Martin B. Leon, MD Columbia University Medical Center Cardiovascular Research Foundation New York City - CACI
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below

CACI in Partnership with TCT:
40 Years of Interventional Cardiology
Martin B. Leon, MD
Columbia University Medical Center
Cardiovascular Research Foundation
New York City 12 mins
Sunday, October 29, 2017
Disclosure Statement of Financial Interest
TCT 2017 Denver, CO; Oct 29 – Nov 2, 2017
Martin B. Leon, MD
Within the past 12 months, I or my spouse/partner have had a financial
interest/arrangement or affiliation with the organization(s) listed below.
Affiliation / Financial Relationship Company
• Grant / Research Support Abbott, Boston Scientific, Edwards
Lifescience, Medtronic
• Consulting Fees / Honoraria Abbott, Boston Scientific
• Shareholder / Equity Cathworks, Claret, Elixir, GDS, Medinol,
Mitralign, Valve Medical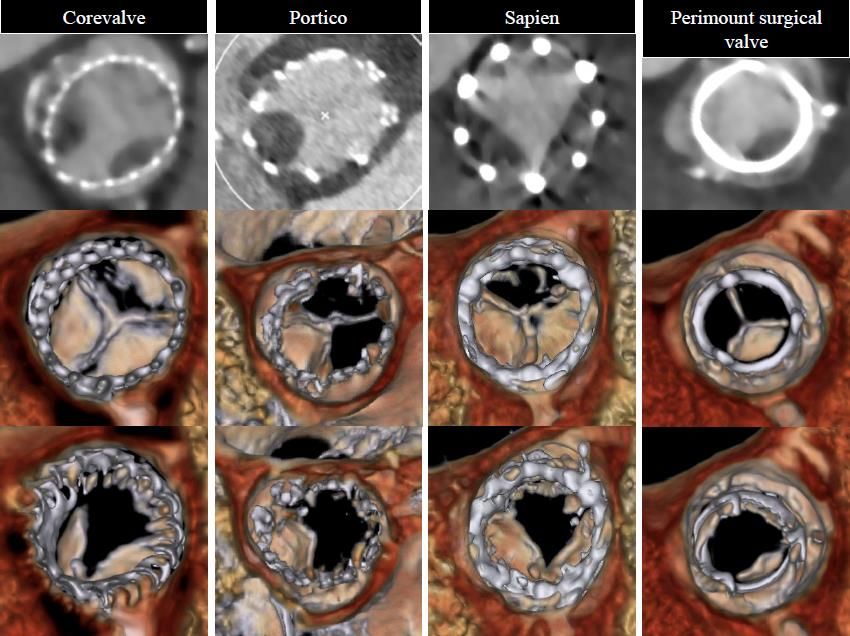
TAVR in Perspective
History
TAVR in Perspective
History
• The “proof-of-concept” first TAVI case
performed by Alain Cribier and his team in
Rouen, FR deserves special attention on this
15th year anniversary!
Antegrade Approach:
Guidewire Position
in LV
MR
Valve Positioning

April 16, 2002; FIM-TAVI, Transseptal
April 16, 2002; FIM-TAVI, Transseptal
April 16, 2002; FIM-TAVI, Transseptal
15 min Post-TAVI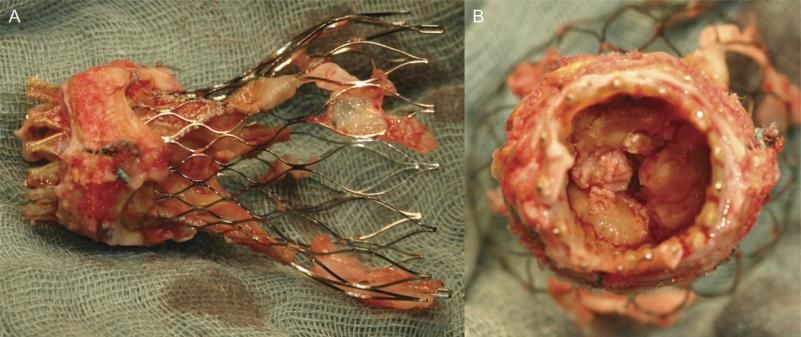
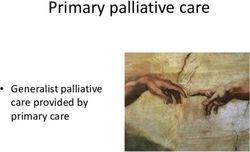
TAVR in Perspective Current Role
TAVR in Perspective
Current Role
• Explosive growth in TAVR worldwideEstimated Global TAVR Growth SOURCE: Credit Suisse TAVI Comment –January 8, 2015. ASP assumption for 2024 and 2025 based on analyst model. Revenue split assumption in 2025 is 45% U.S., 35% EU, 10% Japan, 10% ROW This year > 100,000 and by 2025 almost 300,000!
TAVR in Perspective
Current Role
• Explosive growth in TAVR worldwide
“Drivers” of TAVR Growth
1. commitment to evidence-based medicine
2. rapid technology advancement
3. simplification of the procedure
4. striking reduction in complicationsSymptomatic AS: SAVR Risk
Pipeline of
AS with no
Published symptoms
Low Intermediate High Extreme TAVR Trials
2010 PARTNER 1B across the
2011 PARTNER 1A
2012 spectrum of
2013
Corevalve US HR Corevalve US ER
aortic stenosis
2014
CHOICE
Investigational devices
2015 NOTION PARTNER 2B
2016
Since 2007, in the U.S.,
PARTNER 2A
PARTNER 2 S3
Edwards Sapien/Sapien XT/S3
Medtronic CoreValve/Evolut R
> 15,000 patients have been
PARTNER 2 S3i
2017 Boston Lotus
SURTAVI
Upcoming Direct Flow Medical Direct Flow
enrolled in FDA studies (including
UK TAVI Abbott Vascular Portico
REBOOT
2017
10 RCTs) with multiple generations REPRISE 3
SALUS (stopped)
Symetis Acurate Neo
Any available TAVR system
2018
of four different TAVR systems!
PARTNER 3
US Evolut R LR
PORTICO IDE
SOLVE-TAV
24 TAVR SCOPE 1
TAVR UNLOAD
2019
2020 NOTION 2 RCTs SCOPE 2
2021 EARLY TAVR
Capodanno D, Leon MB. EuroIntervention 2016TAVR Systems with CE-Approval (2007-15)
Courtesy of S. WindeckerTAVR Newcomers
Global Landscape (#25)
• Sapien 3 • J – Valve Ausper
• VitaFlow (Microport)
• Evolut R • Taurus One
• Lotus • Trinity
• Colibri
• Acurate • Inovare
• Current
Portico • Future
Thubrikar
• Valve Medical
• Leaders!
Direct Flow Contenders?
• Triskele
• BioValve (Biotronik)
• Engager • MyVal (Meril Lifescience)
• Jena Valve • HLT Meridian
• NVT (Nautilus)
• Centera • Xeltis
• Venus A Valve • Zurich TEHVTAVR Accessory Devices
Cerebral Embolic Protection (CEP)
• Dual, independent filter (proximal and distal)
Proximal Filter
cerebral embolic(Innominate
protectionArtery)
device with visible
embolic debris capture and
9–15 mmremoval
• The 3rd generation CE-marked embolic protection
device
• Universal size and shape
• Deflectable compound curve sheath facilitates
cannulation of LCC Distal Filter
• Right transradial 6F sheath access using
(LCC Artery)
a standard
6.5–10 mm
0.014” guidewire
• Filters are out of the way of TAVI delivery catheter
and accessories during the TAVI procedureTAVR Perspectives
The Minimalist Strategy
No general anesthesia; use “conscious sedation”
(MAC) with attendant anesthesiologist
> 70% of TAVR cases worldwide are
No TEE, but available TTE support
good candidates for a “minimalist”
Percutaneous
procedural TF access with percutaneous closure
strategy!
Minimize IV lines,
Median LOSno after
Foley catheters,
TAVR is 2careful
days at
sedation and pain meds
Columbia-NYP Hospital!
No ICUs… monitor in recovery area
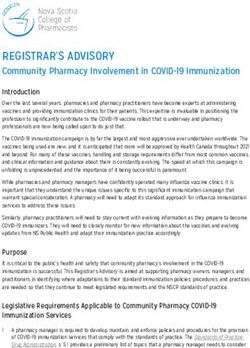
Rapid ambulation and early discharge plans (1-2 dys)All-Cause Mortality at 30 Days
Edwards SAPIEN Valves (As Treated)
20%
PARTNER 1 and 2 Trials
(Overall and TF Patients)
15%
10%
6.3%
5.2%
5% 4.5%
3.7% 3.5%
2.2%
1.6%
1.1% 1.1%
0%
P1B (TF) P1A (All) P1A (TF) P2B (TF) P2B XT (TF) S3HR (All) S3HR (TF) S3i (All) S3i (TF)
175 344 240 271 282 583 491 1072 947
SAPIEN SXT SAPIEN 3Strokes (All) at 30 Days
Edwards SAPIEN Valves
20%
PARTNER 1 and 2 Trials
15%
(Overall and TF Patients)
10%
6.7% Neurologist evaluations (pre- and post)
5.6%
5% 4.1% 4.3%
2.6%
1.5%
0%
P1B (TF) P1A (All) P2B (TF) P2B XT (TF) S3HR (All) S3i (All)
179 344 276 284 583 1076
SAPIEN SAPIEN XT SAPIEN 3Moderate/Severe PVL at 30 Days
Edwards SAPIEN Valves
50%
PARTNER I and II Trials
40% Overall and TF Patients
30%
24.2%
20%
16.9%
12.0% 11.5%
10%
4.2%
2.9%
0%
P1B (TF) P1A (Overall) P2B (TF) P2B XT (TF) S3HR (Overall) S3i (Overall)
179 344 276 284 583 1076
SAPIEN SAPIEN XT SAPIEN 3TAVR in Perspective
Current Role
• Explosive growth in TAVR worldwide
• Evolving recommended use guidelines
and expansion of clinical indicationsTAVR Guidelines
The “New” AHA/ACC Focused Update
Severe AS
Symptomatic
Surgical Risk Strata
Low Intermediate High Prohibitive
SAVR SAVR or TAVR SAVR or TAVR TAVR
IB IIa B IA IATAVR Guidelines
The “New” ESC/EACTS VHD Report
Severe AS
Symptomatic
Surgical Risk Strata
Low Intermediate or High Prohibitive
SAVR SAVR or TAVR TAVR
IB IB IBTAVR Risk Assessment
Risk Stratification Redefined
Traditional
Extreme/
Low Intermediate High
Inoperable
Contemporary
Extreme/inop
LowLower risk
Intermediate Higher
High risk erable
Courtesy of N. PiazzaExpanding TAVR Clinical Indications
A Transformative Technology
at the Crossroads?
• Bioprosthetic aortic valve failure
• Low-risk patients (? all-comers)
• Low-flow, low-gradient AS
• Bicuspid AV disease
• AS + concomitant disease (CAD, MR, AF)
• Severe asymptomatic AS
• Moderate AS + CHF
• High-risk ARTAVR for Bioprosthetic Valve Failure
Valve-in-Valve
• 365 high-risk patients with aortic
bioprosthesis failure treated with TAVR
• 30-day and 1-yr all-cause mortality was 2.7%
and 12.4% respectively
Webb JG et al. JACC 2017;69:2253-62TAVR in Perspective
Current Role
• Explosive growth in TAVR worldwide
• Evolving recommended use guidelines
and expansion of clinical indications
• The Heart Team is now the central
vehicle for managing patients with
complex valve diseaseTAVR in Perspective
Current Role
• Explosive growth in TAVR worldwide
• Evolving recommended use guidelines
and expansion of clinical indications
• The Heart Team is now the central
vehicle for managing patients with
complex valve disease
• Acceptance of multi-modality imaging
for diagnosis, therapy guidance, and FUTAVR Accessory Devices
Novel Imaging Systems
Multi-modality Imaging is the RULE!
Angio CTA
TTE TEE + 3DTAVR in Perspective The Future
TAVR in Perspective
The Future
• Improved disease awareness and
access to TAVR (esp. underserved
populations)AS Based on Surgical Experience
2015 Severe Symptomatic AS Patients in the U.S.1
Patients
Age
(1) Nkomo 2006, Iivanainen 1996, Aronow 1991, Bach 2007, Freed 2010, Iung 2007, Pellikka
2005, Brown 2008, Thourani 2015,AS Including the TAVR Experience
2015 Severe Symptomatic AS Patients in the U.S.1
Patients
Age
(1) Nkomo 2006, Iivanainen 1996, Aronow 1991, Bach 2007, Freed 2010, Iung 2007, Pellikka
2005, Brown 2008, Thourani 2015,AS Patients Undiagnosed and Untreated
2015 Severe Symptomatic AS Patients in the U.S.1
Patients
Age
(1) Nkomo 2006, Iivanainen 1996, Aronow 1991, Bach 2007, Freed 2010, Iung 2007, Pellikka
2005, Brown 2008, Thourani 2015,TAVR in Perspective
The Future
• Improved disease awareness and
access to TAVR (esp. underserved
populations)
• Further innovation of TAVR platforms
(e.g. tissue engineered heat valves)Zurich Tissue Engineered Heart Valve
A “Living” Aortic Valve
Courtesy of Simon P. Hoerstrup, MD, PhDXeltis
Endogenous Tissue Restoration (ETR)
• Synthetic matrix made of novel
biobsorbable supramolecular
polymers using electrospinning
techniques
• Polymer leaflets mounted on
nitinol self-expanding frame
• Regrowth of endogenous tissue
coincident with bioabsorption of
polymer implant
• Natural self-healing anti-
Valve after inflammatory leaflets
bioabsorptionXeltis
Endogenous Tissue Restoration (ETR)
• Synthetic matrix made of novel
biobsorbable supramolecular
polymers using electrospinning
techniques
• Polymer leaflets mounted on
nitinol self-expanding frame
• Regrowth of endogenous tissue
coincident with bioabsorption of
polymer implant
• Natural self-healing anti-
Animal implant inflammatory leafletsTAVR in Perspective
The Future
• Improved disease awareness and
access to TAVR (esp. underserved
populations)
• Further innovation of TAVR platforms
(e.g. tissue engineered heat valves)
• Realization of ‘completely’ new clinical
indications for TAVR - leveraging the
advantages of less-invasive RxEARLY TAVR Trial
Study Flow
Asymptomatic Severe AS and 2D-TTE (PV ≥4m/s or AVA ≤1 cm2)
Exclusion if patient is symptomatic, EF8
Treadmill Stress-Test
Stress-Test Normal Stress-Test Abnormal
CTA and Angiography
TF- TAVR eligibility
Early-TAVR Randomized Trial Early TAVR Registry
Randomization 1:1
Stratified by STS (3)
Clinical
TF- TAVR
Surveillance
Primary Endpoint (superiority): 2-year composite
of all-cause mortality, all strokes, and repeat
hospitalizations (CV)TAVR UNLOAD Trial
Study Design
(600 patients, 1:1 Randomized)
Follow-up:
TAVR Heart Failure TAVR + 1 month Primary Endpoint
UNLOAD LVEF < 50% OHFT 6 months Hierarchical occurrence
Trial NYHA ≥ 2 1 year of:
All-cause death
Optimal HF R
Clinical Disabling stroke
International therapy
endpoints Hospitalizations for
Multicenter (OHFT) HF, aortic valve
OHFT Symptoms
Randomized Moderate AS Alone disease
Echo
Change in KCCQ
QoL
Reduced AFTERLOAD
Improved LV systolic
and diastolic functionTAVR in Perspective
The Future
• Re-defining AS disease classification,
pathophysiology, and “trigger points”
for interventionLMP Ventricular Load MIT - CRF Collaboration
Enhanced Prediction Models
• Predict who will better benefit
from TAVR
• Decide when is the best timing
Impedance spectrum of intervention
5000
Refine
Modulus (Dynes*s/cm^2)
4500
4000
3500
3000
2500
characterization
of CV dynamics
2000
1500
1000
500
0
0 1 Harmonic
2 3 4
to enable
PWA Vascular State Redefine the PathophysiologyTAVR in Perspective
The Future
• Re-defining AS disease classification,
pathophysiology, and “trigger points”
for intervention
• There are still important knowledge
gaps with TAVR which must be resolved
(esp. valve leaflet thickening &
thrombosis, durability, and optimal
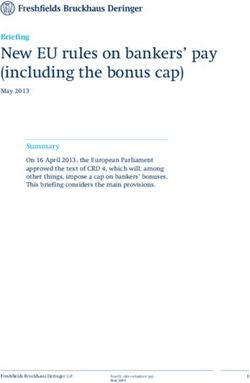
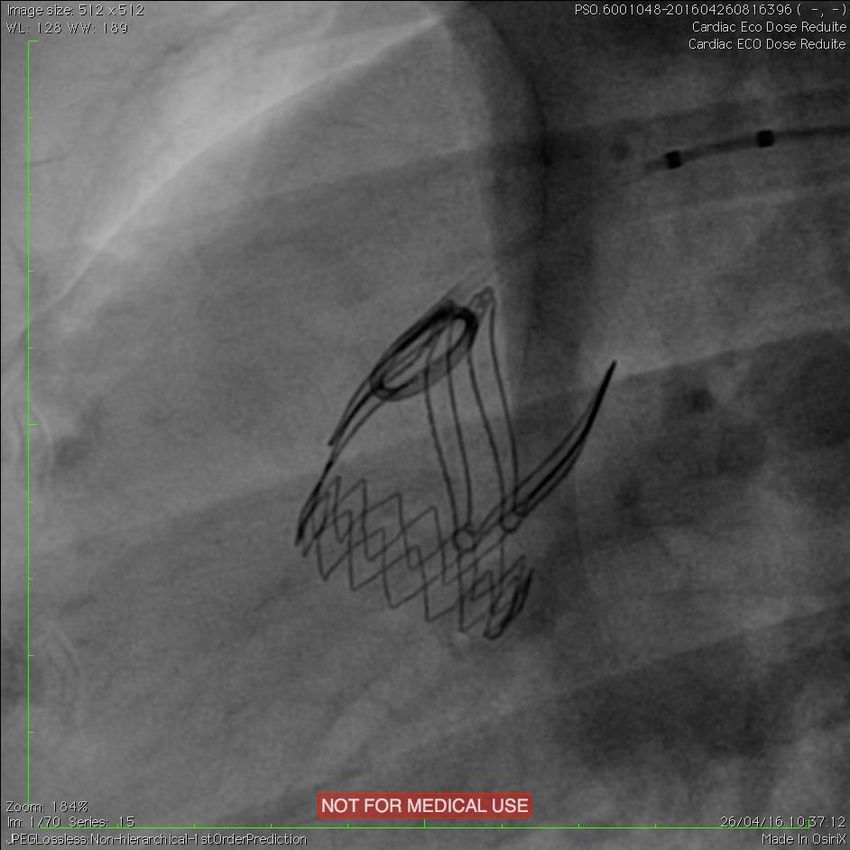
adjunctive pharmacotherapy)Valve Leaflet Abnormalities
Diastole
Systole
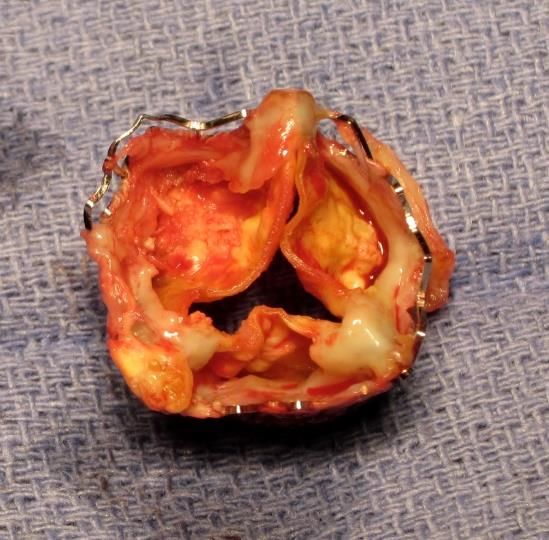
Makkar, et al. NEJM 2015All TAVR systems will certainly demonstrate evidence of valve degeneration during long-term (> 5 years) assessments, especially if echo criteria are applied in the definitions of durability! Surgically explanted Sapien and CorveValve THVs
New EU guidance with
standardized definitions
and endpoints to assess
bioprosthetic aortic valve
deterioration and failure
Capodanno D et al. Europ Heart J 2017TAVR Adjunct Pharmacology Customized Patient-Based Therapy
TAVR is a breakthrough therapy
for our patients!
92 yo man with
critical AS…#1 TAVR
at Columbia-NYP
• severe COPD
• creat 2.8
• previous CABG
(patent LIMA)
• EF 30%
• Class IV CHF
• STS 15.5%You can also read