Midwest Diagnosis: Immigration Reform and the Healthcare Sector
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below

IMMIGRATION INITIATIVE
Midwest Diagnosis: Immigration
Reform and the Healthcare Sector
By Nicole Fisher
March 2016
Executive summary address health issues or avoid receiving care alto-
gether, compromising health outcomes.
Healthcare is a critical part of the local economy, pro-
viding jobs for millions of Midwesterners and billions >> The linguistic and cultural assets of foreign-born
of dollars in wages across the 12-state region. However, healthcare workers are increasingly in demand
the growing healthcare needs of the baby boomers as given the growing diversity of the United States.
they age, coupled with acute shortages of healthcare Yet visa shortages and licensing issues complicate
workers, are straining the sector. Immigrants—for- their hire.
eign-born physicians, researchers, nurses, health aides, A continued stalemate on immigration reform means
and hospital workers—are key to the future vitality of these issues will only grow in urgency. Changes based
healthcare in the United States, and federal immigra- on the following policy recommendations, developed
tion reforms are urgently needed to ensure that the with input from regional stakeholders from the health-
sector is able to maximize their contributions. How- care sector, would not only remedy these issues in the
ever, legislation remains stalled in Congress, leaving Midwest but would ensure a vibrant healthcare sector
Midwest healthcare to grapple with challenging issues: across the country:
>> US-born medical school graduates are likely to >> Issue visas according to labor force demands.
pursue careers in lucrative specialties and relocate
>> Remove quotas and caps on doctors and surgeons.
to coastal cities, causing severe shortages of critical
primary care, pediatric, and family medicine physi- >> Address credentialing challenges for foreign-born
cians in the rural Midwest. professionals.
>> Foreign-born healthcare professionals who have >> Allow undocumented individuals to access some
completed their training overseas face compli- forms of insurance.
cated, inconsistent reaccreditation processes in the >> Train healthcare professionals to provide linguis-
United States, leaving many unable to practice in tically and culturally competent care to diverse
their fields. populations.
>> Undocumented immigrants, unable to access It is vitally important that the region properly plan for
health insurance under current laws, are dependent the employment, economic, and healthcare needs of
on expensive, ineffective emergency room care to all residents, regardless of country of origin.
THE CHICAGO COUNCIL ON GLOBAL AFFAIRS - 1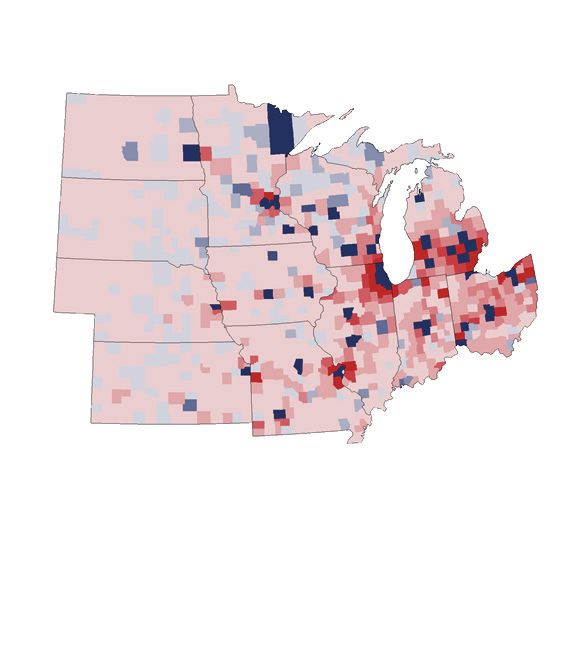
Introduction Figure 1A
The healthcare sector is fundamental to the devel- Hospital Employment as a Percentage of
opment and sustainability of the Midwest economy. the Midwest Economy
In states like Missouri, Nebraska, and North Dakota,
the healthcare sector is the number one employer. In Hospital Percent of total
North Dakota alone, seven of the state’s top 10 employ- State employment employment
ers are in the healthcare sector. Hospitals throughout (Nov. 2015) (Nov. 2015)
the region are responsible for employing nearly 1.3
Illinois 238,700 3.87%
million people, an average of more than 4 percent of
each state’s total employment (see figure 1A). In fact,
Indiana 117,200 3.73%
the US Bureau of Labor Statistics calculates that the
education and healthcare services sector provided Iowa NA NA
nearly 5 million jobs—an average of 15 percent of total
state employment across the 12-state region—and Kansas 48,100 3.33%
generated $51 billion in wages (see figure 1B).1
Michigan 202,900 4.49%
The vitality of the healthcare sector, however,
depends on a functioning immigration system: for-
Minnesota 107,600 3.71%
eign-born professionals accounted for 16 percent of all
civilians employed in healthcare occupations and one- Missouri 123,400 4.18%
fourth of practicing physicians in 2010.2
But more workers are needed. The Midwest Nebraska 44,300 4.51%
is particularly plagued by a physician shortage.3
North
Furthermore, labor-force issues will be exacerbated in 17,200 4.30%
Dakota
the coming years as the healthcare needs of retiring
baby boomers strain the system. Workforce gaps also Ohio 251,000 4.60%
extend to lower-skilled, lower-paid healthcare jobs,
such as home healthcare aides and technicians, as South
24,300 5.51%
US-born workers choose more-lucrative positions in Dakota
other industries. While foreign-born healthcare work-
Wisconsin 111,100 3.74%
ers are well-positioned to fill these gaps in the labor
force (and have been doing so for years), the outdated Total/
1,285,800 4.18%
federal immigration system, along with complicated Average
state-level credentialing requirements, pose hurdles.
Note: Percent of total employment calculated by dividing
What’s more, healthcare systems not only strug- figures from November 2015 “Hospital Employment” from
gle to meet the needs of undocumented immigrants “State and Area Employment, Hours and Earnings” pages,
www.bls.gov/sae/data.htm, by November 2015 total state
unable to access care under current policy, but they employment from “Midwest Information Office-State Economies
also lack the ability to capitalize on the foreign-born at a Glance” pages, http://www.bls.gov/regions/midwest.
workers' linguistic and cultural assets, which are Source: US Bureau of Labor Statistics, “State and Area
Employment, Hours and Earnings” pages, “Hospital Employment”
The Chicago Council on Global Affairs is an independent, nonpartisan organization. All statements of fact and expressions of opinion con- important to providing quality care for increasingly for November 2015, www.bls.gov/sae/data.htm.
tained in this report are the sole responsibility of the author and do not necessarily reflect the views of The Chicago Council on Global Affairs diverse communities.
or of the project funders.
The Midwest healthcare sector needs updated
Copyright © 2016 by The Chicago Council on Global Affairs immigration laws that reflect today’s economic and region will also continue to miss out on productivity
demographic realities and are poised to respond not gains from a robust, fully functioning sector.
All rights reserved.
only to the nation’s but also the region’s unique chal-
Printed in the United States of America.
lenges. Until Congress enacts reforms to immigra-
New strains on an old sector
This report may not be reproduced in whole or in part, in any form (beyond that copying permitted by sections 107 and 108 of the US tion policy that address these issues, the sector will The United States is experiencing an important demo-
Copyright Law and excerpts by reviewers for the public press), without written permission from the publisher. For further information about
The Chicago Council or this study, please write to The Chicago Council on Global Affairs, 332 South Michigan Avenue, Suite 1100, Chicago IL,
continue to struggle with the challenges of providing graphic shift: growing numbers of baby boomers are
60604, or visit The Chicago Council’s website at www.thechicagocouncil.org. quality care with limited personnel and resources. The reaching retirement age. Many regions, like the Mid-
THE CHICAGO COUNCIL ON GLOBAL AFFAIRS - 3Figure 1B Colleges. Overall numbers of students enrolled in Hospital in Evanston are foreign born (48 of 84), as are
medical school is up 25 percent over 2002, to an all- 71 of the 79 internal-medicine and preliminary-year
Education and Health Services as a Percentage of the Midwest Economy time high of nearly 21,000 in 2015. Also encouraging residents at Chicago’s St. Joseph Hospital.16
is the fact that the field is growing more diverse, with Currently, at CoxHealth in Springfield, Missouri,
Education and health Education and health services Total wages earned in Latino enrollees up 6.9 percent and African-American 135 of the 450 physicians across the five-hospital sys-
State services employment as a percentage of total the education and health
(Oct. 2015) employment (Oct. 2015) services industry (Q1 2015) enrollees up 11.6 percent. The number of foreign-born tem are foreign born. That’s 30 percent of the system’s
students increased 9 percent between 2009 and 2015.10 doctors, which is more diverse than the surrounding
Illinois 906,500 14.70% $9,678,070,844 However, unless the federal government approves community, indicating just how strong of an influence
funding to add 4,000 more physicians a year to the the immigrant community already has on the state’s
Indiana 458,200 14.65% $4,473,133,627
pipeline, demand cannot be met and access to health- healthcare system.17
care will remain out of reach for many Americans In addition to physicians, roughly one-fifth of
Iowa 139,700 8.49% $2,058,114,782
throughout the Midwest.11 nurses and home healthcare and psychiatric aides,
Kansas 192,900 13.49% $1,841,888,793 As it stands, the United States will face a short- and more than one-sixth of dentists, pharmacists, and
age of 46,100 to 90,400 physicians by 2025.12 These clinical technicians in the United States were foreign
Michigan 665,300 14.78% $6,927,420,691 shortages will be acutely felt in rural areas, like those
in Wisconsin, which are home to 28 percent of the Box 1
Minnesota 513,200 17.78% $5,579,467,538
state’s population but only 11 percent of its practicing
Missouri 445,900 15.26% $4,408,317,860 physicians.13 Filling Gaps in Leadership and
Wisconsin is not alone in its struggles to provide Research18
Nebraska 155,400 15.85% $1,313,999,072 quality care. Most of the Midwest faces similar cir-
cumstances. More than a quarter of the residents of Italian-born Giovanni Piedimonte is physician-in-chief
North Dakota 59,300 14.88% $673,228,145
Indiana, Iowa, Michigan, Minnesota, Missouri, and of Cleveland Clinic Children’s Hospital and chair of the
Nebraska live in a rural community. In South Dakota, Cleveland Clinic Pediatric Institute. He came to the United
Ohio 908,000 16.65% $8,935,677,945
the number is closer to one in two.14 There are simply States more than 25 years ago, conducting pediatric
research and doing his residency in California before
South Dakota 70,800 16.11% $703,855,539 not enough native-born healthcare workers to meet
completing a fellowship in pulmonary medicine in North
the growing demand and to do so in the geographic
Carolina. He now has over 20 years of experience as a hos-
Wisconsin 447,400 15.14% $4,481,412,122 areas with the greatest need. The Midwest urgently pital administrator and has worked for the last three years
needs a federal immigration policy that facilitates at the prestigious Cleveland Clinic, one of the nation’s top
Total 4,962,600 $51,074,586,958
hiring more foreign-born workers, filling current job five hospitals. “I came from nothing, worked hard, and
Note: Education and health services as a percentage of total employment calculated by dividing the employment figures in column 1 by the openings, and meeting local healthcare needs. played by the rules,” he said. “The United States was built
total state employment for October 2015, http://www.bls.gov/regions/midwest. with stories like this.”
Sources: US Bureau of Labor Statistics Midwest Office, “State Economy at a Glance” pages, Education and Health Services for October 2015, Immigrants already provide care Piedimonte cites “huge personnel shortages” among
http://www.bls.gov/regions/midwest; US Bureau of Labor Statistics, “Quarterly Census of Employment and Wages,” 2015 First Quarter, his peers in hospital leadership positions, in addition to a
www.bls.gov/cew. More than one-quarter of physicians and surgeons in
dearth of primary care physicians and a shrinking supply
the United States were foreign born in 2010. These sta- of specialists in most pediatric subspecialties. These gaps
tistics are consistent in the Midwest, where 25 percent need to be filled by qualified professionals, foreign born or
west, have experienced significant losses in their work- growing rosters of individuals enrolled in Medicaid of physicians and surgeons were born outside of the US born. He adds that he would “be happy to hire
ing-age population, causing challenging labor shortag- due to the Patient Protection and Affordable Care Act country. In Des Moines, Iowa, for example, 150 of the American candidates, but sometimes there are no such
es across a variety of industries, including healthcare. (ACA) and Medicaid expansion.7 In Ohio, for exam- estimated 600 physicians employed by Mercy Medical applicants.”
The US Census Bureau projects a 36 percent growth ple, 25 percent of residents are now covered under He has seen his Colombian-born wife, also a pediatri-
Center were born outside the United States. According
cian and healthcare researcher, challenged by the US im-
in the number of Americans over age 65 in the next government-funded Medicaid and 18 percent under to administrators at Mercy, foreign-born doctors tend migration system. “In order to get [research] funding from
decade, with nearly one-third of all physicians retiring Medicare.8 And these individuals already live in a state to be the system’s “superstars,” an essential part of the the National Institutes of Health, you need to be a perma-
because they fall in that age demographic.4 ranked among the lowest in the country for total pop- workforce. “Without the immigration of professionals nent resident,” he said, citing what is an obstacle for many
At the same time, the number of individuals need- ulation health, meaning its residents are less healthy to Iowa, healthcare would be in complete crisis,” said foreign-born medical students in the United States on
ing healthcare is increasing. Those 65 or older who are and need more care.9 one hospital administrator.15 temporary visas.
enrolled in Medicare make up more than 14 percent As demand for healthcare services increases, the The same is true at Presence Health, the largest “The United States gave me the opportunity to become
who I am today,” he said. “I’m a physician, not a politician,
of the population.5 However, in less than 15 years, an number of medical school students will also increase Catholic healthcare system in Illinois, with more than
but I think others who want to come into this country and
estimated 20 percent of Americans will be 65 or older by 7,000 graduates every year for the next 10 years, 150 locations throughout the state. Administrators said to contribute to its greatness should be able to do so.”
and on Medicare.6 Midwestern states have also seen according to the Association of American Medical that more than half the resident doctors at St. Francis
4 - MIDWEST DIAGNOSIS: IMMIGRATION REFORM AND THE HEALTHCARE SECTOR THE CHICAGO COUNCIL ON GLOBAL AFFAIRS - 5born in 2010.19 It is easy to see that this growing pop- Figure 2 Native-born physicians are, therefore, choosing Box 2
ulation of foreign-born workers has become a corner- more lucrative specializations, such as dermatology,
stone of healthcare in the Midwest. Specialties Pursued by Native- and Foreign- obstetrics, and orthopedics. This leaves generalist Supporting Foreign-Born Doctors in
Yet despite these significant cohorts of foreign-born Born Health Professionals in the United positions like family medicine, internal medicine, and Rural Communities31
workers across the sector, the immigration system States for the 2010–11 Academic Year pediatrics more likely to be filled by foreign-born prac-
curbs their contributions from entry point and educa- titioners (see figure 2).24 Randy Munson, manager of the New Physicians for
tional training to long-term employment. For exam- J-1 Visa US Medical Foreign-born medical professionals are, therefore, Wisconsin program of the Wisconsin Office of Rural Health,
ple, enrollment restrictions and visa requirements Physicians (%) Graduates (%) has been recruiting physicians—native born and foreign
key in addressing the shortage of primary care physi-
for medical and nursing school cohorts limit many born—to work in Wisconsin for more than 25 years. “If doc-
cians in the United States, particularly in underserved
Internal medicine 45.8 15.0 tors are from India or Indiana, they need support in a new
immigrants’ ability to come study in the United States, communities where there are fewer specialists and
environment,” he said.
and outdated visa caps limit hospitals’ ability to recruit Pediatrics 11.0 7.4 therefore a greater need for a broad range of medi- Turnover rates among foreign-born doctors can be es-
these professionals once they finish their training. US cal skills. In fact, the American Academy of Family pecially high, given the isolating nature of work in rural
immigration law also provides almost no opportuni- Family medicine 7.9 5.8 Physicians estimates that although family physicians communities. Munson encourages clinics, hospitals, and
ties for foreign paraprofessionals—such as healthcare make up less than 15 percent of the outpatient work- healthcare systems to “take visas on a case-by-case basis”
aids or nursing assistants—to enter the country as General surgery 7.2 8.4 and to understand the factors—such as marital status,
force, they perform about 42 percent of office visits in
either temporary workers or permanent residents, rural areas.25 connections to the community, previous experience living
Psychiatry 5.2 3.8 in the Midwest—that often bolster the retention of for-
contributing to disparities in care that could be pre-
vented by an updated immigration system that reflects Neurology 4.1 1.5
Challenges in rural communities eign-born professionals in rural areas.
He also coaches foreign-born doctors to become a part
current economic and demographic realities. Rural care is a particularly urgent issue in the Midwest, of the communities where they are working. “There’s an
Overall, the United States’ outdated federal immi- Obstetrics and whose combined 16 million rural residents account for
1.9 5.0 onus on doctors to ‘be seen’ in town; living and working in
gration system presents several challenges to the gynecology
28 percent of the 12-state region’s population.26 The la- the community will help their practice grow.”
healthcare sector: shortages of highly skilled workers, bor shortages affecting the nation as a whole translate Even with challenges, “some foreign-born doctors stay
Orthopedic surgery 1.4 4.5
shortages of workers in entry-level jobs, limited access to particularly compromised quality of care in rural 10 to 15 years in rural communities,” he said, citing the case
to care for immigrants, and meeting the linguistic and of an Indian-born born doctor who worked at urban Cook
Diagnostic radiology 1.4 5.5 communities.
cultural needs of an increasingly diverse patient base. County Hospital in Chicago before successfully transfer-
For example, in Wisconsin’s 104 federally desig-
ring to a rural community in Wisconsin.
Anesthesiology 1.3 5.9 nated primary care Health Professional Shortage Areas
Shortages of highly skilled labor (HPSAs)—many of them rural communities—only
Other specialties/
12.9 37.2 71 percent of primary healthcare demands are cur-
In the Midwest, demand for high-skilled medical labor subspecialties states like Iowa, for example, tend to fill its ratio of 30
is far outpacing supply. The current shortage is no rently being met.27 The Wisconsin Hospital Association waivers quickly, leaving administrators at Des Moines
surprise, however, as it was predicted as far back as Total 100 100 projects that the state will show a shortfall of more
Mercy Medical Center to lament that they are “forced
1990, when the National Center on Education and the than 2,000 physicians by 2030.28 These disturbing
Sources: Educational Commission for Foreign Medical Graduates,
to pass on great candidates” every year. “The Conrad
Economy issued a workforce report discussing future trends come despite the fact that the Wisconsin Office
2012 Annual Report, http://www.ecfmg.org/resources/ECFMG- 30 needs to become the Conrad 50,” they say.32
2012-annual-report.pdf; Sarah E. Brotherton and Sylvia I. of Rural Health is one of the country’s oldest such
high-skilled labor needs.20 With the supply of US-born Etzel, “Graduate Medical Education, 2010–2011,” January 2012, Hospitals and medical centers in rural regions of
medical professionals falling so far short of demand, American Medical Association, http://gsm.utmck.edu/medexp/ bureaus, founded in 1979.
the Midwest often do not have the population density
documents/gme.pdf. In addition to native-born medical students being
it is unfortunate and irresponsible that current immi- to sustain specialty and subspecialty facilities, nor the
gration policy still does not promote the inclusion of The Chicago Council on Global Affairs more likely to pursue specialized fields, reports sug-
financial means to support such practices.33 Therefore,
foreign-born professionals into communities most in gest they are also more likely to pursue work in coastal
they face challenges in meeting the accreditation
need, especially rural areas. Nor does current policy cities on graduation, a trend that particularly deepens
physician shortages in the rural Midwest (see figure requirements that would allow them to teach clinical
encourage foreign-born medical practitioners to stay to specialize more than its foreign-born counterpart,
3).29 Foreign-born doctors, therefore, are increasingly education and train medical students. These factors
in those underserved regions once their education- owing partially to pay.22
key to filling labor gaps in these rural communities. Yet lead some to fear that the healthcare pipeline for rural
al and professional requirements have met federal From 2000 to 2004, the median physician income
few programs incentivize them to fill those gaps. communities will dry up even faster than in other geo-
standards.21 for all primary care positions increased only 10
The US Citizenship and Immigration Services’ graphic areas.
percent, compared to a 16 percent increase in the
Native-born trend toward specialization Conrad 30 J-1 Waiver Program allows foreign-born
same time for all nonprimary care specialties. These Other obstacles for foreign-born professionals
Despite an increasing healthcare demand that ne- increases come on top of an already skewed physician graduates from US medical schools to remain in the
United States postresidency if they practice in an Across the employment spectrum, foreign-born pro-
cessitates a greater number of general and primary pay scale that compensates specialists up to 45 per-
care practitioners, the native-born population that cent more than primary care physicians.23 HPSA for no less than three years. However, with just fessionals face unique obstacles. In rural areas, the
completes medical school in the United States tends 30 waivers allotted per state, the number of these phy- challenges are even more acute. Factors like integra-
sicians still falls far short of demand.30 Midwestern tion issues, connecting with patient populations, and
6 - MIDWEST DIAGNOSIS: IMMIGRATION REFORM AND THE HEALTHCARE SECTOR THE CHICAGO COUNCIL ON GLOBAL AFFAIRS - 7Figure 3 established networks that may give them an advan- Box 4
tage—relocation may be required for IMGs. On being
Shortage and Surplus of Primary Care Physicians in Midwestern States asked if he would consider relocating to Boise, Idaho, Midwestern Legislation Tackles
from Chicago, one IMG told a nonprofit caseworker International Medical Credentialing
that he would “take a residency on Mars if it would
Shortage of over 50 physicians mean that I could practice as a doctor.”39 Facing severe gaps in their local healthcare workforces,
40 to 50 physician shortage Indeed, IMGs may be willing to accept the rural Midwestern legislators are embracing the talents of for-
or remote posts passed up by their peers, offering eign-born professionals trained overseas.
30 to 40 physician shortage
In 2014, Missouri’s state legislature created a new licen-
a solution to the acute physician shortages in these
20 to 30 physician shortage sure classification for “assistant physicians,” designed for
communities. However, given the significant personal,
work-authorized immigrants who have passed required
10 to 20 physician shortage professional, and financial burdens involved in re-cre- sections of the U.S. Medical Licensing Examination but
Shortage of up to 10 physicians dentialing, many IMGs opt for employment in other have not completed postgraduate residency in the United
fields or are underemployed in lower-paying jobs. States. While rule making for the legislation is still in pro-
Surplus of over 50 physicians Rigorous accreditation requirements are essential cess, assistant physicians will eventually be able to practice
40 to 50 physician surplus to ensuring a high standard of professional quality in in Missouri, helping alleviate workforce gaps in the state. 44
the US healthcare system, but they vary widely from Minnesota’s International Medical Graduates
30 to 40 physician surplus
Assistance Program, launched in 2015, helps foreign-born
state to state and may create situations where states
20 to 30 physician surplus physicians in navigating the complex process of credential-
compete against each other for IMGs, raising the pos-
10 to 20 physician surplus ing and licensing in the United States. 45 The bill (S.F. 1049)
sibility of further losses for regions like the Midwest. includes financial provisions to support up to five for-
Surplus of up to 10 physicians For example, Midwestern states like Nebraska, eign-born physicians in residency each year and accept pri-
Missouri, and North Dakota require foreign graduates vate support for additional slots. With over 300 immigrant
Source: Connor Ryan, “Doc Shortage or Maldistribution?,” American Action Forum, August 14, 2014, http://americanactionforum.org/weekly- to complete two more years of postgraduate training physicians living in the state—two-thirds of whom are es-
checkup/doc-shortage-or-maldistribution.
than their native-born counterparts, making these timated to be general practitioners—this initiative could
The Chicago Council on Global Affairs states less appealing to those who attended school be an invaluable source for quality care. 46
outside the United States, despite the vast number of
jobs in the sector.40
in the United States for less than five years. The pro-
low pay often cause high turnover among foreign-born to school for training and education, compete for resi- Carmen Velasquez, founder of Alivio Medical
gram provides information, education, mentorship,
doctors in rural areas, prompting some state and dency, and retake examinations—all after having com- Center in Chicago, cites examples of foreign-born
resources, and advocacy to support foreign-trained
hospital human resources departments to resist hiring pleted similar requirements in their home countries.37 nurses moving as far away as Texas for licensure after
healthcare professionals who must be recertified to
them in the first place.34 In some cases, because of intense competition for being turned away in Illinois, where accreditation
practice in the United States.47 While the reach of these
The Wisconsin Office of Rural Health conducted a limited residency slots—native-born candidates or for- practices by the state were more restrictive.41 Licensure
organizations is still fairly limited—Upwardly Global
study over a five-year period that showed how inte- eign-born graduates of US medical schools may have issues also pose challenges in Kansas, where cardio-
has offices in Chicago and Detroit and is expanding
gration challenges can influence the retention rate of vascular providers from Kansas City sometimes drive
Box 3 throughout the Midwest—taking on accreditation
physicians on J-1 visas compared to their US-born- up to four hours into rural areas of their state to com-
challenges is no longer a solo endeavor for many high-
and-trained counterparts. While retention of US-born- pensate for the lack of local providers. Sometimes
and-trained physicians was close to 90 percent after Undocumented, MD-PhD those same providers have to go into Missouri and
skilled individuals.48
five years of practice, the retention rate for interna- Nebraska to see patients, as licensure requirements
tional medical graduate physicians who were origi- According to Cesar Montelongo, an undocumented stu- have exacerbated shortages in those states and reci- Demand for entry-level healthcare jobs
dent in Illinois, it was easier for him to gain admission to
nally on J-1 visas was notably lower. A full 30 percent procity policies allow Midwestern doctors to cross cer- In addition to depending on high-skilled foreign-born
a highly competitive MD-PhD program than to get his US
of these physicians did not complete three years of tain state boundaries because of need.42 workers to fill doctor and physician shortages, the
visa to practice medicine. “I am one of the first undocu-
service in their assigned HSPA.35 mented immigrant students to have been accepted into an Innovative national nonprofits such as Upwardly healthcare system also relies on low-skilled for-
Foreign-born healthcare professionals who MD-PhD program,” he said. Global and the Welcome Back Initiative help for- eign-born workers to fill other roles. Many positions
completed their education overseas, known as According to his estimates, of the 731,000 applications eign-born healthcare professionals navigate com- require less education but are equally important to the
International Medical Graduates (IMGs), face even to US medical schools in 2014, just 20,343—less than 3 per- plicated licensing requirements and also provide overall functioning of the Midwest’s healthcare ecosys-
more complicated accreditation and licensure pro- cent—were accepted. The number admitted to MD-PhD support services such as career coaching, resume tem and communities.
programs was just 626. Despite his beating these odds and
cesses. While many IMGs are fully authorized to work writing, and professional networking.43 Similarly, the Today, a wide range of jobs, from home health
having lived in the United States for 20 years, and the over-
in the United States, they cannot always practice in Women’s Initiative for Self Empowerment, located in aides to housekeeping staff to data-entry technicians,
whelming shortage of healthcare professionals with his
the healthcare field.36 To maintain US standards, IMGs skill set, Montelongo is still unable to obtain legal status. 38
Minnesota, coordinates a Foreign Trained Professional are more likely to be filled by foreign-born healthcare
seeking to practice as physicians may need to return Recertification Program for refugees who have lived workers than their native-born counterparts (see fig-
8 - MIDWEST DIAGNOSIS: IMMIGRATION REFORM AND THE HEALTHCARE SECTOR THE CHICAGO COUNCIL ON GLOBAL AFFAIRS - 9Figure 4 Box 5 45 million Americans 65 or older already have two or
more chronic conditions that require ongoing medical
Distribution of Direct-Care Workers Definitions of Visas attention or limit activities of daily living and require
Among immigrants, a higher share are working as doctors or lower-skilled nursing aides than among the native born medical assistance.57
J-1 Visa (also known as J Waiver): A temporary visa admin- In 2012, about 58,500 long-term-care service pro-
Percent of foreign born in the healthcare sector working as... Percent of native born in the healthcare sector working as... istered by the US Department of State that allows partic- viders—including adult day service centers, home
ipants to work in “exchange program”-style jobs, ranging
Nursing, psychiatric, and home health aides Registered nurses healthcare agencies, hospices, nursing homes, and
from au pair to scientist to student to physician. In most
19 16.4 assisted living facilities—served approximately 8 mil-
cases, the participant is expected to return to his or her
Registered nurses Nursing, psychiatric, and home health aides home country for at least two years after completion of lion people in the United States.58 The number of peo-
16 10.3 the program. ple receiving care is expected to grow more than 230
Physicians and surgeons Medical assistants and other healthcare support occupations percent—to 27 million—by 2050.59 These trends not
7.7 4.5
H-1B Visas: A temporary visa, awarded via lottery, for high- only mean there will be more job openings in the long-
Medical assistants and other healthcare support occupations Physicians and surgeons skilled workers in specialty occupations. H-1B holders may term care industry but also a need for workers with the
5 4 work only for their sponsoring employer. Requirements skills to address the increasingly complicated health
Personal and home care aides Licensed practical and licensed vocational nurses include a minimum of a four-year university degree or
demands of the elderly as they age.60
4.9 3.8 equivalent and pay at the “prevailing wage.”
In fact, day-to-day care for this population has
already begun to create financial and human-resource
Top five total: Top five total: EB-2 Visa: A permanent visa for a foreign national with an
challenges for the country (care averages $10,082 a
52.6% 38.8% “exceptional ability” to offer the US labor force. Applicants
year for each person older than 65, compared to $3,931
will typically hold an advanced degree or its equivalent.
Source: Audrey Singer, Immigrant Workers in the U.S. Labor Force, Brookings Institution and Partnership for a New American Economy, March 15, for those younger than 65) and intensify costly work-
2012, http://www.brookings.edu/research/papers/2012/03/15-immigrant-workers-singer. force gaps.61 Nevertheless, even though there are not
system also remark on the irony that the Springfield enough US-born workers to meet current demand, the
The Chicago Council on Global Affairs
metro area is among the least diverse in the nation country has yet to update its immigration system in
yet it has a strong immigrant workforce in healthcare. a way that maximizes the contributions of immigrant
However, this foreign-born population is still not workers in this sector, especially as they pertain to low-
ure 4). This trend is partially attributed to the low pay positions, leaving the healthcare sector increasingly enough to fill the community’s health-related needs.
and service-oriented nature of these jobs, as many reliant on immigrants to fill gaps.51 skilled caregivers.
As with higher-skilled positions, certification for
US-born workers have the mobility and language skills As with high-skilled gaps in the healthcare work- these lower-skilled healthcare services is handled by
to move to more-lucrative professions. It can also be force, labor shortages persist in entry-level healthcare each state, often creating confusing barriers to entry.54
Immigrants’ access to care
attributed to the fact that many low-skilled healthcare jobs, despite foreign-born workers’ increasingly filling However, across all states, becoming a certified nurs- In addition to growing workforce gaps across the
positions require less than a high school education. them. In some areas of the Midwest, filling entry- and ing assistant or home healthcare aide requires less healthcare sector, the outdated US immigration sys-
Only 76 percent of foreign-born workers 25 or older even middle-level positions is such a pressing need than two weeks training and is not subject to federal tem presents other hurdles to clinics, hospitals, and
have completed high school, compared to 95 per- that hospitals and healthcare systems are partnering regulations.55 Because this training is so cost effective healthcare-service providers across the country.
cent of US-born citizens, often making these roles a with trade schools and community colleges, as well in plugging labor gaps, some large corporations are Perhaps most urgent is the issue of immigrants’
good fit for their limited US standardized educational as starting their own instruction series to educate and being accused of trying to abuse systems—like the unequal—or often nonexistent—access to health-
background.49 train a new workforce. These various programs cater to H-1B business visa lottery (see box 5)—so they can care services and insurance benefits, despite recent
young adults, immigrants, and others, depending on hire more immigrant workers at lower cost.56 If this improvements in overall rates of insurance coverage
Distribution of direct-care workers the community need and program focus. resulting from the ACA. With few options to access
trend continues, the federal government will need to
As the US baby boomer population continues to age, In an effort close gaps caused by the 800 job change immigration laws and businesses practices. care outside of emergency room treatment, unin-
the demand for long-term home healthcare by profes- vacancies throughout its system, administrators at sured immigrants—both undocumented and autho-
sionals trained to provide personal care and services Missouri’s CoxHealth have developed a scholarship Baby boomers change demand rized populations—often forgo necessary preventive
for the elderly and chronically and terminally ill is program with Ozarks Technical Community College to Given the aging population of baby boomers in the screenings, resulting in delayed disease detection and
growing. Yet the annual salaries for these demanding build a pipeline of healthcare aides, nursing assistants, United States, one healthcare field that has seen a worsening of chronic conditions. Insurance payment
jobs, which typically require less than a high school and therapists.52 The hospital system has also created substantial—and necessary—influx of low-skilled and gaps also leave hospitals struggling to finance expen-
degree, was as low as $20,820 in 2012, with minimal Cox College, which offers a variety of programs rang- entry-level workers is long-term care. With at least sive emergency room care and to meet the level of
increases projected.50 Native-born workers, even those ing from certifications to graduate degrees, training one-fifth of Americans projected to be 65 or older by demand, especially from immigrants.
with low levels of education, tend to pass up these local workers as young as 16 for futures in healthcare 2030, Medicare will face mounting costs for individu- Providing access to adequate healthcare services
jobs, which are often physically demanding, tedious, careers. Still, administrators report, “there just aren’t als who live longer, use more care, and have multiple for uninsured immigrants adds a layer of complex-
and poor paying, for more-lucrative, less-demanding people to fill the jobs.”53 Representatives from the health concerns. In fact, an estimated 75 percent of the ity to existing challenges in caring for increasingly
10 - MIDWEST DIAGNOSIS: IMMIGRATION REFORM AND THE HEALTHCARE SECTOR THE CHICAGO COUNCIL ON GLOBAL AFFAIRS - 11diverse populations. In particular, cultural differences Figure 5 Box 6 financial assistance costs to the Presence Health sys-
and access disparities mean that foreign-born and tem in 2014.73
native-born populations often interact with their local Reasons for Being Uninsured among Hispanic Health Paradoxes Healthcare systems in smaller cities, like Des
When asked in
Uninsured their own
Adults, Fallwords,
2014 the remaining
healthcare systems very differently, leaving already Moines, are also challenged by costs related to the
uninsured said that the main reason they were
short-staffed hospitals struggling to provide appropri- “Immigrants come to this country with health advantag- uninsured. At Mercy Medical Center, charity care costs
without
When insurance
asked, was… u
the remaining ninsured said that the main
es,” said Fernando DeMaio, an associate professor of sociol-
ate linguistic and culturally competent care for com- reason they were without insurance was... (%) the system an estimated $10 million per year. To a
ogy and co-director of the Center for Community Health
munities with a greater number of immigrants. smaller system, this can be just as debilitating to the
Equity at DePaul University in Chicago. “The challenge is
6 that this advantage, on average, is lost over time,” leading
bottom line as $65 million can be to a larger system.74
The challenges of Medicaid and charity care 3
3 to an irony known as the Hispanic Health Paradox. 68 Further, reliance on emergency departments com-
Immigration policy intersects with healthcare policy in Hispanic immigrants in the United States have better plicates health outcomes in rural hospitals, which
7
the long-debated issue of providing care to uninsured health and live longer than their non-Hispanic white coun- see many of the Midwest’s 57,000 migrant agriculture
immigrants. In 2014, noncitizens were more than three terparts despite being poorer and having harsher, more workers present in hospital EDs with injuries caused
times as likely as their native-born counterparts to 6 dangerous jobs and less access to healthcare and educa- by farming equipment.75 In these situations, accessing
tion. 69 According to the Population Reference Bureau, “fa- emergency care often requires traveling long distances,
be uninsured (31 percent and 9 percent, respective- 48 tal chronic diseases—heart disease, cancer, chronic lung
ly), although they represented only 20 percent of the which worsens the acute nature of these traumas.
12 disease, and stroke—are much less prevalent among older
total US uninsured population.62 A 2014 Kaiser Family For hospitals that serve uninsured patients, known
Hispanics than among other racial and ethnic groups.”
Foundation survey of low-income Americans revealed Experts agree that Hispanics’ relative youth, along with as safety-net hospitals, charity care costs will con-
that seven percent of respondents were uninsured lower rates of smoking and higher rates of community in- tinue to grow as congressional budget cuts mount
4
because of their immigration status (see figure 5). volvement, contribute to better mental and overall health in the coming years. Between growing Medicare and
From 2013 to 2014, health insurance coverage rates 12 outcomes than for other groups. 70 The challenge comes in Medicaid rosters, federal budget cuts, and increasing
increased for all groups because of mandates and extending positive health outcomes to second or third healthcare costs, the financial burden may prove to be
opportunities of the ACA. In fact, the foreign-born generations, as Hispanics face higher risks of cardiovascu- prohibitive for some healthcare providers.76
Don’t need it lar disease than Americans overall, which is linked to high
population, including both naturalized citizens and
rates of obesity, diabetes, and high blood pressure.71
noncitizens, experienced a larger increase in health Opposed to the ACA/prefer to pay penalty Cultural understanding and competency
insurance coverage rates than did the native-born
Don’t know how to get it in high demand
population (6.4 percentage points for the foreign The uninsured are most often left with the emer-
born and 2.4 percentage points for the native born).63 gency room as one of their only options when they Providing linguistically and culturally competent care
Immigration status
Illinois, Iowa, and Nebraska felt the impact of those require care. The Emergency Medical Treatment and for an increasingly diverse immigrant population is a
insurance increases most dramatically among the Told they were ineligible Labor Act, passed in 1986, stipulated that no one can Box 7
12 Midwest states, as their immigrant populations Unemployed/work doesn't offer/ be turned away from an emergency department (ED)
increased the most over the last two decades.64 not eligible at work regardless of immigration status. Thus, the emergency Expanding Health Insurance Access
Further, undocumented immigrants are blocked
Don’t know/refused
room has become the most utilized source of care
in Illinois
from purchasing benefits on public exchanges in the for this population, even though ED care is the most
Midwest despite overall improvements in insurance Other reason costly.72 What’s more, emergency care is far less effec- Presence Health and other Illinois-based healthcare pro-
rates for the previously uninsured. Given the informal Too expensive
tive than regular preventative care in the long run, viders, along with nonprofit organizations, civic leaders,
nature of many jobs held by unauthorized workers— further driving up costs for follow-up treatment. The and law-enforcement officials, are part of the steering
one-half of low-income noncitizens are employed in Source: Kaiser Family Foundation, “Key Facts about the Uninsured expenditures for this type of care for the uninsured— committee of Healthy Illinois, a campaign committed to
Population,” October 2015, http://kff.org/uninsured/fact-sheet/
agriculture, construction, or service industries—they key-facts-about-the-uninsured-population/. called charity care—dramatically affect the bottom expanding health insurance options, including those for
are not able to purchase insurance through employ- line of hospitals and clinics across the Midwest. undocumented immigrants. 77 “This country can’t afford
The Chicago Council on Global Affairs not to have universal access to healthcare. It will cost us
ers, as these three industries are historically the least Challenges in providing charity care play out dif-
more in the long run,” said Carmen Velasquez, founder
likely in the United States to offer employer-spon- ferently for urban and rural healthcare systems. For
of Alivio Medical Center in Chicago and a member of the
sored insurance.65 Additionally, even those who are example, Chicago-based Presence Health estimates it
steering committee. 78
newly insured often do not get the same quality of healthcare. Per the Personal Responsibility and Work sees 5 to 10 undocumented immigrants daily in each Illinois’ undocumented immigrants pay more than
care as those who have had long-term access, mostly Opportunity Reconciliation Act of 1996, immigrants of its urban hospitals, although the number could $560 million in state and local taxes annually but are typi-
because of their location, historic and continued lack face a five-year ban on Medicaid participation even be higher owing to challenges in identifying legal cally excluded from access to affordable, comprehensive
of resources, and limited knowledge about where to after naturalization.67 This means that no matter their status. Estimating an average of eight cases of unin- health insurance.79 Citing healthcare benefits to patients
receive the best care.66 legal status, many immigrants do not have access to sured patients per day, these undocumented immi- and fiscal benefits to Illinois taxpayers, the campaign aims
Authorized immigrants face many of the same the same quality of care as their native counterparts. grants account for a large share of the $65 million in to expand coverage options and promote better policy
making in the future.80
challenges as the undocumented when accessing
12 - MIDWEST DIAGNOSIS: IMMIGRATION REFORM AND THE HEALTHCARE SECTOR THE CHICAGO COUNCIL ON GLOBAL AFFAIRS - 13multifaceted challenge that policy alone cannot solve. Chicago’s St. Anthony Hospital has built trust within nonprofit, research, and teaching hospitals are exempt Medicaid. But the Healthy America Act of 2015, pro-
Those born outside the United States do not utilize its community by prioritizing the hiring of diverse from caps, for-profit providers must compete with posed by US Representative Luis Gutierrez (D-IL)
healthcare systems the same way as their native-born staff and making them visible in the neighborhood. other industries to secure limited numbers of visas, in September 2015, takes a small step in expanding
peers do, suggesting that cross-cultural competen- Community health promoters conduct workshops and which are dominated by global outsourcing compa- insurance access for individuals. The bill proposes
cy is an increasingly core part of providing effective, clinics at churches and other community organiza- nies.89 While the bipartisan Immigration Innovation that legal status not be considered in allowing access
quality care. tions, which in turn provide referrals to the hospital. (I-Squared) Act (S. 153), introduced in the Senate in to the healthcare exchange and that all state residents
It is good business practice for any healthcare The hospital has also expanded the ways it works with January 2015, would essentially double the number of should be insured under the ACA.95 The bill has not
provider to foster access to competent, quality care, the uninsured to pay for services, offering cash, credit, H-1B visas extended to those working in science, tech- moved past the introductory phase of the legislative
reducing the frequency and severity of healthcare and sliding scale payment options. The fiscal value of nology, engineering, and math, the legislation does not process because of proposed alterations to the IRS
visits. Healthcare systems that know how to provide this trust is not lost on hospital leaders, who are proud change the competitive lottery system.90 The bill has code and strong political opposition to expanded
superior care to diverse patients—often those that to be able to operate in the black while never turning not moved past its submission to the Committee on insurance coverage.96
prioritize the hiring of foreign-born healthcare pro- anyone away. But administrators recognize the lim- the Judiciary last January. Passing these various proposals would represent
fessionals and individuals who speak multiple lan- itations of expanding community programs under the Even with expansion, the caps on H-1B visas— a step forward in updating the federal immigration
guages—will have a competitive advantage in today’s current immigration system. According to a staff mem- in 2015, a record high number of 233,000 workers system, bringing it into sync with the current demands
global economy. ber, “without comprehensive immigration reform, we applied for just 65,000 visa slots—severely limit the on the Midwest healthcare sector. However, many of
Nearly 40 million people in the United States spoke can’t do this long term.”86 foreign-born professionals allowed to be trained and these stand-alone bills are currently stuck in Congress,
Spanish in 2011, making it the second-most-com- practice healthcare services in the Midwest.91 victims of a longtime political stalemate on immigra-
mon language in the country after English.81 Yet fewer No solutions in sight Unlike the I-Squared Act, the Conrad State 30 and tion that is not likely to be resolved until after the 2016
Physician Access Act (introduced in 2013 as S. 616 and election.97 Indeed, a legislative tracking website pre-
than 4 percent of healthcare providers are proficient Current federal immigration policy hinders the eco- reintroduced in 2015 as S. 1189) proposes an update to dicts that the I-Squared Act and Conrad 30 legislation
in Spanish, let alone other less-common languages.82 nomic development and stability of the Midwest’s the limited Conrad 30 program but does not include have a 1 percent and 0 percent chance, respectively, of
These linguistic barriers limit trust and engagement healthcare sector and also compromises the health provisions to expand the number of available slots. being enacted.98
with healthcare systems, forcing immigrants to and well-being of immigrant communities. Instead, the legislation would provide an EB-2 visa Yet even if piecemeal legislation were passed, larg-
look beyond healthcare providers—often to in-lan- Historically, the system did not interfere with (see Box 5) to a provider who agrees to serve in a med- er-scale, more-comprehensive reforms are still needed
guage television and radio—for health and wellness medical practices of foreign-born healthcare profes- ically underserved area or Veteran Affairs facility for to address the overall shortcomings of current immi-
information.83 sionals. Before 1977, US immigration policies allowed five years, three of which can be under the Conrad 30 gration policy for the Midwest and the entire coun-
Foreign-born healthcare professionals, whether the entry and permanent residence of foreign-born, program.92 Legislation would also make participating try. Even as current elected officials and presidential
trained in the United States or abroad, can conse- internationally trained doctors. However, in 1976, the physicians exempt from worldwide caps, which cause candidates have called for reform, US Speaker of the
quently be the bridge for language and trust gaps Health Professions Educational Assistance Act began long wait times for applicants from countries with high House Paul Ryan has maintained that his chamber will
within the system. Like Upwardly Global, the Welcome to subject international medical graduates to new cri- volumes of petitions, such as India and China. The bill not take up the broader issue of immigration reform
Back Initiative, and the Women’s Initiative for Self- teria and standards—credentialing requirements and is under consideration in the Senate but has not been until at least 2017.99
Empowerment, Chicago’s Bilingual Nurse Consortium temporary visas like the Conrad 30 program—that still deliberated on by a committee since May 2015 and is
is an example of a growing group of programs in the limit their entry and citizenship some 40 years later.87
region that assists underemployed immigrants, many The Resident Physician Shortage Reduction Act of
not yet slated for 2016.
Meeting healthcare labor needs in the
Introduced in June 2015, the Professional’s Access
of whom were healthcare professionals in their home 2015, introduced by US Representatives Joseph Crowly, to Health Workforce Integration Act (H.R. 2709) would
twenty-first century
countries, in re-credentialing in the United States and D-NY, and Charles Boustan Jr., R-LA, who is a medical support internationally trained healthcare profession- Immigration reform is urgently needed for a robust
finding sustainable employment. The program not doctor, aims to address some of the shortages created als in “entering into and advancing in” the American healthcare sector across the country and especially
only fills gaps in the Midwest labor sector but also by the 1976 law.88 The bill (H.R. 2124) proposes the healthcare workforce. The bill directs the Department in the Midwest. The following policy recommenda-
builds a linguistically and culturally skilled workforce.84 addition of 15,000 residency slots nationwide by 2019. of Health and Human Services, through the National tions, developed with feedback from regional hospital
Trust is another key factor in providing effective However, the likelihood of this legislation passing in Institute on Minority Health and Health Disparities, administrators, physicians, healthcare professionals,
healthcare. Through its community partners, Presence time to meet demand is slim given the current polit- to award grants to organizations that assist immi- and community leaders, should help shape those
Health has heard of undocumented immigrants being ical stalemate in Washington, and even if it passes, it grants with legal work authorization and international reforms. While some of the Midwest healthcare sector’s
afraid to engage with the healthcare system for fear does not address wider immigration policy challenges healthcare credentials by providing evaluation of stake in the current immigration debate is unique,
that hospital records could be shared with immigra- such as permanent residency and the future pipeline foreign credentials and access to English as a Second the recommendations outlined below would not only
tion authorities.85 Administrators have made efforts to of providers. Language courses.93 Since June 2015, the proposal meet the needs of the regional sector but also address
educate the community that hospitals are safe havens Another approach on Capitol Hill has been to revisit has sat in the Subcommittee on Health of the House labor shortages, visa issues, and other immigration-re-
for all, regardless of immigration status, but history H-1B visas, which allow employers to sponsor tempo- Energy and Commerce Committee.94 lated challenges to the healthcare systems across the
and lack of resources in the broader community have rary visas for healthcare professionals but are subject These legislative proposals do not address immi- country, helping keep the region and the nation more
made this messaging difficult for many hospitals. to competitive caps and a lottery (see box 5). While grants’ limited access to health insurance and globally competitive.
14 - MIDWEST DIAGNOSIS: IMMIGRATION REFORM AND THE HEALTHCARE SECTOR THE CHICAGO COUNCIL ON GLOBAL AFFAIRS - 15You can also read