Bugs, Biofilms, and Resistance in Cystic Fibrosis
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
Bugs, Biofilms, and Resistance in Cystic Fibrosis
Jane C Davies MB ChB MRCP MRCPCH MD and Diana Bilton MD FRCP
Introduction
Why the Propensity For Bacterial Infection? Lessons Learned From
Pseudomonas aeruginosa
Acquisition of Infection
Establishing Chronic Infection
Infection With Other Organisms
Burkholderia cepacia complex
Stenotrophomonas maltophilia
Achromobacter (Alcaligenes) xylosoxidans
Pandoraea, Ralstonia, Inquilinus, and other species
Nontuberculous Mycobacteria
New Non-Culture-Based Diagnostic Techniques
Prevention and Treatment
The Basic Tenets of Antibiotic Treatment
Summary
Bacteria infect the respiratory tract early in the course of cystic fibrosis disease, often fail to be erad-
icated, and together with an aggressive host inflammatory response, are thought to be key players in the
irreversible airway damage from which most patients ultimately die. Although incompletely understood,
certain aspects of the cystic fibrosis airway itself appear to favor the development of chronic modes of
survival, in particular biofilm formation; this and the development of antibiotic resistance following
exposure to multiple antibiotic courses lead to chronic, persistent infection. In addition to the common
cystic fibrosis pathogens, such as Staphylococcus aureus, Haemophilus influenzae, and Pseudomonas
aeruginosa, several newer species are becoming more common. Furthermore, new molecular techniques
have led to the identification of multiple different organisms within respiratory secretions, many of
which are not cultured with conventional tools. Future work should aim to develop clinically applicable
methods to identify these and to determine which have the potential to impact pulmonary health. We
outline the basic tenets of infection control and treatment. Key words: cystic fibrosis, biofilm, antibiotic
resistance. [Respir Care 2009;54(5):628 – 638. © 2009 Daedalus Enterprises]
Introduction hood and is chronic by early adulthood. In this article we
discuss: the various hypotheses for the susceptibility of the
Almost all patients with cystic fibrosis (CF) have bac- CF airway to infection, and illustrate with Pseudomonas
teria identified from airway secretions at some point in aeruginosa some of the strategies bacteria have developed
their lives. For the majority, such infection begins in child-
Jane C Davies MB ChB MRCP MRCPCH MD is affiliated with the De- Dr Davies presented a version of this paper at the 43rd RESPIRATORY
partment of Gene Therapy, Imperial College London, and the Department of CARE Journal Conference, “Respiratory Care and Cystic Fibrosis,” held
Paediatric Respiratory Medicine, Royal Brompton Hospital, London, United September 26-28, 2008, in Scottsdale, Arizona.
Kingdom. Diana Bilton MD FRCP is affiliated with the Department of
Respiratory Medicine, Royal Brompton Hospital, London, United Kingdom. Correspondence: Jane C Davies MB ChB MD, Department of Gene
Therapy, Imperial College, Emmanuel Kaye Building, Manresa Road,
The authors have disclosed no conflicts of interest. London SW3 6NP, United Kingdom. E-mail: j.c.davies@imperial.ac.uk.
628 RESPIRATORY CARE • MAY 2009 VOL 54 NO 5
BUGS, BIOFILMS, AND RESISTANCE IN CYSTIC FIBROSIS
to evade host defenses; other organisms that infect the CF
respiratory tract; new diagnostic techniques; and the tenets
of prevention and treatment.
Why the Propensity For Bacterial Infection?
Lessons Learned From Pseudomonas aeruginosa
P. aeruginosa, an environmental pathogen found in moist
areas such as sinks and drains, is of low virulence in the
majority of clinical situations. In the healthy host, bacteria
that enter the lungs are cleared rapidly, without the initi-
ation of an inflammatory response; this involves a variety
of innate host defense strategies, both mechanical (muco-
ciliary clearance) and immunological (resident macro-
phages and antimicrobial peptides). In certain clinical sit-
uations this first line of defense fails, and these normally Fig. 1. Pseudomonas aeruginosa possess multiple, unipolar pili,
harmless bacteria survive, multiply, and lead to organ dam- which mediate adherence and are involved in twitching motility,
age. Such conditions are encountered in mechanically ven- and a single, thicker, motile flagellum. Both of these structures are
tilated patients in intensive care, in those with defective pro-inflammatory and may trigger a host response even if shed
immunity or severe burns, and in patients with CF. from the bacterial cell. In this diagram, the pili are visualized via
transmission electron microscopy after negative staining.
The mechanisms underlying the early acquisition of in-
fection in CF are complex, incompletely understood, and
were recently reviewed.1 Briefly, hypotheses include im-
narrow range of pathogens characteristically associated
paired mucociliary clearance related to low airway surface
with CF (if indeed this is true—more later).
liquid volume (the low-volume hypothesis)2; increased
Bacteria use specific adhesins to bind to receptors, ei-
availability of cell surface receptors3; and impaired inges-
ther on secretions or the cell surface. P. aeruginosa pos-
tion of bacteria by epithelial cells.4 Once within the air-
sess several classes of adhesins, including pili (fine, hair-
way, conditions such as hypoxia within mucus plugs5 may
like unipolar structures) and flagellae, which are also used
attract motile organisms capable of anaerobic survival and
for motility (Fig. 1). Murine studies have confirmed the
encourage biofilm formation. In addition to the biofilm
importance of these structures, as deficient mutants cause
matrix, P. aeruginosa has evolved a huge armamentarium
significantly milder disease.7 The majority of pseudomo-
of strategies by which it evades host defenses and ensures
nas strains isolated from recently infected patients with CF
its survival within the CF respiratory tract.
are piliated, which supports a role for adherence at this
stage. Once chronic infection has been established, the
Acquisition of Infection pilin genes are down-regulated, which leads to loss of the
structures. The receptor for both pili and flagellae has been
The first of these mechanisms, the low-volume hypoth- identified as a disaccharide, GalNAc1-4Gal, contained
esis, is the focus of another article from this conference6 within several asialylated glycocolipids. One of these, asia-
and will not be discussed in detail here. The hypothesis is loGM1, is present in increased abundance on the surface
premised on the concept that the defective cystic fibrosis of CF respiratory epithelial cells,8 and many authors have
transmembrane regulator (CFTR) fails to inhibit sodium reported greater adherence of P. aeruginosa to CF cells
absorption through the epithelial sodium channel.2 Hy- than to those of wild-type (healthy, non-CF) origin.8,9 This
perabsorption of water results, which depletes the airway may be related to the abnormal function or distribution of
surface liquid, impairs mucociliary clearance, and allows sialyltransferase enzymes within the CF cell, and is par-
inhaled bacteria to remain within the airway. This mech- tially correctable with CFTR gene transfer.9 Furthermore,
anism is considered by most to be key in CF pathogenesis, pseudomonads produce an enzyme, neuraminidase, that
although some have questioned the exact nature of its role, cleaves sialic acid off glycolipids.8 Is the organism capa-
given the very different manifestations in another disease ble of increasing its foothold in the CF airway in this way?
with impaired mucociliary clearance: primary ciliary dys- It is unknown whether this mechanism, which has largely
kinesia. Retained cough clearance and/or differences in been observed in vitro in experimental models, is relevant
inflammatory response in primary ciliary dyskinesia may in vivo. Against it, postmortem studies have clearly de-
be explanations. Additionally, the low-volume hypothesis scribed an absence of bacteria in direct contact with air-
alone does not appear to adequately explain the relatively way cells; rather, those studies found large colonies within
RESPIRATORY CARE • MAY 2009 VOL 54 NO 5 629BUGS, BIOFILMS, AND RESISTANCE IN CYSTIC FIBROSIS
luminal mucus.10 Clearly, these tissues were from patients
with severe end-stage disease and chronic infection; these
findings may bear no relation to what occurs during the
early acquisition of infection. Recent studies highlighted
another possible role for asialoglycolipids in the severe
inflammation typical of the CF lung. It has long been
appreciated that adherence of the organism to this receptor
led to an NFB-mediated increase in expression of pro-
inflammatory cytokines such as interleukin-8. This is one
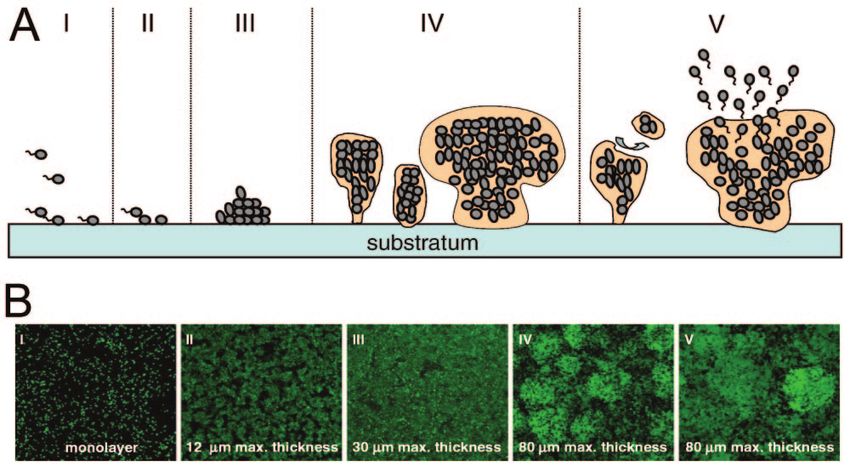
Fig. 2. A: The mucoid phenotype of Pseudomonas aeruginosa
of the major neutrophil attractants in the CF airway and is growing on MacConkey agar. B: Compared to the clearly defined
present in high levels in both sputum and bronchoalveolar borders and matt appearance of non-mucoid colonies. (Courtesy
lavage samples. The complex pathway through which this of Nick Madden MD, Microbiology Department, Royal Brompton
process occurs has now been described, which led to the Hospital, London, United Kingdom.)
suggestion that bacteria in the airway may provoke inflam-
mation without actually adhering to the cell surface, by
shedding of bacterial components such as pili and flagel- between the low glutathione level and predisposition to
lae, which then bind to aGM1 and promote interleukin-8 infection is as yet incompletely understood.
release.11
The adherence hypothesis supports the notion that in- Establishing Chronic Infection
haled pseudomonads have a natural niche on the CF air-
way surface. It would go some way to explaining the high Once the initial foothold has been gained, the bacteria
prevalence of this organism (and S. aureus, which also must survive despite host defenses, both innate and ac-
quired, and repeated courses of both systemic and topical
binds to this receptor), as opposed to other common re-
antibiotics. The bacteria’s armamentarium of immuno-
spiratory organisms (such as S. pneumoniae, which is sur-
evasive strategies includes the secretion of exoproducts,
prisingly rarely cultured), and explaining the exaggerated
antibiotic-resistance proteins, and phenotypic changes that
inflammatory response observed. However, as with the
render them virtually unrecognizable from the bacteria that
airway-surface-liquid hypothesis, it seems unlikely to be
were first on the scene. The physical and immunological
the sole explanation. These 2 hypotheses are in no way
protection provided by the biofilm structures they form is
mutually exclusive, and the predisposition to pseudomo-
probably key in their long-term survival.
nas infection may relate to a combination of these 2 mech-
Both elastase and alkaline protease protect against im-
anisms, or others in addition. mune destruction by cleaving immunoglobulins, comple-
Several years ago, a study by Pier et al reported that ment components, and cytokines. Exotoxin A inhibits
respiratory epithelial cells are capable of ingesting phagocytosis and suppresses the cell-mediated immune re-
P. aeruginosa, and suggested that this, followed by slough- sponse. The siderophores, such as pyocyanin, which has
ing off of these cells, could be a pulmonary defense mech- been detected in CF sputum,15 break down intercellular
anism.4 They showed that cell lines expressing mutant tight junctions, slow ciliary beat frequency, and thereby
CFTR were less capable of ingestion and hypothesized may further impair mucociliary clearance.
that this was the basis for the relationship between pseudo- Our understanding of antibiotic resistance mechanisms
monas and the CF lung. They have since reported that the is growing rapidly, aided in part by new molecular tools,
mechanism for uptake into the cell involves binding to the and the sequencing of the P. aeruginosa genome. High
CFTR protein itself.12 These studies remain controversial, levels of resistance relate to a poorly permeable outer mem-
as the levels of uptake were extremely low, and applica- brane, efficient multidrug efflux pumps, and  lactamases.
bility to the clinical situation has not yet been demon- The details of this complex topic are outside our scope
strated. The levels of nasal and exhaled nitric oxide (NO) here, but the interested reader is referred to the paper by
are low in CF, which is a surprising finding given the fact Hancock and Speert16 for a detailed review.
that NO levels are usually high in inflammation. This is One interesting property of the P. aeruginosa strains
accompanied by low levels of inducible nitric oxide syn- found in the CF lung that differentiates them from strains
thase (NOS2),13 and there is accumulating evidence that found in other clinical settings is that they are unusually
expression of this enzyme is regulated by CFTR. NO has hypermutable.17 They can react promptly to their environ-
certain antibacterial properties, so a low NO level could ment, not only by switching genes on or off, but by an
play a part in the predisposition to infection. Similarly, the increased frequency of mutation events within the genome.
antioxidant glutathione is normally secreted via CFTR, One such mutation event triggers conversion to a mucoid
and is therefore deficient in the CF airway14; the link phenotype (Fig. 2), which is almost pathognomonic for
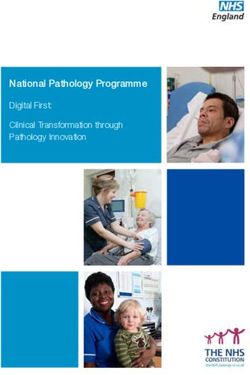
630 RESPIRATORY CARE • MAY 2009 VOL 54 NO 5BUGS, BIOFILMS, AND RESISTANCE IN CYSTIC FIBROSIS Fig. 3. Steps thought to be involved in biofilm formation. The top row (A) diagrams what is believed to be occurring in the bottom row (B), which shows confocal microscopy of fluorescently labeled organisms. Single (planktonic) bacterial organisms are inhaled (I) and settle onto a surface such as the respiratory mucosa (II), where they multiply into microcolonies (III). These evolve into mushroom-like structures and a biofilm matrix (pink) is produced, which surrounds the by now large colonies of less metabolically active organisms (IV). On occasion the biofilm matrix breaks down into parts and a shower of organisms leave the biofilm (V), which might cause respiratory exacerbation, although that hypothesis is difficult to confirm. (Adapted from Reference 19, with permission.) CF.18 In response to environmental triggers such as nutri- bacteria “sense” other bacteria in the vicinity. Once a crit- tional stress or the hypoxia within a CF mucus plug, mu- ical mass is achieved, the quorum-sensing molecules in- tants are selected that over-produce mucoid exopolysac- duce the expression of genes vital to biofilm production. In charide (alginate), which surrounds them and protects them this state, micocolonies of bacteria are surrounded by a from external challenges such as mucociliary clearance, dense matrix that protects against phagocytosis and pre- the host immune response, and antibiotics, and is highly vents penetration by antibiotics (see Fig. 3). This pheno- pro-inflammatory. Cohort studies found worse lung func- typic change probably plays a major role in the persistence tion in patients infected with mucoid strains than in those of pseudomonas infection in the majority of CF patients, with non-mucoid strains. despite best medical attempts at eradication. Another highly successful survival strategy involves the formation of biofilms (Fig. 3).19 Many bacteria protect Infection With Other Organisms themselves in this way: on biological surfaces in diseases such as bacterial endocarditis and osteomyelitis; on syn- S. aureus is relatively common in early childhood and is thetic materials such as indwelling catheters; and on en- often the first bacterial infection to be isolated from the vironmental structures such as the rocks in ponds and riv- respiratory tract.22 Opinion differs as to whether attempt- ers. Over the last decade it has become clear that ing to prevent infection with antibiotics is useful (more on P. aeruginosa (and possibly other chronically infecting this below). Small colony variants have been described in organisms such as Burkholderia cepacia complex) exist in the more recent literature and are commonly associated biofilms within the CF lung.20 Initiation of biofilm forma- with persistent infection and co-infection with other patho- tion is dependent on a process of “quorum sensing.”21 gens, particularly P. aeruginosa. Resistant strains, in par- Bacteria produce molecules such as acyl homoserine lac- ticular, methicillin-resistant S. aureus, pose substantial lo- tones, which diffuse freely in and out across the bacterial gistical problems in CF clinics. Additionally, recent data membrane. Due to this free diffusibility, the concentration suggest a poorer prognosis in patients infected with these within the organism reflects the concentration outside, organisms,23 although whether this relates to preexisting which is a direct read-out of the bacterial number. Thus, factors or is a consequence of the infection is incompletely RESPIRATORY CARE • MAY 2009 VOL 54 NO 5 631
BUGS, BIOFILMS, AND RESISTANCE IN CYSTIC FIBROSIS
understood. H. influenzae is also commonly isolated in
early disease and in childhood. Compared to some of the
other organisms discussed in this article, there is a relative
paucity of research and literature on H. influenzae.
Burkholderia cepacia complex
B. cepacia complex (initially referred to as Pseudomo-
nas cepacia) led to severe outbreaks in CF subjects world-
wide during the 1980s, with substantial morbidity and mor-
tality. The prevalence of B. cepacia complex has remained
relatively stable among CF patients in both the United
States and the United Kingdom during the past several
years; approximately 3– 4% of patients are infected, al-
though prevalence is much higher in certain centers. Since
the introduction of effective infection-control measures,
the numbers of patients in such centers has stabilized or
fallen.
Currently, there are 11 species in what is now collec-
tively referred to as the B. cepacia complex.24 Within CF,
B. cenocepacia (genomovar III), B. multivorans (genomo-
var II), and B. vietnamiensis (genomovar V) account for
the majority of isolates: approximately 50%, 35%, and
5%, respectively,25 although B. dolosa (genomovar VI)
has also come to prominence in recent years.26 Identifying
B. cepacia complex species can be difficult. These species
are easily confused with other non-fermenting Gram-neg-
ative bacteria such as Stenotrophomonas, Alcaligenes, Pan- Fig. 4. Transmission electron micrograph of Toronto/Edinburgh
epidemic clone of Burkholderia cepacia expressing cystic fibrosis
doraea, and Ralstonia. In some studies as many as 10% of
mucus-binding Cbi adhesin pili. High-resolution was achieved with
CF sputum isolates initially identified as B. cepacia were a JEOL 100CX electron microscope and negative staining. (From
in fact misidentified.27 Clinical microbiology laboratories Reference 31, with permission.)
that handle specimens from CF patients must be aware of
this issue and have specific measures in place to ensure
correct identification.28 (2– 4 m) are peritrichously arranged and intertwine to
Several specific features of certain B. cepacia complex form cable-like structures (Fig. 4).31
organisms cause particular concern in the context of CF: B. cepacia complex species are intrinsically resistant to
the potential for transmissibility; antibiotic multi-resistance a broad range of antibiotics and non-oxidative killing by
and host-defense survival strategies; and the association human phagocytic cells. Some strains can invade and sur-
with adverse clinical outcomes, including systemic spread, vive within respiratory epithelial cells 32 or macro-
which makes it almost unique among CF airway patho- phages,33,34 thus potentially evading host defenses. Fur-
gens. ther, they possess an array of virulence factors, including
Early recognition that several members of the complex proteases and highly inflammatory lipopolysaccharide
were highly transmissible and were the cause of outbreaks structures (Table 1),43 which elicit brisk, exaggerated, and
in CF communities29 led to the closure of all CF summer potentially detrimental host responses.44 As with P. aerugi-
camps in the United States and Canada and recommenda- nosa, it appears that B. cepacia complex organisms pro-
tions for cohorting CF patients based on their bacterial duce biofilms in vivo.45 Features, including its nutritional
pathogens. Numerous CF-associated B. cepacia complex versatility and adaptability, and the development of anti-
epidemics have now been described. One particularly trans- biotic resistance, are probably at least in part due to its
missible strain that has spread both within and between CF unusually large, complex, and variable genome.46 Typi-
centers on both sides of the Atlantic is B. cenocepacia cally, these organisms are resistant to aminoglycoside and
strain ET12. It carries the cblA gene,30 which encodes for polymixin antibiotics due to the unusual lipopolysaccha-
the major structural subunit of unique cable pili, which are ride component of their cellular membrane.47 In addition
key structures that mediate binding to mucin components to intrinsic resistance these species can also acquire resis-
and respiratory epithelial cells. These enormously long pili tance during therapy due to  lactamase production,48 up-
632 RESPIRATORY CARE • MAY 2009 VOL 54 NO 5BUGS, BIOFILMS, AND RESISTANCE IN CYSTIC FIBROSIS
Table 1. Burkholderia cepacia Complex Virulence Factors and Their Functions
Virulence Factor Protein/Gene Species (strain) Function First Author, Year
Proteases zmpA Many, not Burkholderia Proteolysis of extracellular matrix Gingues35 2005
multivorans or B. dolosa
zmpB Many, not B. multivorans or Proteolysis of extracellular matrix Kooi36 2006
B. dolosa
mgtC B. cenocepacia (K-562) Survival in macrophages; virulence rat Maloney37 2006
lung-infection model
HtrA protease B. cenocepacia (K-562) Growth under osmotic or thermal Flannagan38 2007
stress, survival rat-infection model
Serine protease (homologous B. cenocepacia (J2315) Digestion of ferritin to release iron Whitby39 2006
to subtilase family)
Lipases Lipase Multiple species Role in invasion Mullen40 2007
Phospholipase C B. cenocepacia, B. multivorans, Digestion of phosphatidylcholine of Carvalho41 2007
B. vietnamiensis, B. ambifaria lung surfactant; no correlation with
virulence yet
Exotoxin LPS Many species Cytokine secretion, inflammatory Reddi42 2003
response
(Adapted from Reference 43.)
regulation of antibiotic efflux pumps,49 and alteration of similarly high rate of S. maltophilia acquisition in patients
antibiotic targets. Inducible resistance is a particular prob- treated with the  lactam ceftazidime.54 In CF the use of
lem in CF patients, who often receive multiple prolonged steroids or antipseudomonal agents, including quinolone
courses of antibiotics. antibiotics and inhaled aminoglycosides, has been impli-
Infection with B. cepacia complex is an independent cated as risk factors, although the findings have not always
negative prognostic indicator in CF. Individuals who ac- been consistent among studies. Epidemiological studies
quire these organisms, however, fall into different clinical suggest that the majority of S. maltophilia infection in CF
groups: they may be asymptomatic; experience rapid re- results from independent acquisition, most likely from en-
spiratory decline; or, as is observed in a minority, develop vironmental sources, rather than from cross-infection. Sev-
the “cepacia syndrome,”50 in which organisms invade sys- eral studies in CF have produced convincing evidence that
temically and cause endotoxic shock, multi-organ failure, acquisition of the organism per se is not detrimental.55-58
and, in many cases, death. The individual’s clinical re- Although patients who acquired S. maltophilia had more
sponse to infection probably relates both to bacteria-spe- advanced disease than those who did not, detection of this
cific and host-specific features, although as yet this area is species in sputum culture did not independently affect the
not fully understood. rate of deterioration or survival. To what extent these ob-
servations reflect the severity of underlying lung disease,
Stenotrophomonas maltophilia as compared to the more frequent use of broad-spectrum
antibiotics in this group of patients, remains to be deter-
S. maltophilia is an aerobic Gram-negative motile rod mined.
with multitrichous flagella. The prevalence of S. malto-
philia in CF increases with age and appears to relate to Achromobacter (Alcaligenes) xylosoxidans
antibiotic exposure history. Prevalence rates of 4 –30%
have been reported in various studies.51-53 The incidence Although A. xylosoxidans, a motile, Gram-negative ba-
of infection in patients who do not have CF has increased cillus, has been recognized for many years as being capa-
steadily in recent years, although single or intermittent ble of causing infection in persons with CF, the proper
isolation of S. maltophilia is common. Broad-spectrum nomenclature of this species has presented an ongoing
antibiotic therapy and selective pressure that could pro- challenge. Its incidence in CF differs between centers, and
mote emergence of multi-resistant bacteria has long been the organism usually coexists with other airway patho-
implicated as a risk factor for S. maltophilia acquisition. gens. Because infection is so often transient, detection and
Among patients who do not have CF, the use of carbap- the reported infection rate are strongly influenced by the
enem antibiotics, especially imipenem, to which S. malto- frequency of sputum culture. A recent study by Tan and
philia are uniformly resistant, has been widely believed to colleagues indicated that 13 (2%) of 557 patients in their
increase the risk of infection. However, there has been a pediatric and adult CF units were chronically infected with
RESPIRATORY CARE • MAY 2009 VOL 54 NO 5 633BUGS, BIOFILMS, AND RESISTANCE IN CYSTIC FIBROSIS
this organism; a further 31 (6%) patients were intermit- been reported that otherwise healthy adults who have pul-
tently colonized.59 With regard to acquisition, there is little monary atypical mycobacteria (with or without bronchi-
evidence that it is acquired by patient-to-patient cross- ectasis), have a high prevalence of unrecognized CF or are
infection.60 Persistence seems to be variable once the lung CF carriers.65 Although the association of atypical myco-
is infected, from transient to up to 6 years in one patient. bacteria with isolated bronchiectasis had been thought to
Based on the available evidence it does not seem that be caused by a weak or ineffective cough, this appears to
infection with A. xylosoxidans contributes greatly to clin- be unlikely. It has been suggested that all patients with
ical deterioration in CF patients. pulmonary non-tuberculous mycobacterial infections and
no apparent immunodeficiency by tested for CF.
Pandoraea, Ralstonia, Inquilinus, and other species
New Non-Culture-Based Diagnostic Techniques
Although CF patients have been identified as being
chronically infected with Pandoraea species, the preva- Conventionally, organisms are identified from sputum,
lence and pathogenic role of these species in CF is un- cough (or oropharyngeal) swabs, or bronchoalveolar la-
known. At present Pandoraea species are most notewor- vage, via culture on agar plates. Specific agars can be
thy and troublesome in CF insofar as they are generally used, tailored toward the commonly recognized organ-
misidentified as other species,61 particularly B. cepacia isms, but all rely on culture. Visible colonies are tested for
complex. The genus Ralstonia was named in 1995, and accurate identification and for antibiotic sensitivity. More
R. insidiosa and R. respiraculi have been identified from recently, however, molecular techniques have been used
isolates recovered from CF sputum culture. The frequency on similar samples. These techniques do not rely on cul-
and clinical impact of Ralstonia species infection in CF ture but instead use specific probes to search for bacterial
have not been systematically studied.62 Organisms in the DNA and/or RNA. The technique is based on the fact that
genus Inquilinus are ␣-protobacteria. Inquilinus is a Gram- different organisms possess different (and mostly well-
negative, non-fermentative bacterium but is not related to described) DNA sequences, so identification is accurate.
P. aeruginosa or B. cepacia complex.63 It is slow-growing Some techniques can also quantify different bacteria, at
and can be difficult to culture and identify. There are least in relative values. These studies showed an unsus-
insufficient data to determine how pathogenic this organ- pectedly wide range of organisms, including numerous
ism is for CF patients. anaerobes, for which most laboratories do not search with
conventional culture.66-68 Interestingly, the healthy non-CF
Nontuberculous Mycobacteria airway, which is often described as sterile, has also been
shown to harbor DNA from multiple organisms, which
Patients with CF have long been recognized as having raises important questions as to how pathogenic these or-
an increased predisposition for non-tuberculous mycobac- ganisms are in the disease setting. Several ongoing studies
teria, including Mycobacteria abscessus, M. avium intra- are addressing that issue. Both culture and molecular tech-
cellulare, and M. chelonae. The majority of patients har- niques rely on the availability of lower-airway secretions,
bor unique strains acquired from the environment, as which can be a problem with many patients with milder
opposed to via patient-to-patient spread. The prevalence disease, particularly children. Experimental strategies fo-
range is 2–20%, and one of the largest studies reported that cused on volatile bacterial products in exhaled breath may
13% of patients had at least one of 3 cultures positive.64 offer an advantage.69 “Electronic noses” and mass-spec-
The rates are increasing, although whether that reflects the trometry-based techniques have shown success in other
increasing age (a significant risk factor for infection) of airway infections and could be applicable to the non-ex-
surviving patients or a true increase in acquisition is un- pectorating CF patient, although further work is clearly
certain. As with some of the organisms discussed above, required.
determining the significance of a single isolation can be
difficult; many infections are transient and not associated Prevention and Treatment
with clinical decline. Evidence suggests that infection with
M. abscessus, in particular, may be more likely to be as- Infection-control measures are discussed in greater de-
sociated with clinical decline.64 Whereas imaging is useful tail in O’Malley’s paper for this conference.70 In brief,
in patients who have the infection but do not have CF, the cross-infection can be substantially limited by simple mea-
appearances typical of CF can make distinguishing any sures such as handwashing between patients, and the use
additional features of non-tuberculous mycobacteria dis- of disposable equipment such as spirometer mouthpieces.
ease extremely difficult. Heavy or persistent isolates, or The incidence of B. cepacia complex infection has de-
those associated with clinical symptoms not explained by creased since most clinics have adopted a cohorting policy
other organisms, should arouse suspicion. It has recently and stopped mingling of CF patients outside the center, for
634 RESPIRATORY CARE • MAY 2009 VOL 54 NO 5BUGS, BIOFILMS, AND RESISTANCE IN CYSTIC FIBROSIS
example in summer camps and conferences. However, rou- that used oral cephalosporins,83 which are not used in the
tine widespread cohorting of patients based on airway cul- United Kingdom. A definitive study to confirm or refute
tures is a controversial issue.71-74 While most would agree the benefits of this strategy is urgently needed.
that cohorting of patients with highly transmissible or multi-
resistant pathogens is advisable, opinion differs with re- 2. P. aeruginosa Can Clearly Be Eradicated If Identi-
gard to specific organisms. Two areas of particular dis- fied Early.84 One of the major developments of the last
agreement are whether to separate patients with and without decade has been the recognition of the benefits of early
antibiotic-sensitive P. aeruginosa, and whether patients identification and aggressive treatment of P. aeruginosa.
with some of the organisms listed above (eg, S. malto- Successful eradication has been reported with regimens
philia), which appear to pose little clinical disadvantage to that included systemic (oral ciprofloxacin or intravenous
the patient, should be isolated. agents) and topical, nebulized treatments. The optimal reg-
When considering the potential benefits of patient seg- imen and duration remain unclear. However, the impor-
regation, several disadvantages need to be addressed. First, tance of careful, frequent surveillance cannot be overem-
each patient can be segregated only on the basis of previ- phasized; any eradication protocol is useless if the infection
ous culture results, which may not reflect current infection is not identified.
status, and which may be difficult to obtain, for example
from children. Second, as it is becoming clear that within 3. Long-Term Suppressive Treatment of P. aeruginosa
a species, some strains may be significantly more detri- Is Advantageous.85 Nebulized antibiotics, in particular
mental than others, cohorting all patients with these or- colomycin, have been used for decades in many parts of
ganisms together may pose a risk for those infected with Europe, although, in the main, this practice evolved in an
the more benign strains. This could be the case, for exam- era when “evidence-based” medicine was less rigorous
ple, in many B. cepacia complex clinics. Third, cohorting that it is today. Wider acceptance of this strategy has come
on the basis of multi-resistance may be hindered by the with the development of inhalable tobramycin, and with
continuously changing susceptibility patterns of many of the well-conducted trials that established the role of long-
these organisms.75 Fourth, there may be a stigma attached term suppressive therapy in maintaining lung function in
to patients within certain of these infection groups. This patients with chronic P. aeruginosa infection.
has already been described for patients with B. cepacia
complex organisms.76,77 Finally, cohorting creates a sub- 4. In Vitro Sensitivity Testing Has Substantial Limita-
stantial logistical burden on CF centers. Perhaps in view of tions. As any clinician well knows, certain patients fail
these concerns it is not surprising that there are no world- to respond to an antibiotic regimen that is based on in vitro
wide standard procedures for cohorting such patients. The sensitivity testing, whereas others appear to respond well
majority of clinics separate patients with B. cepacia com- to a combination that should theoretically be useless. This
plex and methicillin-resistant S. aureus, while others will probably reflects the very different growth modes of the
go further. Whichever model is favored, basic infection- organisms in the airway versus on a culture plate. At-
control guidelines should always be followed. tempts to perform sensitivity testing on organisms grown
in biofilms in the laboratory have been somewhat disap-
The Basic Tenets of Antibiotic Treatment pointing. Further work is needed, as we urgently require a
better method of predicting optimal treatments.
Specifics of therapy have been well reviewed.78-81 Rather
than dealing with organisms individually here, we address 5. Doses Are Often Different Than Those Used in Pa-
some basic principles underlying clinical management, tients Who Do Not Have CF Patients with CF handle
starting with early childhood and progressing through the drugs differently than patients who do not have CF; in
usual disease stages: general, higher doses are required. The action of the anti-
biotic on the organism should be borne in mind when
1. The Role of Prophylaxis for S. aureus Is Unclear.82 designing a dosing regimen, as exemplified by the switch
In the United Kingdom at least, many clinics use anti- to once-daily aminoglycoside antibiotics,86 which achieves
staphylococcal prophylaxis (most commonly flucloxacil- a higher peak (concentration-dependent killing) and longer
lin or amoxicillin/clavulanic acid) in young children, from post-antibiotic effect than conventional 3-times-daily dos-
the time of diagnosis. Although studies have demonstrated ing.
reductions in the incidence of S. aureus infection with this
strategy, no benefits on lung function in the medium term 6. Monotherapy Should Be Avoided When Treating
have been conclusively demonstrated. Concerns have been With Intravenous Agents. Many organisms in CF are
raised that such a strategy may increase the incidence of prone to becoming multi-resistant. Monotherapy (eg, with
P. aeruginosa, although this finding was limited to studies intravenous cephalosporins) greatly encourages multiple-
RESPIRATORY CARE • MAY 2009 VOL 54 NO 5 635BUGS, BIOFILMS, AND RESISTANCE IN CYSTIC FIBROSIS
drug resistance. Use combinations of ⱖ 2 antibiotics from 5. Worlitzsch D, Tarran R, Ulrich M, Schwab U, Cekici A, Meyer KC,
different groups.78 et al. Effects of reduced mucus oxygen concentration in airway
Pseudomonas infections of cystic fibrosis patients. J Clin Invest
2002;109(3):317-325.
7. The Benefits of Synergy Testing for Multi-Resistant 6. Ratjen FA. Cystic fibrosis: pathogenesis and future treatment strat-
Organisms Is Unproven. One is often faced in the clinic egies. Respir Care 2009;54(5):595-602; discussion 603-605.
with a heart-sinking row of “R”s on the antibiogram—a 7. Tang H, Kays M, Prince A. Role of Pseudomonas aeruginosa pili in
problem that increases with advancing age of the patient. acute pulmonary infection. Infect Immun 1995;63(4):1278-1285.
In vitro, combinations of agents that alone are ineffective 8. Saiman L, Prince A. Pseudomonas aeruginosa pili bind to asia-
loGM1 which is increased on the surface of cystic fibrosis epithelial
may be synergistic, although evidence for this translating
cells. J Clin Invest 1993;92(4):1875-1880.
into clinical benefit is largely lacking.87 9. Davies JC, Stern M, Dewar A, Caplen NJ, Munkonge FM, Pitt T, et
al. CFTR gene transfer reduces the binding of Pseudomonas aerugi-
8. There May Be Problems in the Longer Term. The nosa to cystic fibrosis respiratory epithelium. Am J Respir Cell Mol
aggressive use of antibiotics is no doubt one of the major Biol 1997;16(6):657-663.
reasons for the improving prognosis of today’s CF pa- 10. Baltimore RS, Christie CDC, Smith GJW. Immunohistopathologic
localization of Pseudomonas aeruginosa in lungs from patients with
tients. This does, however, come at a price. Subclinical
cystic fibrosis. Implications for the pathogenesis of progressive lung
renal impairment associated with repeated doses of ami- deterioration. Am Rev Respir Dis 1989;140(6):1650-1661.
noglycosides is increasingly recognized in adult patients.88 11. Ratner AJ, Bryan R, Weber A, Ngyen S, Barnes D, Pitt A, et al.
Drug allergies are common and often further impair our Cystic fibrosis pathogens activate Ca2⫹-dependent mitogen-activated
therapy choices. The extended life expectancy of patients protein kinase signaling pathways in airway epithelial cells. J Biol
today means that much more focus is now required on the Chem 2001;276(22):19267-19275.
12. Reiniger N, Ichikawa JK, Pier GB. Influence of cystic fibrosis trans-
medium to long term.
membrane conductance regulator on gene expression in response to
Pseudomonas aeruginosa infection of human bronchial epithelial
Summary cells. Infect Immun 2005;73(10):6822-6830.
13. Kelley TJ, Drumm ML. Inducible nitric oxide synthase is reduced in
cystic fibrosis murine and human airway epithelial cells. J Clin In-
Bacterial infections are a major clinical burden and are vest 1998;102(6):1200-1207.
key in the deterioration of respiratory function in CF. In 14. Gao L, Kim KJ, Yankaskas JR, Forman HJ. Abnormal glutathione
addition to the conventionally associated bacteria, many transport in cystic fibrosis airway epithelia. Am J Physiol 1999;
others are emerging, in part related to antibiotic pressure. 277(1 Pt 1):L113-L118.
15. Haas B, Kraut J, Marks J, Zanker SC, Castignetti D. Siderophore
New diagnostic techniques are increasing awareness of as
presence in sputa of cystic fibrosis patients. Infect Immun 1991;
yet unidentified organisms, although the clinical relevance 59(11):3997-4000.
of many of these remains to be determined. 16. Hancock RE, Speert DP. Antibiotic resistance in Pseudomonas aerugi-
The best therapy is prevention, which can be aided by nosa: mechanisms and impact on treatment. Drug Resist Updat 2000;
infection-control measures. Simple precautions to prevent 3(4):247-255.
carrying bacteria from one patient to the next are extremely 17. Oliver A, Cantón R, Campo P, Baquero F, Blázquez J. High fre-
quency of hypermutable Pseudomonas aeruginosa in cystic fibrosis
important and, for the most part, easy, whereas strict co-
lung infection. Science 2000;288(5469):1251-1254.
horting is challenging and has substantial disadvantages. 18. Pedersen SS. Lung infection with alginate-producing, mucoid Pseudo-
Appropriate and judicious use of antibiotics is critically monas aeruginosa in cystic fibrosis. APMIS Supplementum 1992;
important to limit the development of resistance and ad- 28:1-79.
verse effects in patients who undergo multiple courses of 19. Wagner VE, Iglewski BH. P.aeruginosa biofilms in CF infection.
antibiotics. Clin Rev Allergy Immunol 2008;35(3):124-134.
20. Singh PK, Schaefer AL, Parsek MR, Moninger TO, Welsh MJ,
Greenberg EP. Quorum-sensing signals indicate that cystic fibrosis
REFERENCES lungs are infected with bacterial biofilms. Nature 2000;407(6805):
762-764.
1. Davies JC. Pseudomonas aeruginosa in cystic fibrosis: pathogenesis 21. Pesci EC, Iglewski BH. The chain of command in Pseudomonas
and persistence. Paediatr Respir Rev 2002;3(2):128-134. quorum sensing. Trends Microbiol 1997;5(4):132-135.
2. Matsui H, Grubb BR, Tarran R, Randell SH, Gatzy JT, Davis CW, 22. Stone A, Saiman L. Update on the epidemiology and management of
Boucher RC. Evidence for periciliary liquid layer depletion, not Staphylococcus aureus, including methicillin-resistant Staphylococ-
abnormal ion composition, in the pathogenesis of cystic fibrosis cus aureus, in patients with cystic fibrosis. Curr Opin Pulm Med
airways disease. Cell 1998;95(7):1005-1015. 2007;13(6):515-521.
3. Saiman L, Prince A. Pseudomonas aeruginosa pili bind to asialoGM1 23. Dasenbrook EC, Merlo CA, Diener-West M, Lechtzin N, Boyle MP.
which is increased on the surface of cystic fibrosis epithelial cells. Persistent methicillin-resistant Staphylococcus aureus and rate of
J Clin Invest 1993;92(4):1875-1880. FEV1 decline in cystic fibrosis. Am J Respir Crit Care Med 2008;
4. Pier GB, Grout M, Zaidi TS, Olsen JC, Johnson LG, Yankaskas JR, 178(8):814-821.
Goldberg JB. Role of mutant CFTR in hypersusceptibility of cystic 24. Coenye T, LiPuma JJ. Molecular epidemiology of Burkholderia spe-
fibrosis patients to lung infections. Science 1996;271(5245):64-67. cies. Front Biosci 2003;8:E55-E67.
636 RESPIRATORY CARE • MAY 2009 VOL 54 NO 5BUGS, BIOFILMS, AND RESISTANCE IN CYSTIC FIBROSIS
25. LiPuma JJ, Spilker T, Gill LH, Campbell PW 3rd, Liu L, Mahenthiral- 42. Reddi K, Phagoo SB, Anderson KD, Warburton D. Burkholderia
ingam E. Disproportionate distribution of Burkholderia cepacia com- cepacia-induced IL-8 gene expression in an alveolar epithelial cell
plex species and transmissibility markers in cystic fibrosis. Am J line: signaling through CD14 and mitogen-activated protein kinase.
Respir Crit Care Med 2001;164(1):92-96. Pediatr Res 2003;54(3):297-305
26. Kalish LA, Waltz DA, Dovey M, Potter-Bynoe G, McAdam AJ, 43. McClean S, Callaghan M. Burkholderia cepacia complex: epithelial
Lipuma JJ, et al. Impact of Burkholderia dolosa on lung function and cell-pathogen confrontations and potential for therapeutic interven-
survival in cystic fibrosis. Am J Respir Crit Care Med 2006;15; tion. J Med Microbiol 2009;58(Pt 1):1-12.
173(4):421-425. 44. Shaw D, Poxton IR, Govan JR. Biological activity of Burkholderia
27. McMenamin JD, Zaccone TM, Coenye T, Vandamme P, LiPuma JJ. (Pseudomonas) cepacia lipopolysaccharide. FEMS Immunol Med
Misidentification of Burkholderia cepacia in US cystic fibrosis treat- Microbiol 1995;11(2):99-106.
ment centers: an analysis of 1,051 recent sputum isolates. Chest 45. Conway BA, Venu V, Speert DP. Biofilm formation and acyl ho-
2000;117(6):1661-1665. moserine lactone production in the Burkholderia cepacia complex. J
28. International Burkholderia cepacia Working Group. What is the In- Bacteriol 2002;184(20):5678-5685.
ternational Burkholderia cepacia Working Group? http://users. 46. Lessie TG, Hendrickson W, Manning BD, Devereux R. Genomic
ugent.be/⬃tcoenye/index_bestanden/page317.htm. Accessed March complexity and plasticity of Burkholderia cepacia. FEMS Microbiol
18, 2009. Lett 1996;144(2–3):117-128.
29. Pegues DA, Carson LA, Tablan OC, Simmons SC, Roman SB, Miller 47. Moore RA, Hancock RE. Involvement of outer membrane of Pseudo-
JM, Jarvis WR. Acquisition of Pseudomonas cepacia at summer monas cepacia in aminoglycoside and polymyxin resistance. Anti-
camps for patients with cystic fibrosis. Summer Camp Study Group microb Agents Chemother 1986;30(6):923-926.
J Pediatr 1994;124(5 Pt 1):694-702. 48. Aronoff SC. Derepressed beta-lactamase production as a mediator of
30. Sun L, Jiang RZ, Steinbach S, Holmes A, Campanelli C, Forstner J, high-level beta-lactam resistance in Pseudomonas cepacia. Pediatr
et al. The emergence of a highly transmissible lineage of cbl⫹ Pseudo- Pulmonol 1988;4(2):72-77.
monas (Burkholderia) cepacia causing CF centre epidemics in North 49. Wigfield SM, Rigg GP, Kavari M, Webb AK, Matthews RC, Burnie
America and Britain. Nat Med 1995;1(7):661-666. JP. Identification of an immunodominant drug efflux pump in Burk-
31. Goldstein R, Sun L, Jiang RZ, Sajjan U, Forstner JF, Campanelli C. holderia cepacia. J Antimicrob Chemother 2002;49(4):619-624.
Structurally variant classes of pilus appendage fibers coexpressed
50. Tablan OC, Martone WJ, Doershuk CF, Stern RC, Thomassen MJ,
from Burkholderia (Pseudomonas) cepacia. J Bacteriol 1995;177(4):
Klinger JD, et al. Colonization of the respiratory tract with Pseudo-
1039-1052.
monas cepacia in cystic fibrosis. Risk factors and outcomes Chest
32. Sajjan US, Yang JH, Hershenson MB, LiPuma JJ. Intracellular traf-
1987;91(4):527-532.
ficking and replication of Burkholderia cenocepacia in human cystic
51. Goss CH, Otto K, Aitken ML, Rubenfeld GD. Detecting Stenotro-
fibrosis airway epithelial cells. Cell Microbiol 2006;8(9):1456-1466.
phomonas maltophilia does not reduce survival of patients with cys-
33. Saini LS, Galsworthy SB, John MA, Valvano MA. Intracellular sur-
tic fibrosis. Am J Respir Crit Care Med 2002;166(3):356-361.
vival of Burkholderia cepacia complex isolates in the presence of
52. Karpati F, Malmborg AS, Alfredsson H, Hjelte L, Strandvik B.
macrophage cell activation. Microbiology 1999;145(Pt 12):3465-
Bacterial colonisation with Xanthomonas maltophilia-a retrospective
3475.
study in a cystic fibrosis patient population. Infection 1994;22(4):
34. Lamothe J, Huynh KK, Grinstein S, Valvano MA. Intracellular sur-
258-263.
vival of Burkholderia cenocepacia in macrophages is associated with
53. Graff GR, Burns JL. Factors affecting the incidence of Stenotro-
a delay in the maturation of bacteria-containing vacuoles. Cell Mi-
phomonas maltophilia isolation in cystic fibrosis. Chest 2002;121(6):
crobiol 2007;9(1):40-53.
35. Gingues S, Kooi C, Visser MB, Subsin B, Sokol PA. Distribution 1754-1760.
and expression of the ZmpA metalloprotease in the Burkholderia 54. Carmeli Y, Samore MH. Comparison of treatment with imipenem vs.
cepacia complex. J Bacteriol 2005;187(24):8247-8255 ceftazidime as a predisposing factor for nosocomial acquisition of
36. Kooi C, Subsin B, Chen R, Pohorelic B, Sokol PA. Burkholderia Stenotrophomonas maltophilia: a historical cohort study. Clin Infect
cenocepacia ZmpB is a broad-specificity zinc metalloprotease in- Dis 1997;24(6):1131-1134.
volved in virulence. Infect Immun 2006;74(7):4083-4093 55. Goss CH, Mayer-Hamblett N, Aitken ML, Rubenfeld GD, Ramsey
37. Maloney KE, Valvano MA. The mgtC gene of Burkholderia ceno- BW. Association between Stenotrophomonas maltophilia and lung
cepacia is required for growth under magnesium limitation condi- function in cystic fibrosis. Thorax 2004;59(11):955-959.
tions and intracellular survival in macrophages. Infect Immun 2006; 56. Gladman G, Connor PJ, Williams RF, David TJ. Controlled study of
74(10):5477-5486. Pseudomonas cepacia and Pseudomonas maltophilia in cystic fibro-
38. Flannagan RS, Aubert D, Kooi C, Sokol PA, Valvano MA. Burk- sis. Arch Dis Child 1992;67(2):192-195.
holderia cenocepacia requires a periplasmic HtrA protease for growth 57. Demko CA, Stern RC, Doershuk CF. Stenotrophomonas maltophilia
under thermal and osmotic stress and for survival in vivo. Infect in cystic fibrosis: incidence and prevalence. Pediatr Pulmonol 1998;
Immun 2007;75(4):1679-1689. 25(5):304-308.
39. Whitby PW, Vanwagoner TM, Springer JM, Morton DJ, Seale TW, 58. Marchac V, Equi A, Le Bihan-Benjamin C, Hodson M, Bush A.
Stull TL. Burkholderia cenocepacia utilizes ferritin as an iron source. Case-control study of Stenotrophomonas maltophilia acquisition in
J Med Microbiol 2006;55(Pt 6):661-668 cystic fibrosis patients. Eur Respir J 2004;23(1):98-102.
40. Mullen T, Markey K, Murphy P, McClean S, Callaghan M. Role of 59. Tan K, Conway SP, Brownlee KG, Etherington C, Peckham DG.
lipase in Burkholderia cepacia complex (Bcc) invasion of lung epi- Alcaligenes infection in cystic fibrosis. Pediatr Pulmonol 2002;34(2):
thelial cells. Eur J Clin Microbiol Infect Dis 2007;26(12):869-877 101-104.
41. Carvalho AP, Ventura GM, Pereira CB, Leão RS, Folescu TW, Higa 60. Krzewinski JW, Nguyen CD, Foster JM, Burns JL. Use of random
L, et al. Burkholderia cenocepacia, B. multivorans, B. ambifaria and amplified polymorphic DNA PCR to examine epidemiology of
B. vietnamiensis isolates from cystic fibrosis patients have different Stenotrophomonas maltophilia and Achromobacter (Alcaligenes) xy-
profiles of exoenzyme production. APMIS. 2007 Apr;115(4):311- losoxidans from patients with cystic fibrosis. J Clin Microbiol 2001;
318 39(10):3597-3602.
RESPIRATORY CARE • MAY 2009 VOL 54 NO 5 637BUGS, BIOFILMS, AND RESISTANCE IN CYSTIC FIBROSIS
61. Moore JE, Reid A, Millar BC, et al. Pandoraea apista isolated from 73. Armstrong DS, Nixon GM, Carzino R, et al. Detection of a wide-
a patient with cystic fibrosis: problems associated with laboratory spread clone of Pseudomonas aeruginosa in a pediatric cystic fibro-
identification. Br J Biomed Sci 2002;59(3):164-166. sis clinic. Am J Respir Crit Care Med 2002;166(7):983-987.
62. Stelzmueller I, Biebl M, Wiesmayr S, et al. Ralstonia pickettii-in- 74. Speert DP, Campbell ME, Henry DA, et al. Epidemiology of Pseudo-
nocent bystander or a potential threat? Clin Microbiol Infect 2006; monas aeruginosa in cystic fibrosis in British Columbia, Canada.
12(2):99-101. Am J Respir Crit Care Med 2002;166(7):988-993.
63. Wellinghausen N, Essig A, Sommerburg O. Inquilinus limosus in 75. Davies G, McShane D, Davies JC, Bush A. Multiresistant Pseudo-
patients with cystic fibrosis, Germany Emerg Infect Dis 2005;11(3): monas aeruginosa in a pediatric cystic fibrosis center: natural history
457-459. and implications for segregation. Pediatr Pulmonol 2003;35(4):253-
64. Olivier KN, Weber DJ, Wallace RJ Jr, Faiz AR, Lee JH, Zhang Y, 256.
et al; Nontuberculous Mycobacteria in Cystic Fibrosis Study Group. 76. Geddes DM. Of isolates and isolation: Pseudomonas aeruginosa in
Nontuberculous mycobacteria. I: multicenter prevalence study in adults with cystic fibrosis. Lancet 2001;358(9281):522-523.
cystic fibrosis. Am J Respir Crit Care Med 2003;167(6):828-834. 77. Duff AJ. Psychological consequences of segregation resulting from
65. Ziedalski TM, Kao PN, Henig NR, Jacobs SS, Ruoss SJ. Prospective chronic Burkholderia cepacia infection in adults with CF. Thorax
analysis of cystic fibrosis transmembrane regulator mutations in adults 2002;57(9):756-758.
with bronchiectasis or pulmonary Nontuberculous mycobacterial in- 78. Smyth A, Elborn JS. Exacerbations in cystic fibrosis: 3–Manage-
fection. Chest 2006;130(4):995-1002. ment. Thorax 2008;63:180-4.
79. Remmington T, Jahnke N, Harkensee C. Oral anti-pseudomonal an-
66. van Belkum A, Renders NH, Smith S, Overbeek SE, Verbrugh HA.
tibiotics for cystic fibrosis. Cochrane Database Syst Rev 2007;(3):
Comparison of conventional and molecular methods for the detec-
CD005405.
tion of bacterial pathogens in sputum samples from cystic fibrosis
80. Ratjen F. Treatment of early Pseudomonas aeruginosa infection in
patients. FEMS Immunol Med Microbiol 2000;27(1):51-57.
patients with cystic fibrosis. Curr Opin Pulm Med 2006;12(6):428-
67. Rogers GB, Carroll MP, Serisier DJ, Hockey PM, Jones G, Kehagia
432.
V, et al. Use of 16S rRNA gene profiling by terminal restriction
81. Ratjen F. Diagnosing and managing infection in CF. Paediatr Respir
fragment length polymorphism analysis to compare bacterial com-
Rev 2006;7(Suppl 1):S151-S153.
munities in sputum and mouthwash samples from patients with cys-
82. Smyth A, Walters S. Prophylactic antibiotics for cystic fibrosis. Co-
tic fibrosis. J Clin Microbiol 2006;44(7):2601-2604.
chrane Database Syst Rev 2003;(3):CD001912.
68. Rogers GB, Stressmann FA, Koller G, Daniels T, Carroll MP, Bruce 83. Stutman HR, Lieberman JM, Nussbaum E, Marks MI. Antibiotic
KD. Assessing the diagnostic importance of nonviable bacterial cells prophylaxis in infants and young children with cystic fibrosis: a
in respiratory infections. Diagn Microbiol Infect Dis 2008 Oct;62(2): randomized controlled trial. J Pediatr 2002;140(3):299-305.
133-141. 84. Wood DM, Smyth AR. Antibiotic strategies for eradicating Pseudo-
69. Carroll W, Lenney W, Wang T, Spanel P, Alcock A, Smith D. monas aeruginosa in people with cystic fibrosis. Cochrane Database
Detection of volatile compounds emitted by Pseudomonas aerugi- Syst Rev 2006;(1):CD004197.
nosa using selected ion flow tube mass spectrometry. Pediatr Pul- 85. Ryan G, Mukhopadhyay S, Singh M. Nebulised anti-pseudomonal
monol 2005;39(5):452-456. antibiotics for cystic fibrosis. Cochrane Database Syst Rev 2003;(3):
70. O’Malley CA. Infection control in cystic fibrosis: cohorting, cross- CD001021.
contamination, and the respiratory therapist. Respir Care 2009;54(5): 86. Smyth AR, Tan KH. Once-daily versus multiple-daily dosing with
641-655; discussion 656-657. intravenous aminoglycosides for cystic fibrosis. Cochrane Database
71. Saiman L, Siegel J. Infection control recommendations for patients Syst Rev 2006;3:CD002009.
with cystic fibrosis: microbiology, important pathogens, and infec- 87. Aaron SD. Antibiotic synergy testing should not be routine for pa-
tion control practices to prevent patient-to-patient transmission. Am J tients with cystic fibrosis who are infected with multiresistant bac-
Infect Control 2003;31(3 Suppl):S1-S62. terial organisms. Paediatr Respir Rev 2007;8(3):256-261.
72. Ramsey BW. To cohort or not to cohort: how transmissible is Pseudo- 88. Smyth A, Lewis S, Bertenshaw C, Choonara I, McGaw J, Watson A.
monas aeruginosa? Am J Respir Crit Care Med 2002;166(7):906- Case-control study of acute renal failure in patients with cystic fi-
907. brosis in the UK. Thorax 2008;63(6):532-535.
Discussion the risk to the caregiver who does a Perhaps people do not want to face
lot of hands-on care if they’re immu- the possibility that the staff might be
Rubin: I hope I’m not stealing any nocompetent? Are any of these things benignly colonized with these organ-
of Catherine O’Malley’s thunder, be- things that respiratory therapists isms. It’s strange that there’s so much
cause I know she’s going to talk about should be concerned about? Should infection-control strategy from the pa-
infection control and cohorting right we be routinely looking at caregivers’ tient’s perspective but very little from
after lunch. I do have a question re- flora in their nose or in their orophar- ours. Bruce, I don’t think the data are
lated to the respiratory therapist. ynx? there to provide an answer, but it’s
There’s really a concern about this something that we should not “duck,”
killer bacteria, MRSA [multiply- Davies: That’s an important point. and we are ducking it at the moment.
resistant Staphylococcus aureus]. It At my institution and many others in
sells a lot of newspapers here in the the United Kingdom, we routinely Geller: You gave a wonderful pre-
United States. We’ve had concerns, screen patients but completely ignore sentation of how smart the Pseudo-
not only with cohorting, but what is the staff who interact with the patients. monas organism is in avoiding our
638 RESPIRATORY CARE • MAY 2009 VOL 54 NO 5You can also read