www.safekidskansas.org.
The Sexual Violence Prevention and Education (SVPE) Program, funded by the Centers for Disease
Control and Prevention (CDC) since 1995, engages in a range of activities including prevention
strategies, educational seminars, professional training and leveraging resources through partnerships.
The SVPE program encourages the development of comprehensive prevention strategies to address all
6
To protect and improve the health and environment for all Kansans.
levels of the social ecological model. Additional information about SVPE is available at
https://www.kdheks.gov/rpe/index.html.
The Kansas Violent Death Reporting System (KSVDRS), funded by CDC since 2014, provides a clearer
understanding of violent deaths to guide decisions about efforts to prevent violence and track progress
over time. KSVDRS is the only state-based reporting system that pools data on violent deaths from
multiple sources into a usable, anonymous database. These sources include state and local medical
examiner, coroner, law enforcement, crime lab, and vital statistics records. KSVDRS covers all types of
violent deaths including homicides and suicides in all settings and for all age groups. KSVDRS may
include data on mental health problems, recent problems with a job, finances or relationships, physical
health problems, and information about the circumstances of death. Such data is far more
comprehensive than what is available elsewhere. Please visit
https://www.kdheks.gov/idp/KsVDRS.htm for more information on KSVDRS.
The Kansas Essentials for Childhood Initiative, funded by CDC since 2019, is led by the Kansas Power of
the Positive (KPoP), a statewide coalition that is committed to all Kansas children growing up in safe,
stable, nurturing relationships and environments. The coalition focuses on societal level interventions
to prevent adverse childhood experiences and believes the conditions in which families live, including
influence of family friendly workplace policies and practices, are key. Learn more about Kansas
Essentials for Childhood Initiative at http://www.kansaspowerofthepositive.org/.
The Implementation of Zero Suicide in Health Systems, funded by the Substance Abuse and Mental
Health Services Administration (SAMHSA) in 2020, supports safer suicide care in behavioral health and
healthcare systems. Zero Suicide is a model and framework that believes suicide deaths for individuals
under the care of health and behavioral health systems are preventable. For systems dedicated to
improving patient safety, Zero Suicide presents a framework for systemwide transformation toward
safer suicide care. This work will involve key partners across the state, including Veterans Affairs and
the 26 licensed Community Mental Health Care Systems that have more than 4,500 staff supplying
mental health services in every county (120+ locations) to more than 140,000 Kansans annually.
Besides the policies, protocols and practices the Zero Suicide model supports, objectives include
supplying evidence-based trainings and practices to support a prepared, competent and confident
mental health workforce and coordinated suicide prevention efforts across the state.
7
To protect and improve the health and environment for all Kansans.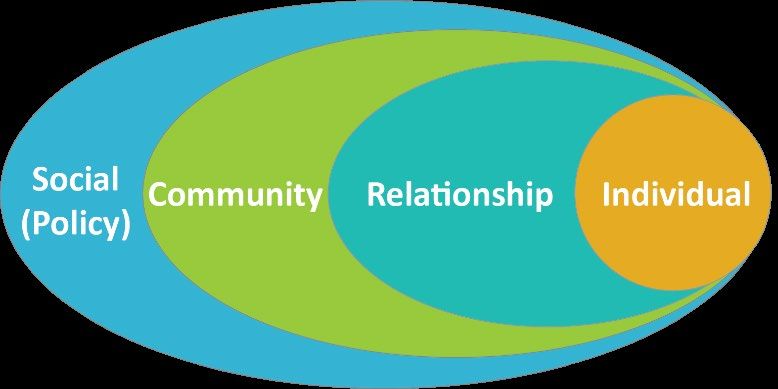
Introduction
Defining Injury
Injuries are typically categorized in terms of mechanism and intent. Mechanism (or cause) typifies how
the injury occurred— for instance motor vehicle, firearm, struck by an object, falling, etc. Intent is
classified as unintentional or intentional. While unintentional injuries often result as a form of rapid
transfer of energy from object to person (e.g., being struck by a motor vehicle), intentional injuries are
the result of intentional harm imposed upon one person by another, or upon oneself (e.g., suicide).
Injury as a Public Health Issue
Public health focuses on the wellbeing of entire populations by seeking to understand the roots of a
problem and then prevent it from occurring. The public health approach to unintentional injury
prevention involves identifying and defining the
problem, identifying risk and protective factors,
developing and testing prevention strategies, and
assuring widespread adoption of effective
strategies. Instead of focusing on the treatment of
individual injuries as they arise, public health
focuses on broad causes and prevention solutions.
Sometimes, prevention at the community level involves changing the environment in which injuries
occur. For example, installing traffic signals at intersections or requiring certain products to be fire safe.
At other times prevention at the community level involves education. For example, informing school
programs about preventing traumatic brain injuries or providing information to guide changes in health
policies or laws. Although the public health workforce may not always directly provide prevention
services, public health agencies identify the important conditions and patterns that contribute to
unintentional injury at the community level and identify and leverage solutions through community
partnerships to promote prevention.
Unintentional Injury
Unintentional injury is the most common type of fatal injury in Kansas. From 2016 to 2019,
unintentional injuries were the cause of 67% of all fatal injuries among Kansans. All ages, sexes, races
are at risk of unintentional injuries. The bullet points below demonstrate that while all are at risk, there
are populations that have a higher burden of incidents:
• Men in Kansas are twice as likely to die from unintentional injuries as women.
• Adults ≥85yrs had the highest risk of dying or being hospitalization due unintentional injuries.
• Emergency Department Visits (EDV) for adults ≥85yrs and young children 1-4 years old were
more likely to be for treatment or care of unintentional injuries.
• Hispanics had a death rate due to unintentional injury 19% higher than the state average.
• Non-Hispanic Blacks and Whites were more likely to visit ED or be hospitalized for unintentional
injuries than others.
• The less population-dense regions (Frontier, rural, and densely-settled rural counties) had
higher death rates than state average.
• The death rate due to poisoning had a statistically significant increase of 36% between 2016 to
2019 (9.5 versus 12.9 per 100,000 populations).
8
To protect and improve the health and environment for all Kansans.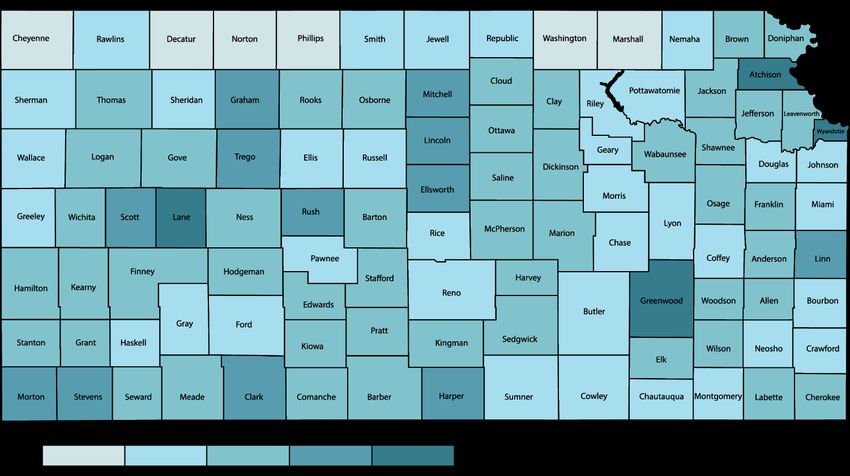
Kansas Unintentional Injury Prevention Plan
This plan builds on the previous plan, 2016-2020 Kansas Injury Prevention Plan, and focuses on
unintentional injuries. Subject matter experts from committed and passionate partners were relied
upon for development of this plan and identified the need for continued focus on raising awareness,
building capacity, and implementing policies, practices, and protocols that support unintentional injury
prevention. Kansas has other strategic plans already developed for other injury and violence areas:
• Child Health Advisory Committee: Kansas Blue Ribbon Panel on Infant Mortality
• Kansas Prescription Drug and Opioid Misuse and Overdose Strategic Plan
• Kansas Strategic Highway Safety Plan
• Kansas Sexual and Domestic Violence Prevention Plan
• Kansas Suicide Prevention Plan
• State of Kansas Child Maltreatment Prevention Plan
In reviewing the other state strategic plans
with focus on injury and violence
prevention, it is important to recognize that
across the various entities we might use
different terms or language, but we hold
the same goal, the safety of our Kansans.
We also often have shared priorities and
common challenges. This provides
opportunities for collaboration, alignment
of strategies, shared communication, and
identification of resources to address social
determinants of health.
Goals
• Increase public awareness about unintentional injury prevention.
• Identify the connection between all unintentional injury prevention areas and provide
interventions that focus on shared risk and protective factors.
• Increase health equity across all unintentional injury prevention areas by tailoring interventions
to meet the needs of all Kansans.
• Create an unintentional injury prevention plan that is accessible for all Kansas communities.
• Build the capacity of communities to develop and implement effective unintentional injury
prevention programs.
• Utilize Kansas-specific injury data to inform unintentional injury prevention goals and
strategies.
• Establish permanent funding for unintentional injury prevention initiatives.
• Increase collaboration with community partners to implement unintentional injury prevention
strategies.
• Develop a process for monitoring and evaluating the implementation of the Kansas
Unintentional Injury Prevention Strategic Plan.
• Increase the use of evidence-based unintentional injury prevention interventions.
• Increase the priority level for unintentional injury prevention issues among policymakers.
9
To protect and improve the health and environment for all Kansans.Recommendations/Enhancing Injury Prevention
The Safe States Alliance identifies the following six core components as essential, foundational
elements of an effective injury and violence prevention program:
1. Build and sustain a solid, stable infrastructure
2. Collect, analyze and disseminate injury data
3. Select, implement and evaluate effective program and policy strategies
4. Engage partners for collaboration
5. Effectively communicate information to key stakeholders
6. Training and technical assistance
Stakeholders have identified the following limitations and barriers to a robust unintentional injury
prevention system in Kansas:
• Unintentional injury prevention work is happening in pockets and silos, shared risk and
protective factors and strategies may be overlooked
• Failure to leverage existing initiatives, especially across injury areas and between different
groups
• Data is available however there is a need for more specific data to drive decision making
• People at the local level wear multiple hats and find it difficult to completely focus on injury
prevention
• Limited funding and competition for limited available funding
• Some current state laws/policies are weak and do little to change behavior
• General lack of awareness by the public of unintentional injury risks and prevention
opportunities
Stakeholders have also identified the need for all unintentional injury areas to include the following
overarching priorities:
• Increasing awareness of unintentional injury risk prevention via the utilization of traditional and
social media with new data and increase tactical use of social media
• Ensure that all information, resources, strategies, and programs are equitable across all
populations as well as accessible to those with disabilities
• Identify strategies that target those that are at the highest risk for unintentional injury
• Implement strategies that target shared risk and protective factors across unintentional injury
areas
• Further review unintentional injury prevention data to include additional analysis and review
literature to identify disparate populations
Recommendations for Virtual Adaptations
Stakeholders discussed virtual adaptations due to the challenges that 2020 has presented due to the
global pandemic. Many strategies for each injury prevention area can be adapted virtually, including
education and awareness activities. Additionally, there are many opportunities to further reach
isolated populations through virtual adaptations. Current evidence is demonstrating that older adults
are not conducting regular wellness visits during the pandemic (March 2020-current) or flu season,
similar patterns are seen for well-child visits and wellness visits in general. Regular wellness visits and
10
To protect and improve the health and environment for all Kansans.medication screenings are an essential piece of injury prevention. Telehealth may be utilized as a
strategy to ensure regular wellness visits can occur safely. Exploring options available through
Medicare can ensure that services needed are received (i.e. ensuring necessary technology is available
for services). While some programs cannot be fully adapted to a virtual environment, some
components can be.
Overview of the Planning Process
11
To protect and improve the health and environment for all Kansans.Overview of the plan
This Unintentional Injury Prevention Plan focuses on the top six
unintentional injury areas and their shared risk and protective factors.
In Kansas between 2016-2019, unintentional injury caused 1,501
deaths, 13,933 hospitalizations, and 200,202 emergency
department visits.
The top six injury areas in 2019 were as follows: Poisonings, Motor
Vehicle Crashes, Falls, Suffocation, Fire/burn, and Drowning. It is
important to consider the shared risk and protective factors for each
of these unintentional injury areas.
This plan includes the following strategies:
Prevent Poisoning
• Increase education and awareness on poison risks, prevention resources, and strategies
• Increase the utilization of K-TRACS
• Promote the safe use, storage, and disposal of medications and hazardous household items
• Raise awareness of risks, signs and symptoms, and resources for the prevention of carbon
monoxide and lead poisoning
Decrease Motor Vehicle Crash-related Injuries and Death
• Increase awareness and education programming
• Increase restraint use, increase enforcement of laws, and increase safe roadway engineering
• Enhance the trauma system and create a data repository
Prevent Falls
• Increase participation in fall prevention programs and increase awareness of risk factors for
falls
• Develop an active state coalition with regional networks
• Further analyze falls data to identify disparate populations
Reduce Suffocation
• Increase education and awareness of suffocation risks, prevention strategies, and resources
• Increase access to suffocation data
Decrease the Number of Fire and Burn Related Injuries and Death
• Increase awareness and provide education and resources that supports best practice in fire
prevention, oxygen safety, and safety plans
• Further review fire and burn data to include additional analysis and review literature to identify
disparate populations
Reduce Drownings
• Increase education and awareness of drowning risks, prevention strategies, and resources
• Enhance efforts related to the primary and secondary prevention of drowning
• Further analyze drowning data to identify disparate populations
12
To protect and improve the health and environment for all Kansans.Healthy Equity and Shared Risk and Protective Factors
Health Equity
Health equity means that everyone has a fair
and just opportunity to reach their highest level
of health. It requires removing barriers to
health and their consequences. For example,
people who experience barriers such as poverty
and discrimination also experience a lack of
access to good jobs with fair pay, quality
education, housing, and health care which leads
to poorer health outcomes. In unintentional
injury prevention, we must tailor our © Robert Wood Johnson Foundation 2017
interventions to meet the needs of all people.
For more information about the public health framework for reducing health inequities visit
https://www.barhii.org/barhii-framework.
Applying a Health Equity Lens
1 2 3 4 5
Compare the most Use systemic Authentically Consider cultural Review all work for
advantaged groups framing to focus engage with competency and equity including
with less on root causes your community implicit biases. implicit bias and
advantaged groups and examine the with equal explicit equity.
instead of the context in which consideration for
overall or average. people live. all groups.
Ask: in our injury Examine: the Commit to: full Evaluate: do we Work: to identify
prevention area, do effects of transparency, have the skills to implicit bias and
we know what disparities across accountability, apply equity and foster equity
groups are being systems and the and justice to our through active
affected the most, impact of systems collaboration in work? Are we engagement and
or more than other treating people the co-creation trained to be empowerment of
groups? Set specific unfairly. and co- culturally and the stakeholders
goals that target ownership of linguistically and community
those specific solutions. competent? members.
populations.
KDHE recognizes that social, economic, and environmental inequities are rooted in our history and
continue to result in adverse health outcomes today. These structural inequities have greater influence
on health outcomes than access to health care or an individual’s choices. They affect communities
differently and we acknowledge that improving health equity and reducing disparities through policies,
processes, and systems can help improve the health and wellbeing of all Kansans.
13
To protect and improve the health and environment for all Kansans.Shared Risk and Protective Factors
Shared risk and protective factor (SRPF) approaches are efforts to improve multiple population health
and quality-of-life outcomes by aligning diverse, multi-sector interventions that positively and
equitably impact the social determinants of health. The social determinants of health include factors
such as employment, income, housing, transportation, childcare, education, discrimination, and the
quality of the places where people live, work, learn, pray, and play, including access to a quality
affordable healthcare system.
A Shared Risk and Protective Factor Approach:
Improves multiple population outcomes
Impacts the social determinants of health
in ways that are positive and equitable
Engages partners across multiple disciplines
and sectors
SRPF examines how we can work more effectively using an upstream approach to figure out why these
problems are occurring and how we can address some of the root causes related to the social
determinants of health. A technique to discover the root causes of a problem is to ask the 5 Why
questions. In the above image, asking questions about why there are suddenly so many more people
in the hospital will eventually lead us to walk up the river and find the broken bridge. Fixing the bridge
will prevent the immediate issue (people being harmed in the river) more effectively than trying to
educate each individual about the potential for harm, but may also improve other conditions like
economic problems by providing access to the other side of the river where better jobs at the hospital
are, and could even reduce rates of chronic diseases like heart disease and diabetes by making exercise
easier.
The Social Ecological Model
The Social Ecological Model can be used as a guide for prevention efforts. This model helps to
understand how risk and protective factors can be influential at the individual, relational, community
and societal levels and how each level can influence another. For example, one’s experiences at the
14
To protect and improve the health and environment for all Kansans.individual level can impact their relationships. Prevention efforts are most effective and impactful
when addressing all levels of the Social Ecological Model. While the crux of the public health approach
to unintentional injury prevention is at the societal and community level, often proven programs
implemented in Kansas communities support increasing individual’s safety (i.e., older adult falls
prevention classes, car seat education and distribution, and swim lessons). Prevention is more effective
and can have a bigger impact if we expand our focus to include strategies that address multiple levels.
The Safe States Alliance identified six shared risk and protective factors for unintentional injury, they
are:
Approaching unintentional injury prevention through the utilization of shared risk and protective
factors allows us to better address root causes and be more effective in unintentional injury prevention
work.
15
To protect and improve the health and environment for all Kansans.State Plan Indicators
Injuries are a major public health issue and have significant impact on the well-being of Kansans.
Injuries can affect anyone, regardless of age, sex, race, or socioeconomic background. While injuries
cause a significant burden, they also are largely preventable. Data collection is the first step in the
public health approach with accurate information being key to directing, designing, implementing, and
evaluating unintentional injury prevention efforts.
From 2016-2019, 5,915 Kansans died from unintentional injuries, 53,247 were hospitalized, and
763,793 had an emergency department (EDV) visit due to unintentional injuries. The breakdown by
each unintentional injury area from 2016-2019 are as follows:
The graph below shows the age-adjusted death rate per 100,000 for each unintentional injury area, per
year from 2016 – 2019. Poisonings showed a steady rise, and, in 2019, surpassed the rate of Motor
Vehicle Crashes and Falls.
Unintentional Injury Death, Age-Adjusted Rate per 100,000
14
12
10
8
6
4
2
0
2016 2017 2018 2019
Drowning Fall Fire/Burn MVC Poisoning Suffocation
16
To protect and improve the health and environment for all Kansans.The map below shows the burden of all unintentional injury deaths (age-adjusted rate per 100,000) by
population density1 from 2016-2019. Frontier counties (dark blue) had the highest rate (65.8 per
100,000), followed by Rural (58.7 per 100,000), Semi-Urban (47.9 per 100,000), and Urban (42.6 per
100,000). Death rates from Frontier and Rural counties were not statistically significantly different. The
rates for counties with unintentional injury deaths < 20 are not shown.
The map below shows the burden of all unintentional injury hospitalizations (age-adjusted rate per
100,000) by county from 2016-2019, showing the age-adjusted rates by county.
Please see the Kansas Unintentional Injury State Action Plan data dashboard for more information and
data: https://www.kdheks.gov/idp/core_injury.html.
___________
1 Counties grouped by population density in persons per square mile (ppsm); frontier < 6.0, rural 6.0-19.9, densely-settled rural 20.0-39.9,
and urban ≥ 150.0.
17
To protect and improve the health and environment for all Kansans.Poisoning
Introduction
Related to unintentional poisoning in Kansas, from 2016-2019 there were 1,230 deaths, more than
4,400 hospitalizations, and nearly 13,000 emergency department visits in 2016-2019. Poisonings are
the third leading causes of unintentional injury death in Kansas. The Kansas Poison Control Center
reports that a majority of the most serious calls they receive are among those in the age groups of
adolescence through older adulthood. Poisoning injuries and deaths happen in a variety of settings.
However, this plan focuses on prevention of poisonings in residences.
Objectives
1. Prevent an increase in the number of unintentional poisoning deaths by 2025
2. Prevent an increase in number of unintentional poisoning related hospitalizations by 2025
3. Prevent an increase in the number of unintentional poisoning related emergency department
visits by 2025
Goals
• Increase awareness of poison risks, prevention, and resources
• Improve and increase individual health literacy on medication safety
Increase the number of registered and approved DEA-licensed prescribers and the total number
of patient queries in K-TRACS, the Prescription Drug Monitoring Program in Kansas
• Increase the safe use, storage, and disposal of medications and other hazardous household
items
Strategies, and Actions
To decrease poisonings the plan includes a public education campaign, increasing health literacy on
poison prevention and safety, expanding use of the K-TRACS System and increasing the safe use,
storage, and disposal of medications and other hazardous household items. Strategies and actions to
accomplish these objectives include the following:
• Include Poison Control Center’s number on resource lists
• Utilize traditional and social media with new data and increase tactical use of social media
• Provide medication safety education to various audiences; virtually and in person
• Create incentive programs and accountability steps for prescribers and pharmacists to use
K-TRACS
Evaluate legislative, local, and organizational policy interventions
18
To protect and improve the health and environment for all Kansans.• Disseminate protocols for drug-take back programs
• Provide public education and outreach on drug-take back programs and in-home disposal
• Promote safe use, storage, and disposal of medications and poisonous household products
• Increase blood lead testing and statewide surveillance for elevated blood lead levels
• Increase awareness of risks, signs and symptoms, and resources for the prevention of carbon
monoxide poisoning and lead poisoning
Best Practices
Potential Resources and Partners
and Programs
• Hunter and Scout Poison Patrol • 911 Dispatchers
program • County health departments
• Operation Prevention • Emergency Medical Services (EMS), Fire Departments
• Older Adult Medication Safety • Hospitals
program • Kansas Board of Pharmacy
• Scholastic OTC Medicine Safety • Kansas Department for Aging and Disability Services
• Poison Prevention for Child • Kansas Poison Control Center
Care Providers training • KDHE Injury Epidemiologist
• Kansas Childhood Lead • Safe Kids Kansas
Poisoning Prevention Program - • Schools
866-UnleadedKS • Department for Children and Families
• KDHE Residential Lead Hazard • Primary Care Providers, pediatricians
Prevention Program • Drug Endangered Children Alliances
• Get Alarmed Program for • Child Care Providers
smoke and carbon monoxide • Indian Health Services
detectors • Housing authority
Target Populations Protective Factors
• Youth and older adults • Livable wages
• 25-64 age group • Physical and mental health wellness
• Parents, general adults • Supportive relationships
• White Males • Health insurance
• Marginalized Racial and Ethnic Groups • Adequate access to providers
including Non-Hispanic Blacks • Positive family/peer role models
• Low literacy (including non-English speaking) • Lack of family/peer substance misuse
• Individuals with disabilities and/or chronic • Patient education
disease (all ages) • Utilizing only one pharmacy
• Tribal Communities • Strong support systems
• Public awareness
19
To protect and improve the health and environment for all Kansans.Goal #1: Design/initiate a public education/awareness campaign to increase awareness of
the problem of poisoning
Strategies
1.1 Increase awareness of 1.2 Increase distribution 1.3 Increase knowledge of 1.4 Create social media
the Poison Control hotline and use of poison data potential poison hazards package
1-800- 222-1222
Actions
1.1a Include Poison 1.2a Widely distribute 1.3a Develop awareness 1.4a Develop common
Control Center 800 news releases and social materials messages
number on resource lists media when new data is
(printed and electronic) available, including data
1.3b Continue to develop 1.4b Enhance/maintain
from KDHE data
and disseminate annual Facebook page
dashboards
calendar with poison
prevention messaging
1.4c Enhance/maintain
Twitter presence
1.3c Develop materials on
poison hazards as a priority
including medications,
household products, carbon
monoxide, lead, etc.
1.3d Raise awareness of risks
and signs and symptoms of
poison hazards
1.3e Raise awareness of
resources to prevent poison
risks such as where to access
carbon monoxide detectors,
how to identify and mitigate
lead exposure, how to
reduce access to
medications and medication
mistakes/misuse, etc.
20
To protect and improve the health and environment for all Kansans.Goal #2: Improve and increase individual health literacy on medication safety.
Strategies
2.1 Provide medication safety education to various audiences; virtually and in person
Actions
2.1a Implement American Association of Poison Control Centers Over the Counter (OTC) curriculum for youth
2.1b Continue to implement Hunter and Scout programming
2.1c Ensure materials and trainings are accessible to those with disabilities
2.1d Continue the statewide implementation of the Older Adult Medication Safety training for older adults and
their caregivers
Goal #3: Increase the number of registered and approved DEA-licensed prescribers and the
total number of patient queries in K-TRACS.
Strategies
3.1 Ensure prescribers and pharmacists are registered with K-TRACS
Actions
3.1a Provide toolkits and resources to providers on patient safety
3.1b Encourage all ERs and urgent care centers to utilize K-TRACS
3.1c Continue to increase the number of prescribers listing their specialty in K-TRACS
3.1d Ensure prescribers and pharmacists registered are implementing best practices and/or increase coordination
of care practice through K-TRACS usage
3.1e Create incentive programs; explore recognizing providers or programs that shine in the use of K-TRACS
21
To protect and improve the health and environment for all Kansans.Goal #4: Increase the safe use, storage, and disposal of medications and other hazardous
household items.
Strategies
4.1 Develop user friendly protocols for 4.2 Promote the safe use, storage, and disposal of medications and other
drug destruction programs hazardous household items
Actions
4.1a Disseminate protocols to nursing 4.2a Raise awareness of poison risks associated with medications and
homes, hospitals, law enforcement other hazardous household items
agencies, pharmacies, and community
take-back programs 4.2b Promote the safe use of medications and other hazardous
household items and associated resources
4.1b Provide education and outreach
to the general public for drug 4.2c Promote the safe storage of medications and other hazardous
destruction programs household items and associated resources such as lockbox programs and
storage protocols
4.2d Promote the safe disposal of hazardous household items, such as
proper disposal guidelines
4.2e Raise awareness of available resources for proper medication
disposal
4.2e(i) All drug collection programs must be registered through the
Kansas Board of Pharmacy. Because of this, the Kansas Board of
Pharmacy is now tracking all collection programs in our state and this
information can be found on their website
4.2e(ii) Raise awareness of free in-home disposal resources available
through DCCCA and the Kansas Poison Control Center
22
To protect and improve the health and environment for all Kansans.Motor Vehicle Crashes
Introduction
Regarding vehicle miles travel-related crashes that occur on public roadways in Kansas, there were
1,609 deaths, more than 6,300 hospitalizations, and more than 67,000 emergency department visits
between 2016 and 2019. Motor vehicle crashes are the 2nd leading cause of unintentional injury
death.
Objectives
1. Decrease the number of motor vehicle crash deaths by 5% by 2025
2. Decrease the number of motor vehicle crash related hospitalizations by 5% by 2025
3. Decrease the number of motor vehicle crash related emergency department visits by 5% by
2025
Goals
1. Reduce crash-related injury rate per vehicle miles traveled in the state by 5%
2. Reduce crash death rate per vehicle miles traveled (VMT) (100 million miles) in the state by 10%
Strategies and Actions
To decrease crash-related injuries and death, the plan focuses on increased restraint use, education
programs, enforcement of laws, safe roadway engineering, enhancing the trauma system and creating
a data repository. Strategies and actions to accomplish these objectives include the following:
• Promote the Safety Break! Program for ages 9-14 and SAFE Program in high schools
• Continued enforcement of the seat belt law
• Enhance and enforce the Graduated Driver’s License law
• Increase driving assessments for physical and cognitive ability and promote frequent testing
• Create and promote distracted driving messages
• Strengthen distracted driving laws and ensure enforcement
• Develop and require roadway signage including median and train crossings, and implement
safety features
• Create a data repository for crashes, injuries, and fatalities, and map high crash areas
• Ensure enhanced 911 is available statewide
• Provide funding for trauma training to healthcare providers
• Promote use of CDC field triage guidelines
23
To protect and improve the health and environment for all Kansans.• Increase collaboration between EMS and hospital providers
• Maintain a Level 3 or higher trauma center in each region
• Maintain and enhance child safety seat programs
• Enforce impaired driving laws, rules, and regulations
Best Practices
Potential Resources and Partners
and Programs
• Seat Belts are For • Child Death Review • Kansas Traffic Safety Resource Office
Everyone (SAFE) Board • Kansas Hospital Association
• CPST Certification & • Emergency Medical • KDHE Maternal Child Health
Recertification Training Services (EMS) • Local law enforcement
• Kansascarseatcheck.org • Fatality Analysis • Safe Kids
• AAA CarFit Reporting System • Schools, colleges
• Booster to Belts • Hospitals • State Farm
• Safety Break • Kansas Department of • Youth groups
• www.KTSRO.org Transportation • AAA
• Drivers Ed Toolkit • Kansas Highway Patrol • Area Agencies on Aging, ADRC
• Standardized Field • Child Care Providers • Department of Revenue
Sobriety Testing (SFST) • Health Departments, • Tribal communities
• Advanced Roadside WIC offices • FHWA
Impaired Driving • Healthcare providers • NHTSA
Enforcement (ARIDE) (PCPs, OBGYNs, • KS Wildlife and Parks
• Drug Recognition Expert optometrists, etc.) • Railway Companies
(DRE) • Alzheimer’s Association • Kansas Medical Society
• Countdown2Drive • American Association of • Regional trauma councils
• Eisenhower Legacy Retired Persons (AARP)
Transportation Program • Brain Injury Association
• Be Responsible and Keep of Kansas, Spinal Cord,
Everyone Safe (BRAKES) TBI, and other Injury
• Older Driver Safety Groups
Courses
Target
Protective Factors
Populations
• Men • Mental Health Wellness
• Tribal communities • Marital status
• Hispanic population • Seatbelt Use
• 25-34 year old age group • Group Norms That Promote Safe Driving Practices
• Rural drivers, agricultural • States that enforce mobile device use laws
drivers, pickup drivers • Positive role models displaying responsible driving and health
• Older drivers (55-64, 65+) behaviors
• Children • Workplace norms around not taking calls while driving
• Teen and novice drivers • Timely access to care and first responder response
24
To protect and improve the health and environment for all Kansans.Goal #1: Reduce crash-related injury rate per vehicle miles traveled (VMT) in the state by
5%
Strategies
1.1 Increase 1.2 Provide 1.3 Increase 1.4 Provide education, 1.5 Enforce laws, rules,
restraint use education awareness of the resources and programs and regulations related
programs for Graduated for older drivers to drivers (including older
novice drivers Driver’s License adults)
law
Actions
1.1a Promote 1.2a Utilize SAFE 1.3a Educate the 1.4a Promote the AAA 1.5a Increase driving
the Safety Program public and raise CarFit program assessments for both
Break! program, awareness of physical and cognitive
Seat Belts are 1.2b Eisenhower Graduated 1.4b Promote the ability
For Everyone Legacy Driver’s License NHTSA Older Driver
(SAFE), Boosters Transportation law Safety 1.5b Promote more
to Belts, Bucks 4 Program – Driver frequent drivers license
Buckles, and Education 1.3b Reevaluate testing as you age
1.4c Promote the AARP
other programs Reimbursement the Graduated Smart Driver Program
Grant Driver’s License 1.5c Educate health
1.1b Continue to Law and look for care providers and LE
1.4d Promote the
enforce seat belt 1.2c Promote the opportunities to on medical issues
Alzheimer’s Association
laws; consider Drivers Ed Toolkit enhance law and reporting processes
resources and
incremental provide clarity on
programming
increases to seat applicability
1.2d 1.5d Provide education
belt fines,
Countdown2Drive 1.4e Promote KTRSO to LE to increase
continue to 1.3c Enforce
resources & links to enforcement and
reevaluate fines Graduated
1.2e Be various programs reporting of medical
and look for Driver’s License
Responsible and https://www.ktsro.org/ issues
opportunities law
for Keep Everyone older-drivers
enhancements Safe (BRAKES) 1.5e Develop a process
(consider 1.4f Raise awareness of for screening someone
enforcing the resources among the to give up their keys and
same fine for all medical community transportation
individuals/ages) alternatives
25
To protect and improve the health and environment for all Kansans.Goal #1: Reduce crash-related injury rate per vehicle miles traveled (VMT) in the state by
5% (Continued)
Strategies (Continued)
1.6 Reduce distracted 1.7 Promote safe roadway 1.8 Enforce impaired 1.9 Raise awareness of
driving through engineering driving laws, rules, and employer strategies to increase
implementation and regulations safe driving habits among
enforcement of laws, employees
rules, and regulations
Actions
1.6a Strengthen 1.7a Develop and require 1.8a Enforce impaired 1.9a Implement an awareness
existing distracted signage, median and train driving laws, rules and campaign targeting large
driving laws crossings, and implement regulations employers to include
more roadway safety incentives for safe driving
1.6b Ensure features like rumble strips, 1.8b Address impaired habits in their wellness
enforcement of etc. driving and including programs (seatbelt checks,
distracted driving multiple substances, Bucks for Buckles, etc.)
laws 1.7b Create a data other drugs
repository for crashes,
1.6c Conduct injuries, and fatalities 1.8c Continue to
inattentive distracted increase the number
driving campaign; 1.7c Map high crash areas of DRE and ARIDE
Hands Free Bill trained LEOs
1.7d Utilize data from 1.7b
1.6d Promote and 1.7c for targeted
distracted driver education efforts
education
1.7e Ensure that enhanced
911 is available statewide
1.7f Ensure proper design
elements and to creating
safer intersections between
pedestrians, bicycles, and
vehicles
1.7g Ensure the
identification and
incorporation of safety
enhancements when road
work is in process
26
To protect and improve the health and environment for all Kansans.Goal #2: Reduce crash death rate per vehicle miles traveled (VMT) (100 million miles) in
the state by 5% by 2025
Strategies
2.1 Enhance trauma system to improve patient outcomes
Actions
2.1a Develop a community group to offer first aid and unintentional injury prevention education
2.1b Provide funding for trauma training to care providers
2.1c Promote use of Centers for Disease Control (CDC) Field Triage Guidelines
2.1d Increase collaboration between emergency medical services (EMS) and hospital providers
2.1e Develop a Level 3 or higher trauma center in each region
27
To protect and improve the health and environment for all Kansans.Falls
Introduction
Related to falls in Kansas, between 2016-2019 there were 1,727 deaths, nearly 33,600 hospitalizations
and more than 270,000 emergency department visits. Falls were the most common causes of
unintentional injury death in Kansas. Falls happen across the lifespan, however, adults 55 years old,
and older are more susceptible to life-altering injury and death related to falls. While we recognize that
children ages 1-4 also are more susceptible to falls, these are not typically as life-altering as falls among
older adults.
Objectives
1. Prevent an increase in the number of fall-related deaths by 2025
2. Prevent an increase in fall-related hospitalizations by 2025
3. Prevent an increase in fall-related emergency department visits by 2025
Goals
1. Prevent an increase in fall-related deaths among all persons
2. Prevent an increase in fall-related deaths among adults aged 65 years and older
3. Prevent an increase in the rate of hospitalizations due to falls by 2025
4. Increase collaboration among community partners to assess and address opportunities for fall
prevention by 2025
5. Further review unintentional injury prevention data to include additional analysis and review
literature to identify disparate populations
Strategies and Actions
To prevent an increase in the rate of hospital discharges due to falls, the plan focuses on increasing
participation in fall prevention programs and increasing public awareness of risk factors for falls.
Strategies and actions to accomplish these objectives include the following:
• Increase use of Kansas Self-Management Education online resource
https://selfmanageks.org/Default
• Develop and distribute public service announcements and publish articles on falls prevention
• Encourage education through physicians
• Promote falls prevention through traditional and social media
To increase collaboration among community partners to assess and address opportunities for falls
prevention, the plan recommends using a community assessment tool that includes fall risk and
developing an active state coalition with regional networks. Strategies and actions to accomplish this
objective include the following:
• Assess and improve the home environment (e.g. furniture, rugs, lighting, etc.)
28
To protect and improve the health and environment for all Kansans.• Assess and improve the built environment (e.g. sidewalks, curbs, crosswalks, etc.)
• Support a statewide coalition by providing resources, data, education, engagement and
networking
To further review unintentional injury prevention data to include additional analysis and review
literature to identify disparate populations. Strategies and actions to accomplish this objective include
the following:
• Identify additional data sets that may be available for review
• Conduct a comprehensive review of available data related to falls with special emphasis on age,
race, gender, and people with disabilities
Best Practices
Potential Resources and Partners
and Programs
• Stepping On • AARP • Public works
• Fall Less in Kansas • American Automobile Association • Regional Trauma Councils
• Tai Chi for Health (AAA) • Health Departments
• HomeFit Guide • Centers for Disease Control and • Nursing students at technical
• Screenings for fall risk Prevention (CDC) colleges
• Well child visits • Safe Kids • Canadian Resources – EMT and PT
• CPSC guidelines for • Local Fire Departments • Retired Senior Volunteer Program
safe playgrounds and • OSFM (RSVP)
other spaces • City Engineers • National Fire Protection
• Evidence-Based Falls • Community Civic organizations Association
Prevention Programs • Faith-Based Organizations • Medical Community
• Evidence-Based Self- • Insurance Providers o Primary Care Providers
assessments Guides • Managed Care Organizations o Pediatricians
o STEADI • Kansas Injury Epidemiologist o Home Health
o AARP resources • Departments of Aging o Trauma Centers
• Centers for Independent Living o EMS Paramedics
• Program support and program leaders o Physical Therapists
o E.g., Stepping On, Tai Chi for o Occupational Therapists
Health, Matter of Better Balance o Optometrists
• Community Mental Health o Pharmacists
Target Populations Protective Factors
• Adults (55+) • Medication checks reduce impact of
• Individuals with disabilities medication-related falls
• Individuals living alone or those who don’t have support in • Regular vision exams and vision correction
the home • Clutter free, well-lit homes
• Parents with children ages 0-4 • Physical activity
• Caregivers of older adults (formal and informal) • Annual examinations with fall risk assessment
• Caregivers of people with disabilities and appropriate referrals
• Individuals who have experienced one or more falls • Access to durable medical equipment
previously • Opportunities for socialization
29
To protect and improve the health and environment for all Kansans.Goal #1: Prevent an increase in the rate of hospital discharges due to falls by 2025
Strategies
1.1 Increase 1.2 Increase 1.3 Increase 1.4 Offer 1.5 Provide 1.6 Increase 1.7 Increase
participation public the number evidence- education on the number of parental
in fall awareness of of evidence- based fall home safety providers education on
prevention risk factors for based fall prevention completing fall fall risks for
programs falls prevention programs screens for young
programs adults children
provided
Actions
1.1a Increase 1.2a Develop 1.3a 1.4a Develop 1.5a Utilize 1.6a Incentivize 1.7a Connect
use of Kansas communication Encourage a listing of all AARP HomeFit providers to do with
Self- tools to raise falls evidence- as a tool for fall screens community
Management awareness of prevention based home safety mental health
Education risk factors for programs to programs education 1.6b Provide to identify
online falls register their available in NCOA Current parental
resource, courses on the Kansas 1.5b Provide Procedure resources
https://selfm 1.2b Encourage Kansas Self- education on Code to that are
anageks.org/ falls prevention Management 1.4b Provide home safety, providers to available on
Default and risk Education resources to clear paths of cover screening falls
awareness online help program travel for people costs
1.1b Support through resource, attendees with disabilities 1.7b Promote
marketing of physicians, https://selfma maintain 1.6c Encourage CPSC
falls pharmacists, nageks.org/De their 1.5c Develop home health guidelines
prevention and fault exercises home safety providers to and Safe Kids
programs optometrists checklists for complete Kansas
1.4c Provide EMS to complete assessments for educational
1.1c Identify a Fall a quick fall prevention pieces that
and Prevention evaluation of the are applicable
implement Kit as part of home 1.6d Explore for children
virtual program legislative
adaptations participation 1.5d Provide mandates for
for fall resources to fall prevention
prevention EMS to provide screenings
programs in-home
education to fall 1.6e Identify
assistance calls procedures for
providers
1.5e Offer to begin
occupational assessing for
and physical fall screenings
therapy as home at age 50
safety tools
30
To protect and improve the health and environment for all Kansans.You can also read

















































