Local Anesthetic Systemic Toxicity (LAST) Revisited: A Paradigm in Evolution - Anesthesia Patient Safety Foundation
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below

APSF.ORG
NEWSLETTER
THE OFFICIAL JOURNAL OF THE ANESTHESIA PATIENT SAFETY FOUNDATION
Volume 35, No. 1, 1–32 Circulation 122,210 February 2020
Local Anesthetic Systemic Toxicity (LAST)
Revisited: A Paradigm in Evolution
by Guy Weinberg, MD; Barbara Rupnik, MD; Nitish Aggarwal, MD, MBA; Michael Fettiplace, MD, PhD; and Marina Gitman, MD
INTRODUCTION INCIDENCE
Combined clinical and basic science efforts LAST can happen in any practice setting, but it
over several decades have enhanced our is often ignored or underappreciated by practi-
understanding of the underlying mechanisms tioners until experienced firsthand. Reported
and clinical spectrum of local anesthetic sys- estimates of its frequency vary greatly. Although
temic toxicity (LAST). The APSF Newsletter has some single-site studies at academic institutions
played an important role in educating clini- report extremely low rates of LAST,1 recent anal-
cians and increasing awareness of the various yses of large registry2 and administrative3,4 data-
presentations and optimal treatment of LAST, In particular, the adoption of ultrasound guid- bases generally agree on a rate of approximately
undoubtedly improving patient outcomes from ance, catheter and intravenous infusions, local 1 per 1000 peripheral nerve blocks. However,
this life-threatening iatrogenic complication. infiltration, and the expanding roles of regional given the strong likelihood of under-reporting,
The changing landscape of regional anesthe- anesthesia and local anesthetics in ERAS, multi- misdiagnosis, or other causes of failed case
sia, characterized by new uses and forms modal analgesia, and possible cancer risk mod- capture, it is possible the actual rate is higher.
of local anesthetics, has led to recent shifts in ification, require attention to the changing
the clinical features and context of LAST. features of LAST. See “LAST Revisited,” Page 5
A Patient With E-Cigarette Vaping Associated Lung Injury
(EVALI)—Coming to an Operating Room Near You!
by Todd Dodick, MD, and Steven Greenberg, MD
INTRODUCTION THE CASE
The use of e-cigarettes, commonly referred Recently, in our institution, a 30-year-old male
to as vaping, has increased exponentially in the presented to our emergency department with
past several years. E-cigarettes were initially
shortness of breath, daytime sweats, chills, and
marketed as a smoking cessation aid, but their
use among adolescents and young adults progressive shortness of breath. He reported
doubled from 2017 to 2019. In early 2019, cases “vaping all day” and admitted to vaping both tet-
of e-cigarette, or vaping, product use associated rahydrocannabinol (THC) and nicotine for the last
lung injury (EVALI) began to be presented to 5 years. After a battery of tests were negative,
hospitals across the United States. Although severe EVALI was presumed, which required
other chemicals have been implicated in EVALI, ICU admission with high FiO2 and PEEP require-
The Centers for Disease Control and Prevention
ments. The patient was started on IV methyl-
(CDC) has now suggested that vitamin E acetate,
commonly added to illicit cannabis vaping prednisolone 40 mg twice per day. During his
liquids, is the most likely cause of EVALI.1 As of ICU stay, he developed an acute left tension
December 10, 2019, a total of 2409 cases have pneumothorax while on non-invasive ventilation
been reported to the CDC.1 requiring chest tube placement and endotra-
cheal intubation. The patient was found to have In the operating room, he was appropriately
preoxygenated, but rapidly desaturated to an
AANA and Other Readers: bilateral apical blebs on chest computer tomog-
SpO2 of 51% following induction of anesthesia,
If you are not on our mailing list, please raphy scan. After being weaned from the ventila-
tor, our thoracic surgeons scheduled pleurodesis recovering to SpO2 >90% with manual ventila-
subscribe at https://www.apsf.org/subscribe
and resection of a large bleb due to a persistent tion. Oxygenation and ventilation during one-
and the APSF will send you an email of the lung ventilation were expectedly difficult.
large left pneumothorax despite persistent chest
current issue.
tube therapy. See “Vaping,” Page 4
TABLE OF CONTENTS, NEXT PAGE
APSF NEWSLETTER February 2020 PAGE 2
TABLE OF CONTENTS
ARTICLES:
Local Anesthetic Systemic Toxicity (LAST) Revisited: A Paradigm in Evolution........................................................................Cover
NEWSLETTER
A Patient With E-Cigarette Vaping Associated Lung Injury (EVALI)—Coming to an Operating Room Near You!...........Cover
The Official Journal of the
2020 President's Report: What APSF is Doing to Promote Perioperative Patient Safety and
How Each of Us Can Make a Positive Impact ....................................................................................................................................Page 3 Anesthesia Patient Safety Foundation
Healthy Relationships Between Anesthesia Professionals and Surgeons Are Vital to Patient Safety..............................Page 8 The Anesthesia Patient Safety Foundation Newsletter
Rapid Response: Airway Emergencies and Safety in Magnetic Resonance Imaging (MRI) Suite......................................Page 10 is the official publication of the nonprofit Anesthesia
APSF Awards 2020 Grant Recipients...................................................................................................................................................Page 12 Patient Safety Foundation and is published three
times per year in Wilmington, Delaware. Individuals
Rapid Response: An Incident of GlideScope® Stat Cover Failure...............................................................................................Page 14
and corporations may subscribe for $100. If multiple
Portable Point of Care Ultrasound (PPOCUS): An Emerging Technology for Improving Patient Safety...........................Page 15 copies of the APSF Newsletter are needed, please
Q&A: Navigating Perioperative Insulin Pump Use ...........................................................................................................................Page 19 contact: maxwell@apsf.org. Contributions to the
How Can We Tell How “Smart” Our Infusion Pumps Are?..............................................................................................................Page 21 Foundation are tax-deductible. ©Anesthesia Patient
Patient Blood Management Program Reduces Risks and Cost, While Improving Outcomes.............................................Page 23 Safety Foundation, 2020.
APSF-Sponsored 2019 ASA Panel on "Practical Approaches to Improving Medication Safety"........................................Page 24 The opinions expressed in this Newsletter are not
A Difficult Airway Early Warning System in Patients at Risk for Emergency Intubation: A Pilot Study...............................Page 26 necessarily those of the Anesthesia Patient Safety
PRO and CON:
Foundation. The APSF neither writes nor promul-
gates standards, and the opinions expressed herein
PRO: Artificial Intelligence (AI) in Health Care.................................................................................................................. Page 27 should not be construed to constitute practice stan-
CON: Artificial Intelligence is Not a Magic Pill.................................................................................................................. Page 28 dards or practice parameters. Validity of opinions pre-
Balancing Sustainability and Infection Control: The Case for Reusable Laryngoscopes....................................... Page 29 sented, drug dosages, accuracy, and completeness
Rapid Response: Perils and Pitfalls With the Rapid Infusion Catheter (RIC)................................................................. Page 30 of content are not guaranteed by the APSF.
APSF Executive Committee 2019:
APSF ANNOUNCEMENTS: Mark A. Warner, MD, President, Rochester, MN; Daniel
Guide for Authors.......................................................................................................................................................................................Page 2 J. Cole, MD, Vice President, Los Angeles, CA; Matthew
APSF Stoelting Conference 2020 Announcement..........................................................................................................................Page 13 B. Weinger, MD, Secretary, Nashville, TN; Douglas A.
APSF Donor Page.......................................................................................................................................................................................Page 18 Bartlett, Treasurer, Boulder, CO; Maria van Pelt, CRNA,
Crowdfunding Announcement...............................................................................................................................................................Page 31 PhD, Director At-Large, Boston, MA.
Legacy Members........................................................................................................................................................................................Page 31 APSF Newsletter Editorial Board 2019:
2019 Board Members and Committee Members:.................................................................https://www.apsf.org/about-apsf/board-committees/
Steven B. Greenberg, MD, Editor-in-Chief, Chicago, IL;
Edward A. Bittner, MD, PhD, Associate Editor, Boston,
MA; Jennifer M. Banayan, MD, Associate Editor, Chi-
cago, IL; Meghan Lane-Fall, MD, Assistant Editor, Phila-
Guide for Authors and have appropriate referencing (see http://www.apsf.org/
authorguide). The articles should be limited to 2,000 words with
delphia, PA; Trygve Armour, MD, Rochester, MN; JW
Beard, MD, Wilmette, IL; Heather Colombano, MD,
The APSF Newsletter is the official journal of the Anesthesia Patient no more than 25 references. Figures and/or tables are strongly Winston-Salem, NC; Jan Ehrenwerth, MD, New Haven,
Safety Foundation. It is widely distributed to a variety of anesthesia encouraged. CT; John H. Eichhorn, MD, San Jose, CA; Nikolaus Gra-
professionals, perioperative providers, key industry representatives, 2. Q&A articles are submitted by readers regarding anesthesia venstein, MD, Gainesville, FL; Joshua Lea, CRNA,
and risk managers. Therefore, we strongly encourage publication of patient safety questions to knowledgeable experts or desig- Boston, MA; Bommy Hong Mershon, MD, Baltimore,
those articles that emphasize and include the multidisciplinary, mul- nated consultants to provide a response. The articles should be MD; Tricia A. Meyer, PharmD, Temple, TX; Glenn S.
tiprofessional approach to patient safety. It is published three times limited to 750 words. Murphy, MD, Chicago, IL; Brian Thomas, JD, Kansas
a year (February, June, and October). Deadlines for each issue are 3. Letters to the editor are welcome and should be limited to 500 City, MO; Jeffrey S. Vender, MD, Winnetka, IL; Wilson
as follows: 1) February Issue: November 15th, 2) June Issue: words. Please include references when appropriate. Somerville, PhD, Editorial Assistant, Winston-Salem,
March 15th, 3) October Issue: July 15th. The content of the news- 4. Rapid Response (to questions from readers), formerly known as, NC. Please see the links of international editors at
letter typically focuses on anesthesia-related perioperative patient "Dear SIRS," which was the “Safety Information Response https://www.apsf.org/wp-content/uploads/newsletter/
safety. Decisions regarding content and acceptance of submissions System,” is a column that allows for expeditious communication APSF-International-Editors.pdf
for publication are the responsibility of the editors. Some submis- of technology-related safety concerns raised by our readers, with
sions may go in future issues, even if the deadline is met. At the dis- Address all general, contributor, and subscription
input and response from manufacturers and industry representa- correspondence to:
cretion of the editors, submissions may be considered for tives. Dr. Jeffrey Feldman, current chair of the Committee on
publication on our APSF website and social media pages. Technology, oversees the column and coordinates the readers’ Stacey Maxwell, Administrator
Articles submitted that are not in accordance with the following Anesthesia Patient Safety Foundation
inquiries and the response from industry.
instructions may be returned to the author prior to being reviewed Charlton 1-145
5. Invited conference reports summarize clinically relevant anesthe- Mayo Clinic
for publication.
sia patient safety topics based on the respective conference 200 1st Street SW
1. Please include a title page which includes the submission’s title,
discussion. Please limit the word count to less than 1000. Rochester, MN 55905, U.S.A.
authors' full name, affiliations, conflicts of interest statement for
Commercial products are not advertised or endorsed by the APSF maxwell@apsf.org
each author, and 3–5 keywords suitable for indexing. Please
Newsletter; however, upon exclusive consideration from the edi-
include word count on the title page (not including references). Address Newsletter editorial comments, questions,
tors, articles about certain novel and important safety-related tech-
2. Please include a summary of your submissions (3–5 sentences)
nological advances may be published. The authors should have no
letters, and suggestions to:
which can be used on the APSF website as a way to publicize Steven B. Greenberg, MD
commercial ties to, or financial interest in, the technology or com-
your work. Editor-in-Chief, APSF Newsletter
3. All submissions should be written in Microsoft Word in Times mercial product.
If accepted for publication, copyright for the accepted article is greenberg@apsf.org
New Roman font, double-spaced, size 12.
4. Please include page numbers on the manuscript. transferred to the APSF. Except for copyright, all other rights such Edward A. Bittner, MD, PhD
as for patents, procedures, or processes are retained by the author. Associate Editor, APSF Newsletter
5. References should adhere to the American Medical Association
Permission to reproduce articles, figures, tables, or content from bittner@apsf.org
citation style.
Example: Prielipp R, Birnbach D. HCA-Infections: Can the anes- the APSF Newsletter must be obtained from the APSF. Jennifer M. Banayan, MD
thesia provider be at fault? APSF Newsletter. 2018; 32: 64–65. Additional information: Associate Editor, APSF Newsletter
https://www.apsf.org/article/hca-infections-can-the-anesthesia 1. Please use metric units whenever possible. banayan@apsf.org
provider-be-at-fault/ Accessed August 13, 2019. 2. Please define all abbreviations. Meghan Lane-Fall, MD
6. References should be included as superscript numbers within 3. Please use generic drug names. Assistant Editor, APSF Newsletter
the manuscript text. 4. Please be aware of HIPAA and avoid using patient names or per- lanefall@apsf.org
7. Please include in your title page if Endnote or another software sonal identifiers. Send contributions to:
tool for references is used in your submission. 5. Plagiarism is strictly prohibited.
Individuals and/or entities interested in submitting material for Anesthesia Patient Safety Foundation
Types of articles include (1) Invited review articles, Pro/Con Debates
Charlton 1-145
and Editorials, (2) Q and As, (3) Letters to the Editor, (4) Rapid publication should contact the Editor-in-chief directly at green-
Mayo Clinic
Response, and (5) Conference reports. berg@apsf.org. Please refer to the APSF Newsletter link: http:// 200 1st St SW
1. Review articles, invited Pro/Con debates, and Editorials are www.apsf.org/authorguide that will provide detailed information Rochester, MN 55905, U.S.A.
original manuscripts. They should focus on patient safety issues regarding specific requirements for submissions. Or please donate online at www.apsf.org.
APSF NEWSLETTER February 2020 PAGE 3
2020 President's Report: What APSF is Doing to Promote Perioperative
Patient Safety and How Each of Us Can Make a Positive Impact
by Mark A. Warner, MD
There are many opportunities available to us consistently high. We also are collaborating
as a specialty as well as individually to improve with the Patient Safety Movement Foundation
the safety of our patients as they go through to develop an anesthesia-specific patient safety
their perioperative episodes of care. As a spe- curriculum for training programs and for indi-
cialty, and for APSF, specifically, we must priori- vidual practitioners, with adaptations that will
tize high-value issues that need to be make it applicable for use in both high- and
addressed. As individuals, we must focus limited-resource countries. Thanks to the
acutely on the safety of each and every one of efforts of our newsletter and social media lead-
our patients…every day. ers, Steven B. Greenberg, MD, and Marjorie P.
Stiegler, MD, respectively, APSF’s patient safety
APSF’S PATIENT SAFETY PRIORITIES recommendations and articles now reach more
AND PARTNERSHIPS than 600,000 anesthesia professionals world-
There are specific issues that we all know wide, in every country and on every continent
need to be addressed. Table 1 provides a list of of the globe, with information on important
the top perioperative patient safety issues that topics in perioperative patient safety.
the APSF believes need targeted attention, dis-
cussion, and support at this time, no matter WHAT EACH OF US CAN DO TO
where you live and work. We use this set of HAVE A POSITIVE IMPACT ON
global priority issues to help us determine the PATIENT SAFETY
topics of our Stoelting Conferences, solicit arti- Dr. Mark Warner, APSF President Beyond the efforts of APSF and many of our
cles for our APSF Newsletter, drive social specialty’s professional organizations to
media content, and allocate resources for addressed through global as well as regional or improve perioperative patient safety, there are
research and education projects. local partnerships. The APSF is partnering with actions we all can take to improve patient
Beyond these global topics on perioperative the World Federation of Societies of Anaesthe- safety—individually and every day. For exam-
patient safety, there are local issues that impact siologists (WFSA) and other global and regional ple, we can simply follow the Golden Rule,
patient safety. Examples include limitations on organizations to assist with improving educa- “Treat others as you would like to be treated.”
personnel, equipment, and medications. While tion opportunities for anesthesia professionals. This rule is not tied to any culture and appears
present to some degree everywhere, these Specific to the WFSA, we are supporting efforts in some modification in all of the world’s major
limitations are most prevalent in lower resource to ensure that the value of subspecialty fellow- religions and regions.
countries. These issues often must be ships offered by the WFSA around the world is
Basically, we need to take a few deep
breaths before patients come under our care
and consider how we would wish to be treated
Table 1: APSF’s 2020 Top Ten Perioperative Patient Safety Priorities if we were in their places. Over the years I’ve
had the good fortune to be able to study sev-
1. Preventing, detecting, and mitigating clinical deterioration in the perioperative period eral major perioperative morbidities in detail
a. Early warning systems in all perioperative patients (e.g., pulmonary aspiration, ulnar neuropathy,
b. Monitoring for patient deterioration and pneumonias). I’ve also had the misfortune
i. Postoperative continuous monitoring on the hospital floor to have cared for patients who have suffered
ii. Opioid-induced ventilatory impairment and monitoring from these and other significant perioperative
iii. Early sepsis complications. Like many of you, I’ve seen
c. Early recognition and response to decompensating patient patients receive medications in error, some-
2. Safety in out-of-operating room locations such as endoscopy and interventional radiology times with significant detrimental events asso-
suites ciated with them. I can tell you from personal
experience that an unanticipated perioperative
3. Culture of safety: the importance of teamwork and promoting collegial personnel interac- infection is not the outcome you wish to have.
tions to support patient safety While many of these morbidities have complex,
4. Medication safety confounding etiologies that involve patient
a. Drug effects characteristics and patient care that spans the
b. Labeling issues perioperative continuum, we can and must do
c. Shortages better at reducing our personal errors or omis-
d. Technology issues (e.g., barcoding, RFID) sions that can negatively impact the safety of
e. Processes for avoiding and detecting errors our patients. It is the right thing to do for our
5. Perioperative delirium, cognitive dysfunction, and brain health patients. It is what we would want from our col-
6. Hospital-acquired infections and environmental microbial contamination and transmission leagues when we are the patients.
7. Patient-related communication issues, handoffs, and transitions of care Before providing care for individual patients,
we might ask ourselves:
8. Airway management difficulties, skills, and equipment • Have we used checklists to ensure that we
9. Anesthesia professionals and burnout have everything we need at hand when we
10. Distractions in procedural areas proceed with anesthetic care?
See “President's Report,” Next Page
APSF NEWSLETTER February 2020 PAGE 4
Follow the Golden Rule: "Treat Others As You Would Like To Be Treated"
From “President's Report,” Preceding Page For all of our patients, we might ask: to assist clinician investigators and others to
• Have we actively avoided contamination of • Have we participated in our local institutions develop new knowledge that can improve
our equipment and medications to reduce to develop the clinical pathways, practices, patient safety. These organizations can help
the risk of microorganism transmission peri- and policies that increase their safety develop recommendations that can be used to
operatively? throughout the perioperative period? guide care and potentially improve patient
• Have we made the effort to know our safety. Our industry partners can develop the
• Have we worked within our institutions and
patients and their risk factors for potential new equipment and medications that contrib-
with our colleagues to improve team interac-
intraoperative or postoperative complica- ute to safer care. However, each of us has a
tions and implement the cultural changes
tions? that allow all members of the perioperative personal responsibility to contribute to
• Have we allowed production pressures or team to point out actions that might cause improved perioperative patient safety. Deliber-
distractions (e.g., cell phones) to interfere patient harm? ate consideration of the Golden Rule before
with our focused efforts to provide the best providing care to each patient seems essential.
• Have we taken leadership roles, locally or
care we can? beyond, that allow us to make a positive Dr. Mark Warner is currently president of the
• Have we provided the appropriate handoff impact on the perioperative safety of the APSF and the Annenberg Professor of Anesthe-
communication before leaving the patients in populations we serve? siology, Mayo Clinic, Rochester, MN.
another anesthesia professional’s care? Perioperative patient safety is not something
• Are we “treating our patients as we would that someone else can resolve. The APSF and Dr. Warner has no disclosures with regards to
like to personally be treated”? other organizations can provide the resources the content of the article.
Perioperative Management of EVALI Patients is Challenging
From “Vaping,” Cover Page Table 1: Suggested Diagnostic Criteria for EVALI3,4
Physiologic derangements included a PaCO2
of 78 mmHg with an ETCO2 of 47 mmHg, indi- Use of e-cigarettes
cating significant dead space, and a PaO2 of
Pulmonary infiltrate on chest radiograph or ground glass opacities on computerized
69 mmHg on an FiO2 of 1.0 indicating a signifi- tomography (CT) scan
cant A-a gradient. The PEEP was 8 cm H20 and
plateau pressure was 32 mmHg. The proce- Elevated WBC count and inflammatory markers (c-reactive protein, erythrocyte sedimentation
dure was successful and he was returned to the rate)
ICU. Several days later, while he was no longer
Absence of pulmonary infection—negative for respiratory viruses including influenza,
requiring positive pressure ventilation, he negative HIV or HIV-related infections, negative blood, sputum and/or bronchial alveolar
developed another tension pneumothorax in lavage (BAL) cultures
the contralateral lung. He again underwent
pleurodesis and bleb resection. Foamy macrophages containing vitamin E acetate on BAL/lung pathology4
DISCUSSION No evidence of alternative medical causes (e.g., heart failure, rheumatologic disease, cancer)
To our knowledge, no case reports describe
the intraoperative management of a patient corticosteroids may be beneficial, and have the Department of Anesthesia and Critical Care
with EVALI, with only one other EVALI-associ- been widely administered in published reports.4 at the University of Chicago Pritzker School of
ated pneumothorax noted previously.2,3 Intra- Thus far, the CDC has documented 52 deaths Medicine, Chicago, IL.
operative ventilation of these patients may be across the United States.1 While much remains
challenging, and high levels of FiO2 and PEEP to be elucidated regarding EVALI, e-cigarette Dr. Greenberg is editor-in-chief of the APSF
may be required to maintain adequate gas use is increasingly prevalent. We are likely to Newsletter.
exchange. If significant difficulty is expected, see more cases in our hospitals and increas-
venovenous extracorporeal membrane oxy- ingly, our operating rooms in the future. REFERENCES
genation may be warranted in capable centers.
Dr. Dodick is an anesthesiologist in the Depart- 1. CDC. Outbreak of lung injury associated with the use of
Patients with EVALI present almost univer- ment of Anesthesiology, Critical Care and Pain e-cigarette, or vaping, products. https://www.cdc.gov/
sally with constitutional, respiratory, and gastro- tobacco/basic_information/e-cigarettes/severe-lung-dis-
Medicine at NorthShore University HealthSys- ease.html Accessed November 13, 2019.
intestinal symptoms. Common presenting tem, Evanston, IL, and is clinical instructor in the 2. Lewis N, McCaffrey K, Sage K, et al. E-cigarette use, or
symptoms and findings are detailed in Table 1. Department of Anesthesia and Critical Care at vaping, practices and characteristics among persons with
Severity can range from mild, not requiring hos- the University of Chicago Pritzker School of associated lung injury—Utah, April–October 2019. MMWR.
pitalization (5–10%) to severe, requiring ICU Medicine, Chicago, IL. 2019;68:953–6.
admission (44–58%) and, often, non-invasive 3. Layden JE, Ghinai I, Pray I, et al. Pulmonary illness related to
ventilation (32–36%) or intubation with mechan- Dr. Dodick has no conflicts of interest. e-cigarette use in Illinois and Wisconsin—preliminary report.
ical ventilation (11–32%).2-4 Management of N Engl J Med. DOI: 10.1056/NEJMoa1911614.
these patients is largely supportive, with lung Dr. Greenberg is vice chair of Education in the 4. Blagev DP, Harris D, Dunn A, et al. Clinical presentation,
treatment and short-term outcomes of lung injury associ-
protective ventilation with low tidal volumes and Department of Anesthesiology, Critical Care and ated with e-cigarettes or vaping: a prospective observa-
high PEEP employed similar to those used in Pain Medicine at NorthShore University Health- tional cohort study. Lancet. DOI: 10.1056/S0140-6736
Acute Respiratory Distress Syndrome. Empirical System, Evanston, IL, and is clinical professor in (19)32730–8.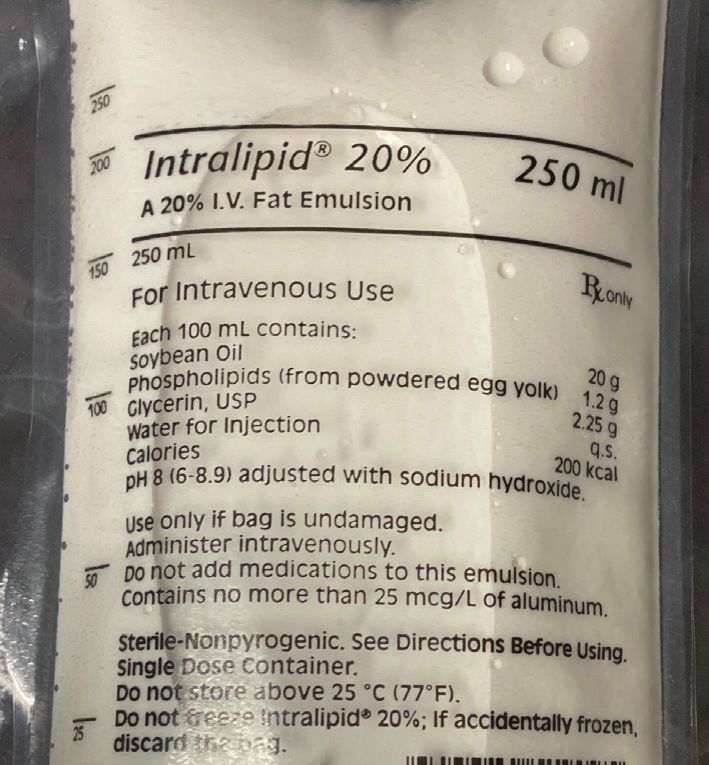
APSF NEWSLETTER February 2020 PAGE 5
Risk Factors For LAST
From “LAST Revisited,” Cover Page
Table 1: Management of LAST
Notably, Morwald et al. identified an overall rate
for signs and symptoms consistent with LAST of CLINICAL FEATURES OF LOCAL ANESTHETIC TOXICITY
1.8/1000 peripheral nerve blocks during joint
replacement; however, for the use of lipid emul- Risk Factors Prevention
sion, considered a surrogate for LAST, in the • Hypoxia or acidosis • Use of lowest effective dose
same population, they identified, for 2014, a rate • Extremes of age • Use of vascular marker (e.g., epi)
during knee replacement of 2.6/1000 or 1 in 384
• Small patient size or muscle mass • Adequate monitoring
surgeries with a block.3 For a "rare event," that's
not so rare! This reminds us of the need to • Frailty • Incremental injection
remain vigilant for the possibility of LAST in virtu- • Heart disease: • Intermittent aspiration
ally any patient receiving local anesthetic. – Coronary artery disease, low cardiac out-
• Individualized dosing
put, arrhythmias, bundle branch blocks
RISK • System safety (e.g., preparedness)
• Mitochondrial dysfunction
Understanding factors that increase risk is • Educating doctors and nurses
vital, as identifying patients with an elevated sus- • Liver or kidney disease
ceptibility to LAST enables clinicians to modify • Carnitine deficiency • Assessing patient risk factors
treatment and reduce the risk. Hypoxia and aci-
dosis were recognized decades ago as factors Presenting Symptoms and Signs
predisposing to LAST.5 More recently identified
co-morbidities include pre-existing heart disease Prodrome Major CNS Major CV
(especially ischemia, arrhythmias, conduction • Tinnitus • Agitation/confusion • Bradycardia/heart block
abnormalities, and low ejection fraction),
extremes of age, frailty, and conditions that • Metallic taste • Obtundation • Hypotension
cause mitochondrial dysfunction (e.g., carnitine • Hypertension • Seizure • Ventricular tachycardia
deficiency); liver or kidney disease can also or fibrillation
• Tachycardia • Coma
increase the risk of delayed LAST by depressing • Asystole
local anesthetic metabolism or disposition.5
Interestingly, Barrington and Kruger2 examined a Treatment of Local Anesthetic Systemic Toxicity
registry of ~25,000 peripheral nerve blocks per- 1. Stop administering local anesthetic/call for help
formed in Australia from January 2007 to May
2. Manage airway
2012 and identified 22 cases of LAST (overall
incidence, 0.87 per 1000). They found that ultra- 3. Control seizures with benzodiazepine
sound guidance lowered the risk of LAST (odds 4. CPR as needed
ratio, 0.23, CI: 0.088–0.59, p=0.002)—presum- 5. 20% lipid emulsion 1.5 mL/kg (bolus given over 2–3 min)
ably a result of fewer unidentified intravascular
injections and possibly lower volumes of the Initial resuscitation of LAST differs from standard CPR by focusing on reversing underlying
drug used to achieve a block. Nevertheless, no toxicity rather than or in addition to sustaining coronary perfusion. Hence, initial emphasis is on
single method can completely eliminate these seizure suppression and establishing normal arterial oxygen saturation since both acidosis and
events and roughly 16% of reported LAST hypoxia aggravate LAST. For severe LAST, contact a perfusion team early to assure a path to
occurred despite the use of ultrasound. Bar- extracorporeal support should CPR fail. During CPR, avoid local anesthetic anti-arrhythmics (they
rington and Kruger also noted that small patient worsen LAST), beta blockers and calcium channel blockers (they depress contractility), and vaso-
size was a risk factor for LAST. The role of skele- pressin (increasing afterload alone is undesirable since the poisoned heart doesn’t contract well).
tal muscle as a large reservoir compartment for Epinephrine is acceptable for treating hypotension but should be used in small doses since it can
local anesthetic may explain this phenomenon impair lipid resuscitation, e.g., boluses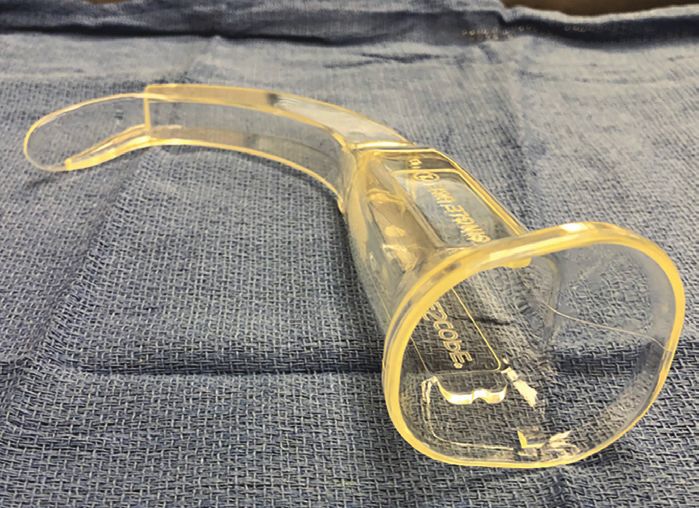
APSF NEWSLETTER February 2020 PAGE 6
LAST Can Have Delay in Onset
From “LAST Revisited,” Preceding Page Administration of non-bupivacaine local
Roughly 80% of LAST cases over the past anesthetics within 20 minutes of Exparel, which
decade occurred in hospitals, ~10% in offices, can occur when a surgeon and an anesthesia
and the remainder in emergency rooms or professional fail to communicate, may cause a
even at home. Anesthesia professionals or sudden release of liposomal bupivacaine, dan-
trainees were involved in about 60% of cases, gerously increasing free plasma bupivacaine
with surgeons involved in approximately 30%, concentrations; the exact mechanism of this
and the remainder spread among dentists, phenomenon is not elucidated. Toxicity of the
emergency physicians, pediatricians, cardiolo- two local anesthetics is then additive. Burbridge
gists, and dermatologists. This reminds us of and Jaffe13 emphasize the importance of safety
the need to take every opportunity to educate measures such as educating the operating
our colleagues about the risks and manage- room staff as well as a “time-out” label on the
ment of LAST. drug vial to prompt discussion around avoiding
simultaneous administration of other local anes-
TIMING thetics within 20 minutes of Exparel injection.
The three large-scale studies show a trend to The FDA Adverse Event Reporting System
progressive delay in the onset of LAST over the (FAERS) database contains reports submitted
past 40 years, reflecting the advent of both increase in LAST secondary to absorption or by practitioners and consumers. An analysis of
ultrasound guidance and catheter-based tech- gradual onset during infusion. The most FAERS data received between January 1, 2012,
niques. Competent use of ultrasound can common presenting features of CV toxicity and March 31, 2019, where Exparel was listed
reduce the chance of intravascular injection and were arrhythmias (including bradycardia, as the suspect medicinal product and signs or
immediate-onset LAST. Delays of more than 10 tachycardia, VT/VF), conduction disturbances symptoms of LAST occurred (seizure or both
minutes in single-shot blocks occurred in only CNS symptoms and CV disturbance), were
(bundle branch block, AV conduction block,
studied by disproportionality analysis—a phar-
~12% of cases before 2009 but in ~40% of widened QRS), hypotension, and cardiac arrest
those published in the last decade. Recent macovigilance tool that measures the “Informa-
(including nonshockable rhythms, PEA, and
reports describe LAST with an onset that is tem- tion Component” (IC025) and is used by the
asystole). Progressive toxicity (especially hypo- World Health Organization.14 This compares the
porally removed from the start of treatment by tension and bradycardia) with rapid deteriora- rate at which a particular event of interest co-
several hours or even days for catheter or intra- tion over minutes is typical of severe LAST. It is occurs with a given drug versus the rate this
venous infusion. This presumably occurs as the impossible to predict which patients will prog- event occurs without the drug in the event data-
result of drug accumulation in target tissues and ress. However, early treatment can delay or pre- base. If the lower limit of the 95% confidence
is a particular concern since both the timing and vent progression; therefore, it is important to be interval of the IC025 is greater than zero, then
setting are problematic. The long interval can prepared to intervene early in any patient there is a statistically significant signal. Such an
obscure the connection to local anesthetic receiving local anesthetic who has signs or adverse event signal was found between LAST
administration; moreover, when LAST occurs symptoms consistent with LAST. and liposomal bupivacaine. From January 1,
“off-site,” away from the operating rooms, 2012, to March 31, 2019, the analysis yielded an
where it is rarely seen, the responsible caregiv- LIPOSOMAL FORMULATION overall IC025 of 1.65. Splitting the dataset into
ers are probably less mindful or knowledgeable Liposomal bupivacaine (LB) harbors local two time periods (January 2012 to December
of the problem, its detection, and treatment. anesthetic in a nanoparticle carrier matrix 2015 and January 2016 to March 2019) showed
designed to prolong its action by slow release. persistence of a significant signal in both time
PRESENTATION Exparel® (Pacira Pharmaceuticals, San Diego, periods. While this does not prove a causal rela-
LAST provokes a variable array of signs and CA) comes in a 20-mL vial containing a total of tionship, it nevertheless points to a statistically
symptoms of central nervous system (CNS) and 266 mg (1.3%) bupivacaine, which is the manu- significant signal between Exparel and signs or
cardiovascular (CV) toxicity (Table 1). These can facturer’s maximum recommended dose for an symptoms of LAST.
be mild or severe and can occur separately or adult patient. It was approved by the Food and
together. Isolated CNS symptoms occur in Drug Administration (FDA) in 2011 for injection REPORTING OF LAST IS PROBLEMATIC
approximately half of reported cases, combined directly into the operative site to augment post- A recent Cochrane Library update of periop-
CNS and CV symptoms in about one-third and operative analgesia and later in 2018 for inter- erative intravenous lidocaine infusion by Weibel
isolated CV symptoms in the remainder. Many scalene brachial plexus block.12 Three percent et al.15 found that of 68 clinical trials comparing
of the latter occurred under general anesthesia of the drug is free and presumably initiates a lidocaine infusion with thoracic epidural analge-
or heavy sedation where CNS toxicity is difficult certain level of analgesia upon administration. sia, 18 did not comment on adverse events at all.
to ascertain. Seizure was the most common ini- Blood levels of bupivacaine can last up to 96 Unfortunately, the degree of heterogeneity in the
tial sign overall, occurring in roughly 50% of hours after injection of LB; therefore, patients reporting methods of the remaining 50 studies
cases. Minor CNS features or “prodromes” must be adequately monitored for delayed tox- precluded a meta-analysis of these data. There is
such as tinnitus, metallic taste, hallucinations, icity. As with any local anesthetic, patients with clearly a need to improve and standardize ascer-
slurred speech, limb twitching, extremity pares- specific co-morbidities are at an increased risk tainment and reporting of LAST in clinical trials
thesia, intention tremor, facial sensorimotor, and for developing acute or delayed toxicity, either involving local anesthetics. This applies particu-
eye movement abnormalities were noted in as a result of increased sensitivity (e.g., isch- larly to studies of catheter and intravenous infu-
only about 16% of patients by DiGregorio et al., emic heart disease) or impaired metabolism sions where systems for identifying LAST are not
but about 30% in combined data from Vasques (e.g., liver disease) with resulting increased as robust as in the operating room. Until this
et al. and Gitman et al.; this is consistent with an plasma levels of bupivacaine. See “LAST Revisited,” Next Page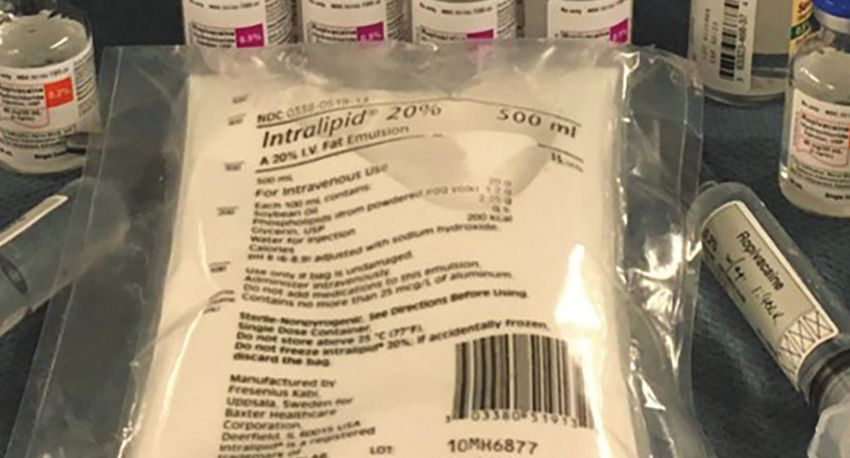
APSF NEWSLETTER February 2020 PAGE 7
Treating LAST Involves Administering Large Quantities
of Lipid Emulsion Quickly
From “LAST Revisited,” Preceding Page perfusion team at the outset of a severe event so REFERENCES
occurs, understanding the associated risks will that alternative, extracorporeal methods of circu- 1. Liu SS, Ortolan S, Sandoval MV, et al. Cardiac arrest and
remain hampered by reliance on anecdotal latory support can be readied should initial seizures caused by local anesthetic systemic toxicity after
resuscitation fail. peripheral nerve blocks: should we still fear the reaper?
reports and personal experience. Reg Anesth Pain Med. 2016;41:5–21.
CONCLUSIONS 2. Barrington MJ, Kluger R. Ultrasound guidance reduces the
TREATMENT risk of local anesthetic systemic toxicity following peripheral
In 2010 the Association of Anaesthetists of LAST can occur anytime local anesthetics are nerve blockade. Reg Anesth Pain Med. 2013;38:289–97.
Great Britain and Ireland (AAGBI) and the Amer- used. Even with appropriate dosing and perfect
3. Morwald EE, Zubizarreta N, Cozowicz C, et al. Incidence of
ican Society of Regional and Pain Medicine technique, patient susceptibility, system prob- local anesthetic systemic toxicity in orthopedic patients
(ASRA) Working Group on Local Anesthetic Tox- lems, and random errors prevent its eradication. receiving peripheral nerve blocks. Reg Anesth Pain Med.
icity separately published first-ever recommen- The increasing use of regional anesthesia in an 2017;42:442–445.
dations for a systematic approach to treating agng population, and the advent of catheter 4. Rubin DS, Matsumoto MM, Weinberg G, et al. Local anes-
and intravenous infusion of local anesthetic for thetic systemic toxicity in total joint arthroplasty: incidence
LAST.16 Both groups focused on airway man- and risk factors in the United States from the national inpa-
agement and seizure suppression along with opiate-sparing anesthesia, multimodal analge- tient sample 1998–2013. Reg Anesth Pain Med. 2018;
the rapid infusion of lipid emulsion as key ele- sia, or cancer risk modification assure that LAST 43:131–137.
ments specific to treating LAST (Table 1). will continue to occur increasingly at unex- 5. Neal JM, Barrington MJ, Fettiplace MR, et al. The third
American Society of Regional Anesthesia and Pain Medi-
Interestingly, the rate of published reports pected sites and with delayed timing despite
cine practice advisory on local anesthetic systemic toxicity:
increased from ~3 LAST cases per year before our best efforts. Identifying “at-risk” patients executive summary 2017. Reg Anesth Pain Med.
and improving system safety will reduce the 2018;43:113–123.
2009 to ~16/year in the last decade. If reporting
likelihood of LAST. 6. Fettiplace MR, Lis K, Ripper R, et al. Multi-modal contribu-
bias is constant, this could reflect greater will- tions to detoxification of acute pharmacotoxicity by a triglyc-
ingness to report events as patient outcomes Clinicians should have a treatment plan eride micro-emulsion. J Control Release. 2015;198:62–70.
improved over the past decade. ASRA has ready for LAST wherever local anesthetics are 7. Di Gregorio G, Neal JM, Rosenquist RW, et al. Clinical pre-
used. Any unusual CNS signs or CV instability in sentation of local anesthetic systemic toxicity: a review of
updated their advisory twice since 2010 with published cases, 1979 to 2009. Reg Anesth Pain Med.
modifications that include the adoption of a the setting of regional anesthesia, anesthetic 2010;35:181–187.
checklist approach and a simpler method for infiltration, or infusion should be considered 8. Vasques F, Behr AU, Weinberg G, et al. A review of local
infusing lipid emulsion. 5 Two key points possible LAST until proven otherwise, since anesthetic systemic toxicity cases since publication of the
American Society of Regional Anesthesia recommenda-
deserve mention. First, mechanism informs early intervention can prevent or slow progres-
tions: to whom it may concern. Reg Anesth Pain Med.
method. Infusing lipid emulsion reverses LAST sion. Anesthesia professionals must actively 2015;40: 698–705.
by accelerating the redistribution of local anes- educate other health care providers who 9. Gitman M, Barrington MJ. Local anesthetic systemic toxicity:
thetic.6 This results from partitioning and a direct administer local anesthetics to patients. This a review of recent case reports and registries. Reg Anesth
Pain Med. 2018;43:124–130.
inotropic effect exerted by lipid emulsion17 that includes informing those in other specialties
10. Yu RN, Houck CS, Casta A, et al. Institutional policy changes
combine to “shuttle” drug away from sensitive having a syringe in hand and staff on the floor to prevent cardiac toxicity associated with bupivacaine
organs (brain, heart) to reservoir organs (skeletal responsible for care of patients receiving local penile blockade in infants. A A Case Rep. 2016;7:71–75.
muscle, liver). This requires infusing a relatively anesthetic infusion. Improved models of LAST 11. Weber F, Guha R, Weinberg G, et al. Prolonged pulseless
and its treatment will continue to inform mea- electrical activity cardiac arrest after intranasal injection of
large quantity of lipid quickly (e.g., ~1.5 mL/kg lidocaine with epinephrine: a case report. A A Pract. 2019;
over ~2 minutes) to establish a lipid “bulk phase” sures we can adopt to improve patient safety 12:438–440.
in the plasma. The bolus infusion may be and save lives. 12. Balocco AL, Van Zundert PGE, Gan SS, et al. Extended
repeated or followed by an infusion at a slower release bupivacaine formulations for postoperative analge-
Dr. Weinberg is a professor of Anesthesiology at sia: an update. Curr Opin Anaesthesiol. 2018;31:636–642.
rate—the difference in method is likely not as the University of Illinois College of Medicine at 13. Burbridge M, Jaffe RA. Exparel®: a new local anesthetic with
important as the need to sustain a bulk phase. Chicago and staff physician at the Jesse Brown special safety concerns. Anesth Analg. 2015;121:1113–1114.
An important study by Liu et al.18 showed in a rat VA Medical Center, Chicago, IL. 14. Aggarwal N. Local anesthetics systemic toxicity association
model of bupivacaine toxicity that repeated with Exparel® (bupivacaine liposome)—a pharmacovigi-
Dr. Rupnik is a consultant anesthetist at the Bal- lance evaluation. Expert Opin Drug Saf. 2018;17:581–587.
bolus dosing is superior to bolus + infusion in
grist University Hospital, Zurich, Switzerland. 15. Weibel S, Jelting Y, Pace NL, et al. Continuous intravenous
reversing LAST. However one chooses to deliver perioperative lidocaine infusion for postoperative pain and
lipid, it is important to respect the upper dosing Dr. Aggarwal is a hospital resident at Yale New recovery in adults. Cochrane Database Syst Rev. 2018;6:
limit of ~10–12 mL/kg ideal body weight to avoid Haven hospital, New Haven, Connecticut.. CD009642.
fat overload. That is, don’t forget to turn it off! 16. Weinberg GL. Treatment of local anesthetic systemic toxic-
Dr. Fettiplace is a resident in Anesthesiology at ity (LAST). Reg Anesth Pain Med. 2010;35:188–93.
Second, the treatment strategy for CV instability Massachusetts General Hospital, Boston, MA. 17. Fettiplace MR, Ripper R, Lis K, et al. Rapid cardiotonic
in LAST differs from that used for ischemic car- effects of lipid emulsion infusion.* Crit Care Med. 2013;41:
diac arrest since the underlying pathophysiology Dr. Gitman is an assistant professor of Anesthe- e156–162.
of ischemia and pharmaco-toxicity differ. There- siology at the University of Illinois College of 18. Liu L, Jin Z, Cai X, et al. Comparative regimens of lipid
fore, it is preferable to treat the underlying toxicity Medicine, Chicago, IL. rescue from bupivacaine-induced asystole in a rat model.
Anesth Analg. 2019;128:256–263.
by infusing lipid and, if needed, use reduced
Dr. Weinberg is an officer and shareholder of 19. Weinberg GL, Di Gregorio G, Ripper R, et al. Resuscitation
doses of epinephrine (boluses ~1 mcg/kg) to sup- with lipid versus epinephrine in a rat model of bupivacaine
ResQ Pharma, Inc., and maintains the educa-
port blood pressure.19 Vasopressin should be overdose. Anesthesiology. 2008;108: 907–913.
tional website, www.lipidrescue.org. Drs. 20. Di Gregorio G, Schwartz D, Ripper R, et al. Lipid emulsion is
avoided since increasing afterload alone has no
Rupnik, Aggarwal, Fettiplace, and Gitman have superior to vasopressin in a rodent model of resuscitation
benefit and a deleterious effect has been con- from toxin-induced cardiac arrest. Crit Care Med. 2009;37:
no conflicts of interest.
firmed in animal models.20 It is sensible to alert a 993–999.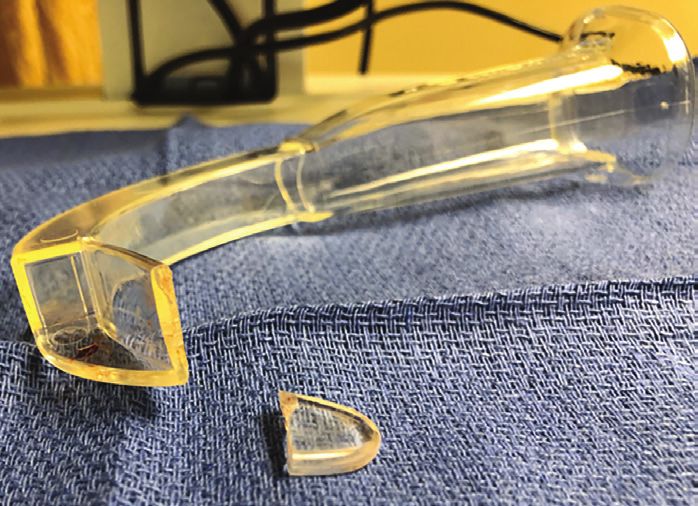
APSF NEWSLETTER February 2020 PAGE 8
Healthy Relationships Between Anesthesia Professionals and
Surgeons Are Vital to Patient Safety
by Jeffrey B. Cooper, PhD
Effective teamwork in perioperative teams is a
prerequisite for patient safety. Yet, what is rarely
discussed openly is the special importance of
dyads in teams—the relationship between two
individuals. If you’re an anesthesia professional,
you likely are aware, at least subliminally, of the
erosion of patient safety when you are working
with a surgical colleague with whom your rela-
tionship is not a pleasant one. At the least, it can
make for an unpleasant workday experience; at
worst, a dysfunctional relationship can be a criti-
cal element that enables or causes an adverse
outcome. On the flip side, when one is working
with a trusted, respected colleague and the feel-
ing is mutual, you are much more likely to have a
happy day and your patient is more likely to have
an optimal outcome.1* I addressed this topic in a
commentary published simultaneously in Anes- have been prevented by a positive relationship. Considering how important it is that surgeons
thesiology and The Journal of the American Col- More importantly, I’d heard one too many disre- and anesthesiologists work collaboratively, it is
lege of Surgeons (an unusual occurrence) and spectful remarks that represented stereotypes surprising that there is little research about this
more recently, in my presentation for the annual that anesthesia professionals have about sur- topic, almost none specifically about the anes-
Ellison C. Pierce, Jr., MD, Lecture hosted by the geons. I don’t have as much opportunity to hear thesiologist-surgeon dyad. Lorelei Lingard and
APSF and the ASA.2,3 I summarize here key similar comments from surgeons, but when I’ve colleagues have, in several studies, examined
observations and suggestions for action. probed, I have found similar stereotypes there situations where the discourse within the peri-
as well. While the stereotypes and disrespectful operative team revolves around conflict.4 One
In the presentation and the article, I focus on
remarks are not in themselves potentially harm-
the dyad between the physicians in the team, comment arising from those studies is that
ful to patients, the attitudes they represent can
anesthesiologists and surgeons. I do note that “Subjects’ constructions of other professions’
lead to communication failures and lack of col-
the other dyads are also of high importance to roles, values, and motivations were often dis-
laboration and collegiality that can either cause,
patient safety, i.e., that between surgeon and sonant with those professions’ constructions of
enable, or fail to prevent an adverse event.
OR nurse and between surgeon and any anes- themselves.” Related to that comment is the
thesia professional. Yet, my gut tells me that Some of the specific negative stereotypes observation that “Team members use assump-
there are aspects of the physician dyad that are listed in Table 1. These come from years of tions about speaker motivation to interpret
create the potential for particularly problematic listening as well as my seeking input from sur-
communicative exchanges.”
dysfunction; that is my current focus (maybe I’ll geon and anesthesiologist colleagues, near
get to the others soon). Why did I choose to and far, with both private practice and academic Jonathan Katz has specifically addressed
focus attention on this topic? Over the years (47 experiences. Again, I have no data on which to conflict in the OR.5 He notes that “cancellation…
plus since I began working in health care), in provide concrete evidence, but no one I’ve pre- for additional evaluation… is among the most
various quarters, I’d heard one too many anec- sented this to has challenged any of the com- frequent causes of conflict between surgeon
dotes about adverse events that were either ments nor pushed back on my assertion that and anesthesiologist.” He also notes that
caused by relationship dysfunction or could this is too prevalent and not healthy. sources of conflict present an opportunity for
*If you want to organize a focus group or presentation, I can send you a link to the animations I used during the collaboration. A goal should be to turn all such
lecture, including a shortened version of “There is a Fracture.” (You can find the original on Youtube.) The other two opportunities into productive collaboration in
animations are of the view surgeons have of anesthesiologists and of what a healthy collaboration would look like.”
(No charge. You just have to promise to use them for good.) the interest of the patient, seeking to learn what
is right, not who is right.
Table 1: Negative stereotyping
Diana McLain Smith writes about how func-
Examples of anesthesia professionals’ Examples of surgeons’ stereotypes tional and dysfunctional dyads in leadership
stereotypes of surgeons: of anesthesia professionals: teams are critical to either success or failure in
• They never admit how much blood they’ve • They just want to go home early—don’t care organizations.6 The characteristics and out-
lost. about my patient. comes she describes are clearly applicable to
• They just want to make a lot of money doing • They are ready to cancel a case at the drop perioperative care and to the leadership team
more cases. of a hat. in the OR. What is different about this construct
• They don’t know anything about medical • They’re often distracted, not paying attention. from the usual discussion about teams is that
issues. the focus is on relationships between two indi-
• They never tell us about the pressors they’re
• They always underestimate how long the using. viduals rather than on the team as a whole.
case will be. See “Healthy Relationships,” Next Page
APSF NEWSLETTER February 2020 PAGE 9
Building Healthy Perioperative Relationships
From “Healthy Relationships,” Preceding Page practical; yet, taking the first step isn’t easy. In relationships, e.g., “Difficult Conversations,”9
Both are important. What I'm suggesting is that most relationships needing improvement, or “Thanks for the Feedback.”10 Relationships
relationships between individuals are equally, if each party needs to “buy in.” You might think, are hard. There’s a lot to learn. Fortunately,
not more important, to understand and improve. “it’s not mostly my fault; it’s the surgeons who there are lots of good models to learn from.
need to behave better.” I’m not judging who is
What are specific ways that the interactions more at fault when things aren’t going well. I’m not promising you a rosy world if you
in this dyad impact patient safety for better or But I can say for sure that nothing will get work at this. But I think it’s worth your time for
worse? I've heard many stories in my almost 35 better if at least one person doesn’t try to start your patients’ safety to try as much as you can.
year's experience as a member of a quality a constructive dialogue. Doing nothing will mean nothing will change. If
assurance review committee and via many your efforts succeed, you’ll have made a huge
vignettes told to me as I’ve probed more into Here’s some suggestions, any one of which
you could consider trying (I didn’t make these advance for patient safety, and you're likely to
this topic. Consider an anesthesiologist, who
all up. Many of your colleagues already do find more joy and meaning in your professional
even though junior, may be more expert than
some of these. You can think of your own too): daily life.
the surgeon in physiology, and who tried to
communicate to the surgeons that their diagno- 1. Take a surgeon to lunch or dinner. (this is an Dr. Cooper is professor of Anaesthesia, Harvard
sis did not comport with the data. Not having an especially productive thing to do when a new Medical School and the Department of Anaesthe-
established, trusting relationship with the sur- surgeon joins your hospital) sia, Critical Care and Pain Medicine, Massachu-
geon, the surgeon disregarded his sugges- 2. Form a focus group to discuss one of the setts General Hospital. He is a founder of the
tions. When the anesthesiologist was right, the articles in the references. Listen more than APSF, retiring from the Board of Directors and
patient outcome was much worse than it might you talk. Seek to understand why behaviors Executive Committee in 2018 after 32 years of ser-
have been if the surgeon collaborated with him. you observe may come from different vice. This article is a summary of a portion of his
Or the anesthesiologist who, despite the sur- sources than you imagine.* lecture for the Ellison C. Pierce, Jr., MD, Memorial
geon’s extensive experience in performing cri-
3. Work together on common issues, e.g., low- Lecture at the American Society of Anesthesiolo-
cothyrotomy, disregarded the surgeon’s
suggestion that it was time to move the difficult- ering the risk of surgical infection, which gists Annual Meeting, October 19, 2019.
airway algorithm along and the situation dan- anesthesia professionals might contribute to;
implement emergency manuals together. Dr. Cooper reports no conflicts of interest.
gerously went downhill. These were true stories
that are likely familiar to you. 4. Assume the best intentions, as in the “basic
REFERENCES
assumption”7 now widely taught in simulation
There is the flip side: I heard independently 1. Katz D, Blasius K, Isaak R, et al. Exposure to incivility hinders
and modified for this application as: “my sur- clinical performance in a simulated operative crisis. BMJ
from an anesthesiologist and surgeon about a
gical colleagues are intelligent, doing things Qual Saf. 2019;28:750–757.
situation where their prior trusting relationship
in the best interest of their patients, and 2. Cooper JB. The critical role of the anesthesiologist-surgeon
was clearly an enabler for success. A needle relationship for patient safety. Anesthesiology. 2018;
trying to improve.” It’s not always so, but it
with a pop-off suture had separated prema- 129:402–405. (Pub ahead of print) (co-publication in J Amer
mostly is. Coll Surg. 2018;227:382–86) http://anesthesiology.pubs.
turely. The surgeons, unable to locate the
asahq.org/article.aspx?articleid=2695026
needle, were fixated deep in the wound seek- 5. When someone does something that makes
3. Cooper JB. Respectful, trusting relationships are essential
ing to find it. The anesthesiologist, watching the you think “WTF,” the “F” should stand for for patient safety, especially the surgeon-anesthesiologist
struggle, waited for an appropriate moment to “frame.”8 Instead of attributing a negative ste- dyad. Ellison C. Pierce, Jr. Memorial Lecture. Annual Meet-
reotype, be curious, seek to find out what the ing of the American Society of Anesthesiologists, October
suggest a brief regrouping and consideration of
19, 2019. Accessed November 11, 2019. https://www.apsf.
options. That led to the use of fluoroscopy to rationale behind the action is. You are likely org/news-updates/watch-jeffrey-b-cooper-ph-d-give-the-
find the needle. I’ve heard of situations as well to learn something new; even if what the anesthesiology-2019-asa-apsf-ellison-c-pierce-memorial-
where a surgeon gave his or her anesthesia person is doing isn’t optimal or right, it’s usu- lecture/
colleague a heads-up the day before, or earlier, ally for a good reason. If there's not a good 4. Lingard L, Reznick R, DeVito I, et al. Forming professional
identities on the health care team: discursive constructions
about a patient issue with anesthesia-related reason, you’ll have an easier time getting of the “other” in the operating room. Med Educ.
implications that averted a patient safety issue. I them to see things differently versus just 2002;36:728–734.
suspect that most anesthesiologists reading assuming they are irrational. 5. Katz JD. Conflict and its resolution in the OR. J Clin Anes.
2007;19:152–158.
this have had similar experiences. Indeed, 6. Train together in simulation with the entire
6. McLain Smith D. The elephant in the room. San Francisco:
some of you are fortunate enough to have reg- team. It’s a proven way to improve the team’s Jossey-Bass; 2011.
ular experiences of this latter type rather than crisis management skills. In addition, it puts 7. Rudolph J. What’s up with the basic assumption. https://har-
the former. Every patient should be so lucky. you in a position to have dialogue at an equal vardmedsim.org/search-results/?swpquery=basic+assump
level. More simulation programs are doing tion Accessed November 11, 2019.
If what I’m describing rings true for you, 8. Rudolph J. Helping without harming. SMACC, Berlin, June
what can be done to make this dyad function this. You could even take the lead and sug-
26, 2017. https://www.youtube.com/watch?v=eS2aC_
more routinely effective? I’m not aware of gest a team try it out. Sure, it costs money yyORM Accessed October 29, 2019.
empirical evidence to guide suggestions, but and takes a lot to organize (just getting the 9. Stone D, Patton B, Heen S. Difficult conversations: how to
there are some general principles about rela- people there is tough), but it’ll pay off in lots discuss what matters most. Penguin Books, Ltd., London,
1999.
tionship-building that can apply. I’ve sug- of ways.
10. Stone D, Heen S. Thanks for the feedback. Penguin Books,
gested in the article a few things that are 7. Read a book about communicating across New York, 2014.
You can also read