Ketosis Leads to Increased Methylglyoxal Production on the Atkins Diet
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
Ketosis Leads to Increased Methylglyoxal
Production on the Atkins Diet
BENJAMIN G. K. BEISSWENGER, ELIZABETH M. DELUCIA, NANCY LAPOINT,
REBECCA J. SANFORD, AND PAUL J. BEISSWENGER
Sections of Endocrinology, Diabetes, and Metabolism, Department of Medicine,
Dartmouth Medical School, Hanover, New Hampshire 03756, USA
ABSTRACT: In the popular and widely used Atkins diet, the body burns fat as
its main fuel. This process produces ketosis and hence increased levels of -
hydroxybutyrate (BOB) acetoacetate (AcAc) and its by-products acetone and
acetol. These products are potential precursors of the glycotoxin methylglyox-
al. Since methylglyoxal and its byproducts are recognized as a significant cause
of blood vessel and tissue damage, we measured methylglyoxal, acetone, and
acetol in subjects on the Atkins diet. We found that by 14–28 days, methylghy-
oxal levels rose 1.67-fold (P = 0.039) and acetol and acetone levels increased 2.7-
and 6.12-fold, respectively (P = 0.012 and 0.028). Samples from subjects with
ketosis showed even greater increases in methylglyoxal (2.12-fold), as well as
acetol and acetone, which increased 4.19- and 7.9-fold, respectively; while no
changes were seen in samples from noncompliant, nonketotic subjects. The in-
crease in methylglyoxal implies that potential tissue and vascular damage can
occur on the Atkins diet and should be considered when choosing a weight-loss
program.
KEYWORDS: Atkins diet; ketosis; methylglyoxal; acetone; acetol
INTRODUCTION
The Atkins diet (AD) has become extremely popular over the last decade. The
book Dr. Atkins’ New Diet Revolution1 has sold over 10 million copies, and many
people use this low-carbohydrate diet as a tool to achieve rapid weight loss. On the
Atkins diet, people consume less than 20 grams of carbohydrates per day for the first
two weeks and less than 40 grams thereafter. Therefore the body burns fat as its main
fuel, a process that produces ketosis. With the huge number of people using the At-
kins diet, the critical question is whether or not this ketosis-producing diet is safe.
Very few studies have been done on the Atkins diet, and the two that have ap-
peared in the New England Journal of Medicine were purely descriptive. Several
studies of people who have undergone periodic weight loss, “weight cycling,” which
commonly occurs on diets such as the Atkins diet,2 have shown increased cardiovas-
cular problems, although the reason for this is unclear. Short-term weight loss has
Address for correspondence: Paul J. Beisswenger, M.D., Professor of Medicine, Dartmouth
Medical School, Dartmouth Hitchcock Medical Center, 1 Medical Center Drive, Lebanon, NH
03756.Voice: 603-650-8630/1808; fax: 603-650-2240/1808.
paul.j.beisswenger@dartmouth.edu
Ann. N.Y. Acad. Sci. 1043: 201–210 (2005). © 2005 New York Academy of Sciences.
doi: 10.1196/annals.1333.025
201202 ANNALS NEW YORK ACADEMY OF SCIENCES
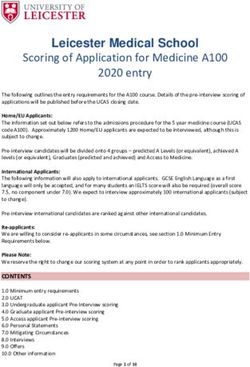
FIGURE 1. Sources of methylglyoxal in vivo. Under normal conditions. MG is formed
primarilyfrom triose phosphates. Pathways exist (lower right corner) to convert ketones to
MG.
been documented on the Atkins diet, but there is reasonable cause for concern that
the very low carbohydrate intake and the unlimited intake of saturated fat and cho-
lesterol may produce adverse effects. With such limited information about the risks
involved, it is particularly worrisome that this diet is now being recommended for
long-term use. The specific aim of this study is to evaluate the potentially toxic effect
of the Atkins diet through the increased production of the important glycation prod-
uct, methylglyoxal. Methylglyoxal (MG) is up to 40,000 times more chemically re-
active than glucose, and it has multiple cytotoxic effects. These include inhibition of
cell growth, apoptosis, mutagenic effects, inhibition of enzymatic activity, produc-
tion of protein cross-linking and fragmentation, and serving as an important precur-
sor for advanced glycation end product (AGE) formation.
There are many potential sources of methylglyoxal,6 the most common of which
is the glycolytic pathway, where the triose-phosphates, glyceraldehydes-3-phos-
phate, and dihydroxyacetone-phosphate are the primary presursors. There are also
less significant pathways where Amadori products or serine/threonine can act as MG
precursors (FIG. 1). Another pathway that could be very significant to Atkins dieters
is MG production through ketone bodies. On a low-carbohydrate diet such as the At-
kins diet, patients become ketotic, with elevated levels of aceto-acetate and β-hy-
droxybutyrate. Acetoacetate breaks down into acetone, which studies have shown
oxidizes into acetol,7,8 a possible precursor of methylglyoxal.9 We believe that this
is an important issue to address since methylglyoxal is recognized as a significant
cause of blood vessel and tissue damage.3–5BEISSWENGER et al.: KETOSIS LEADS TO INCREASED METHYLGLYOXAL 203
METHODS
Men and women between 30 and 60 years of age, who had chosen to initiate the
Atkins diet, participated in the study. The study was approved by the Dartmouth
Committee for the Protection of Human Subjects, and all participants signed a con-
sent form that described the study and the risks involved. To participate, subjects
were required to have a body mass index (BMI) > 25 and normal fasting blood glu-
cose (204 ANNALS NEW YORK ACADEMY OF SCIENCES nary AcAc and plasma BOB levels). A significant difference was considered a P val- ue of
BEISSWENGER et al.: KETOSIS LEADS TO INCREASED METHYLGLYOXAL 205
TABLE 1. Characterists of subjects on Atkins’ diet
Subject
Characteristic 1 2* 3 4 5 6* 7 8 10*
Weight loss (kg) 3.6 3.4 5.4 2.3 5.5 0 1.6 0.8 0.2
BOB (mM) .4 0 .3 .2 .7 .2 .8 .4 .1
AcAc (mg/dL) 15–40 15 15–40 15–40 40 0 40 15 0
Days to test 19 21 28 15 14 15 14 14 14
Age 50 50 50 48 50 58 50 49 51
*Nonketotic, defined as negative acetoacetate (AcAc), β-hydroxybutyrate (BOB), or both.
1.35 kg, and this subgroup showed a rise in both BOB (mean 0.5 ± 0.2 mM) and
AcAc (≥15 mg/dL).
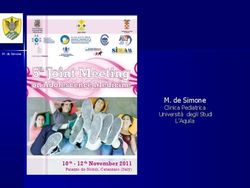
When plasma MG levels were determined for the intent-to-treat group after start-
ing the AD, they were found to be significantly elevated from the original values of
113.6 ± 38.6 to 189.3 ± 72.7 nM (P = 0.039) (FIG. 3A). In the group that was shown
to have stayed on the diet (compliant group), MG levels were found to be more than
twice as high as they were prior to dieting. (216.5 ± 73.5 nM on diet vs 97.9 ±
34.7nM baseline, P = 0.005 (FIG. 3B).
FIGURE 3. Levels of methylglyoxal on the Atkins diet. Plasma levels of methylglyox-
al in the complete study population (A) and in the 6/10 subjects who were ketotic and com-
pliant with the diet (B), prior to and after 14–28 days on the Atkins diet. Significant
increases were seen in group A, and greater increases were seen in group B, while on the
diet, with P values of 0.039 and 0.005, respectively.206 ANNALS NEW YORK ACADEMY OF SCIENCES
FIGURE 4. Change in acetone and
acetol in all subjects and those who were
most compliant with the Atkins diet.
Change in acetone (A and C) and acetol
(B and D), in all subjects and in those
who had positive ketones and were pre-
sumably compliant (n = 6) with the At-
kins diet. For each metabolite, highly
significant increases were seen while on
the diet, with P values of 0.012 and
0.0008 for A and C, and 0.0097 and
0.003 for B and D, respectively.BEISSWENGER et al.: KETOSIS LEADS TO INCREASED METHYLGLYOXAL 207 FIGURE 5. Comparison of change in methylglyoxal, acetol, and acetone in subjects who were compliant (N = 6) and noncompliant (N = 3) with the Atkins diet. The change above baseline (value on diet − baseline value) for methylglyoxal (A), acetol (B). and ace- tone (C) in subjects who had documented ketosis (compliant) relative to those who were nonketotic (noncompliant). P values for differences in acetol and acetone were significant (P = 0.03), while the difference in MG did not quite achieve significance (P = 0.09), perhaps secondary to the small N.
208 ANNALS NEW YORK ACADEMY OF SCIENCES
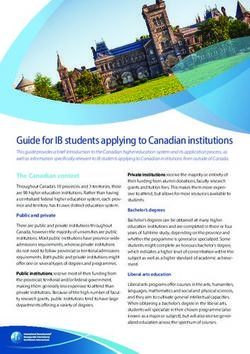
FIGURE 6. Linear regression analysis of MG and acetol levels. A highly significant re-
lationship was observed between methylglyoxal and its putative precursor, acetol (P =
0.0002, R = 0.79).
In the intent-to-treat group, acetone and acetol also rose from 218.8 ± 146.1 and
1.05 ± 0.5 to 1338.2 ± 1010 and 2.9 ± 1.8 µM, respectively (P values of 0.012 and
0.028), as shown in FIGURES 4A and 4B. Greater differences in acetone (1852.5 ±
822 on the AD and 234.15 ± 178.70 µM prediet, P = 0.0008, FIG. 4C) and acetol
(3.73 ± 1.7 on the AD compared with 0.89 ± 0.50µM prediet, P = 0.003 FIG. 4D)
were observed when only the compliant subjects were analyzed. When the increases
above baseline (value on diet, value prediet) for MG, acetol, and acetone levels were
analyzed in subjects who did not strictly follow the diet (nonketotic), minimal
changes were observed (3.7 ± 9.4, −0.11 ± 0.26, and 121.5 ± 38.2 µM, respectively)
relative to those who were compliant with the diet, where increases of 114.9 ± 99.3,
2.83 ± 1.86, and 1618.4 ± 899 were seen, respectively (FIG. 5A–5C). We then exam-
ined the relationship between MG and acetol with a linear regression analysis and
found that it was highly significant (P = 0.0002, R = 0.79) (FIG. 6). We observed a
similar highly significant relationship between acetol and acetone. (P = 0.0001, R =
0.78) (data not shown).
DISCUSSION
This study shows that the AD leads to highly significant increases in methylgly-
oxal levels in otherwise-healthy people. The increase in MG that was seen was great-
er than that seen in people with poorly controlled diabetes,9–11 where increased
vascular and neuropathic problems are a common result of this toxin. The rise in MG
appears to be related to the presence of ketosis and not necessarily to the amount of
weight loss. The highly significant relationship that was observed between acetol
and MG suggests that MG is produced directly from acetol by oxidative mecha-
nisms.6 Although ketone bodies are likely to be an important source of MG, it is also
possible that some MG is derived from increased triose phosphates resulting from
increased production of glycerol (from accelerated triglyceride breakdown) or fromBEISSWENGER et al.: KETOSIS LEADS TO INCREASED METHYLGLYOXAL 209
lipoxidation products4 (from the high fat intake) undergoing degradation to MG. The
long-term implications of the elevation of MG while on the AD are not known. How-
ever, it is possible that it could lead to tissue damage since the levels seen are at least
as high as those observed in diabetes, where vascular complications are common.
The degree of tissue damage is likely to depend on the amount of time a person is on
the diet because high MG levels lead to the creation of chemically irreversible ad-
vanced glycation end products (AGEs).12,13 The time people stay on the diet varies,
but many stay on it for several months or more, and recent recommendations by the
Atkins group suggest that the diet be used “life-long.”1 Since most people who use
the diet return to near their original weight within a year,14 the justification for ex-
posure to high levels of MG and possible accumulation of toxic AGEs should be con-
sidered when balancing the risks and benefits of very-low-carbohydrate diets.
Because of the tremendous popularity of low-carbohydrate diets, more studies of
methylglyoxal metabolism and ketosis-producing diets are needed. Important addi-
tional information would include studies to determine whether or not, or in what
time frame, methylglyoxal levels return to baseline after the diet is stopped; how
long it takes for higher levels of methylglyoxal levels in the blood to start creating
irreversible AGEs; and if other diets produce weight loss without increasing meth-
ylgloxal levels. Because of the large number of people nationwide who are on the
Atkins diet and the fact that complications resulting from high levels of methylgly-
oxal can appear after a delayed period of time, very-low-carbohydrate diets could
lead to significant health problems in the future.
ACKNOWLEDGMENTS
This study was supported by a grant from Marie Elise Young to the Hitchcock
Foundation and by a clinical research grant from the American Diabetes Association.
REFERENCES
1. ATKINS, R.C. 2002 Dr. Atkins’New Diet Revolution. Harper Collins Publisher. New
York.
2. WANNAMETHEE, S.G., A.G. SHAPER & M. WALKER. 2002. Weight change, weight fluc-
tuation, and mortality. Arch. Internal Med. 162(22): 2575–2580.
3. THORNALLEY, P., M. WESTWOOD & A. MCLELLAN. 1995. Formation of methylglyoxal-
modified proteins in vitro and in vivo and their involvement in AGE-related pro-
cesses. Contrib. Nephrol. 112: 24–31.
4. BAYNES, J.W. & S.R. THORPE. 2000. Glycoxidation and lipoxidation in atherogenesis.
Free Radical Biol. Med. 28(12): 1708–1716.
5. BEISSWENGER, P., S. HOWELL, R. NELSON, et al. 2003. Alpha oxoaldehyde metabolism
and diabetic complications. Biochem. Soc. Trans. 31(Part 6): 1358–1363.
6. THORNALLEY, P.J. 1996. Pharmacology of methylglyoxal: formation, modification of
proteins and nucleic acids, and enzymatic detoxification—a role in pathogenesis and
antiproliferative chemotherapy. Gen. Pharmacol. 27(4): 565–573.
7. OWEN, O.E., V.E. TRAPP, C.L. SKUTCHES, et al.1982. Acetone metabolism during dia-
betic ketoacidosis. Diabetes 31: 242–248.
8. REICHARD, G.A.J., C.L. SKUTCHES, R.D. HOELDTKE & O.E. OWEN. 1986. Acetone
metabolism in humans during diabetic ketoacidosis. Diabetes 35: 668–674.
9. BEISSWENGER, P., S. HOWELL, K. SMITH & B. SZWERGOLD. 2003. Glyceraldehyde-3-
phosphate dehydrogenase activity as an independent modifier of methylglyoxal lev-
els in diabetes. Biochem. Biophys. Acta 1637: 98–106.210 ANNALS NEW YORK ACADEMY OF SCIENCES
10. BEISSWENGER, P., S. HOWELL, R. O’DELL, et al. 2001. Alpha dicarbonyls increase in the
postprandial period and reflect the degree of hyperglycemia. Diab. Care 24: 726–
732.
11. BEISSWENGER, P., S. HOWELL, A. TOUCHETTE, et al. 1999. Metformin reduces systemic
methylglyoxal levels in type 2 diabetes. Diabetes 48: 198–202.
12. BROWNLEE, M. 2000. Negative consequences of glycation. Metab. Clin. Exp. 49(2
Suppl. 1): 9–13.
13. AHMED, N., S. BATTAH, N. KARACHALIAS, et al. 2003. Increased formation of methylg-
lyoxal and protein glycation, oxidation, and nitrosation in triosephosphate isomerase
deficiency. Biochim. Biophys. Acta 1639(2): 121–132.
14. FOSTER, G.D., H.R. WYATT, J.O. HILL, et al. 2003. A randomized trial of a low-carbo-
hydrate diet for obesity. N. Eng. J. Med. 348(21): 2082–2090.You can also read