Neck Circumference as a New Anthropometric Indicator for Prediction of Metabolic Syndrome in Arab Women
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
International Journal of Health Sciences and Research
Vol.11; Issue: 1; January 2021
Website: www.ijhsr.org
Original Research Article ISSN: 2249-9571
Neck Circumference as a New Anthropometric
Indicator for Prediction of Metabolic Syndrome in
Arab Women
Reem S. Albassam1,2, Nasser M. Al-Daghri3, Kai Y. Lei1
1
Department of Nutrition and Food Science, University of Maryland, College Park, MD 20742, USA.
2
Department of Community Health Sciences, College of Applied Medical Sciences, King Saud University,
Riyadh 11451, Saudi Arabia.
3
Prince Mutaib Chair for Biomarkers of Osteoporosis, Biochemistry Department, College of Science, King Saud
University, Riyadh 11451, Saudi Arabia.
Corresponding Author: Reem S. Albassam
ABSTRACT
Background: Neck circumference has been associated with obesity-related metabolic and
cardiovascular abnormality in several studies. This study designed to evaluate the potency of neck
circumference for identifying cardiometabolic risk factors, and determining the neck circumference
cutoff value for the prediction of metabolic syndrome (MetS).
Methods: This cross-sectional study involving 623 women aged 18-70 years, International Diabetes
Federation (IDF) guidelines was used to diagnose metabolic syndrome among participants. The main
indicators were neck circumference, waist circumference, body mass index, total body fat
percentage, blood pressure, total cholesterol, lipoproteins (HDLc, LDLc), triglycerides,
plasma glucose, and homeostasis model assessment-estimated insulin resistance (HOMA-IR) levels.
Results: Neck circumference was independently associated with all cardiometabolic risk factors (P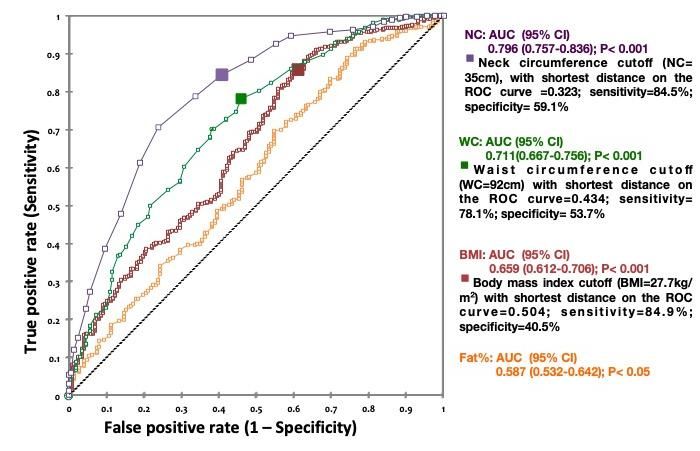
Reem S. Albassam et.al. Neck circumference as a new anthropometric indicator for prediction of metabolic
syndrome in Arab women.
pathogenesis [4]. Raised free fatty acid and its associated consequences in KSA and
concentrations are associated with insulin in the entire Gulf Cooperation Council
resistance, increased very low-density (GCC) countries.
lipoprotein cholesterol production, and
endothelial cell dysfunction [5]. The strong MATERIALS AND METHODS
correlation between SAT and Study Sample
cardiometabolic risk factors has been shown This cross-sectional survey
by the results of some [6, 7] but not all studies study was carried out between September
[8]
. Waist circumference (WC) is reported as 2014 and April 2016 in King Khalid
a cardiometabolic predictor in literature, University Hospital (KKUH) and primary
with some drawbacks. For individuals with health care centers in Riyadh, KSA. We
a body mass index (BMI) ≥35, WC adds undertook an a priori power calculation to
little to the predictive power of the disease determine the sample size required to detect
risk classification of BMI [9]. WC accuracy a small effect size (0.1) with a two-tailed, α
is limited in some situations, including = .05 and power of 80%. The analysis
pregnancy, medical conditions where there indicated a sample size of 600 would be
is distension of the abdomen (as in ascites), sufficient. This number was adjusted
or reduction of the abdomen (as with upwards to account for a possible 5%
abdominal liposuction or tummy tuck dropout rate. Of the 630 women initially
[abdominoplasty]). The main limitation of selected, seven women didn’t show up at the
the WC measure is the huge inter-ethnic second visit (laboratory). Accordingly, the
variations with certain ethnic groups and for final sample size was 623.
children and young people. Special Study recruitment was restricted to
threshold for WC is being recommended for Saudi women aged 18-70 years. We
several different populations and ethnic excluded women who were pregnant,
groups. However, the risk associated with breastfeeding or had thyroid disorders,
particular WC will differ according to organ failure, organ transplant, or cancer.
different populations [10]. This is especially Participants were selected by systematic
relevant in a country without a local cutoff random sampling from the patient list in
level, such as in Saudi Arabia each center. The women who agreed to
(KSA). Several studies have illustrated that participate were scheduled for another visit
NC may be a strong independent correlate to perform blood test, the biochemical
of metabolic risk factors than BMI and WC analysis, within 1 week. And they instructed
[11, 12]
. However, NC has also been presented to fast for 10-12 h. Informed consent was
in another study as a simple, time-saving, gained at the time of data collection after we
and cost effective measure to assess provided a full explanation of the study.
overweight and obesity in busy primary care Ethical approval for this study was
practices [13]. The available up to date cutoff given by the University of Maryland
points of NC for determining subjects with College Park Institutional Review Board
overweight, obesity, and metabolic and (IRB) (No. 411873-4) and the Ethics
cardiovascular disease risks are presented in Committee of KSU, in Riyadh, KSA (No.
the following table. The main goals of this 429679/67/4). All procedures were
study were to examine the usefulness of NC performed in accordance with the 1964
in identifying overweight, obesity, and to Declaration of Helsinki and its later
test NC application in predicting amendments.
cardiometabolic risk in Saudi adult
women. The generated data aim to aid in Data collection
providing standardized assessment tools to Data were collected using a pre-
determine accurate prevalence, treatment coded interview questionnaire that solicited
protocols, and achieve control of obesity the following information: socio-
International Journal of Health Sciences and Research (www.ijhsr.org) 22
Vol.11; Issue: 1; January 2021Reem S. Albassam et.al. Neck circumference as a new anthropometric indicator for prediction of metabolic
syndrome in Arab women.
demographics, medical history, dietary resting comfortably for 5 minutes in the
habits and practices, and physical activity seated position with back support.
and lifestyle. Standardized mercury sphygmomanometers
(Diplomat Presameter 660/360; Rudolf
Anthropometric and clinical measures Riester GmbH, Jungingen, Germany) were
Anthropometric data were taken used.
using standardized procedures and
equipment. The height was recorded to the Biochemical measures
nearest 0.5 cm. The weight was recorded to An overnight fasting (10–12 h)
the nearest 0.1 Kg, and measured without blood sample was collected from all
shoes and with light clothing. BMI was subjects. Samples were analyzed and stored
calculated by the equation: at the Biomarkers Research Program (BRP),
College of Science, KSU. All blood and
BMI = weight in Kg / (height in meters)2 serum samples were stored at −20°C until
According to the World Health analysis. Fasting plasma glucose and serum
Organization's (WHO) BMI categorization, lipids (total cholesterol, triglycerides (TG),
participants were classified into: normal and high-density lipoprotein cholesterol
weight (≤24.99 kg/m2), over-weight (25 (HDLc) were analyzed using the hexokinase
kg/m2 to 29.99 kg/m2), and obese (≥30 and colorimetric methods, (Konelab,
kg/m2) [14]. Thermo Fisher Scientific, Vantaa, Finland),
All circumferences were measured respectively. Low-density lipoprotein
using a non-stretch measuring tape, to the cholesterol (LDLc) was calculated using the
nearest 0.5 cm. NC was measured at the Friedewald formula [17].
middle of the neck, between the mid- LDL = [Total Cholesterol] - [HDLc] -
cervical spine and mid-anterior neck, ([TG]/2.2)
while the subject standing upright with their
face in the Frankfort horizontal plane, and Fasting serum insulin was
the shoulders relaxed, but not hunched determined by the
[13,15]
. WC was measured at the mid-point electrochemiluminescence method
between the highest point of the iliac crest (COBAS-E-411; Roche Diagnostics,
and the last floating rib. Hip circumference Mannheim, Germany). Insulin resistance,
was measured at the largest point of the was defined by the homeostasis model
hips. Waist-to-hip ratio (WHR) was assessment insulin index (HOMA-IR), and
calculated by dividing the waist calculated using the following equation [18]:
circumference (cm) by the hip
circumference (cm). The WHO and IDF HOMA-IR = Fasting insulin (μU/mL) X
recommended that different WC cutoff fasting plasma glucose (mmol/L) /22.5
points should be used to define central Cardiometabolic risk factors definition
obesity among different ethnic groups, and According to the IDF definition
that the Europid standards should be used in guidelines [19], the following thresholds were
our Eastern Mediterranean region until considered cardiometabolic risk:
specific national data become available. WC hypertriglyceridemia (TG ≥1.7 mmol/L),
cutoff points categorized as: >80 cm (31.5 low HDLc (1.29 mmol/L or specific
in) [16]. Body fat percentage (fat%) was treatment for this lipid abnormality),
assessed using a dual-energy X-ray hyperglycemia (fasting plasma glucose ≥5.6
absorptiometry (DEXA) scan (model: mmol/L or previously diagnosed type
Prodigy Advance, GE healthcare, Madison, 2 diabetes), hypertension (systolic BP ≥130
WI, USA). mmHg, diastolic BP ≥85 mmHg or
Blood pressure (BP) was measured treatment for previously diagnosed
using the right arm, while participant was
International Journal of Health Sciences and Research (www.ijhsr.org) 23
Vol.11; Issue: 1; January 2021Reem S. Albassam et.al. Neck circumference as a new anthropometric indicator for prediction of metabolic
syndrome in Arab women.
hypertension), and central obesity (WC ≥80 activity and lifestyle, dietary habits and
cm). Insulin resistance was defined as practice, menopausal status (premenopausal
HOMA-IR >75th percentile. vs. postmenopausal), and current estrogen
Metabolic syndrome was defined as use (no vs. yes).
per (IDF, National Heart, Lung and Blood The receiver operating characteristic
Institute [NHLBI], American Heart curve (ROC) analysis was performed to
Association [AHA], International. determine the cutoff values of NC for
Atherosclerosis Society [I AS], and predicting metabolic syndrome. The optimal
International Association for the Study of cutoff points were determined using the
Obesity [IASO]) harmonized definition shortest distance between any point on the
guidelines [16] as the presence of any three or curve and the top left corner on the y-axis.
more of the previously defined risk factors: The distance on ROC curve values were
(1) raised TG, (2) reduced HDLc, (3) raised calculated as the square root of [(1-
fasting plasma glucose, (4) raised BP, and sensitivity) 2 + (1-specificity) 2]. All
(5) central obesity. tests were 2-sided, and pReem S. Albassam et.al. Neck circumference as a new anthropometric indicator for prediction of metabolic syndrome in Arab women. P
Reem S. Albassam et.al. Neck circumference as a new anthropometric indicator for prediction of metabolic
syndrome in Arab women.
14.96) for hypertension; 15.28 (95% CI: NC quartile, after adjusting for the listed
7.95, 29.36) for elevated fasting plasma confounders (all P75th 1.31 (1.21–1.42)
CI: 3.65, 11.01) for obesity; 27.01 (95% CI: High TG 1.41 (1.29–1.53)
11.87, 61.46) for central obesity; 17.13 High Blood Pressure 1.53 (1.39–1.68)
High Fasting Glucose 1.66 (1.50–1.84)
(95% CI: 8.38, 34.99) for having two or Having 2 or more risks 1.66 (1.49–1.84)
more cardiometabolic risks; and 17.98 (95% Metabolic Syndrome
OR2 1.16 (1.08–1.26)
CI: 8.79, 36.78) for metabolic syndrome (all Low HDLc 1.19 (1.06–1.35)
P75th 1.26 (1.16–1.37)
High TG 1.38 (1.25–1.52)
age, menopausal status, and hormone use High Blood Pressure 1.48 (1.33–1.64)
(Model 2), same trends were found in the High Fasting Glucose 1.60 (1.42–1.78)
Having 2 or more risks 1.59 (1.42–1.78)
risk of the components of metabolic Metabolic Syndrome
syndrome across increasing NC quartiles, OR3 1.14 (1.03–1.26)
Low HDLc 1.20 (1.02–1.40)
except with the Q4 group for high HOMA- HOMA_IR>75th 1.25 (1.13–1.38)
IR (all P< 0.01). Women in the highest NC High TG 1.29 (1.15–1.45)
High Blood Pressure 1.70 (1.48–1.94)
quartile were 12 times more likely (95% CI: High Fasting Glucose 1.61 (1.40–1.84)
5.67, 26.47) to have two or more metabolic Having 2 or more risks 1.61 (1.10–1.85)
Metabolic Syndrome
risk factors compared to the lowest NC OR (95% CI)
quartile. Moreover, women with the highest Note: OR1: unadjusted, OR2: adjusted for age, menopausal
status, and hormonal use, eating index, activity index. OR3:
NC quartile were 13 times (95% CI: 6.35, adjusted for age, menopausal status, hormonal use, BMI, fat%,
28.23) more likely to have metabolic and WC. OR, odds ratio; CI, confidence interval; HDLc, high-
density lipoprotein cholesterol; HOMA-IR, homeostasis model
syndrome compared to those with the lowest assessment-estimated insulin resistance; TG, triglyceride.
Table 3. Logistic regression analysis of risk for metabolic syndrome and its components by quartile of neck circumference level.
OR(95% CI)
NC cm Q1 Q2 Q3 Q4
Women 38 cm
N (614) 144 172 171 127
All P-trend75th
Model 1 1 2.98(1.62–5.50)** 3.29(1.83–5.93)** 3.10( 1.63–5.84)**
Model 2 1 2.67(1.44–4.98)** 2.95(1.62–5.38)** 2.59( 1.34–5.03)**
Obesity: BMI≥ 30
Model 1 1 2.58(1.62–4.09)** 4.78(2.97–7.67)** 6.34( 3.65–11.01)**
Model 2 1 2.68(1.67–4.31)** 4.83(2.97–7.88)** 6.57( 3.69–11.70)**
Central-obesity: WC ≥ 92
Model 1 1 5.37(3.25–8.85)** 10.07(5.89–17.23)** 27.01(11.87–61.46)**
Model 2 1 4.86(2.92–8.12)** 9.07(5.25–15.67)** 23.12(10.00–53.46)**
Having two risks or more
Model 1 1 3.66(2.27–5.90)** 9.35(5.48–15.98) 17.13( 8.38–34.99)**
Model 2 1 2.89(1.74–4.79)** 7.65(4.38–13.38)** 12.57( 5.67–26.47)**
International Journal of Health Sciences and Research (www.ijhsr.org) 26
Vol.11; Issue: 1; January 2021Reem S. Albassam et.al. Neck circumference as a new anthropometric indicator for prediction of metabolic
syndrome in Arab women.
Metabolic Syndrome (harmonized)
Model 1 1 3.84(2.38–6.20)** 9.82(5.74–16.80)** 17.98(8.79–36.78)**
Model 2 1 3.06(1.84–5.08)** 8.13(4.64–14.22)** 13.39(6.35–28.23)**
Metabolic Syndrome (IDF)
Model 1 1 4.14(2.56–6.69)** 10.58(6.18–18.13)** 19.38(9.47–39.67)**
Model 2 1 3.30(1.98–5.49)** 8.83(5.04–15.49)** 14.55(6.89–30.72)**
Model 1: Unadjusted. Model 2: Adjusted for age, postmenopausal status, hormone use, dietary habits & practices, activity level & life style.
** represented significant at 0.001 level.
OR, odds ratio; CI, confidence interval; NC, neck circumference; N, number; Q, quartile; TG, triglyceride; LDLc, low- density lipoprotein
cholesterol; HDLc, high-density lipoprotein cholesterol; HOMA-IR, homeostasis model assessment-estimated insulin resistance; BMI, body
mass index; WC, waist circumference; IDF, International Diabetes Federation.
Optimal Cutoff Points to Predict cutoff value were 77%, 84.5%, and 59.1%,
Cardiometabolic Risks respectively. We determined that WC=92
Receiver operating characteristic cm, with the shortest distance in ROC
(ROC) curves were used to determine the curve=0.434, was our optimal WC cutoff
efficacy of NC as a screening measure for point. This cutoff point had sensitivity and
correctly identifying subjects with accuracy of 78.1% and 70.7%, respectively;
cardiometabolic risks and to select the specificity was 53.7%. Therefore, the
appropriate cutoff points for NC. The ROC appropriate NC and WC cutoffs to predict
curves are presented in Figure 2. For metabolic syndrome in the Saudi women
metabolic syndrome, NC showed the largest were determined as 35 cm and 92 cm,
area under the curve compared with WC, respectively. Furthermore, 27.7 kg/m2
BMI, and fat% as follows: 0.796 (0.757– emerged as the optimal cutoff point for BMI
0.836), 0.711 (0.667–0.756), 0.659 (0.612– with the shortest distance in ROC curve for
0.706), and 0.587 (0.532–0.642), predicting the presence of three or more
respectively, for NC, WC, BMI, and fat% metabolic risk factors. The distance in ROC
(all PReem S. Albassam et.al. Neck circumference as a new anthropometric indicator for prediction of metabolic syndrome in Arab women. the prevalence of metabolic syndrome, (
Reem S. Albassam et.al. Neck circumference as a new anthropometric indicator for prediction of metabolic
syndrome in Arab women.
ceridemia, hypertension, central obesity, =35 cm as the optimal cutoff value for the
metabolic syndrome, and hyperglycemia prediction of metabolic syndrome
1.2; 1.2; 1.3; 1.5; 1.6; and 1.7 times, development [24, 25, 26].
respectively. Several studies have We suggest that a WC value of 92
demonstrated similar results, showing that, cm is more appropriate for defining central
even after controlling for BMI and WC, NC obesity and predicting the presence of two
remained a significant predictor of or more metabolic risk factors in Saudi
metabolic syndrome components 1.3 to 1.9 women. This value differs from the
times [20, 15]. In our study, for women in the recommended thresholds for American (88
fourth quartile (NC >38 cm) there was cm) and European (80 cm) women by 4 and
association with increased OR for all 12 cm, respectively [19]. However, our
metabolic syndrome components. We finding concurs with the results from
observed an extremely elevated risk, as previous studies in the Arabian Gulf region,
much as 23-fold, 13-fold, and 11-fold, with in which the optimal WC cutoff for
central obesity, metabolic syndrome, and metabolic syndrome in Qatari and Iranian
hyperglycemia, respectively. In addition, women were determined [29, 30]. Other
Laakso et al. reported that women with NC studies showed that the optimal WC cutoff
in the highest quintile showed about a points for Omani and Iraqi women were
fivefold increased risk of elevated fasting 84.5 cm and 99 cm, respectively [31, 32].
glucose and a threefold increased OR of Differences in the definitions of
hypertension after adjustment for BMI [21]. metabolic syndrome and in body sizes could
Other studies established that NC in the explain the discrepancies in the optimal
highest quartile added seven-fold, eight- cutoffs of NC and WC among different
fold, or 17 fold risks to the insulin populations. As a result, ethnic-specific
resistance, obesity, and metabolic syndrome cutoff values of NC and WC are required
compared with that in the lowest quartile for the prediction of cardiometabolic
[22]
. abnormalities [19, 23, 27]. Neck circumference
is an excellent independent cardiometabolic
Neck Circumference Cutoff Points predictor, which exceeded other
The overall performance of NC, with anthropometric indices in this study on
an AUC of 0.796, in predicting metabolic Saudi women. WC, BMI, and
syndrome using the IDF criteria was better fat% have denoted lower prediction power.
than the performance of other WC could underestimate the real
anthropometric indices: WC (0.667); BMI cardiovascular risk in subjects with small
(0.659); and fat% (0.587). Few studies have stature, which may be important in many
compared the predictive power of NC with populations, such as our Arab sample [33, 34].
those of other anthropometric indices. Yan Another reason might be the different
et al. found that NC and WC shared the settings of studied populations, since our
same predictive power (NC AUC =0.73, study included subjects in their late middle
WC AUC =0.74) in women [26, 27]. However, ages to older adults, as our inclusion criteria
in Zhou et al.’s study, NC had a included subjects aged 18-70 years [26, 27].
significantly large AUC (0.703), but was For individuals with a BMI ≥ 35, WC adds
relatively lower than those for WHR little to the predictive power of the disease
(0.766); WC (0.764); and BMI (0.723) [23]. risk classification of BMI [9]. Aging women
For women, in this study, the optimal cutoff tend to gain weight and have less estrogen
point to predict metabolic syndrome was 35 protecting them against cardiovascular
cm. The optimal cutoff point reported in this diseases [35]. Fat distribution changes with
study falls within the range of 33-36 cm aging; and women develop a more central
reported in the literature of NC studies [11, 23, distribution (android shape) [35]. These
24, 25, 26, 27, 28]
. Some studies considered NC findings imply that associations between
International Journal of Health Sciences and Research (www.ijhsr.org) 29
Vol.11; Issue: 1; January 2021Reem S. Albassam et.al. Neck circumference as a new anthropometric indicator for prediction of metabolic
syndrome in Arab women.
WC and cardiometabolic risks might have guidance in identifying individuals with
been mediated by obesity (BMI, fat%) and metabolic syndrome.
aging in our sample. Consequently, ethnic-
specific cutoff points of NC should be REFERENCES
required for the prediction of metabolic 1. Graham I, Atar D, Borch-Johnsen K,
syndrome [23, 25, 26, 27], particularly for Saudi Boysen K, Burell G, Cifkova R, et al.
women. Lastly, although NC shows a strong European guidelines on cardiovascular
disease prevention in clinical practice:
association with both central obesity and executive summary: Fourth Joint Task
metabolic syndrome, the consideration of Force of the European Society of
NC as a screening test is a reasonable Cardiology and Other Societies on
approach. Women with NC < 35 cm do not Cardiovascular Disease Prevention in
require additional evaluation. Women with a Clinical Practice (Constituted by
NC above this level require an extensive representatives of nine societies and by
assessment of their metabolic and invited experts). Eur Heart J. 2007; 28(19):
cardiovascular risk. 2375–2414
Our study has its limitations; the 2. Vague J. The degree of masculine
cross-sectional nature of this study prevents differentiation of obesities: a factor
causal inferences. In this study, DEXA scan, determining predisposition to diabetes,
atherosclerosis, gout and uric calculous
which is a valid and widely used disease. Am J Clin Nutr. 1956; 4:20-34.
method, was used to assess body 3. Sjostrom CD, Håkangård AC, Lissner L,
composition. However, other reference Sjostrom L. Body compartment and
methods such as computed tomography subcutaneous adipose tissue distribution risk
(CT) scan, could be used to better quantify factor patterns in obese subjects. Obes Res.
the upper body fat in future study. Our study 1995;3:9-22
was conducted in one city, limiting the 4. Nielsen S, Guo Z, Johnson CM, Hensrud
generalization of our findings to all Saudi DD, Jensen MD. Splanchnic lipolysis in
women. However, given the significant and human obesity. J Clin Invest. 2004;
consistent associations detected in our study 113(11):1582-1588. doi:10.1172/JCI21047
and similar findings from different 5. Koutsari C, Snozek CL, Jensen MD. Plasma
NEFA storage in adipose tissue in the
populations in other studies, NC shows postprandial state: sex-related and regional
promise as an alternative marker for the differences. Diabetologia. 2008;51(11):
metabolic and cardiovascular risks 2041-2048. doi: 10.1007/s00125-008-1126-
associated with central or visceral adiposity. 5.
6. Tulloch-Reid MK, Hanson RL, Sebring NG,
CONCLUSIONS Reynolds JC, Premkumar A, Genovese DJ,
Our findings showed NC as a et al. Both subcutaneous and visceral
stronger independent predictor of metabolic adipose tissue correlates highly with insulin
and cardiovascular risks than BMI and resistance in African Americans. Obes
WC. Furthermore, for Saudi women, the Res. 2004;12(8):1352–1359.
appropriate NC that predicts three or more 7. Garg A. Regional adiposity and insulin
resistance. J Clin Endocrinol Metab.
metabolic risk factors was 35 cm. 2004;89:4206-4210.
Metabolic syndrome, obesity, and central 8. Tong J, Fujimoto WY, Kahn SE, Weigle
obesity were more prevalent in women with DS, McNeely MJ, Leonetti DL, et al.
an NC ≥35 cm. Larger NC was associated Insulin, C-peptide, and leptin concentrations
with greater risk of metabolic syndrome, predict increased visceral adiposity at 5- and
even in women with normal WC or BMI. 10-year follow-ups in nondiabetic Japanese
The current study reaffirms the importance Americans. Diabetes. 2005;54(4):985-990.
of appropriately assessing the upper body doi:10.2337/diabetes.54.4.985
obesity in screening for metabolic 9. National Research Council (US) Committee
syndrome. And it provides practical on Diet and Health. Diet and Health:
International Journal of Health Sciences and Research (www.ijhsr.org) 30
Vol.11; Issue: 1; January 2021Reem S. Albassam et.al. Neck circumference as a new anthropometric indicator for prediction of metabolic
syndrome in Arab women.
Implications for Reducing Chronic Disease ultracentrifuge. Clin Chem. 1972;18:499-
Risk. Washington (DC): National 502
Academies Press (US); 1989. 18. Bonora E, Formentini G, Calcaterra F,
10. Wang J, Thornton JC, Bari S, Williamson Lombardi S, Marini F, Zenari L, et al.
B, Gallagher D, Heymsfield S, et al. HOMA-estimated insulin resistance is an
Comparisons of waist circumferences independent predictor of cardiovascular dis-
measured at 4 sites. Am J Clin Nutr. ease in type 2 diabetic subjects prospective
2003;77(2):379-384. data from the Verona Diabetes
doi:10.1093/ajcn/77.2.379 Complications Study. Diabetes Care.
11. Stabe C, Vasques AC, Lima MM, 2002;25(7):1135-1141.
Tambascia MA, Pareja JC, Yamanaka A, et doi:10.2337/diacare.25.7.1135
al. Neck circumference as a simple tool for 19. Alberti KG, Zimmet P, Shaw J; IDF
identifying the metabolic syndrome and Epidemiology Task Force Consensus
insulin resistance: results from the Brazilian Group. The metabolic syndrome- a new
Metabolic Syndrome Study. Clin worldwide definition. Lancet. 2005;
Endocrinol (Oxf). 2013;78(6):874-881. 366(9491):1059-1062. doi:10.1016/S0140-
doi:10.1111/j.1365-2265.2012.04487.x 6736(05)67402-8
12. Ben-Noun LL, Laor A. Relationship 20. Hingorjo MR, Qureshi MA, Mehdi A. Neck
between changes in neck circumference and circumference as a useful marker of obesity:
cardiovascular risk factors. Exp Clin a comparison with body mass index and
Cardiol. 2006;11(1):14-20. waist circumference. J Pak Med Assoc.
13. Ben-Noun L, Sohar E, Laor A. Neck 2012;62(1):36-40
circumference as a simple screening 21. Laakso M, Matilainen V, Keina¨nen-
measure for identifying overweight and Kiukaanniemi S. Association of neck
obese patients. Obes Res. 2001;9(8):470- circumference with insulin resistance-
477. doi:10.1038/oby.2001.61 related factors. Int J Obes Relat Metab
14. WHO Expert Consultation. Appropriate Disord. 2002;26:873-875.
body-mass index for Asian populations and 22. Joshipura K, Muñoz-Torres F, Vergara J,
its implications for policy and intervention Palacios C, Pérez C. Neck circumference
strategies. Lancet. 2004;363(9403):157-163. may be a better alternative to standard
doi:10.1016/S0140-6736(03)15268-3 anthropometric measures. J Diabetes Res
15. Preis SR, Massaro JM, Hoffmann U, 2016:6058916. doi:
D'Agostino RB Sr, Levy D, Robins SJ, et al. org/10.1155/2016/6058916
Neck circumference as a novel measure of 23. Zhou JY, Ge H, Zhu MF, Wang LJ, Chen L,
cardiometabolic risk: the Framingham Heart Tan YZ, et al. Neck circumference as an
study. J Clin Endocrinol Metab. 2010; independent predictive contributor to
95(8):3701-3710. doi:10.1210/jc.2009-1779 cardio-metabolic syndrome. Cardiovasc
16. Alberti KG, Eckel RH, Grundy SM, Zimmet Diabetol. 2013;12:76. doi:10.1186/1475-
PZ, Cleeman JI, Donato KA, et al. 2840-12-76
Harmonizing the metabolic syndrome: a 24. Onat A, Hergenc G, Yuksel H, Can G,
joint interim statement of the International Ayhan E, Kaya Z, Dursunoglu D. Neck
Diabetes Federation Task Forceon circumference as a measure of central
Epidemiology and Prevention; National obesity: associations with metabolic
Heart, Lung, and Blood Institute; American syndrome and obstructive sleep apnea
Heart Association; World HeartFederation; syndrome beyond waist circumference. Clin
International Atherosclerosis Society; and Nutr. 2009;28:46-51.
International Association for the Study of doi:10.1016/j.clnu.2008.10.006
Obesity. Circulation. 2009; 120(16):1640- 25. Yang GR, Yuan SY, Fu HJ, Wan G, Zhu
1645. LX, Bu XL, et al. Beijing Community
doi:10.1161/CIRCULATIONAHA.109.192 Diabetes Study Group. Neck circumference
644 positively related with central obesity,
17. Friedewald WT, Levy RI, Fredrickson DS. overweight, and metabolic syndrome in
Estimation of the concentration of low- Chinese subjects with type 2 diabetes:
density lipoprotein cholesterol in plasma, Beijing Community Diabetes Study 4.
with- out use of the preparative
International Journal of Health Sciences and Research (www.ijhsr.org) 31
Vol.11; Issue: 1; January 2021Reem S. Albassam et.al. Neck circumference as a new anthropometric indicator for prediction of metabolic
syndrome in Arab women.
Diabetes Care. 2010;33(11):2465-2467. doi: mass index, waist circumference and waist-
10.2337/dc10-0798. to-hip ratio using the Framingham coronary
26. Yan Q, Sun D, Li X, Zheng Q, Li L, Gu C, heart disease risk score in an Arab
et al. Neck circumference is a valuable tool population of the Middle East. Diabetes
for identifying metabolic syndrome and Vasc Dis Res. 2008;5:304-309.
obesity in Chinese elder subjects: a 32. Mansour AA, Al-Hassan AA, Al-Jazairi MI.
community-based study. Diabetes Metab Toward establishing normal waist
Res Rev. 2014;Jan;30(1):69-76. doi: circumference in Eastern Mediterranean and
10.1002/dmrr.2464. Middle East (Arab) populations. Cutoff
27. Limpawattana P, Manjavong M, Sopapong values for waist circumference in Iraqi
R. Can Neck Circumference Predict adults. Int. J Diabetes Metab. 2007;15(1):
Metabolic Syndrome? An Experience From 14-16.
A University Community. Endocr Pract. 33. Hsieh SD, Yoshinaga H: Do people with
2016;22:8-15. similar waist circumference share similar
28. Luo Y, Ma X, Shen Y, Xu Y, Xiong Q, health risks irrespective of height? Tohoku J
Zhang X, et al. Neck circumference as an Exp Med. 1999;188(1):55-60.
effective measure for identifying cardio- 34. Ferreira-Hermosillo A, Ramírez-Rentería C,
metabolic syndrome: a comparison with Mendoza-Zubieta V, Molina-Ayala MA
waist circumference. Endocrine. 2017; Utility of the waist-to-height ratio, waist
55(3):822-830. circumference and body mass index in the
29. Bener A, Yousafzai MT, Darwish S, Al- screening of metabolic syndrome in adult
Hamaq AO, Nasralla EA, Abdul-Ghani M. patients with type 1 diabetes mellitus.
Obesity index that better predict metabolic Diabetol Metab Syndr. 2014;6(1):32. 7
syndrome: body mass index, waist pages. doi: 10.1186/1758-5996-6-32.
circumference, waist hip ratio, or waist 35. De Bold MLK. Estrogens, natriuretic
height ratio. J Obes. 2013;2013:269038. peptides and the renin-angiotensin system.
doi:10.1155/2013/269038 Cardiovasc. Res. 1999;520(41):524-531.
30. Gharipour M, Sarrafzadegan N, Sadeghi M, 36. Mahan LK, Escott-Stump S. Krause’s food,
Andalib E, Talaie M, Shafie D, et al. nutrition & diet therapy, 11th edn. Saunders,
Predictors of metabolic syndrome in the Philadelphia; 2004. p. 1319
Iranian population: waist circumference,
body mass index, or waist to hip ratio? How to cite this article: Albassam RS, Nasser
Cholesterol. 2013;2013:198384. doi: M. Al-Daghri, Kai Y. Lei. Neck circumference
10.1155/2013/198384. as a new anthropometric indicator for prediction
31. Al-Lawati JA, Barakat NM, Al-Lawati AM, of metabolic syndrome in Arab women. Int J
Mohammed AJ. Optimal cut-points for body Health Sci Res. 2021; 11(1):21-32.
******
International Journal of Health Sciences and Research (www.ijhsr.org) 32
Vol.11; Issue: 1; January 2021You can also read