Myelodysplastic Syndromes (MDS) - A Guide for Patients - Leukaemia Care
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
Myelodysplastic Syndromes (MDS) A Guide for Patients
Introduction
Being diagnosed with a myelodysplastic syndrome
(MDS) can be a shock, particularly when you may never
have heard of it. This booklet has been written to help
you understand more about MDS. It describes what the
various forms are, how they are diagnosed and treated
and also the expected outcome (prognosis). It will also
provide information on coping with the emotional impact
of an MDS diagnosis.
For more information, your Bowen, Honorary Professor of
haematologist or clinical nurse Myeloid Leukaemia Studies and
specialist will be able to provide Consultant Haematologist at St
advice that is specific to your James’s Institute of Oncology. The
diagnosis. booklet has also been reviewed
by patients and we are grateful
This booklet has been
to Chris Dugmore and Claudia
written by Dr Sally Killick,
Richards for their valuable
Consultant Haematologist; Dr
contribution.
Dominic Culligan, Consultant
Haematologist; Philip Alexander, Throughout this booklet you will
Counsellor and Cognitive see a number of quotations. These
Behaviour Psychotherapist; are the real experiences of MDS
Geke Ong and Janet Hayden, patients and will hopefully help
Clinical Nurse Specialists; and you to understand your situation
peer reviewed by Professor David a bit better.
If you would like any information on the sources
used for this booklet, please email
communications@leukaemiacare.org.uk
for a list of references.
Version 2
Printed: 11/2018
2 www.leukaemiacare.org.uk Review date: 10/2021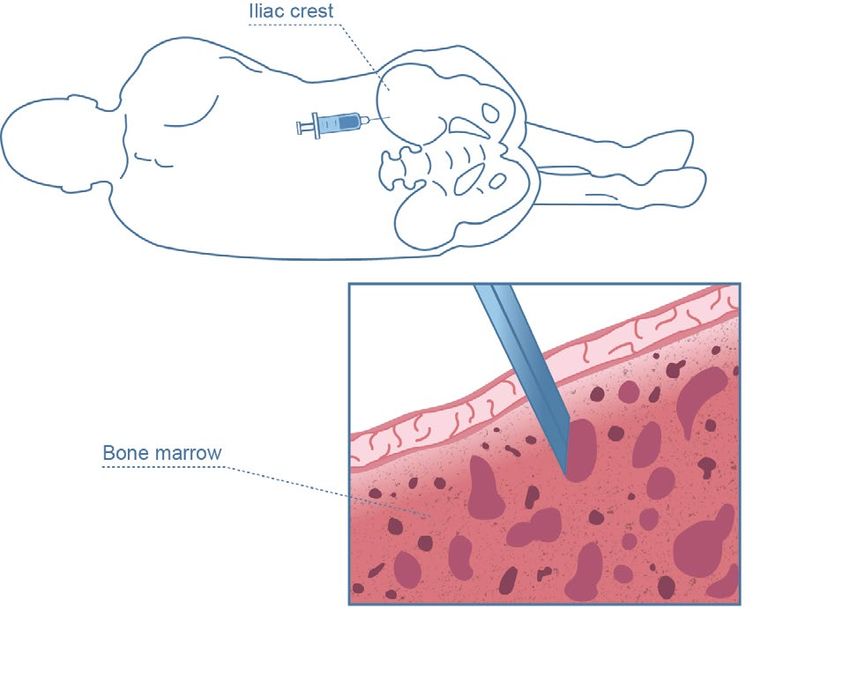
In this booklet
Introduction 2
In this booklet 3
Acknowledgements 4
About Leukaemia Care 6
MDS at a glance 10
Who gets MDS and why? 12
Signs and symptoms 13
Diagnosis 14
What are the types of MDS? 17
What is the prognosis of MDS? 19
Treatment of MDS 22
The psychological impact of MDS 33
Living with MDS 44
MDS specialist centres and 53
other useful organisations
Glossary 58
Appendix 60
Helpline freephone 08088 010 444 3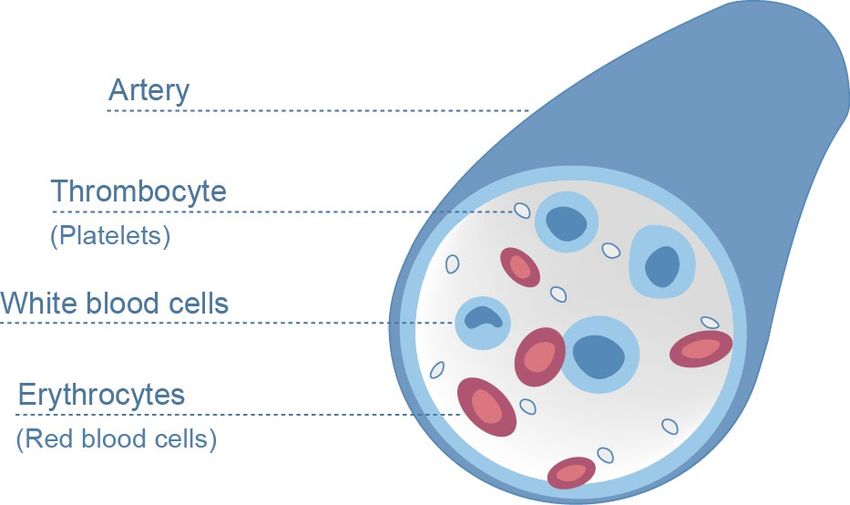
Acknowledgements
This booklet has been compiled assistance and advice to
by MDS UK Patient Support Group, patients and families affected
Leukaemia Care and Bloodwise by myelodysplastic syndromes.
in a joint collaboration. Although We offer a helpline, newsletter,
you are reading the version website, chat forum and meeting
supplied by Leukaemia Care, groups nationwide to facilitate
all of the wording is the same contact with other MDS patients
in each organisation’s booklet. and their families. Based at King’s
This booklet does not endorse College Hospital, MDS UK is the
any specific product or brand only national support group solely
– any names mentioned are for dedicated to MDS.
information only.
About Leukaemia Care
Acknowledgements and further
Leukaemia Care is dedicated to
thanks to The Irish Cancer Society
providing information, support
for their permission to use
and advice to blood cancer
information and images from
patients, their carers and loved
their MDS booklet.
ones.
This booklet has been endorsed
Whether they need a listening ear
by the Leukaemia & Lymphoma NI
from our Patient Advocacy team,
charity.
a buddy to chat to who has been
Leukaemia & Lymphoma NI funds in a similar position, a visit to
research into the causes and one of our support groups or good
cures of leukaemia, lymphoma quality, trusted information about
and myeloma in Northern Ireland. a diagnosis, treatment or side
effects, we are here for them all.
Contributing charities
About Bloodwise
About MDS UK
We’re the UK’s leading blood
MDS UK Patient Support cancer research charity. We fund
Group provides information, research to improve treatment
4 www.leukaemiacare.org.uk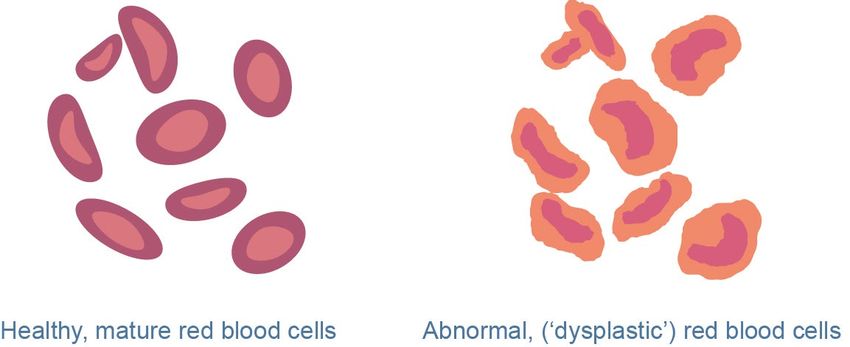
and care for people living with
all types of blood cancer, and
we provide anyone affected with
information and support.
Helpline freephone 08088 010 444 5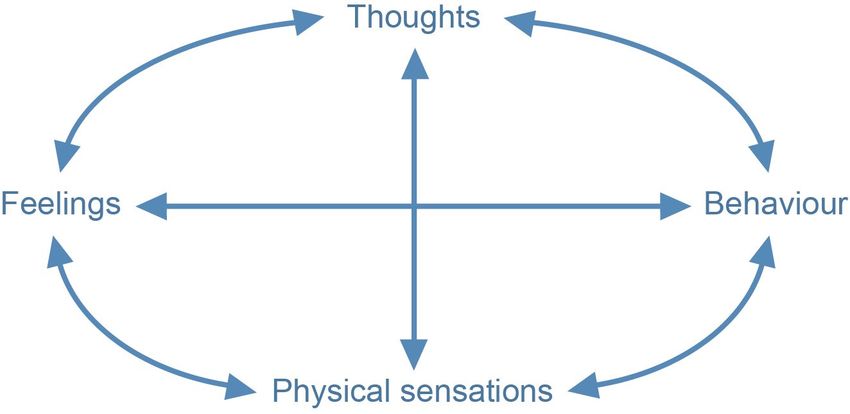
About Leukaemia Care
Leukaemia Care is a national charity dedicated to ensuring
that people affected by blood cancer have access to the
right information, advice and support.
Our services found on our website at www.
leukaemiacare.org.uk/support-
Helpline and-information/help-and-
Our helpline is available 9.00am - resources/information-booklets/
10.00pm on weekdays and
Support Groups
9.00am - 12.30pm on Saturdays.
If you need someone to talk to, Our nationwide support groups
call 08088 010 444 are a chance to meet and talk
to other people who are going
Nurse service through a similar experience.
We have two trained nurses on For more information about a
hand to answer your questions support group local to your area,
and offer advice and support, go to www.leukaemiacare.org.
whether it be through emailing uk/support-and-information/
nurse@leukaemiacare.org.uk, support-for-you/find-a-support-
over the phone on 08088 010 444 group/
or via LiveChat.
Buddy Support
Patient Information Booklets We offer one-to-one phone
We have a number of patient support with volunteers who have
information booklets like had blood cancer themselves
this available to anyone who or been affected by it in some
has been affected by a blood way. You can speak to someone
cancer. A full list of titles – both who knows what you are going
disease specific and general through. For more information
information titles – can be on how to get a buddy call
6 www.leukaemiacare.org.uk
08088 010 444 or email service, LiveChat (9am-5pm
support@leukaemiacare.org.uk weekdays).
Online Forum Campaigning and Advocacy
Our online forum, Leukaemia Care is involved in
www.healthunlocked.com/ campaigning for patient well-
leukaemia-care, is a place being, NHS funding and drug
for people to ask questions and treatment availability. If you
anonymously or to join in the would like an update on any of
discussion with other people in a the work we are currently doing or
similar situation. want to know how to get involved,
email advocacy@leukaemiacare.
Patient and carer conferences org.uk
Our nationwide conferences
provide an opportunity to Patient magazine
ask questions and listen to Our quarterly magazine
patient speakers and medical includes inspirational patient
professionals who can provide and carer stories as well as
valuable information and support. informative articles by medical
professionals. To subscribe go
Website to www.leukaemiacare.org.uk/
You can access up-to-date communication-preferences/
information on our website,
www.leukaemiacare.org.uk, as
well as speak to one of our care
advisers on our online support
Helpline freephone 08088 010 444 7
Your details:
Date of diagnosis
My diagnosis/type of
MDS
Cytogenic results
Date Details and Good, normal or poor
chromosome affected
8 www.leukaemiacare.org.ukName Contact details
Consultant
haematologist
Specialist nurse
GP
Haematology day care
unit
Haematology inpatient
ward
Emergency contact
number
Helpline freephone 08088 010 444 9Myelodysplastic syndromes at
a glance
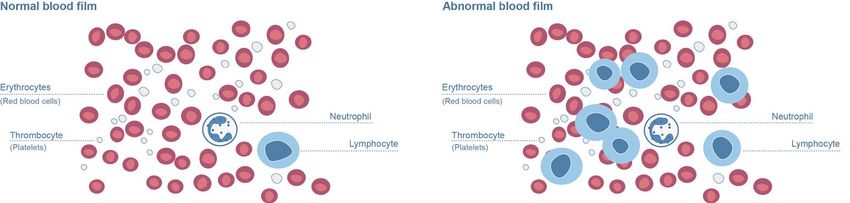
What are This results in the number of
blood cells in the bloodstream
myelodysplastic being reduced. This is referred to
syndromes? as a ‘cytopenia’. Some patients
The myelodysplastic syndromes, have just one type of blood cell
or MDS for short, are a group of that is low (such as red blood
diseases in which the production cells), however, sometimes MDS
of blood cells by the bone marrow can cause a reduction in all the
is faulty. It is a type of cancer and types of blood cells. When this
sometimes may be referred to as occurs, it is called ‘pancytopenia’.
bone marrow failure. The bone
marrow is located inside some of Can MDS lead to any
your bones and it is the factory other conditions?
where blood cells are made. It is In addition to low blood counts,
here where the problem lies. the myelodysplastic syndromes
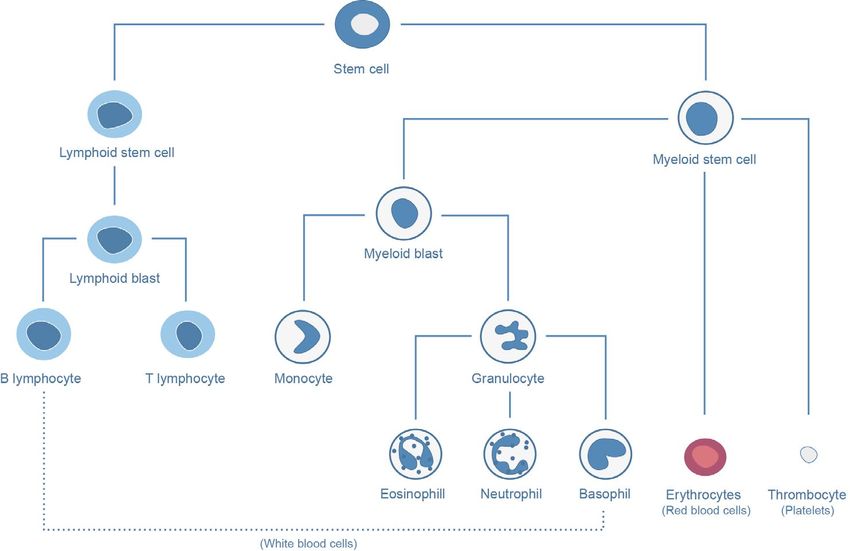
The bone marrow makes three share a common tendency to
main types of blood cells: develop into acute myeloid
leukaemia (AML) over time. In
1. Red blood cells that carry MDS, the bone marrow has a
oxygen around the body number of immature abnormal
cells called blasts. In some
2. White blood cells that fight
patients with MDS the number
infections
of blasts increases with time.
3. Platelets that prevent bleeding Leukaemia (AML) is defined as
having more than 20% blast cells.
What causes MDS?
The risk of AML occurring depends
In MDS, the bone marrow is on the type of MDS, but some
usually more active than normal, patients may never progress to
yet the blood cells it produces AML.
are not healthy (we refer to that
as ‘dysplastic’); do not work as You can find out more about
well as they should and many AML in factsheets and booklets
die either before they reach the available from Bloodwise and
bloodstream or shortly afterwards. Leukaemia Care.
10 www.leukaemiacare.org.ukIs MDS a cancer?
You do not need to
MDS is a form of bone marrow
learn everything about
cancer, although its progression
into leukaemia does not always MDS at once. You can
occur. It is included in the World keep this booklet and
Health Organisation Classification refer back to it, reading
of Haematopoietic (blood and different sections as
bone marrow) Tumours.
and when you’re ready.
Helpline freephone 08088 010 444 11Who gets MDS and why?
MDS is a rare disease. It may be previous chemotherapy or
diagnosed at any age but it is very radiotherapy.
rare in children and young adults.
This booklet deals with MDS ••Inherited disorders – very
rarely, MDS can be inherited or
occurring in adults.
may develop from another rare
The typical age for patients to blood disorder. For this reason,
develop MDS is around 75 years young patients may be tested
old. About 9 out of 10 patients for any diseases that are linked
are over 50 years at the time to MDS. However, for the vast
of diagnosis. Men are slightly majority of patients, MDS will
more likely than women to be not be passed down to children
diagnosed with MDS. and is not an inherited genetic
disease.
The cause of MDS remains largely
unknown, although there are ••Environmental factors –
many research groups around the exposure to toxic chemicals
world who are trying to improve such as benzene may
our understanding of why it marginally increase the risk of
occurs and in whom. There are MDS, but such exposure is now
certain factors that may increase uncommon.
your chance of developing MDS
and these include:
MDS is not an
••Previous chemotherapy with infectious disease and
or without radiotherapy – this it cannot be passed on
treatment may have been given
to other people.
in the past (usually for other
cancers). It is thought that the
treatment damages the bone
marrow and may cause MDS
in some patients. This is called
secondary or therapy-related
MDS, as it is secondary to the
12 www.leukaemiacare.org.ukSigns and symptoms
What are the signs and manifest itself as a rash on your
skin. These are tiny bleedings
symptoms of MDS? under the skin called petechiae
Symptoms vary from person to and often appear where clothes
person and depend on which are tight fitting like around the
blood cells have become reduced ankles or waist. Nose or gum
in your bloodstream. About 8 in bleeds can also be a sign of a low
10 patients have anaemia, whilst platelet count.
about 2 in 10 present to their
doctor with infections or bleeding. Recurrent and persistent
infections are another common
Anaemia is due to a lack of red symptom of MDS due to low white
blood cells (also referred to as low blood cell counts.
haemoglobin), which may lead to
fatigue and shortness of breath, Some MDS patients have no signs
even on light exertion. or symptoms and are diagnosed
by chance as a result of a routine
"When I was diagnosed I was blood test.
surprised; I had not heard of MDS
before. But I also felt relieved; a
reason why I was so fatigued." Anaemia is the most
commonly experienced
When your platelet count is low,
you can suffer from easy bruising
symptom in MDS.
and bleeding. This can sometimes
Helpline freephone 08088 010 444 13Diagnosis
How are the condition or monitor response to
treatment.
myelodysplastic
syndromes diagnosed? What does a bone marrow test
involve?
Full blood count
This is usually performed as an
Low blood counts are picked
outpatient, meaning you don’t
up by a simple test called a full
need to stay in hospital overnight
blood count (FBC). The laboratory
and can go home after the
performing the test will then
procedure. A small liquid bone
examine the blood cells on a slide
marrow sample is taken followed
(called a blood film) under the
by a biopsy, generally from the
microscope. If you are found to
pelvis. The doctor will numb the
have changes on the blood film
area with local anaesthetic and
that suggest MDS, you will usually
insert a needle into the bone
be referred to a blood specialist
marrow cavity in order to take the
(haematologist). It is important
sample. The procedure usually
to rule out other causes of a low
takes around 20-30 minutes, but
blood count so the doctor will ask
you should allow an hour of your
general health questions and give
time. It may be uncomfortable at
you a physical examination.
the time, or later that evening, but
Bone marrow test simple paracetamol is usually
enough to relieve the pain. You
As MDS is a disease of the bone may be asked to lie on your back
marrow, a bone marrow test is after the procedure for 10 minutes
usually needed to diagnose the to reduce the risk of bleeding.
14 www.leukaemiacare.org.ukA small dressing or plaster is changes in the structure of
applied to the site. the chromosomes in the
affected cells. In addition, there
"I remember very little from when I
is a general move towards
was diagnosed as I was terrified and
molecular testing (to look for
in shock."
DNA mutations), which we hope
will lead to more precision
How long do I have to and therefore make care more
wait for the results? personalised. However, at the
Preparing the sample and moment we are still learning what
analysing all the results can take the molecular changes may mean
two to three weeks. The bone for MDS patients.
marrow sample is examined by
If the bone marrow changes are
a doctor under a microscope
not clear and there is doubt about
to look for changes seen in
whether or not you have MDS, your
MDS. Additional tests are often
doctor may decide to monitor your
requested on the bone marrow
blood counts and repeat the bone
sample, which may help to
marrow test at a later stage.
make the diagnosis and provide
information about how the A bone marrow sample may not
disease will behave (prognosis). be necessary in some cases, for
example if the results are unlikely
These tests include cytogenetics
to affect treatment decisions for
(sometimes called a ‘karyotype’),
the person.
which is the study of the
Helpline freephone 08088 010 444 15Diagnosis (cont.)
You can find details of all the
different support organisations
Waiting for your test in Chapter 10: MDS specialist
results may be an centres and other useful
anxious time. Talk to organisations.
your family and friends
or contact patient
support organisations
which can assist in
different ways. They
can help put you
in touch with other
patients over the
phone, in person or
through online forums.
You can read about the
experiences of other people who
are going through or have been
through something similar on
the websites of patient support
organisations. It is important at
an early stage to get support and
information from recommended
and reputable sources, as the
internet can present misleading
and unvetted information.
"There is a lot of confusing and scary
literature around, so talk with real
people about it; it’s really helpful."
16 www.leukaemiacare.org.ukWhat are the types of MDS?
Your doctor will describe the type included in the current 2016
of MDS that you have, as each classification. These are:
type can behave differently. The
World Health Organization (WHO)
1. MDS with single lineage
dysplasia (MDS-SLD)
has developed a regularly updated
classification for separating the 2. MDS with multilineage
different types of MDS. This was dysplasia (MDS-MLD)
updated in 2016, and replaces
the older classification of MDS in 3. MDS with ring sideroblasts
2008. Both classifications may (MDS-RS)
still be referred to and therefore 4. MDS with excess blasts (MDS-
the old classification can be seen EB); MDS-EB-1 and MDS-EB-2
as an Appendix at the end of the
booklet. This system is based on 5. MDS, unclassifiable (MDS-U)
the blood results, the appearance
of the bone marrow, the number
6. MDS with isolated del(5q) or
with 1 additional abnormality
of abnormal immature blast cells
and any chromosome changes Please note: Information on
found. The immature cells are CMML (chronic myelomonocytic
called blasts, which may be leukaemia) is available as a
increased in some of the types of separate booklet, as it now
MDS. falls under the WHO 2016
category of ‘Myelodysplastic/
There are six broad types of MDS
Myeloproliferative neoplasms’.
Helpline freephone 08088 010 444 17What are the types of MDS?
(cont.)
is missing.
There are many types What does high risk
of MDS and this can be and low risk MDS
difficult to understand. mean?
Spend time talking to It is often easier to consider
your doctor or nurse whether the type of MDS you have
so you understand falls into what is called a LOW
how your MDS will be risk group or a HIGH risk group.
treated. It’s important The ‘risk’ refers to your chance
of developing acute myeloid
that you know and leukaemia (AML) and your life
understand your exact expectancy (survival). In the low
diagnosis. You could risk disease group a patient
ask your treatment has about a 1 in 10 chance of
team to write it in the progressing to AML. The low risk
group includes MDS-SLD, MDS-
front of this booklet, MLD, MDS-RS, MDS-U and MDS
so that you have it to with del(5q) either in isolation or
hand. with 1 additional abnormality. In
contrast, the risk of developing
leukaemia is greater in the high
The terminology used can be
risk disease group (MDS-EB). The
difficult to understand, so ask
separation into these groups is
your doctor to explain which
important as the treatment of
type of MDS you have. Dysplasia
patients with low risk and high
means that the bone marrow cells
risk disease can differ. Your doctor
are abnormal in their appearance.
may use the WHO classification
Sideroblasts are young red blood
to decide whether your disease
cells that have a very distinctive
is low or high risk; although
ring of iron granules seen under
it is usually better to use the
the microscope. MDS with isolated
prognosis score discussed next.
del(5q) means the chromosome
tests show part of chromosome 5
18 www.leukaemiacare.org.ukWhat is the prognosis of MDS?
Prognosis refers to the expected time your MDS is diagnosed
outcome or survival from MDS
and is therefore different from •• The number of abnormal
immature cells (blasts) in your
classification. Your prognosis
bone marrow at diagnosis
can depend on many factors,
including those not related •• The chromosome test results
to MDS, such as your general from your bone marrow at
fitness and age. However, to diagnosis
allow your doctor to make the
right treatment decisions, MDS The calculator adds together the
doctors and scientists around individual scores to give a final
the world have designed a score, which puts you into one of
number of scoring systems to the following IPSS-R risk groups:
help predict how your MDS is
likely to behave. Over time, these
•• Very low
scoring systems have evolved to •• Low
give more accurate estimations.
The most commonly used •• Intermediate
scoring system is the revised •• High
International Prognostic Scoring
System (IPSS-R). This replaces the •• Very high
previous IPSS. The risk groups describe the
expected risk of developing acute
Can you explain the myeloid leukaemia (AML) and
scoring systems in expected survival. This helps your
more detail? doctor to identify and discuss
The British Society of with you the best treatment
Haematology MDS Guidelines choices for you as an individual.
recommend using the IPSS-R as a For more information about
scoring system (see appendix). the risk and survival predicted
in each group, see page 62
The IPSS-R score is calculated [appendix]. It is important to
from: understand that the expected
outcomes for each group give an
•• Your blood count results at the
Helpline freephone 08088 010 444 19What is the prognosis of MDS?
(cont.)
an indication of what may happen UK MDS Forum and
in that group of patients as a
collective. This gives a useful
British Society of
framework for a discussion about Haematology (BSH)
the future and the options for MDS Guidelines
treatment, but it is not possible
A group of expert haematologists,
to give a precise outcome figure
with a specialist interest in MDS,
for an individual patient. As our
has prepared guidelines for the
understanding of the molecular
diagnosis and therapy of adult
changes seen in MDS increases,
myelodysplastic syndromes.
this may allow us to more
These are updated periodically
accurately work out an individual
to reflect changes in medical
patient’s outcome and guide
practice. The content of the
treatment further.
treatment section of this booklet
Doctors sometimes refer to ‘low is based on the BSH guidelines,
risk’ and ‘high risk’ MDS. If doctors the full version of which can be
are using the older IPSS, ‘low found online at www.b-s-h.org.
risk’ refers to patients with Low uk/guidelines
and Intermediate-1 categories,
It is important to understand that
whilst ‘high risk’ refers to
although guidelines represent
patients with IPSS Intermediate-2
the collected opinions of a group
and High categories. The risk
of experts based on best clinical
designation is more difficult
practice from available evidence,
with the more recent IPSS-R,
they are only guidelines. In most
‘low risk’ certainly including
cases, a patient’s treatment will
Very Low and Low categories and
be based on these but a doctor
‘high risk’ including High and
may decide that it is not in
Very High categories. As yet, the
the best interests of a specific
risk designation for the IPSS-R
patient to be treated exactly, or
Intermediate group has not been
even broadly, according to the
confirmed.
guidelines. If this is the case for
you, then your doctor will discuss
20 www.leukaemiacare.org.ukthe reasons for this.
The UK MDS Forum is an expert
organisation open to those
healthcare workers and scientists
with an interest in MDS. The
aim of the forum is to increase
the awareness of MDS through
education and increase access
to clinical trials for patients with
MDS across the UK.
Helpline freephone 08088 010 444 21Treatment of MDS
How is MDS treated? The MDT meetings
The way that MDS behaves varies involve doctors, nurses
from person to person, and and other healthcare
depends on the type of MDS that professionals putting
you have. The types of MDS have
been described in detail earlier in
their heads together
this booklet. Treatment is based and deciding the best
on British Guidelines agreed by treatment specifically
MDS specialists, and your care for you.
will be discussed in your local
multidisciplinary team (MDT)
meeting. Treatment planning
Once the diagnosis of MDS has
What is an MDT? been made, you and your doctors
Your diagnosis and treatment will decide on the best treatment
will be discussed and reviewed for you. The treatment that you are
by a team of clinical specialists offered will depend on the type of
including haematologists in your MDS you have, your own wishes,
local area. They are called your your age, your general wellbeing
multidisciplinary team (MDT). or fitness and the IPSS-R score,
They hold regular meetings or in some cases the IPSS score
which allow your case to be (see earlier section). Before your
discussed by many doctors and treatment starts, your doctor or
healthcare professionals in the nurse will explain the benefits
Haematology clinical team. It and side effects of the chosen
may also be necessary to ask for treatment so that you can give
an opinion outside of this group your consent. It is likely that you
to help either with the diagnosis will need to sign a consent form to
or to discuss the best form of agree to the treatment. If you are
treatment. unsure about anything, do ask,
as MDS is a complicated disease
to understand. The BSH MDS
guidelines recommend that all
patients who are newly diagnosed
with MDS are discussed with a
22 www.leukaemiacare.org.ukregional or national expert in MDS so it can grow new healthy blood
given that the disease is rare. You cells in the bone marrow
are entitled to ask your doctor if
Unfortunately, most patients’
they have done this. The NHS also
MDS cannot be cured but MDS
allows you to ask to see a regional
can usually be controlled and
or national expert in MDS if you
often improved.
think that this would help you.
The first question that your
Not all patients need active
doctor will ask themselves is
treatment, as some do not have
whether there is a treatment
any symptoms. If you are not
option that has a chance of curing
starting treatment, you will have
the MDS. The only treatments
regular check-ups which is often
that can possibly cure MDS
referred to as ‘watch and wait’ or
are either a stem cell or bone
‘active monitoring’.
marrow transplant from another
"The challenge is predominantly person or, very rarely, intensive
mental since it’s very hard to accept chemotherapy.
that I have cancer but that it isn’t
If a stem cell transplant is
being treated."
an option for you, you will be
Broadly speaking, treatment of identified early so that a search
MDS will include one or more of for donors can be started and a
the following: transplant considered at an early
stage.
••Supportive care – this aims to
control the symptoms of MDS What is a clinical trial?
••Non-intensive treatment – this Research into MDS continues
treatment tries to slow down worldwide to improve our
the progression of MDS and knowledge of why MDS occurs,
improve your blood counts how individual types of MDS
behave and how best to treat the
••Intensive chemotherapy – this condition. Today we benefit from
involves giving high doses of
the thousands of patients who
chemotherapy in hospital
have been part of clinical trials
••Stem cell transplant – this and research studies in the past.
gives your body new stem cells The words ‘research’, ‘trial’ or ‘new
Helpline freephone 08088 010 444 23Treatment of MDS (cont.)
drug’ sometimes scare people, but your research team if you have
rest assured, patients receiving any questions.
new drugs in a trial are monitored
very closely for side effects. Your Supportive care
doctor may discuss with you a All patients will need supportive
clinical trial available at your care at some stage, either alone
hospital; however, you cannot be or to support other treatments
entered into a trial without your being given. Supportive care is
permission. The trial needs to be not directed at the underlying
fully explained to you, and you disease but rather at controlling
need to have time to think about the symptoms and complications
the treatment before deciding. caused by the disease. The nature
This is called ‘informed consent’. and extent of supportive care
If you agree to be treated in a needed depends on which blood
clinical trial, you can still change cells are affected and exactly
your mind at any point and come how low the blood levels fall.
out of the trial. If you decide not to Most patients will need blood
go into a clinical trial, you will be transfusions at some stage.
given the best-proven treatment
available. Please ask if there are Treating anaemia
any clinical trials suitable for you Most patients (but not all)
available in your hospital or at diagnosed with MDS are anaemic.
your nearest specialist centre. This can cause symptoms such
as tiredness and shortness of
When you have a bone marrow
breath, affecting your quality
test to diagnose MDS or monitor
of life. Some patients continue
how well treatment is working,
having a normal or reasonable
your doctor may ask your
quality of life despite anaemia
permission to store some of your
and so will not necessarily need
blood or bone marrow for future
treatment for the anaemia at that
research into the biology of MDS
stage. Other patients will need
(what causes MDS). There will be
blood transfusions to improve
an information sheet for you to
the symptoms caused by the
read and you will then be asked
anaemia. The haemoglobin (Hb)
to give your informed consent for
level in your blood results will
this research. Remember to ask
show your level of anaemia.
24 www.leukaemiacare.org.ukGrowth factors Blood transfusions
Blood cell numbers can Blood transfusions are a very
sometimes be increased by important part of your care. They
the use of growth factors. will be considered if you have
Growth factors are like natural symptoms from anaemia. There
‘hormones’ that stimulate our is no set haemoglobin level at
blood production. We all make which a blood transfusion is
these growth factors every day. given, but your doctor will assess
For example, erythropoietin your symptoms and you will
(sometimes known as ‘EPO’) is a decide together. The frequency
growth factor that increases red of transfusions will vary between
blood cell numbers. Granulocyte- patients; some need transfusions
colony stimulating factor (or every few months whilst others
‘G-CSF’) increases white blood need one every couple of weeks.
cell numbers. Not all patients Usually, once you have started
are suitable for this treatment, having regular blood transfusions,
and only some MDS patients will the length of time between
respond. Your doctor can advise transfusions will gradually get
you on your suitability for growth shorter. If you find that your
factors. EPO is considered a safe symptoms of anaemia come back
treatment in MDS. well before your next transfusion
is due, contact your Haematology
Growth factors are given as an
team and discuss whether the
injection under the skin. The
interval between transfusions
number of injections needed
should be shorter, or the number
will vary from patient to patient.
of units of blood increased. This
A district nurse can give the
varies between patients. An
injections, or you (or a family
improvement in your symptoms
member) can learn how to give
after having a transfusion may
the injections yourself. The skin
not be immediate, sometimes
around the injection site may
it can take a few days to start
become irritated, so it is best to
feeling the benefit.
regularly change the injection
site. Do talk to your nurse(s) about
this and also the common side
effects that you may expect.
Helpline freephone 08088 010 444 25Treatment of MDS (cont.)
you are offered iron chelation
It is important that therapy or not will depend on the
you are transfused likely benefits versus the likely
adequately to control disadvantages in your individual
your symptoms as it case. This will be discussed with
you before you make a decision
will help your quality to start iron chelation. It is
of life. Discuss this important that you do not reduce
with your haematology the number of blood transfusions
team.” you receive due to the concern
about your iron levels, as this
may not adequately control your
symptoms.
With every unit of blood you
receive from a transfusion, you Desferal (deferoxamine) is a
will receive an excess amount of drug used to treat the build-up
iron. Over time this can build up in of excess iron and is given as
your body and may possibly cause a continuous subcutaneous
damage to certain organs, like injection under your skin by a
your heart or liver. Because blood pump. There are special teams
transfusions are rich in iron, it is that can teach you how to
important that you do not take administer the drug at home.
additional iron tablets unless your Exjade is another iron chelator
doctor prescribes them. There is and comes in tablet form.
still uncertainty about whether However, in most cases this is
too much iron in your body is only available for patients who
always harmful. The level of iron in cannot tolerate subcutaneous
the body will be regularly checked Desferal, who have serious side
if you are on regular transfusions effects on Desferal or where it
and treatment will be considered is thought not to be working
if there is a build-up of excess adequately. Both treatments can
iron. This treatment is called iron have certain side effects and
chelation; however, there remains often need to be continued for a
uncertainty about the benefits long period of time to be effective.
of removing iron. Whether Your doctor can discuss this with
26 www.leukaemiacare.org.ukyou. Don’t hesitate to discuss your infection, are on blood thinners
iron levels with your doctor at any or have suffered from bleeding,
time during your treatment. you might benefit from platelet
transfusions to keep your platelet
"Having a blood transfusion is an
count at a higher level. Your doctor
amazing feeling. People around me
or nurse will inform you when this
could see the colour returning to
is necessary.
my face. I had a shower and danced
because at last it no longer hurt to Antibiotics
stand and wash my hair. The relief
It is important for you to
was immediate."
understand that patients with
Platelet transfusions MDS have a higher risk of
developing infections. Antibiotics
About half of MDS patients will
are not usually given to prevent
have a reduced platelet count
infections, as they cause side
at diagnosis (this is called
effects and may cause the
thrombocytopenia). The platelets
bacteria to become resistant. But
may also function poorly and this
if you do get an infection, this
means that bruising and bleeding
should be treated quickly with
can sometimes be a serious
antibiotics, and you may need
problem in MDS. If you have a
to be admitted into hospital so
low platelet count, it is usually
that the antibiotics can be given
advisable to avoid blood-thinning
through a vein (intravenously).
agents and non-steroidal anti-
Most specialist units will have
inflammatory drugs. However, this
a direct phone number to call
should be discussed with your
for advice in the event of a fever
doctor as there are exceptions
occurring.
where the benefit you will receive
from these drugs outweighs the
risks.
Platelets can be transfused but
because they only last about four
days, they are not routinely given
even when the platelet count
is very low. But if you have an
Helpline freephone 08088 010 444 27Treatment of MDS (cont.)
progression of the disease. It
If you are feeling may be considered if your blood
unwell, check your counts are quite low or falling, or
if there are signs that the disease
temperature. If it
is developing into leukaemia. The
is raised, or you idea is to treat the disease with
experience shivers, as few side effects as possible,
contact your specialist thereby maintaining a good
nurses at the hospital quality of life. These treatments
will not cure your MDS but may
or call the helpline
‘modify’ the disease. These
number you have been treatments are usually given as
given. an outpatient.
Hypomethylating agents (HMA)
Treatment extending beyond
supportive care can be classed Hypomethylating agents work
as low-intensity, high-intensity on the behaviour of cancer
or high-intensity with a stem cell cells at the DNA level and can
transplant. turn genes on and off. Drugs
such as azacitidine work to
improve bone marrow function
Fact sheets for all and slow the progression to
treatments are leukaemia. They are currently
available. Please ask used in high risk MDS patients
your nurse specialist (IPSS Intermediate-2 and High
categories) who are not fit
for the correct patient enough for a stem cell transplant.
information sheet Azacitidine is usually given as
to help you fully an injection under the skin. Side
understand your effects can include:
treatment. •• Mild nausea
•• Diarrhoea or constipation
Non-intensive
treatment •• Skin irritation at the injection
site
Low-intensity or non-intensive
treatment aims to slow the •• Becoming more prone to
28 www.leukaemiacare.org.ukinfections (due to lowered blood In a small number of patients with
counts) MDS, the number of bone marrow
cells is unusually low (termed
Lenalidomide hypoplastic). This is similar to
If you have a certain type of a blood disease called aplastic
MDS which has deletion of part anaemia. Patients can sometimes
of chromosome 5 (this may respond to drugs targeted at
be referred to as the 5q minus suppressing the immune system,
syndrome or del 5q), you may be such as anti-thymocyte globulin
offered lenalidomide if you are (ATG) or ciclosporin.
anaemic. This is taken orally as
a capsule and works in several Intensive
ways to suppress the MDS cells, chemotherapy
including altering the immune
If you have high risk MDS, you
system. Therefore, it is often
may benefit from intensive
referred to as a type of immune
chemotherapy. It is the same
modulation therapy. On starting
treatment that is used to treat
the treatment, your blood counts
acute myeloid leukaemia
fall before a response is seen.
and aims to kill a significant
During this early stage, you may
proportion of the diseased cells
need transfusions of blood and/
from your bone marrow to allow
or platelets. Some patients also
the bone marrow to work normally
need G-CSF. Other side effects can
again (remission). The treatment
include:
has a high number of side effects
•• Rashes so you need to stay in hospital for
four to six weeks for each course.
•• Fatigue
A small proportion of people
•• Diarrhoea may be cured by intensive
•• A small increased risk of blood chemotherapy alone, although
clots usually when a donor is available,
a stem cell transplant will follow.
As lenalidomide can cause birth Achieving remission, even if not a
defects, you must avoid getting cure for the disease, can improve
pregnant whilst taking the drug. your quality of life (often almost
to normal quality) as long as the
Immunosuppressive therapy remission lasts.
Helpline freephone 08088 010 444 29Treatment of MDS (cont.)
How is intensive chemotherapy •• Infections
given?
•• Bleeding
Most chemotherapy is given
as an infusion into a vein •• Anaemia
(intravenously), but sometimes Other side effects can include:
as a tablet. It is given as a course
or cycle of treatment, whereby a •• Hair loss
combination of chemotherapy
is given over a number of days
•• Nausea
followed by a rest period. It is •• Vomiting
often easier for you to have a
Hickman line inserted, which •• Sore mouth
allows all the drugs to be given •• Diarrhoea
and blood tests to be taken. This
is a line that is carefully inserted •• Loss of appetite and taste
into a large vein and can stay
in place for the duration of your
•• Skin and nail changes
treatment. •• Infertility
What are the most common Allogeneic stem cell
side effects from intensive transplant
chemotherapy?
A stem cell transplant, also
The chemotherapy used in MDS referred to as a bone marrow
is specially designed to kill the transplant, offers the chance of
cancer cells in the bone marrow, curing the disease.
so your blood counts will fall
after the chemotherapy and In an allogeneic transplant,
remain low for a number of weeks. healthy bone marrow or stem cells
Healthy bone marrow cells are are taken from another person
also ‘stunned’ in a type of ‘friendly whose tissue DNA is identical or
fire’ but can recover better than almost identical to yours. This
the MDS cells if remission is means the donor is compatible
achieved. During this time there with you. The bone marrow or
can be serious, sometimes life- stem cells are taken from a donor
threatening side effects, the most – either a family member (usually
common of which are: a sibling) or an unrelated donor.
30 www.leukaemiacare.org.ukThe donor has a simple blood of this treatment to you as an
test to see if they are matched to individual. Always try to take a
you – they do not need to have a family member or friend to the
bone marrow test. The results are appointments.
usually available in two to three
weeks. You can find out
As medical knowledge and more about stem
experience has progressed, more cell transplants in
patients can now be considered several booklets: ‘The
for a transplant. Reducing the
intensity of the conditioning
Seven Steps’ booklets,
treatment done before the available from
transplant also means the side Bloodwise and Anthony
effects from the transplant itself Nolan, or those from
are less severe. This approach Leukaemia Care.
is called a reduced intensity
conditioning (RIC) transplant.
About one third of patients who Follow-up
receive this treatment are free of Once MDS has been diagnosed,
disease over many years but the your specialist will discuss
disease may return (relapse). treatment options and follow-up.
This treatment has many side For some patients, this will only
effects and it is important mean infrequent outpatient visits
that the decision to have an to check if the disease is showing
allogeneic stem cell transplant signs of progressing. Sometimes
is carefully thought through these check-ups can be shared
by your healthcare team and with the GP. For those patients
yourself. It is also important where the disease is thought to
to know that the side effects be high risk or for those who have
from a stem cell transplant can received active treatment, the
continue for a number of years outpatient visits may be more
after the transplant. If you are frequent. This will be individually
suitable for a transplant, you will tailored to you.
be referred to a specialist centre
to discuss the benefits and risks
Helpline freephone 08088 010 444 31The psychological impact of
MDS
This chapter is about the these emotional ups and downs is
emotional impact of having MDS, adjustment.
which can be as significant as the
"The diagnosis hit me like a ton
physical impact of the illness. It
of bricks. My emotions were on a
is important to emphasise that
rollercoaster."
each person with MDS will cope
in their own unique way, and your Adjustment is something every
healthcare team are experienced person will experience as they go
at considering your emotional through significant life events like
needs, as well as your physical divorce, bereavement or illness.
needs. It involves changes and losses
of varying kinds and includes
A Holistic Needs Assessment or
both practical and mental
Quality of Life questionnaire or
adjustments. In the case of an
assessment can often help to
illness these include:
identify certain problems, or help
discuss them with staff. •• Getting used to being monitored
Not everything in this chapter will •• Having medical appointments
apply to you, but there are some and treatments
common thoughts and feelings
that you could be familiar with – •• Potential loss of – or reduction
and, to some extent, your relatives in – some physical capabilities
and carers too. which, in turn, could affect
things like employment, or
Adjustment personal roles and relationships
People living with MDS •• Disruption to one’s usual life
sometimes experience a range patterns and routines
of complex thoughts and intense
feelings as they try to cope with •• Questioning things normally
the diagnosis, monitoring or taken for granted, like good
treatment. This is often described health and future plans –
as ‘being on an emotional perhaps making people more
rollercoaster’. The formal term for worried about things than usual
32 www.leukaemiacare.org.ukGiven the losses and changes issues.
involved – which to some can
"The emotions that went through my
feel frightening – and the need to
body cannot be explained – there
adapt to and cope with something
was anger, worry, fear and sadness.
new, adjustment can be both
But the overwhelming one was
stressful and distressing. The
determination that we would get
good news is, while the emotional
through this."
ups and downs of adjustment
aren’t always easy, with time most
people do adapt well to their new
Coming to terms with
situation. your diagnosis
Although everyone is different,
What feelings might generally it is helpful to ‘process’
you experience and your thoughts and feelings, rather
how can you help than ignore them. This means
thinking about your diagnosis,
yourself? including what it means to you
This section describes many and how you might cope. It means
of the common emotions (and being aware of your feelings and
related thoughts) that people with being able to express them when
MDS might experience. Following you want to. It can be helpful to
each description are some talk about your situation with
suggested coping strategies. other people, both professionals
These are drawn from evidence- and those in your personal life.
based psychological practices, as Writing thoughts and feelings
well as feedback from patients down can help you to process
about what has helped them. It them too. It is useful to strike a
is important to remember that balance between thinking and
not everyone will experience all talking about your situation,
of these feelings, but it is equally and having periods in which you
important to emphasise that if focus on other, meaningful and
you have some – or all – of them, enjoyable things instead.
you are not alone and it is not a
sign of weakness or mental health "It’s so important to stay positive,
Helpline freephone 08088 010 444 33share what’s going through your mind to change negative thoughts and
and know that you’re not alone." thinking patterns. In short, the
way we think affects the way we
There is a link between feel.
thoughts, feelings,
physical sensations Managing thoughts
and behaviour Writing negative thoughts and
worries down can be helpful.
Before we move on, it is useful You will notice that some of
to explain that within every type them are ‘valid’ (this means
of mood there are four elements: understandable and acceptable)
thoughts, feelings, physical given your situation, but some
sensations and behaviours of them are ‘catastrophic’
(the actions we take, or don’t (meaning they predict the worst
take, to cope). Also, each of case scenario) or are very ‘black
these elements interacts with and white’ (meaning things are
and affects the other, as in this all good or all bad). Here are
diagram (above). some examples: "because of
It is hard to directly ‘access’ and this illness, my life’s ruined"; "I
change an emotion, whereas know the treatment won’t work";
thoughts and behaviours and, "nothing ever goes right for me";
to some extent, physical states, "everything’s awful"; "there’s no
are more easily changed. This hope"; "I must be a bad person".
can help to improve emotional Take a step back and ask yourself
feelings. It is particularly effective whether those thoughts are facts
or opinions. Say to yourself "is
34 www.leukaemiacare.org.ukthere another way of looking at even a little exercise, moderating
this?", or "is that actually what my alcohol consumption, and
medical team said to me?" Write connecting with other people will
down alternative, more helpful help your mood. Another helpful
thoughts next to the original behaviour is ‘pacing’. This means
worries. This is not the same as doing a consistent amount of
‘positive thinking’, as you may activity on a regular basis, but
have some valid concerns; it is not overextending yourself on a
about maintaining perspective, good day. Overextending activities
having a balanced view, and not tends to result in people being
getting too caught up in your so exhausted that they cannot
thoughts. function for a few days.
"I think at the beginning I did bottle "I have accepted that first thing in the
my feelings up too much, trying to morning I am not going to leap out of
stay strong for everyone else." bed; my whole body aches so I take it
slowly. I feel human and am able to
Changing behaviour cope with almost anything. I still play
Some types of behaviour make golf a couple of times a week, and,
emotional distress worse. For being a competitive person I have to
example, when people avoid remind myself each time how lucky I
activity, socialising and exercise am just to be out in the sunshine."
(even doing basic things like
having a shower and getting Specific emotions and
dressed) they make depression coping strategies
worse, rather than better. And, Shock, disbelief, helplessness
when people avoid situations that and feeling out of control
make them anxious, this also
tends to make the problem worse, These feelings and sensations are
rather than better. common when people experience
something outside of the realm
Behavioural change, which of their normal experience, like
includes engaging in enjoyable a diagnosis of a serious illness.
and meaningful activities, doing The situation can feel threatening
Helpline freephone 08088 010 444 35The psychological impact of
MDS (cont.)
and people wonder whether they •• ‘Grounding’ techniques can be
can cope. These thoughts and useful. These are simply things
feelings can be so overwhelming people can do to bring their
that people become shocked or awareness to the reality of the
numb as a means of protecting present moment, in other words
themselves. Some people describe to feel less detached or unreal.
a sense of unreality. You can find more information
on grounding techniques at
"There was a total overwhelming
www.healthyplace.com
feeling of helplessness and being
out of control of my everyday life. "At diagnosis I was shocked and
But I had to carry on regardless for upset. But I was determined to fight it
everyone else." and live a long life."
Coping strategies Worry, anxiety and living with
•• Time is needed for the uncertainty
information to sink in and to be MDS often carries with it a
‘processed.’ degree of uncertainty which can
lead to worry and anxiety. It is
•• It can be helpful to talk things normal to experience fear about
through with others and to
something which is threatening.
express feelings. This helps
The emotional response to
people to make sense of their
fear is anxiety, or even panic.
situation and to think about
This tends to be driven by the
how they will cope.
physical response to fear, which
•• Having access to the right is a release of adrenaline into
information at this time is the bloodstream. This leads to
important. It can be difficult many of the physical symptoms
to take everything in, so it of anxiety like increased heart
can be useful to write down rate and dry mouth. The mental
questions that need answering aspect of fear is worry. This is
or clarifying by the healthcare what people do as they try to
team. predict and control things that
might happen in the future.
36 www.leukaemiacare.org.ukWhile it is normal for people to •• A widely-used technique is
worry about their illness to some called ‘progressive muscle
degree, excessive worry will lead relaxation’. This gets people
to chronic anxiety and exhaustion. to consciously tense and un-
tense their muscles to induce
"I was anxious a lot and focused on
relaxation.
my diagnosis and what might happen
to me. I didn’t want to die." •• Notice your negative thoughts
and worries and write them
Coping strategies down to challenge them.
•• Managing the physiological part
of anxiety is key as this will help •• Take gentle exercise.
to reduce the level of fear and •• Various forms of distraction, or
stop the pulse - and thoughts - mental exercises like Sudoku,
from racing. can help.
•• To do this, it is necessary to "Living with uncertainty has been a
reduce hyperventilation (over phrase which I have often used in the
breathing) and excessive past. But living with MDS tests it to
adrenaline production, which extremes. In reality, it’s very difficult
are always present in anxiety. to live when you are uncertain what
the next few months or years have
•• Slow, controlled breathing is in store for you. Uncertainty breeds
the most effective method.
anxiety."
Practices like mindfulness
and meditation can be useful, Finally, a vital aspect of managing
but there are also a number of worry is to accept that some
different breathing exercises things you cannot know in
that are helpful. For examples advance or control. Also, while
of these online, visit www. it is possible to reduce some of
getselfhelp.co.uk and www. the symptoms of anxiety, it is
patient.co.uk not possible to eliminate them
altogether. As human beings we
•• Reducing tension in the all live with a degree of anxiety.
muscles is another means of
A useful means of managing
alleviating anxiety.
uncertainty is to focus on the
Helpline freephone 08088 010 444 37The psychological impact of
MDS (cont.)
‘here and now’ – on the things you common), dwelling on the
can change, and on the things thoughts behind it tends to
that you find meaningful and make the anger worse. Talk
enjoyable in the present moment. things through with others.
Anger •• Write down some of your
thoughts and notice those
It is common for people to
that keep the anger going; try
feel angry that they have been
to change them or distance
diagnosed with a serious illness.
yourself from thoughts about
For a number of reasons it can
things that have no explanation
feel confusing, unfair, or that it
or cannot be changed.
is outside of their control – for
example if the illness is rare, •• Use relaxation techniques,
if they believe that they have a or exercise, for managing
healthy lifestyle, if there’s no the physiological symptoms
history of similar illnesses in of anger (similar to those in
their family, or if they believe that anxiety, and also driven by
they have already had too many adrenaline).
problems in life to cope with.
Sometimes it can be difficult to •• ‘Venting’ anger at others tends
know what to do with feelings of to be self-defeating because it
anger or to understand at what alienates people, rather than
the anger is directed. As a result eliciting feelings of compassion
anger can sometimes get directed from them.
at loved ones, or even towards
oneself.
•• Self-soothe. Treat yourself to
things you enjoy; treat yourself
"At diagnosis I felt distraught, with compassion.
devastated and angry. It was unfair.
Stress
Why me?"
We experience stress when we
Coping strategies feel that we are under too much
•• Although a sense of disbelief pressure or have too many
or injustice at being diagnosed demands being made of us and
with MDS is valid (and that we don’t have the resources
38 www.leukaemiacare.org.ukto cope. Understandably, people •• Pace yourself, rather than doing
can feel like this at times when too much or trying to cope with
they are ill and they are trying everything at once.
to cope with the demands
of treatment as well as with •• Take breaks and ‘time out’.
other concerns, for example •• Ask for help and support.
financial issues, employment
and relationships. The emotional •• Maintain a ‘here and now’ focus
symptoms of stress can include on things that are enjoyable and
low mood, anxiety and irritability. meaningful to you.
Coping strategies Useful online resources include:
•• Relaxation techniques ••www.helpguide.org
(controlled breathing,
progressive muscle relaxation) ••www.getselfhelp.co.uk
and/or exercise to manage the ••www.nhs.uk/conditions/
physical, adrenaline-fuelled stress-anxiety-depression
aspects of stress (which are the
same as those in anxiety and Guilt and blame
anger). Although becoming ill is never
anyone’s fault, it is common for
•• Notice the negative thoughts people to experience feelings
which contribute to anxiety,
of guilt and blame about their
tension and irritability,
illness. For example people might
producing adrenaline as they
question whether they became ill
arise: "this is unbearable", "I
because of something they did, or
can’t cope".
their ‘lifestyle’. Some people might
•• Challenge negative thoughts by think that they are a burden on
writing them down and coming other people because they need
up with more helpful ones e.g. their help, or because they are
"although this is difficult, I can not functioning as they once
cope (especially with support)". did. Although these thoughts are
common, they are not valid. They
•• Plan, prioritise, break things can be part of people’s attempts
down into manageable ‘chunks’ to find meaning in the situation,
(writing this out is helpful).
Helpline freephone 08088 010 444 39You can also read