MDS-ES INFUSION COURSE 2020 APOMORPHINE, MANAGEMENT OF ADVERSE EVENTS AND COMPLICATIONS OF APOMORPHINE THERAPY
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
MDS-ES INFUSION COURSE 2020
APOMORPHINE, MANAGEMENT OF ADVERSE EVENTS AND
COMPLICATIONS OF APOMORPHINE THERAPY
Tove Henriksen, MD,
Movement Disorder Clinic
University Hospital of Copenhagen
Nymphaea caerula, blue Egyptian water lily
Apomorphine, T. Henriksen, 2020
Royal Botanic Gardens Kew, UK
Apomorphine, T. Henriksen, 2020 APOMORPHINE INFUSION

SIDE EFFECTS
Dopaminergic effect/systemic effect
Apomorphine, T. Henriksen, 2020
Mode of administration
Technical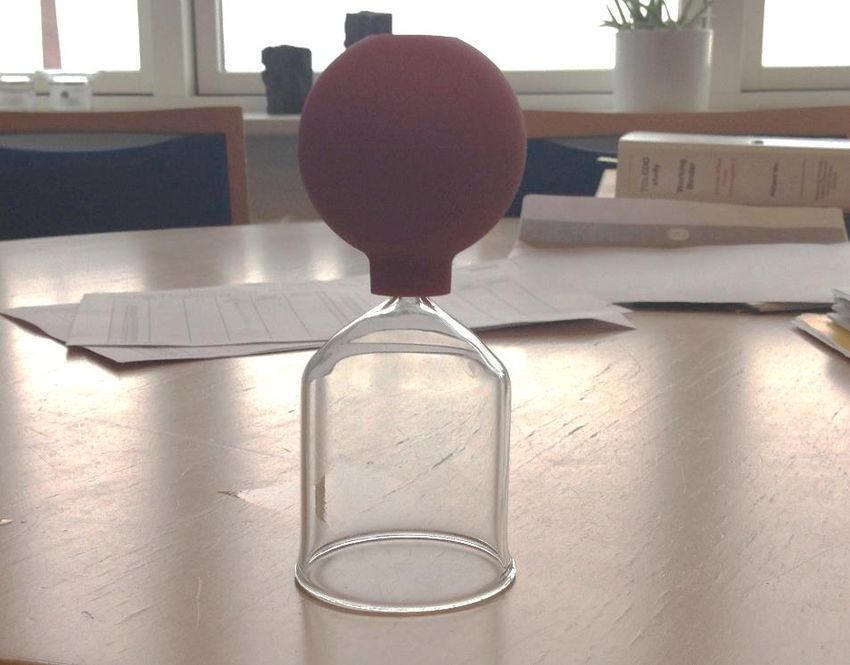
Apomorphine, T. Henriksen, 2020 Long term evaluation of CSAI of 82 PD patients Tertiary hospitals in Spain Prospective data Mean follow up 20 months Baseline data compared with last follow up data

Apomorphine, T. Henriksen, 2020 From 148 adverse events collected: 93 (62.8%) were mild 44 (29.7%) moderate 11 (7.4%) severe but did not lead to treatment dropout. No case of HA was reported in these 82 long-term-treated patients. MOVEMENT DISORDERS 2008
Apomorphine, T. Henriksen, 2020 • 10 years 230 patients with APO (mean age 66.8) • As of June 2016, 93 remained on Apo, 137 had stopped. • Main indication for APO lack of DBS criteria • Average time since APO onset was 40.0 months. • In the active group, APO decreased off-state in 4 h • Dyskinesia and balance did not worsen. • Cognitive decline did not change within the first 15 months. • Hallucinations were the same within the first 39 months. • The presence of subcutaneous nodules was the most frequent adverse event • The main reason for discontinuation was side effects, being psychosis the • most common

REASONS FOR DISCONTINUATION, 137 (59,6%)
Apomorphine, T. Henriksen, 2020
Apomorphine, T. Henriksen, 2020

Apomorphine, T. Henriksen, 2020 ICD BEFORE AND AFTER APO
Apomorphine, T. Henriksen, 2020
Apomorphine, T. Henriksen, 2020 STUDY DESIGN
Apomorphine, T. Henriksen, 2020 SIDE EFFECTS
DEALING WITH SIDE EFFECTS, 1
Nausea, vomiting
Usually in the starting phase/titration
Domperidone 20 mg t.i.d.
EMA may 2014, 10 mg tid, for a maximum of 1 week
Apomorphine, T. Henriksen, 2020
If present at apomorphine test
Lower initial dose, slow up titration
Ortostatic hypotension
Frequent in PD
Domperidone
Critical review of the total medication
Anti-hypertensive medication, diuretics
Water repletion (2-2.5 l/day)
Liberal intake of salt/salt tablets 500 mg t.i.d.
Ibrufen 200 mg t.i.d.
Rarely fludrocortison 0.1 mg b.i.d.Apomorphine, T. Henriksen, 2020
Small increased risk of serious cardiac adverse drug reactions related to the
use of domperidone, including QTc prolongation, torsade de pointes, serious
ventricular arrhythmia and sudden cardiac death.
A higher risk was observed in patients older than 60 years, adults taking daily
oral doses of more than 30 mg, and those taking QT prolonging medicines or
CYP3A4 inhibitors concomitantly
Domperidone should be used maximum treatment duration should not usually
exceed one week.
10 mg orally up to three times daily (maximum dose of 30 mg daily). Adults
may also be given 30 mg twice daily
Contraindication: underlying cardiac disease such as congestive heart failure,
and when coadministered with QT - prolonging medicines or potent CYP3A4
inhibitors.Apomorphine, T. Henriksen, 2020
Prophylactic use of antiemetics was prohibited except in those
who had been receiving antiemetic treatment before the start
of study.
20% of the subjects reported gastrointestinal AEs, including
nausea and vomiting.
Some of them required an antiemetic or apomorphine dose
reduction and disappeared soon after these action taken, but
none discontinued the study for gastrointestinal AEs,
suggesting that it is feasible to start apomorphine without pre-
treatment with antiemetics.DEALING WITH SIDE EFFECTS, 2
Sedation
Rare rapports on sudden sleep attacts, similar to other DA’s
Apomorphine, T. Henriksen, 2020
Information important
Driving
Operating machines, work hazard
Hemolytic anemia
Reports of a positive Coomb’s test in both DA’s and l-dopa
In very rare cases corticosteroids
A Coomb’s test before starting, and every ½ y
If positive and associated with anemia:
Full haematological work up and cessation of ApomorphineDEALING WITH SIDE EFFECTS, 3
Neuropsychiatric complications
Close monitoring
Apomorphine, T. Henriksen, 2020
Clozapine
Rivastigmine
Case: 54 y old patient with familial PD. On amantadin and
high L-dopa load, already internet addiction prior to
apomorphine. After risky financial transactions (Struhal et al
2012):
Dysregulation Syndrome
Psychosis
Depression and paranoia lead to suicide attemptPSYCHOSIS
Switching from conventional p.o. dopamin agonist to
apomorphine infusions reduces confusion, hallucinations,
Apomorphine, T. Henriksen, 2020
paranoia (Ellis 1997)
Improvement in mood on BDI when switching to Apomorphine
infusion (Di Rosa 2003)
DBS and Apomorphine: motor effect greater in DBS, but NPI
better in Apomorphine group (De Gaspari 2006, Alegret 2004)
• Open label pilot study, fluctuations and severe visual
hallucinations, apomorphine, NPI-Q improved significantly
(Van Laar 2010)
▫ Due only to reduction in hallucinations
Cognitive impairment the red flag?• Open label pilot study
• 8 ppts with PD, fluctuations and severe visual hallucinations
▫ Despite use of anti-psychotics and/or cholineesterase inhibitors in
7/8
• Mean apomorphine 5.2 mg/h
• LEDD did not change significantly
• NPI-Q improved significantly
▫ Due only to reduction in hallucinations
• NPI-Q distress score improved significantly
• Mean MMSE and mean FAB unchanged
• Discontinuation of oral DA Apo
mor
phin
e, T.
HenDOPAMINE DYSREGULATION SYNDROME
Related to
Impulse control disorders
Pathological gambling
Apomorphine, T. Henriksen, 2020
Kleptomania
Compulsive sexual behavior
Binge eating
Compulsive buying
Punding
L-dopa, Apomorphine, oral DA
Injections worse then infusions to produce DDS (Lees A
et al 2000)
Case rapport, woman pen 24/ day, 75 mg apomorphine
(Tellez C 2006)There is a trend showing
that the proportion of ICD
is related to the selectivity
for D3 receptors over D2
receptors, with
pramipexole having the
highest association with, or
frequency of ICD.
Apomorphine, T. Henriksen, 2020
32% for pramipexole,
25% for ropinirole,
16% for pergolide,
22% for rotigotine,
10% for apomorphine
6.8% for bromocriptineApomorphine, T. Henriksen, 2020 Role of D3 in impulse–control disorder: the proportion of patients with impulse– control disorder for pramipexole and other agonists correlates with the D3 selectivity, compared to D2, of these drugs. For each molecule of pramipexole that occupies a D2 receptor to alleviate Parkinson’s disease, there are 66 molecules of pramipexole that occupy the D3 receptor
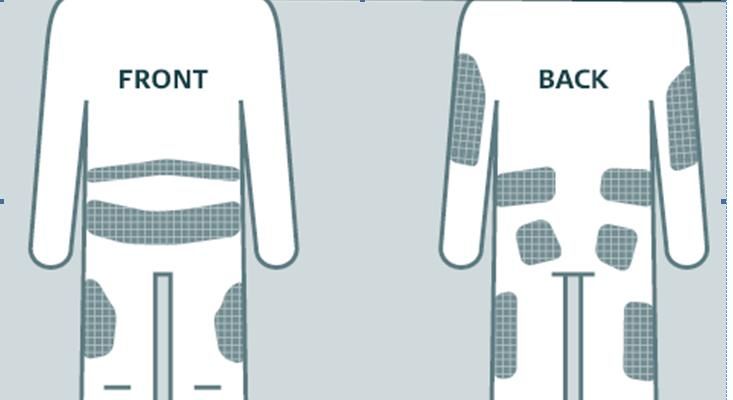
DEALING WITH SIDE EFFECTS, 4
Subcutaneous noduli/infection
Almost all patients
Apomorphine, T. Henriksen, 2020
Localized discomfort at infusion site
Require attention not to result in
Serious skin infection
Ulcerations
Scaring of the skinApomorphine, T. Henriksen, 2020
Apomorphine, T. Henriksen, 2020
REDUCE RISK OF NODULI
Educate expert carer (spouse, district nurses) by the outpatient
clinic as soon as the treatment is started
Proper hygiene at injection site
Apomorphine, T. Henriksen, 2020
A new needle/injection line every day
Rotation of injection site every day
No reuse of the needle if it falls out
Ultra sound treatment of the injection sites once or twice a week
from the start
A minimum angle of 45° of the needle to avoid injection intra-
dermal
Hand massages/massage with a spiky rubber ball of the injected
areas on a daily basis
To avoid long term skin problems in general ensure sufficient
protein intake monitored by weight control on a regular
basis/dietician.Apomorphine, T. Henriksen, 2020
If nodules/panniculitis develops:
Silicone gel patches placed overnight on injection site
Apomorphine, T. Henriksen, 2020
Diluting the apomorphine solution from 0.5% to 0.25%.
Change type of needle, use Teflon (Comfort short, Cleo)
instead of steel
Change injection technique
If this is not helpful, let a specialist nurse monitor the
procedure used by the patient/carer of placement of
needle to give a brush up of the right procedure
If infection occurs:
Oral antibiotics according to resistance pattern of
bacteria and if needed, surgical treatment of abscessSUGGESTIONS TO PREVENT NODULES
Apomorphine should only be used in centers with
experience using the treatment, this could include specialist
nurses and an outpatient setup suited for this specialized
treatment.
Expert carer (spouse, district nurses) including education
Apomorphine, T. Henriksen, 2020
commenced by the outpatient clinic as soon as the
treatment is started
Rotation of injection site every dayApomorphine, T. Henriksen, 2020
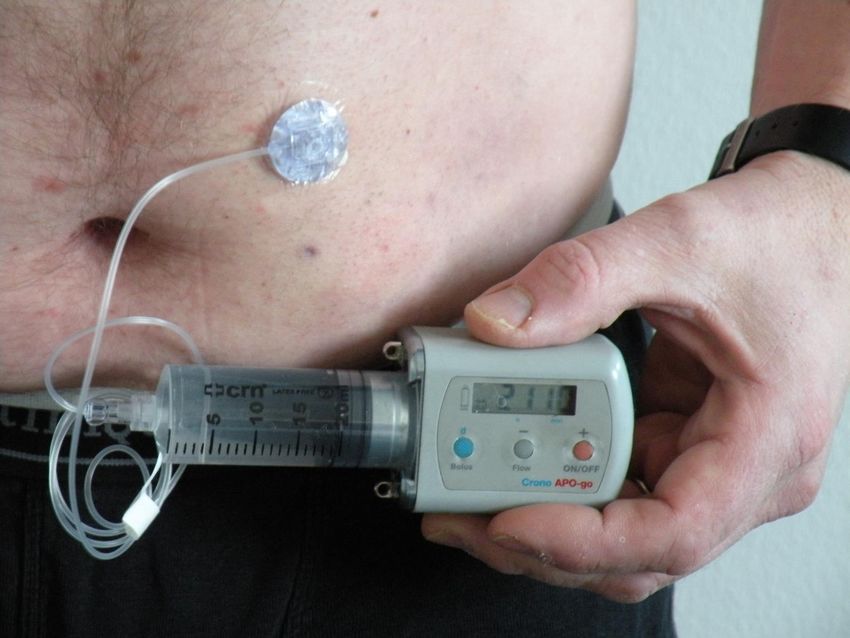
TECHNICAL ISSUES
Clotting of connections
Arrest of pump
Leakage at injection site
Disconnection of/rotation of syringe
Never leading to cessation
Apo
mor
phin
e, T.
HenREASONS FOR STOPPING PUMP TREATMENT,
72 OF 103 PATIENTS
Apomorphine, T. Henriksen, 2020SIDE EFFECTS RESULTING IN STOPPING TREATMENT
Apomorphine, T. Henriksen, 2020MAXIMIZE COMPLIANCE
Perform an apomorphine test
effect and side effects, give the patient and caregiver an idea of what the
treatment entails
Ensure that the clinical problem in question can be expected to be
alleviated by the treatment
Convey to patient and caregiver that the treatment is
Apomorphine, T. Henriksen, 2020
not disease modifying
involves numerous follow up visits
can have complications and side effects
Demonstrate pump, syringe and needle for the patient and caregiver
Inform about the risk of discoloration of clothing by apomorphine
Educate the patient, spouse and district nurses/ other professional,
caregivers in the pump
Provide patient and caregiver with emergency phone numbers for 24
h help
Propose an information source not related to the hospital
Reliable websites
Peers from a local Parkinson AssociationApomorphine, T. Henriksen, 2020 THANK YOU FOR YOUR ATTENTION
You can also read