IMAP Statement on Abortion Self-Care - IPPF
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
June 2021
IMAP Statement
on Abortion Self-Care
Introduction care, away from a medicalized and provider-
This statement has been prepared by the led approach, within a people-centred model
International Medical Advisory Panel (IMAP) and which empowers individuals and is supported
was approved in May 2021. by community collectives and social networks,
however still backed-up by the healthcare system
This statement supports IPPF’s commitment to whenever needed or required. This statement
improving access to abortion care for all and also serves as an advocacy tool to create an
to creating a supportive social, policy, and legal enabling environment for abortion self-care.
environment for abortion by offering guidance
and information on abortion self-care. This
is an evidence-based approach that enables Understanding abortion self-care
women, girls, and all people who have the Broadly speaking, self-care encompasses“the
capacity to become pregnant1 to realize their ability of individuals, families and communities
sexual and reproductive rights, prevent mortality to promote health, prevent disease, maintain
and morbidity associated with unsafe abortion, health, and to cope with illness and disability
and overcome coercive legal restrictions and with or without the support of a healthcare
inadequate health systems, while simultaneously provider”.i Self-care is not a new concept, nor
challenging harmful social norms and patriarchal does it apply exclusively to abortion. Health
structures. workers and health experts have been promoting
and encouraging this approach for decades, and
Guided by the existing evidence and even more so as technology increasingly supports
practices, this statement provides practical more straightforward access to information,
recommendations for IPPF Member Associations enabling individuals to make informed decisions
and other sexual and reproductive health about their health and take control over
stakeholders on how to manage abortion implementing specific health tasks.
1
This document is inclusive of women and girls and all people who can become pregnant, including intersex people, transgender men and boys, and
people with other gender identities that may have the reproductive capacity to become pregnant and have abortions. For the purposes of this document,
references to “women and girls” refer to all people who have the capacity to become pregnant.
1IMAP Statement on abortion self-care
In the field of abortion, there is not a single non-discrimination, information, and the right
way of defining self-care, yet, it is essential to to enjoy the benefit of scientific progress.iii
acknowledge that many stakeholders associate People-centred: Providing options relevant to
the concept primarily to self-administration of the individual’s needs, preferences, and lived
medical abortion. With the increasing access to experiences supports people’s self-efficacy to
highly sensitive pregnancy tests and availability control their lives and decisions and tackle
of simple, safe, highly-effective abortion abortion stigma and the silencing that comes
pills (misoprostol alone or mifepristone and with it.
misoprostol combined), more and more women Gender transformative: Every woman and
and girls have the option of safely and effectively girl has the right to abortion, in a manner
ending a pregnancy with or without the that respects their rights, autonomy, dignity,
involvement of a health provider.ii and needs, taking their lived experiences
and circumstances into account, placing
the individual at the centre, enhancing
their decision-making and control over their
IPPF understands abortion lives, and challenging gender norms, roles,
self-care as the right of women and and stereotypes that stigmatize women’s
girls to lead, in part or entirely, their reproductive autonomy.iv
abortion process, with or without Inclusiveness: All individuals who may need
an abortion must have access to care that
support from health providers2
considers their unique needs, irrespective of
visible or invisible differences.
Equity in health: All efforts should be made
to address avoidable and unjust differences
This usually includes the self-administration of in exposure to health risk factors, health
medical abortion, but could also mean being in outcomes and their social and economic
charge of other aspects of the abortion process, consequences, healthcare access, and capacity
such as the post-abortion care or the decision of to finance care.v
engaging (or not) other stakeholders throughout Quality: Care delivered should be in line with
the process (i.e., abortion doulas;3 peers; the available evidence and the needs, values,
pharmacists). and preferences of the clients, free of stigma
and with compassion and empathy.
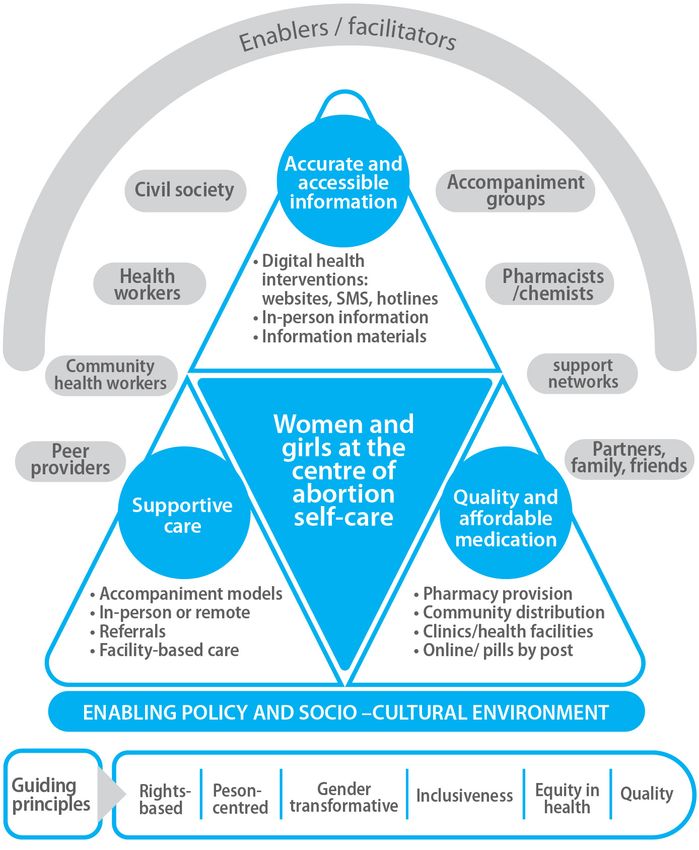
Abortion self-care is underpinned by the
following principles: Abortion self-care places women and girls firmly
at the centre of the abortion process, as the
Rights-based: Bodily integrity and autonomy key decision makers in control of their bodies.
is a fundamental human right, central to However, multiple stakeholders can also play a
sexual rights and gender and reproductive role in enabling and facilitating this approach,
justice. People’s right to make autonomous by acting on three components of support for
decisions about their own bodies and abortion self-care: a. Delivery of accurate and
reproductive functions, is at the core of their accessible information; b. Access to quality
fundamental rights to life, health, equality and and affordable medication; and c. Provision of
supportive care:vi
2
Individuals who face spontaneous abortions, incomplete abortion, and intrauterine foetal demise may also decide to lead – when considered safe and
based on the specificities of the case – parts of the abortion process.
3
Individuals trained to provide emotional, physical, and informational support, free of stigma, during and after an abortion procedure.
2IMAP Statement on abortion self-care
Women and girls have access to quality
medical abortion pills, either misoprostol
alone or a combipack of mifepristone and
misoprostol.
Women and girls have the conditions to
implement the abortion with the desired level
of privacy.
The World Health Organization
recommends that up to 12 weeks
gestation, individuals can self-
administer mifepristone and
misoprostol medication without
the direct supervision of a health
provider.viii
An important condition for safety of self-
induced abortion is the ability to self-determine
Abortion self-care: safe, effective, wanted! gestational age. Evidence has shown that
Emerging research suggests that abortion outside women, in different contexts, geographies,
the medical setting is an overall safe, effective, socio-economic, and educational levels, are
and wanted way to end a pregnancy. reasonably good at estimating gestational age
based on their last menstrual period (LMP),
Safety without the need for a physical examination or
The safest environment for self-managed an ultrasound.ix Some women in specific personal
abortion is one where: or medical conditions may have challenges
estimating gestational age, in which case they
Women and girls’ health literacy is supported. may benefit from clinic or laboratory support.
That is, their capacity to obtain, process,
and understand evidence-based health Recommended resources: for more information on
information, explore their options, ask critical the evidence supporting self-administered medical abortion and
questions about their choices, and actively protocols, see the following WHO guidelines:
participate in decisions and tasks concerning
their care. • Health worker roles in providing safe abortion care
Medical care is accessible when chosen and and post-abortion contraception https://www.who.
needed, with referral mechanisms in place for int/reproductivehealth/publications/unsafe_abortion/
women to access in-clinic care, including in abortion-task-shifting/en/
case of complications or for complementary • Medical Management of Abortion https://www.who.int/
services.vii reproductivehealth/publications/medical-management-
abortion/en/
3IMAP Statement on abortion self-care
Effectiveness information on how to safely self-manage
The statement is aimed at service providers, an abortion — are deeply appreciated
advocates, programme staff, managers and by women who self-administer medical
volunteers in IPPF Member Associations and abortion and may provide the technical
the secretariat, and other SRHR and women’s information and emotional support that can
organizations. ensure safe, complete abortions with few
or no complications.xv Similarly, research has
A recent systematic scoping review of peer found that community-based distribution of
reviewed research found that studies reporting misoprostol – which enables abortion self-care
on self-managed medication abortion reported – can safely and effectively support abortion
high-levels of effectiveness.x care.xvi
The effectiveness of specific self-care abortion
interventions has also been documented by
Abortion hotlines and websites
recent studies:
have been shown to be highly
Most women and girls who self-manage their effective in facilitating self-
abortions facilitated through pharmacies managed abortions, as most
report high effectiveness without surgical women do not present any
interventions and are willing to use this
complications nor require surgical
service again if need be. The challenge with
this model is with regard to the quality of intervention after taking the
the information provided by pharmacists, abortion pills. These information
especially related to timing and dosing of the hubs have proved to have a positive
medication (usually, misoprostol). Therefore, impact on access to safe abortion
more work needs to be done in terms of
for women, both in legal as well as
equipping pharmacists and drug sellers with
the correct information.xi xii in legally restricted contexts.xvii
A study conducted in Uruguay showed that
services provided under a model known as
“the harm reduction model” – in which Often, a wanted alternative
providers offer evidence and rights-based Evidence suggests that in some settings as much
information and care before and after an as 70% or 80% of abortions are self-managed.xviii
abortion, to the extent allowed by the In legally or socially restrictive settings, or for
law, and women and girls self-manage the those living in humanitarian settings, abortion
procedure itself, in other words, taking the self-care may not always be the preferred option,
abortion pills – contributed to a reduction but the only available option.
in maternal mortality.xiii A study conducted
at the Buguruni Health Centre in Tanzania – A robust body of qualitative studies show that
which adapted the harm reduction model to abortion self-care is often a wanted alternative
the local context – showed that these type for some women; because it is affordable, it
of services are feasible and acceptable, and implies reduced transportation needs, ease of
could provide an opportunity to reduce unsafe scheduling, earlier intervention in the pregnancy,
abortion.xiv privacy, reduced stigma, sense of control,
Research also indicates that accompaniment comfort, and easier access for people with
groups – networks of activists/volunteers/ restricted mobility (e.g. from refugees to people
peers which provide people with step-by-step with disabilities).xix xx xxi xxii
4IMAP Statement on abortion self-care
What abortion self-care is not Recommendations for Member
Abortion self-care is not an approach that Associations and other organizations on
removes the duty of care away from the how to support abortion self-care
formal health system. The formal health
system must facilitate access to information, 1. Transform policy and legislation to create an
services, commodities, and referrals, as enabling environment for abortion self-care as
needed and wanted, within the national legal part of a supportive health system for abortion
and policy framework. care.
Abortion self-care is not an approach driven Advocate with governments to remove
by the aim of reducing costs for the health abortion from the penal code and end criminal
system. While it is true that studies on self- penalties for women who self-manage their
care interventions highlight their potential abortion process.
to save resources both for users and the Advocate to ensure that national regulations
healthcare system,xxiii abortion self-care should and guidelines explicitly integrate self-
be strongly guided by a people-centred managed abortion as a legitimate and
approach and existing evidence on its safety permissible pathway to abortion care.
and effectiveness. Work with governments to ensure the
Abortion self-care is not an approach that availability and accessibility of quality medical
undermines or eliminates advocacy efforts abortion products with the inclusion of
to expand legal access to abortion. The mifepristone and misoprostol in policy and
decriminalization of abortion is still essential to service guidance documents, lists of essential
ensure that all individuals can realize the right medicines, and procurement catalogues.
to a safe and dignified abortion, on their own Advocate for medical abortion products to be
terms and informed by the values and needs free or subsidized for poor and marginalized
most important to them, and to guarantee populations.
that health workers can perform their duty of Advocate for the withdrawal of unnecessary
care without fear of prosecution. regulations on the provision of medical
Abortion self-care is not an approach limited abortion products, and advocate for over-the-
to legally restricted settings or humanitarian counter sale of medical abortion drugs.
settings. However, in such settings, it can Work with governments to expand access
play a significant role in increasing access, to generic formulations of medical abortion
reducing mortality and morbidity associated products and promote public-sector availability
to unsafe procedures, and transforming and competitive pricing in the private
negative abortion narratives and stigma. marketplace, including innovations in retail-
Even in contexts with legal, quality, and market options, such as bundling pregnancy
comprehensive services widely available, some tests and medical abortion products.xxii
women and girls may prefer or need abortion Advocate for eradicating censorship of
self-care. A concrete example is in the context online evidence-based abortion information
of the COVID-19 pandemic, as women and to improve individuals’ ability to make safe
girls have seen their mobility restricted, choices in any place and any context.
affecting their capacity to access facility-based Advocate for the implementation of service
abortion care. delivery strategies that eliminate access
barriers for women and girls who decide
to involve health providers in the abortion
process. Self-care can be complemented with,
5IMAP Statement on abortion self-care
for example, task sharing to mid-level health Engage students of health-related professions
workers or with telemedicine guided clinical or in dialogues around self-care. This contributes
emotional support, supervision, or counselling. to long-term change, gradual transformation
of the provider-client relationship, and de-
2. Improve knowledge and attitudes around medicalization of issues that, while health-
abortion self-care and catalyse sociocultural related, have the potential to be managed
change by creating positive narratives and social outside the health system.
movements to remove stigma. Educate the medical community about
Develop public campaigns to increase health the safety and effectiveness of abortion
literacy regarding abortion care and to inform self-care, in order to reduce unnecessary
individuals about their right to manage their clinical concern, overmedicalization and
care, based on the available evidence and overtreatment of clients, and stigmatization
within the restrictions of their legal context. or criminalization of women seeking abortion
Information should be made available in local care.
languages and in a format that supports Support community engagement initiatives
the needs/information-seeking practices of that could help to build trust in the systems/
overlooked populations, such as women with structures that enable and facilitate abortion
disabilities, refugees, indigenous women, and self-care, i.e. work with community leaders
sex workers, among others. and local media to ensure they are supportive
Develop positive messaging and narratives of locally-led accompaniment groups.
on abortion self-care, including response to Participate in forums that aim to catalyse
concerns or opposition to abortion self-care sustainable social change for women and
from a range of actors. This could include normalize and facilitate abortion self-care.
developing factsheets to address common
myths and misconceptions, and using 3. Implement person-centred, on-demand models
evidence and rights-based arguments to of care that support and enable an individual
counter opposition. throughout an abortion self-care experience.
Include content on agency, abortion self- Through collaboration with legal experts,
care, abortion stigma as part of evidence- assess your legal framework to understand
based comprehensive sexuality education how the regulatory framework supports or
programmes and outreach to young people. restricts abortion self-care initiatives. Any
Implement participatory processes to restrictions should be understood in order to
gather the stories of individuals who have create risk mitigation strategies while, at the
experienced abortion self-care, as well as of same time, supporting women and girls in
those who have played a role in enabling and their abortion process.
facilitating abortion self-care. Disseminate Map existing interventions that enable or
these stories in relevant spaces. limit abortion self-care in your geographical
Engage partner organizations, including areas of operation. Avoid duplication of
feminist groups, professional bodies of efforts by partnering with other like-minded
health providers, and nursing and medical stakeholders.
institutions, to create a diverse network of Review your organization’s existing
champions for abortion self-care. strengths, initiatives, and models of care
Generate safe spaces for dialogue between and consider how they can be adapted
health workers and groups leading the to integrate components of support for
conversation on and implementation of abortion self-care. For example, a strong
abortion self-care, to discuss challenges and network of community health workers could
opportunities for collaboration. be leveraged to create an accompaniment
6IMAP Statement on abortion self-care
network for abortion self-care. An existing address other sexual and reproductive health
hotline model or telemedicine service could needs before, during, or after their abortion.
be adapted to include a dedicated team Collect data on the safety, effectiveness, and
providing information and support for women acceptability of self-care interventions to
undertaking abortion self-care. improve programming and support advocacy
Based on the outcomes of mapping and efforts. This can include operational research
assessment work, develop interventions to on how to improve women’s experience of
provide on-demand support for individuals self-managed abortion, how to overcome
who choose abortion self-care through barriers and challenges to facilitating
innovative approaches, considering the three abortion self-care, and the contribution
main components of support for self-care: of abortion self-care to reducing abortion
• Delivery of accurate and accessible stigma, increasing self-efficacy, and catalysing
information on abortion and, particularly, sociocultural change.
on medical abortion (dosage, regimen,
contraindications, side effects, and
signs of complications). Strategies may
Special consideration should be
include hotlines, peer provision, websites,
or referral to other reliable sources of made when supporting abortion
information and support. self-care to vulnerable groups,
• Access to quality medical abortion pills. including very young adolescents;
Strategies may include digital prescriptions, women with disabilities; sex
partnership with pharmacists, and sending
workers; women subject to gender-
pills by post or dispensed by community
health workers. based violence; transgender or
• Providing supportive care during the trans men; and women subject to
self-care process. Strategies may include human trafficking.
adaptation of clinical protocols to ensure
readiness to meet the needs of a woman at
any point in her abortion process; provision
of on-demand abortion counselling when 4. Recommendations on abortion self-care during
requested; and setting up referral networks the COVID-19 pandemic and humanitarian crises.
in case of doubts or for treatment of Ensure that supply chains that support
complications, post-abortion care, or other the distribution of abortion pills remain
relevant services, as needed. operational.
Strengthen the capacity of your organization Build alliances with humanitarian actors for
to undertake abortion self-care programming. the delivery of medical abortion supplies
For example, update institutional policies and and contraceptives, as well as accurate and
guidelines on abortion to include self-care, comprehensive information on the use of
conduct values clarification exercises for staff abortion pills.
and volunteers at all levels to build support Accelerate the development of digital
and commitment for abortion self-care, and initiatives focused on providing evidence-
provide training for health providers on how based information on abortion and
to provide person-centred care for a woman abortion-related services, to ensure women´s
self-managing an abortion. reproductive choices are not undermined as a
Clinical, psychosocial, and protection services result of circumstances that limit their mobility.
must be available for vulnerable groups to
7IMAP Statement on abortion self-care
Recommended resources Mbizvo (Chair), Janet Meyers, and Professor
• Her in charge - Medical abortion and women’s lives - A Hextan Yuen Sheung Ngan for their valuable and
call for action https://www.ippf.org/resource/her-charge- timely guidance and reviews offered during the
medical-abortion-and-womens-lives-call-action development process.
• IPPF’s Medical Abortion Commodities Database http://
medab.org/ Who we are
• Self-care interventions communications toolkit https:// The International Planned Parenthood Federation
www.who.int/reproductivehealth/self-care-interventions/ (IPPF) is a global service provider and a leading
WHO-Self-Care-SRHR-Comms_Kit.pdf advocate of sexual and reproductive health and
• WHO consolidated guideline on self-care interventions rights for all. We are a worldwide movement
for health: sexual and reproductive health and rights of national organizations working with and for
https://www.who.int/reproductivehealth/publications/ communities and individuals
self-care-interventions/en/
• Evidence-based information websites: www. IPPF
womenonweb.org, www.womenhelp.org, www. 4 Newhams Row
safe2choose.org. London SE1 3UZ
United Kingdom
IPPF, as a global service provider and leading tel: +44 20 7939 8200
advocate of sexual and reproductive health care, fax: +44 20 7939 8300
pledges to uphold its commitment to providing email: info@ippf.org
gender‑sensitive and rights‑based comprehensive www.ippf.org
abortion care to all, and to working in partnership
with others to ensure that the conditions and UK Registered Charity No. 229476
structures are in place to help women access safe
abortion in the way that works best for their lives. Published June 2021
Acknowledgements
We would like to express our appreciation to
Marcela Rueda Gomez and Josephine Mugishagwe
from IWORDS Global and Rebecca Wilkins for
drafting this statement, and to Dr France Anne
Donnay, Professor Kristina Gemzell Danielsson,
Dr Raffaela Schiavon, Professor Oladapo Alabi
Ladipo, Professor Michael Mbizvo, and Professor
Hextan Yuen Sheung Ngan for providing technical
input and guidance as the lead reviewers. We are
also grateful to Seri Wendoh, Karthik Srinivasan,
Manuelle Hurwitz, IPPF Programme Directors and
other IPPF Member Association and Secretariat
colleagues for their input and review of this
document. Finally, we gratefully acknowledge
the support from IPPF’s International Medical
Advisory Panel (IMAP): Dr Ian Askew, Anneka
Knutsson, Dr France Anne Donnay, Professor
Kristina Gemzell Danielsson, Dr Raffaela Schiavon,
Professor Oladapo Alabi Ladipo, Professor Michael
8IMAP Statement on abortion self-care
References xiii
Labandera A., Gorgoroso M., and Briozzo L. (2016)
i
World Health Organization (2021) Self-care interventions for ‘Implementation of the risk and harm reduction strategy
health. Available at: https://www.who.int/health-topics/self- against unsafe abortion in Uruguay: From a university hospital
care#tab=tab_1 (Accessed: 21 April 2021). to the entire country’, International Journal of Gynecology and
ii
Ipas (2021) Abortion self-care. Available at: https://www.ipas. Obstetrics, 134 (1), pp. S7-S11 doi: https://doi.org/10.1016/j.
org/our-work/abortion-self-care/ (Accessed: 21 April 2021). ijgo.2016.06.007
iii
UN General Assembly (1966) International Covenant on Civil and xiv
Kahabuka C., Pembe A., and Meglioli A. (2016) ‘Provision of
Political Rights. Available at: www.refworld.org/docid/3ae6b3aa0. harm-reduction services to limit unsafe abortion in Tanzania’,
html (Accessed: 23 April 2021). International Journal of Gynecology and Obstetrics, 136, pp. 210-
iv
International Planned Parenthood Federation (2017) Gender 214 doi: 10.1002/ijgo.12035
Equality Strategy. Available at: https://www.ippf.org/resource/ippf- xv
Zurbriggen R., Keefe-Oates B., Gerdts C. (2018)
2017-gender-equality-strategy (Accessed: 21 April 2021) ‘Accompaniment of second-trimester abortions: the model
v
World Health Organization (2021) Social determinants of of the feminist Socorrista network of Argentina’, Elsevier
health. Available at: https://www.who.int/health-topics/social- Incorporated, 97 (2), pp. 108-115 doi: https://doi.org/10.1016/j.
determinants-of-health#tab=tab_3 (Accessed: 21 April 2021) contraception.2017.07.170
vi
Pizzarossa L., and Nandagiri R. (2021) ‘Self-managed abortion: xvi
Foster A., Arnott G., Hobstetter M. (2017) ‘Community-based
a constellation of actors, a cacophony of laws?’, Sexual and distribution of misoprostol for early abortion: Evaluation of a
Reproductive Health Matters, 29(1), pp. 1-8 https://doi.org/10.10 program along the Thailand-Burma border’, Contraception, 96 (4)
80/26410397.2021.1899764 doi: 10.1016/j.contraception.2017.06.006.
vii
Conti J., Cahill E. (2019) ‘Self-managed abortion’, Current xvii
Drovetta, R. (2015) ‘Safe abortion information hotlines: An
Opinion in Obstetrics and Gynaecology, 31(6), pp. 435-440. effective strategy for increasing women’s access to safe abortions
doi:10.1097/GCO.0000000000000585 in Latin America’, Reproductive Health Matters, 23(45), pp. 47-57
viii
World Health Organization (2018) Medical management doi: https://doi.org/10.1016/j.rhm.2015.06.004
of abortion. Available at: https://www.who.int/ xviii
Singh S. (2018) ‘The incidence of abortion and unintended
reproductivehealth/publications/medical-management-abortion/ pregnancy in India, 2015’, 6(1), pp. 111-120 doi: https://doi.
en/#:~:text=Medical%20management%20of%20abortion%20 org/10.1016/S2214-109X(17)30453-9
generally,effective%20and%20acceptable%20abortion%20care xix
Wainwright, M., Colvin, C., Swartz, A., Leon, N. (2016)
(Accessed: 21 April 2021). ‘Self-management of medical abortion: a qualitative evidence
ix
Schonberg D., et al. (2014) ‘The accuracy of using last menstrual synthesis’, Reproductive Health Matters, 24 (47). pp. 155-167
period to determine gestational age for first trimester medication doi: https://doi.org/10.1016/j.rhm.2016.06.008
abortion: a systematic review, Contraception, 90(5), pp. 480-487 xx
Assis M. and Larrea, S. (2020) ‘Why self-managed abortion is
doi: 10.1016/j.contraception.2014.07.004 so much more than a provisional solution for times of pandemic’,
x
Moseson H., et al. (2020) ‘Self-managed abortion: A systematic Sexual and Reproductive Health Matters, 28(1) doi: https://doi.org
scoping review’, Best Practice & Research Clinical Obstetrics & /10.1080/26410397.2020.1779633
Gynaecology, 63, pp. 87-110 doi: https://doi.org/10.1016/j. xxi
Baiju N. et al. (2019) ‘Effectiveness, safety and acceptability
bpobgyn.2019.08.002 of self-assessment of the outcome of first-trimester medical
xi
Stillman M, et al. (2020) ‘Women’s self-reported experiences abortion: a systematic review and meta-analysis’, BJOG, 126, pp.
using misoprostol obtained from drug sellers: a prospective 1536-1544 doi: http://dx.doi.org/10.1111/1471-0528.15922
cohort study in Lagos State, Nigeria’, BMJ Open, 10(e034670), xxii
Moseson H., et al. (2020) ‘Self-managed abortion: A systematic
pp. 1-10 doi: http://dx.doi.org/10.1136/bmjopen-2019-034670 scoping review’, Best Practice & Research Clinical Obstetrics &
xii
Tamang A., Puri M., Lama K., Shrestha P. (2014) ‘Pharmacy Gynaecology, 63, pp. 87-110 doi: https://doi.org/10.1016/j.
workers in Nepal can provide the correct information about using bpobgyn.2019.08.002
mifepristone and misoprostol to women seeking medication to xxiii
Remme M., et al. (2019) ‘Self-care interventions for sexual and
induce abortion’, Reprod Health Matters, 22 (44 Suppl 1) ,pp. reproductive health and rights: costs, benefits, and financing’,
104-15 doi: https://doi.org/10.1016/s0968-8080(14)43785-6 BMJ, 365 (l1228), doi: doi: https://doi.org/10.1136/bmj.l1228
9You can also read