North East London (NEL) Management of Infection Guidance for Primary Care
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
North East London (NEL) Management of Infection Guidance for Primary Care
Adapted from the Public Health England (PHE) and National Institute for Health and Care Excellence (NICE) Management of infection guidance. For primary
care for use across the East London Health and Care Partnership (ELHCP)
These guidelines have been developed in collaboration with:
• Barking, Havering and Redbridge University NHS Trust (BHRuT)
Microbiology team
• Barts Health NHS Trust Microbiology teams
• Homerton University Hospital NHS Foundation Trust Microbiology
team (HUHFT)
• NHS North East London Foundation NHS Trust (NELFT)
• NHS East London Foundation Trust (ELFT)
• NHS Barking and Dagenham, NHS Havering and NHS Redbridge
(BHR) Clinical Commissioning Groups (CCGs)
• NHS City and Hackney (C&H) CCG
• NHS Newham CCG
• NHS Tower Hamlets CCG
• NHS Waltham Forest CCG
The guideline review group has involved a range of healthcare
professionals including GPs, Microbiologists/Infectious disease
consultants, Primary Care Pharmacists, Prescribing Advisors, and
Antimicrobial Pharmacists. Advice has also been sought from local
dermatologists, obstetricians and gastroenterologists where
appropriate.
https://asweknowitlife.wordpress.com/2012/12/04/antibiotic-resistance-cycle/ The development and maintenance of this guideline is a key function of
the North East London Antimicrobial Resistance Strategy Group (NEL
Updated: October 2020 AMRSG), which is a local collaboration of health and social care
Date of review: October 2021, or sooner if required partners.
Version: 1.2
1|Page
Contents
Page
No.
Guideline Statement, Aims and Objectives 3
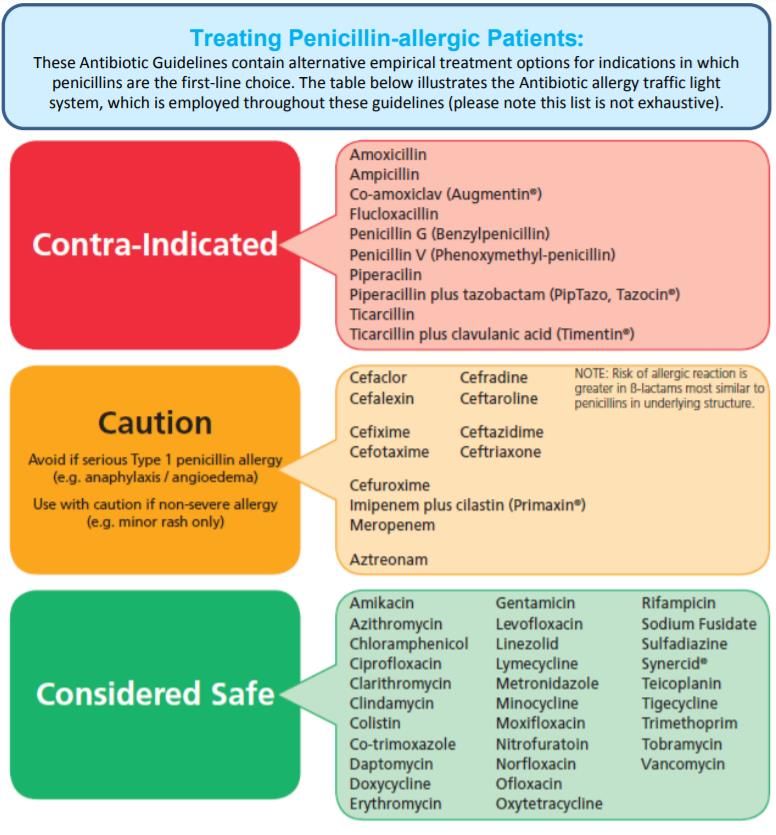
Antimicrobial Prescribing Guidance / Treating Penicillin-Allergic Patients 4
Upper respiratory tract infections 5
Lower respiratory tract infections 7
Urinary tract infections 12
Meningitis 17
Gastrointestinal tract infections 17
Genital tract infections 20
Skin and soft tissue infections 23
Eye Infections 30
Suspected dental infections (outside dental settings) 30
Information for Patients 32
Notification for Diseases 35
Other References and Useful Links 36
Key Contacts and Guideline Review Group 37
Document Version Control 38
Date ratified by
Organisations who have adopted this document
organisation
NHS Barking and Dagenham, NHS Havering and NHS Redbridge (BHR) Clinical Commissioning Groups 17th November 2020
NHS Waltham Forest, NHS Newham, and NHS Tower Hamlets (WEL) Clinical Commissioning Groups 28th October 2020
NHS City and Hackney (C&H) Clinical Commissioning Group 9th November 2020
*Endorsed by North East London Antimicrobial Resistance Strategy Group (NEL AMRSG) 28th October 2020*
2|Page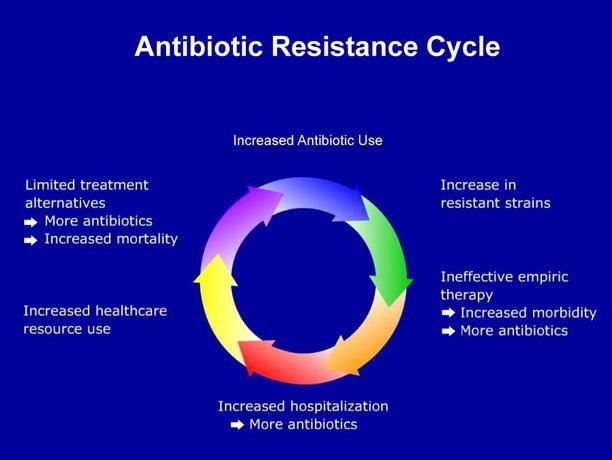
Guideline Statement
These guidelines are to be read in conjunction with current guidance from NICE and PHE, other national bodies (e.g. BASHH – British Association for Sexual
Health and HIV), relevant NICE Clinical Knowledge Summaries (CKS) and resources from the RCGP TARGET Toolkit. Evidence-based antimicrobial prescribing
is essential to begin to address the challenge of increasingly antibiotic-resistant bacteria, and the rise in health care acquired infections. The Health and Social
Care Act 2008 (updated 2011) introduces the Code of Practice for the Prevention and Control of HealthCare Associated Infections, also known as the Hygiene
Code. This Code requires all health care organisations to have a policy in place on antimicrobial prescribing, in order to reduce the incidence and prevalence of
Health Care Associated Infections (HCAI). Where possible, treatment is based on national guidance (Public Health England: Management of infection guidance
for primary care for consultation and local adaptation). Local adaptation has been applied where required on advice of the local acute trusts department of
infection, based on local sensitivities and resistance patterns.
Infections account for a large proportion of the acute workload seen in general practice and cause considerable patient distress. The prescriber is sometimes
put under pressure to prescribe by patients who perceive that antibiotics will provide quick resolution, particularly if they are under pressure to return to work.
However, the evidence to support antibiotic treatment is often weak or lacking, and certain illnesses can be self-limiting. Good communication between the
prescriber and patient, with adequate time given to the consultation, is known to bring about more selective and appropriate prescribing
Aims and Objectives of the Guidance
The aims are to:
• Support the rational, safe and cost-effective use of antibiotics by selecting the best approach to managing common infections from the evidence
available.
• Promote the selective use of antibiotics to reduce the emergence of antimicrobial resistance in the community.
• Empower patients with information and support mechanisms so they can cope with their infection.
The objectives are to:
• Assist prescribers in managing individuals with infections by providing clear information on the likely clinical outcome with or without treatment and to
indicate possible risk.
• Help the prescriber decide whether or not antibiotic treatment is indicated and which antibiotic is the most appropriate.
This guidance should always be applied in conjunction with clinical judgement and consideration of important
individual case factors including allergy, pregnancy, drug interactions and drug safety advice from the MHRA. The
recommendations apply only in the absence of contra- indications. Please refer to the latest BNF, BNFc or Summary
of Product Characteristics (SmPC) for further information
3|Page
Antimicrobial prescribing guidance – managing common infections
• For all PHE guidance, follow PHE’s principles of treatment
• See BNF for appropriate use and dosing in specific populations,
for example, hepatic impairment, renal impairment, pregnancy
and breastfeeding.
Click symbols to
access doses
Key
for children
Click to access
NICE’s printable
visual summary
The strength of each PHE recommendation is qualified by a letter in
parenthesis. This is an altered version of the grading recommendation
system used by SIGN
RECOMMENDATION
STUDY DESIGN GRADE
Good recent systematic review and meta-
A+
analysis of studies
One or more rigorous studies; randomised
A-
controlled trials
One or more prospective studies B+
One or more retrospective studies B-
Non-analytic studies, for example case
C
reports or case series
Formal combination of expert opinion D
Abbreviations
BD, twice a day; eGFR, estimated glomerular filtration rate; IM,
intramuscular; IV, intravenous; MALToma, mucosa-associated lymphoid
tissue lymphoma; m/r, modified release; MRSA, methicillin-resistant
Staphylococcus aureus; MSM, men who have sex with men; stat, given
immediately; OD, once daily; TDS, 3 times a day; QDS, 4 times a day.
4|PageDoses Visual
Infection Key points Medicine Length
Adult Child summary
Upper respiratory tract infections
Advise paracetamol, or if preferred and suitable, First choice: 500mg QDS or
Acute sore 5 to 10 days
ibuprofen for pain. phenoxymethylpenicillin 1000mg BD
throat
OTC Medicated lozenges may help pain in adults. Penicillin allergy:
250mg to 500mg BD 5 days
Use FeverPAIN or Centor to assess symptoms: clarithromycin OR
FeverPAIN 0-1 or Centor 0-2: no antibiotic; erythromycin (preferred if 250mg to 500mg 5 days
FeverPAIN 2-3: no or back-up antibiotic; pregnant) QDS or
FeverPAIN 4-5 or Centor 3-4: immediate or 500mg to 1000mg
back-up antibiotic. (erythromycin or BD
Public Health Systemically very unwell or high risk of clarithromycin only
England complications: immediate antibiotic. needed for 5 days as they
Avoid broader-spectrum penicillins (e.g. have a broader spectrum of
amoxicillin) for the empirical treatment of sore activity than
Last updated: throat. phenoxymethylpenicillin
Jan 2018 For detailed information click the visual summary icon.
and more likely to drive
bacterial resistance)
Influenza Annual vaccination is essential for all those ‘at risk’ of influenza. 1D Antivirals are not recommended for healthy adults.1D,2A+
Treat ‘at risk’ patients with 5 days oseltamivir 75mg BD,1D when influenza is circulating in the community, and ideally within 48 hours of onset (36 hours
for zanamivir treatment in children),1D,3D or in a care home where influenza is likely.1D,2A+
Public Health At risk: pregnant (and up to 2 weeks post-partum); children under 6 months; adults 65 years or older; chronic respiratory disease (including COPD and
England asthma); significant cardiovascular disease (not hypertension); severe immunosuppression; chronic neurological, renal or liver disease; diabetes
mellitus; morbid obesity (BMI>40).4D See the PHE Influenza guidance for the treatment of patients under 13 years.4D In severe immunosuppression, or
Last updated: oseltamivir resistance, use zanamivir 10mg BD5A+,6A+ (2 inhalations twice daily by diskhaler for up to 10 days) and seek advice.4D
Feb 2019
Access supporting evidence and rationales on the PHE website.
Prompt treatment with appropriate antibiotics Phenoxymethylpenicillin Not available.
Scarlet fever 2D 500mg QDS2D 10 days3A+,4A+,5A+ Access
significantly reduces the risk of complications.1D
(GAS) supporting
Vulnerable individuals (immunocompromised, the Penicillin allergy: evidence and
Public Health comorbid, or those with skin disease) are at 500mg OD 5 days (NICE)
Azithromycin rationales on the
England increased risk of developing complications.1D Optimise analgesia2D and give safety netting advice PHE website
Scarlet fever is a notifiable disease, health professionals must inform local health protection teams of suspected cases.
Last updated:
Oct 2018
North East and North Central London Health Protection Team (NENCLHPT) numbers:
NICE CKS • Daytime Tel: 020 3837 7084 (option 2)
update Mar 2020 • For Out of Hours Advice: Tel: 0151 909 1215 (between 5pm and 9am and during weekends and Bank Holidays)
• Email: necl.team@phe.gov.uk ; phe.nenclhpt@nhs.net
5|PageDoses Visual
Infection Key points Medicine Length
Adult Child summary
Acute otitis Regular paracetamol or ibuprofen for pain (right First choice: amoxicillin - 5 to 7 days
media dose for age or weight at the right time and Penicillin allergy:
maximum doses for severe pain). -
clarithromycin OR
Otorrhoea or under 2 years with infection in 5 to 7 days
erythromycin (preferred if
both ears: no, back-up or immediate antibiotic. -
Public Health pregnant)
England Otherwise: no or back-up antibiotic. Second choice: 5 to 7 days
Systemically very unwell or high risk of co-amoxiclav
complications: immediate antibiotic. -
Last updated: Feb
2018 For detailed information click on the visual summary.
Second line:
First line: analgesia for pain relief,1D,2Dand apply OTC (>12yrs) topical acetic 1 spray TDS5A- 7 days5A
Acute otitis localised heat (such as a warm flannel).2D acid 2%2D,4B- OR
externa Second line: OTC topical acetic acid (>12yrs) topical neomycin sulphate Not available.
e.g. EarCalm spray OR topical antibiotic +/- with corticosteroid2D,5A- Access
steroid e.g. betamethasone 0.1% neomycin 7 days (min) to supporting
Public Health 3 drops TDS5A-
(Betnesol N drops) or Otomize Spray: similar cure evidence and
England (consider safety issues if 14 days (max)3A+
at 7 days.2D,3A+,4B- rationales on the
perforated tympanic
If cellulitis or disease extends outside ear PHE website
membrane)6B-
Last updated: canal, or systemic signs of infection, swab ear,
Nov 2017 start oral flucloxacillin and refer to exclude 250mg QDS2D
If cellulitis:
malignant otitis externa.1D If severe: 500mg 7 days2D
flucloxacillin7B+
QDS2D
Sinusitis First choice:
Advise OTC paracetamol or ibuprofen for pain. 500mg QDS 5 days
phenoxymethylpenicillin
Little evidence that nasal saline or nasal
Penicillin allergy:
decongestants help, but people may want to try 200mg on day 1,
doxycycline (not in under
them OTC. then 100mg OD
12s) OR
Symptoms for 10 days or less: no antibiotic.
clarithromycin OR 500mg BD 5 days
Symptoms with no improvement for more than
erythromycin (preferred if 250 to 500mg QDS
10 days: no antibiotic or back-up antibiotic
Public Health pregnant) or
depending on likelihood of bacterial cause.
England Consider high-dose nasal corticosteroid (if over 500 to 1000mg BD
12 years). Second choice or first
Systemically very unwell or high risk of choice if systemically
complications: immediate antibiotic. very unwell or high risk of 500/125mg TDS 5 days
Last updated: complications:
Oct 2017 For detailed information click on the visual summary.
co-amoxiclav
6|PageDoses Visual
Infection Key points Medicine Length
Adult Child summary
Lower respiratory tract infections
First choice: 500mg TDS (see
BNF for severe -
Acute amoxicillin OR infection)
exacerbation of
200mg on day 1,
COPD 5 days
Many exacerbations are not caused by bacterial then 100mg OD (see
doxycycline OR -
infections so will not respond to antibiotics. BNF for severe
Consider an antibiotic, but only after considering infection)
severity of symptoms (particularly sputum colour clarithromycin 500mg BD -
changes and increases in volume or thickness),
Second choice: use alternative first choice
need for hospitalisation, previous exacerbations,
hospitalisations and risk of complications, Alternative choice (if
previous sputum culture and susceptibility results, person at higher risk of
500/125mg TDS -
and risk of resistance with repeated courses. treatment failure):
Public Health Some people at risk of exacerbations may have co-amoxiclav OR
England antibiotics to keep at home as part of their co-trimoxazole OR 960mg BD -
exacerbation action plan. levofloxacin (with 5 days
For detailed information click on the visual summary. specialist advice if co-
See also the NICE guideline on COPD in over 16s. amoxiclav or co-
500mg OD -
trimoxazole cannot be
Last updated: used; consider safety
Dec 2018
issues)
IV antibiotics (specialist only)
Acute Send a sputum sample for culture and First choice empirical
exacerbation of susceptibility testing. treatment: 500mg TDS
bronchiectasis amoxicillin (preferred if
(non-cystic Offer an antibiotic. pregnant) OR
fibrosis) doxycycline (not in under 200mg on day 1, 7 to 14 days
When choosing an antibiotic, take account of
severity of symptoms and risk of treatment failure. 12s) OR then 100mg OD
People who may be at higher risk of treatment clarithromycin 500mg BD
failure include people who’ve had repeated
7|PageDoses Visual
Infection Key points Medicine Length
Adult Child summary
courses of antibiotics, a previous sputum culture Alternative choice (if
with resistant or atypical bacteria, or a higher risk person at higher risk of
of developing complications. treatment failure) 500/125mg TDS
empirical treatment:
Public Health Course length is based on severity of
England bronchiectasis, exacerbation history, severity of co-amoxiclav OR
exacerbation symptoms, previous culture and
susceptibility results, and response to treatment. levofloxacin (adults only:
with specialist advice if
Do not routinely offer antibiotic prophylaxis to co-amoxiclav cannot be 500mg OD or BD 7 to 14 days
Acute
exacerbation of prevent exacerbations. used; consider safety
bronchiectasis issues) OR
Seek specialist advice for preventing
(non-cystic exacerbations in people with repeated acute ciprofloxacin (children
fibrosis) cont. exacerbations. This may include a trial of only: with specialist advice
if co-amoxiclav cannot be -
antibiotic prophylaxis after a discussion of the
Last updated: possible benefits and harms, and the need for used; consider safety
Dec 2018 regular review. issues)
IV antibiotics (specialist only)
For detailed information click on the visual summary.
When current susceptibility data available: choose antibiotics accordingly
8|PageDoses Visual
Infection Key points Medicine Length
Adult Child summary
Adults first choice (if 200mg on day 1,
indicated): then 100mg OD -
Some people may wish to try honey (in over 1s), doxycycline
the herbal medicine pelargonium (in over 12s), Adults alternative first
cough medicines containing the expectorant choices:
guaifenesin (in over 12s) or cough medicines 500mg TDS -
amoxicillin (preferred if
containing cough suppressants, except codeine, pregnant) OR 5 days
(in over 12s). These self-care treatments have
limited evidence for the relief of cough symptoms. clarithromycin OR 250mg to 500mg BD -
Acute cough with upper respiratory tract
250mg to 500mg
infection: no antibiotic.
erythromycin (preferred if QDS or
Acute bronchitis: no routine antibiotic. -
pregnant) 500mg to 1000mg
Acute cough and higher risk of complications
BD
Acute Cough (at face-to-face examination/remote
examination): immediate or back-up antibiotic. Children first choice (if -
Acute cough and systemically very unwell (at indicated):
face to face examination/remote examination): amoxicillin
immediate antibiotic. -
Higher risk of complications includes people with Children alternative first
pre-existing comorbidity; young children born choices:
prematurely; people over 65 with 2 or more of, or clarithromycin OR
over 80 with 1 or more of: hospitalisation in erythromycin OR -
Last updated: previous year, type 1 or 2 diabetes, history of
Feb 2019 congestive heart failure, current use of oral doxycycline (not in under -
corticosteroids. 12s)
Do not offer a mucolytic, an oral or inhaled 5 days
bronchodilator, or an oral or inhaled corticosteroid
unless otherwise indicated.
For detailed information click on the visual
summary. See also the NICE guideline on
pneumonia for prescribing antibiotics in adults
with acute bronchitis who have had a C-reactive
protein (CRP) test (CRP100mg/l: immediate antibiotic).
9|PageDoses Visual
Infection Key points Medicine Length
Adult Child summary
On 23 April 2020, NICE clarified the First choice 200mg on day 1,
recommendations on antibiotic treatment for doxycycline (not in under then 100mg OD for 4 5 Days
bacterial pneumonia in the community during the 12s) days
COVID-19 pandemic. Alternative: amoxicillin 500mg TDS 5 Days
As COVID‑19 pneumonia is caused by a virus,
antibiotics are ineffective. Do not offer an
COVID-19 rapid antibiotic for treatment or prevention of
guideline: pneumonia if COVID‑19 is likely to be the cause
managing and symptoms are mild.
suspected or For choice of antibiotics in
Offer an oral antibiotic for treatment of pneumonia penicillin allergy, pregnancy
confirmed in people who can or wish to be treated in the
pneumonia in and more severe disease,
community if the likely cause is bacterial or it is or if atypical pathogens are
adults in the unclear whether the cause is bacterial or viral and
community likely, see the normal
symptoms are more concerning or they are at community acquired
[NG165] high risk of complications because, for example, pneumonia NICE guidance
they are older or frail, or have a pre-existing below
comorbidity such as immunosuppression or
significant heart or lung disease (for example
bronchiectasis or COPD), or have a history of
severe illness following previous lung infection.
Community- First choice (low severity
Assess severity in adults based on clinical 500mg TDS (higher
acquired in adults or non-severe in
judgement guided by mortality risk score (CRB65 doses can be used,
pneumonia children):
or CURB65). See the NICE guideline on see BNF)
amoxicillin
pneumonia for full details: Alternative first choice
low severity – CRB65 0 or CURB65 0 or 1 (low severity in adults or
200mg on day 1, 5 days*
moderate severity – CRB65 1 or 2 or CURB65 2 non-severe in children):
then 100mg OD
doxycycline (not in under
high severity – CRB65 3 or 4 or CURB65 3 to 5.
12s) OR
Public Health clarithromycin OR 500mg BD
England Each CRB65 parameter scores one: erythromycin (in
500mg QDS
• Confusion (AMT30/min;
amoxicillin doses can be used, -
• BP systolic 65 pathogens suspected)
clarithromycin OR 500mg BD -
10 | P a g eDoses Visual
Infection Key points Medicine Length
Adult Child summary
Assess severity in children based on clinical erythromycin (in
500mg QDS -
Community- judgement. pregnancy)
acquired Offer an antibiotic. Start treatment as soon as Alternative first choice
pneumonia possible after diagnosis, within 4 hours (within 1 (moderate severity in 200mg on day 1,
-
cont. hour if sepsis suspected and person meets any adults): then 100mg OD
high-risk criteria – see the NICE guideline on doxycycline OR
sepsis). clarithromycin 500mg BD -
When choosing an antibiotic, take account of First choice (high severity
severity, risk of complications, local antimicrobial in adults or severe in
Last updated: Sept
resistance and surveillance data, recent antibiotic children):
2019 500/125mg TDS
use and microbiological results. co-amoxiclav
AND (if atypical
* Stop antibiotics after 5 days unless pathogens suspected)
microbiological results suggest a longer course is clarithromycin OR 500mg BD 5 days*
needed or the person is not clinically stable.
erythromycin (in
For detailed information click on the visual summary. 500mg QDS
pregnancy)
See also the NICE guideline on pneumonia.
Alternative first choice
(high severity in adults):
500mg BD -
levofloxacin (consider
safety issues)
IV antibiotics (specialist only)
11 | P a g eDoses Visual
Infection Key points Medicine Length
Adult Child summary
Urinary tract infections
Non-pregnant women
100mg m/r BD (or if
Advise paracetamol or ibuprofen for pain and to first choice:
unavailable 50mg -
drink sufficient fluids to avoid dehydration. nitrofurantoin (if eGFR
QDS)
Non-pregnant women: back up antibiotic (to use ≥45 ml/minute) OR 3 days
if no improvement in 48 hours or symptoms trimethoprim (only if
worsen at any time) or immediate antibiotic. culture results available and 200mg BD -
Pregnant women, men, children or young susceptible)
people: send midstream urine for culture and Non-pregnant women
Lower urinary 100mg m/r BD (or if
sensitivity before treatment empirically. second choice:
tract infection unavailable 50mg - 3 days
When considering antibiotics, take account of nitrofurantoin (if eGFR
QDS)
severity of symptoms, risk of complications, ≥45 ml/minute) OR
previous urine culture and susceptibility results, *pivmecillinam (a 400mg initial dose,
- 3 days
previous antibiotic use which may have led to penicillin) OR then 200mg TDS
resistant bacteria and local antimicrobial 3g single dose
*fosfomycin - single dose
resistance data. sachet
For detailed information click on the visual summary. Pregnant women first
See also the NICE guideline on urinary tract infection in 100mg m/r BD (or if
choice: nitrofurantoin
under 16s: diagnosis and management and the Public unavailable 50mg - 7 days
(avoid at term) – if eGFR
Health England urinary tract infection: diagnostic tools QDS)
≥45 ml/minute
for primary care.
Pregnant women second
*Only if non-pregnant woman has failed any first- choice: amoxicillin (only if
500mg TDS -
choice treatment options for in the last 1 month or culture results available and 7 days
risk factor for increased resistance susceptible) OR
cefalexin 500mg BD -
Risk factors for increased resistance – Treatment of asymptomatic bacteriuria in pregnant women: choose from
• care home resident nitrofurantoin (avoid at term), amoxicillin or cefalexin based on recent culture
• recurrent UTI (2 in 6 months; 3 in 12 and susceptibility results
Public Health
months) Men first choice: 100mg m/r BD (or if
England
• hospitalisation for >7 days in the last 6 nitrofurantoin (if eGFR unavailable 50mg -
months ≥45 ml/minute) OR QDS)
7 days
• recent travel to country with increased Trimethoprim
resistance (only if culture results 200mg BD -
• previous resistant isolates, unresolving available and susceptible)
urinary symptoms Men second choice: basing antibiotic choice on recent culture and susceptibility
results. Consider alternative diagnoses
12 | P a g eDoses Visual
Infection Key points Medicine Length
Adult Child summary
Children and young
people (3 months and
over) first choice:
-
trimethoprim (only if
culture results available and
susceptible) OR
nitrofurantoin (if eGFR
-
≥45 ml/minute)
Children and young
Lower urinary people (3 months and -
tract infection over) second choice:
cont. -
nitrofurantoin (if eGFR
≥45 ml/minute and not used
as first choice) OR
Last updated: amoxicillin (only if culture
Oct 2018
results available and -
susceptible) OR
cefalexin -
First advise about behavioural and personal First choice antibiotic
100mg single dose
hygiene measures, and self-care (with D- prophylaxis:
when exposed to a
mannose or cranberry products) to reduce the risk nitrofurantoin (avoid at -
trigger or
of UTI. term) - if eGFR
50 to 100mg at night
For postmenopausal women, if no improvement, ≥45 ml/minute OR
Recurrent consider vaginal oestrogen (review within 200mg single dose
urinary tract 12 months). trimethoprim (avoid in when exposed to a
infection -
For non-pregnant women, if no improvement, pregnancy) trigger or
consider single-dose antibiotic prophylaxis for 100mg at night
exposure to a trigger (review within 6 months). 500mg single dose
For non-pregnant women (if no improvement or Second choice antibiotic
when exposed to a
no identifiable trigger) or with specialist advice for prophylaxis: -
trigger or
pregnant women, men, children or young people, amoxicillin OR
250mg at night
Public Health consider a trial of daily antibiotic prophylaxis cefalexin 500mg single dose -
England (review within 6 months). when exposed to a
Last updated:
For detailed information click on the visual trigger or
Oct 2018
summary. See also the NICE guideline on urinary 125mg at night
tract infection in under 16s: diagnosis and
management and the Public Health England
urinary tract infection: diagnostic tools for primary
care.
13 | P a g eDoses Visual
Infection Key points Medicine Length
Adult Child summary
Acute Advise paracetamol (+/- low-dose weak opioid) for Non-pregnant women and
pyelonephritis pain for people over 12. Send midstream urine men first choice: 1g TDS - 7 to 10 days
(upper urinary sample for culture and susceptibility testing cefalexin OR
tract) Offer an antibiotic. co-amoxiclav (only if
When prescribing antibiotics, take account of culture results available and 500/125mg TDS - 7 to 10 days
severity of symptoms, risk of complications, susceptible) OR
previous urine culture and susceptibility results, trimethoprim (only if
previous antibiotic use which may have led to culture results available and 200mg BD - 14 days
resistant bacteria and local antimicrobial susceptible) OR
resistance data. People at higher risk of
complications include those with abnormalities of ciprofloxacin (consider
500mg BD - 7 days
the genitourinary tract or underlying disease (such safety issues)
as diabetes or immunosuppression). Non-pregnant women and men IV antibiotics (click on visual summary)
For detailed information click on the visual summary. Pregnant women first 500mg BD or TDS
See also the NICE guideline on urinary tract infection in choice: (up to 1g to 1.5g
under 16s: diagnosis and management and the Public - 7 to 10 days
cefalexin TDS or QDS for
Public Health Health England urinary tract infection: diagnostic tools severe infections)
for primary care.
England Pregnant women second choice or IV antibiotics (click on visual summary)
Children and young
people (3 months and
-
over) first choice:
cefalexin OR -
co-amoxiclav (only if
culture results available and -
susceptible)
Last updated:
Oct 2018 Children and young people (3 months and over) IV antibiotics (specialist
only)
14 | P a g eDoses Visual
Infection Key points Medicine Length
Adult Child summary
Catheter- Antibiotic treatment is not routinely needed for Non-pregnant women and
associated asymptomatic bacteriuria in people with a urinary men first choice if no 100mg m/r BD (or if
urinary tract catheter. upper UTI symptoms: unavailable 50mg -
infection Consider removing or, if not possible, changing nitrofurantoin (if eGFR QDS)
the catheter if it has been in place for more than 7 ≥45 ml/minute) OR
days. But do not delay antibiotic treatment if it is 7 days
trimethoprim (if low risk of
indicated. 200mg BD -
resistance) OR
Advise paracetamol for pain. amoxicillin (only if culture
Advise drinking enough fluids to avoid results available and 500mg TDS -
dehydration. susceptible)
Offer an antibiotic for a symptomatic infection. Non-pregnant women and
When prescribing antibiotics, take account of men second choice if no 400mg initial dose,
upper UTI symptoms: - 7 days
severity of symptoms, risk of complications, then 200mg TDS
previous urine culture and susceptibility results, pivmecillinam (a penicillin)
previous antibiotic use which may have led to
Non-pregnant women and 500mg BD or TDS
resistant bacteria and local antimicrobial men first choice if upper (up to 1g to 1.5g
Public Health resistance data. UTI symptoms: -
TDS or QDS for
England Do not routinely offer antibiotic prophylaxis to
cefalexin OR severe infections) 7 to 10 days
people with a short-term or long-term catheter.
co-amoxiclav (only if
For detailed information click on the visual summary.
See also the Public Health England urinary tract culture results available and 500/125mg TDS -
infection: diagnostic tools for primary care. susceptible) OR
trimethoprim (only if
culture results available and 200mg BD - 14 days
susceptible) OR
ciprofloxacin (consider
500mg BD - 7 days
safety issues)
Non-pregnant women and men IV antibiotics (specialist only) (click on visual
summary)
500mg BD or TDS
Pregnant women first
(up to 1g to 1.5g
choice: - 7 to 10 days
TDS or QDS for
cefalexin
severe infections)
Pregnant women second choice or IV antibiotics (specialist only) (click on
visual summary)
15 | P a g eDoses Visual
Infection Key points Medicine Length
Adult Child summary
Catheter- Children and young
associated people (3 months and
urinary tract over) first choice:
-
infection cont. trimethoprim (only if
culture results available and
Last updated: susceptible) OR
Nov 2018 amoxicillin (only if culture -
results available and -
susceptible) OR
cefalexin OR -
co-amoxiclav (only if
culture results available and -
susceptible)
Children and young people (3 months and over) IV antibiotics (specialist
only)
First choice (guided by
Advise paracetamol (+/- low-dose weak opioid) for susceptibilities when
Acute available): 500mg BD -
pain, or ibuprofen if preferred and suitable.
prostatitis ciprofloxacin (consider
Offer antibiotic.
safety issues) OR
Review antibiotic treatment after 14 days and 14 days then
either stop antibiotics or continue for a further ofloxacin (consider safety review
200mg BD -
14 days if needed (based on assessment of issues) OR
history, symptoms, clinical examination, urine and trimethoprim (if
blood tests). fluoroquinolone not
200mg BD -
Quinolones achieve higher prostate levels. Admit appropriate; seek specialist
Public Health advice)
England to hospital if man has any of the following:
severely ill or in acute urinary retention. Consider Second choice (after
urgent referral if man is immunocompromised or discussion with specialist):
500mg OD - 14 days, then
has diabetes or had a pre-existing urological levofloxacin (consider
Last updated: condition. safety issues) OR review
Oct 2018
For detailed information click on the visual summary. co-trimoxazole 960mg BD -
IV antibiotics (specialist only)
16 | P a g eDoses Visual
Infection Key points Medicine Length
Adult Child summary
Meningitis
Transfer all patients to hospital immediately.1D Stat dose;1D
Suspected If time before hospital admission,2D,3A+ if ChildDoses Visual
Infection Key points Medicine Length
Adult Child summary
Helicobacter Always test for H.pylori before giving antibiotics. Always use PPI2D,3D,5A+,12A+
pylori Treat all positives. If negative, only retest for First line and first relapse
-
H.pylori if DU, GU, family history of cancer, and no penicillin allergy
MALToma, or if test was performed within two PPI PLUS 2 antibiotics
weeks of PPI, or four weeks of antibiotics.21B+,27C
amoxicillin2D,6B+ PLUS 1000mg BD14A+
Leave a 2-week washout period after proton
pump inhibitor (PPI) use before testing for H. clarithromycin2D,6B+ OR 500mg BD8A-
pylori with a carbon‑13 urea breath test (UBT) or
Public Health a stool antigen test (STA), or laboratory-based metronidazole2D,6B+ 400mg BD2D
England serology where its performance has been locally
validated Penicillin allergy and
Do not test for H pylori in proven GORD previous clarithromycin:
Do not offer eradication for GORD.3D PPI WITH bismuth -
See PHE quick Do not use clarithromycin, metronidazole or subsalicylate PLUS 2 - 7 days2D
reference guide quinolone if used in the past year for any antibiotics MALToma
for diagnostic infection.5A+,6B+,7A+ bismuth subsalicylate13A+ 14 days7A+,16A+
525mg QDS15D Not available.
advice: PHE Penicillin allergy: use PPI PLUS clarithromycin PLUS
Access
H. pylori PLUS metronidazole.2D If previous metronidazole2D PLUS 400mg BD2D supporting
clarithromycin, use PPI PLUS bismuth salt evidence and
PLUS metronidazole PLUS tetracycline tetracycline2D 500mg QDS15D
rationales on the
hydrochloride.2D,8A-,9D Relapse and previous PHE website
Relapse and no penicillin allergy use PPI PLUS metronidazole and
- -
amoxicillin PLUS clarithromycin or clarithromycin:
metronidazole (whichever was not used first line) PPI PLUS 2 antibiotics
Last updated: 2D
amoxicillin2D,7A+ PLUS 1000mg BD14A+
Feb 2019
Relapse and previous metronidazole and
tetracycline2D,7A+ OR 500mg QDS15D
clarithromycin: use PPI PLUS amoxicillin
PLUS either tetracycline OR levofloxacin (if levofloxacin (if tetracycline
250mg BD7A+
tetracycline not tolerated).2D,7A+ cannot be used)2D,7A+
Relapse and penicillin allergy (no exposure to Third line (specialist only)
- -
quinolone): use PPI PLUS metronidazole PLUS PPI WITH
levofloxacin.2D bismuth subsalicylate
525mg QDS15D - 10 days
Relapse and penicillin allergy (with exposure PLUS
to quinolone): use PPI PLUS bismuth salt PLUS 2 antibiotics as above not
metronidazole PLUS tetracycline.2D - -
previously used OR
rifabutin14A+ OR 150mg BD -
18 | P a g eDoses Visual
Infection Key points Medicine Length
Adult Child summary
Retest for H. pylori: post DU/GU, or relapse after furazolidone17A+ 200mg BD
second-line therapy,1A+ using UBT or SAT,10A+,11A+
consider referral for endoscopy and culture.2D -
PPI – Use either Omeprazole 20mg BD OR
Lansoprazole 30mg BD
Mild first episode:
Review need for antibiotics,1D,2D PPIs,3B- and 400mg TDS1D,2D 10 to 14 days1D,4B-
metronidazole2D,4B-
antiperistaltic agents and discontinue use where Severe, type 027 or
Clostridium possible.2D Mild cases (38.5, or WCC>15, rising Recurrent or second line: PHE website
creatinine, or signs/symptoms of severe fidaxomicin2D,5A- 200mg BD5A- - 10 days5A-
Last updated:
Oct 2018 colitis): 1D,2D,5A- review progress closely,1D,2D and (specialist only)
consider hospital referral.2D 2D specialist to treat
with oral vancomycin
Acute Acute diverticulitis and systemically well: First-choice 500/125mg TDS -
diverticulitis Consider no antibiotics, offer simple analgesia (for (uncomplicated acute
example paracetamol), advise to re-present if diverticulitis):
symptoms persist or worsen. co-amoxiclav
Acute diverticulitis and systemically unwell, Penicillin allergy or co- cefalexin: 500mg BD -
immunosuppressed or significant amoxiclav unsuitable: or TDS (up to 1g to
Last updated: Nov
2019 comorbidity: offer an antibiotic. cefalexin (caution in 1.5g TDS or QDS for
Give oral antibiotics if person not referred to penicillin allergy) AND severe infections)
hospital for suspected complicated acute metronidazole OR metronidazole:
diverticulitis. 400mg TDS 5 days*
Give IV antibiotics if admitted to hospital with trimethoprim AND trimethoprim: 200mg -
suspected or confirmed complicated acute metronidazole OR BD
diverticulitis (including diverticular abscess). metronidazole:
If CT-confirmed uncomplicated acute diverticulitis, 400mg TDS
review the need for antibiotics. ciprofloxacin (only if ciprofloxacin: 500mg
* A longer course may be needed based on switching from IV BD
clinical assessment. ciprofloxacin with metronidazole:
specialist advice; consider 400mg TDS
safety issues) AND
metronidazole
19 | P a g eDoses Visual
Infection Key points Medicine Length
Adult Child summary
For IV antibiotics in complicated acute diverticulitis
(including diverticular abscess) (specialist only)
Traveller’s Standby: Not available.
diarrhoea 500mg OD1D,3A+ - 1 to 3 days1D,2D,3A+
Prophylaxis rarely, if ever, indicated.1D Consider azithromycin Access
Public Health supporting
standby antimicrobial only for patients at high risk Prophylaxis/treatment: 2 tablets QDS1D,2D - 2 days1D,2D,4A- evidence and
England of severe illness,2D or visiting high-risk areas.1D,2D bismuth subsalicylate rationales on the
Last updated:
Oct 2018
PHE website
Treat all household contacts at the same Child >6 months: 1 dose;3B- repeat in
Threadworm time.1D Mebendazole should be advised OTC for mebendazole1D,3B- (OTC 100mg stat3B- 2 weeks if
all patients >2yrs for >2yrs) persistent3B- Not available.
Advise hygiene measures for 2 weeks1D (hand Access
Public Health supporting
hygiene;2D pants at night; morning shower, ChildDoses Visual
Infection Key points Medicine Length
Adult Child summary
azithromycin started and until symptoms resolved if
urethritis).3A+,4A+
If chlamydia, test for reinfection at 3 to 6 months
Chlamydia following treatment if under 25 years; or consider if over
25 years and high risk of re-infection.1B-,3B+, 5B-
trachomatis/
urethritis cont. Second line, pregnant, breastfeeding, allergy, or
intolerance: azithromycin is most
effective.6A+,7D,8A+,9A+,10D As lower cure rate in
pregnancy, test for cure at least 3 weeks after end of
treatment.3A+
Consider referring all patients with symptomatic
urethritis to GUM as testing should include Mycoplasma
Last updated: genitalium and Gonorrhoea.11A-
July 2019 If M.genitalium is proven, use doxycycline followed by
azithromycin using the same dosing regimen and
advise to avoid sex for 14 days after start of treatment
and until symptoms have resolved.11A-,12A+
Doxycycline1A+,2D OR 100mg BD1A+,2D 10 to 14 days1A+,2D Not available.
Epididymitis Access
Usually due to Gram-negative enteric bacteria in -
Public Health Ofloxacin (consider safety supporting
men over 35 years with low risk of STI.1A+,2D 200mg BD1A+,2D 14 days1A+,2D
England issues) 1A+,2D OR evidence and
Last updated: If under 35 years or STI risk, refer to GUM.1A+,2D
Ciprofloxacin (consider 500mg BD1A+,2D,3A+ 10 days1A+,2D,3A+ rationales on the
Nov 2017 PHE website
safety issues) 1A+,2D
clotrimazole1A+,5D OR 500mg pessary1A+ Stat1A+
Vaginal All topical and oral azoles give over 80% clotrimazole OR 200mg pessary 3 nights
cure.1A+,2A+ -
candidiasis clotrimazole1A+ OR 100mg pessary1A+ 6 nights1A+ Not available.
Pregnant: avoid oral azoles, the 7-day courses oral fluconazole1A+,3D 150mg1A+,3D Stat1A+ Access
Public Health are more effective than shorter ones.1A+,3D,4A+ supporting
Recurrent (>4 episodes per year):1A+ 150mg 150mg every evidence and
England If recurrent: 72 hours 3 doses
oral fluconazole every 72 hours for 3 doses rationales on the
induction,1A+ followed by 1 dose once a week for fluconazole THEN - PHE website
Last updated:
Oct 2018 6 months maintenance.1A+ (induction/maintenance)1A+ 150mg once a 6 months1A+
week1A+,3D
Bacterial 400mg BD1A+,3A+ 5 - 7 days (NICE CKS
Oral metronidazole is as effective as topical oral metronidazole1A+,3A+ 2018) OR
vaginosis OR Not available.
treatment,1A+ and is cheaper.2D OR
2000mg1A+,2D Stat2D Access
Public Health 7 days results in fewer relapses than 2g stat at metronidazole 0.75% 5g applicator at supporting
- 5 nights1A+,2D,3A+
England 4 weeks.1A+,2D vaginal gel1A+,2D,3A+ OR night1A+,2D,3A+ evidence and
Pregnant/breastfeeding: avoid 2g dose.3A+,4D rationales on the
clindamycin 2% 5g applicator at PHE website
Last updated: Treating partners does not reduce relapse.5A+ 7 nights1A+,2D,3A+
Nov 2017 cream1A+,2D night1A+,2D
21 | P a g eDoses Visual
Infection Key points Medicine Length
Adult Child summary
400mg TDS1A+,3A+ 5 days1A+
Advise: saline bathing,1A+ analgesia,1A+ or OTC
topical lidocaine for pain,1A+ and discuss oral aciclovir1A+,2D,3A+,4A+ 200mg five times a
Genital herpes 5 day (NICE CKS 2017) Not available.
transmission.1A+ OR day
Access
First episode: treat within 5 days if new lesions 800mg TDS (if supporting
Public Health 2 days1A+
or systemic symptoms,1A+,2D and refer to GUM.2D recurrent)1A+ - evidence and
England
Recurrent: self-care if mild,2D or immediate short Valaciclovir (specialist rationales on the
500mg BD1A+ 5 days1A+
course antiviral treatment,1A+,2D or suppressive only) 1A+,3A+,4A+ OR PHE website
Last updated: therapy if more than 6 episodes per year.1A+,2D 250mg TDS1A+ 5 days1A+
Famciclovir (specialist
Nov 2017 1000mg BD (if
only) 1A+,4A+ 1 day1A+
recurrent)1A+
Antibiotic resistance is now very high.1D,2D
Refer to GUM.3B- Test of cure is essential.2D Not available.
Gonorrhoea ceftriaxone2D OR 1000mg IM2D Stat2D
Use IM ceftriaxone if susceptibility not known Access
Public Health supporting
England prior to treatment2D. - evidence and
Last updated: Use ciprofloxacin only If susceptibility is known ciprofloxacin2D
(only if known to be 500mg2D Stat2D rationales on the
Feb 2019 prior to treatment and the isolate is sensitive to PHE website
ciprofloxacin at all sites of infection1D,2D sensitive)
Trichomoniasis Oral treatment needed as extravaginal infection 400mg BD1A+,6A+ 5 to 7 day1A+
Not available.
common.1D Treat partners,1D and refer to GUM for metronidazole1A+,2A+,3D,6A+ 2g (more adverse Access
Stat1A+,6A+
Public Health other STIs.1D effects)6A+ supporting
England Pregnancy to treat 100mg pessary at - 6 nights5D evidence and
Pregnant/breastfeeding: avoid 2g single dose
metronidazole;2A+,3D clotrimazole for symptom symptoms: night5D rationales on the
Last updated: clotrimazole2A+,4A-,5D PHE website
Nov 2017 relief (not cure) if metronidazole declined.2A+,4A-,5D
Refer women and sexual contacts to GUM.1A+ First line therapy:
Pelvic Raised CRP supports diagnosis, absent pus cells ceftriaxone1A+,3C,4C PLUS 1000mg IM1A+,3C Stat1A+,3C
inflammatory in HVS smear good negative predictive value.1A+ metronidazole1A+,5A+ PLUS 400mg BD1A+ 14 days1A+
disease Exclude: ectopic pregnancy, appendicitis, doxycycline1A+,5A+ 100mg BD1A+ 14 days1A+
endometriosis, UTI, irritable bowel, complicated Not available.
Second line therapy:
ovarian cyst, functional pain. 400mg BD1A+ 14 days1A+ Access
metronidazole1A+,5A+ PLUS supporting
Public Health Moxifloxacin has greater activity against likely ofloxacin1A+,2A-,5A+ - evidence and
pathogens, but always test for gonorrhoea, 400mg BD1A+,2A- 14 days1A+
England OR rationales on the
chlamydia, and M. genitalium .1A+ PHE website
If M. genitalium tests positive use moxifloxacin alone1A+
Last updated: moxifloxacin.1A+ (first line for M. genitalium 400mg OD1A+ 14 days1A+
Feb 2019 BASHH guideline for the Management of Pelvic associated PID)
Inflammatory Disease (2019 Interim Update)
22 | P a g eDoses Visual
Infection Key points Medicine Length
Adult Child summary
Skin and soft tissue infections
Note: Refer to RCGP Skin Infections online training.1D For MRSA, discuss therapy with microbiologist.1D
Localised non-bullous impetigo: Topical antiseptic:
1% BD - TDS
Hydrogen peroxide 1% cream (other topical hydrogen peroxide
antiseptics are available but no evidence for First choice topical
Impetigo impetigo). If hydrogen peroxide unsuitable or antibiotic if hydrogen
ineffective, short-course topical antibiotic. 2% ointment TDS
peroxide unsuitable
Widespread non-bullous impetigo: Fusidic Acid
Short-course topical or oral antibiotic. Take
account of person’s preferences, practicalities of Fusidic acid resistance
administration, previous use of topical antibiotics suspected or confirmed: TDS
because antimicrobial resistance can develop mupirocin 2%
rapidly with extended or repeated use, and local First line oral antibiotic
antimicrobial resistance data. 500mg QDS 5 days*
oral flucloxacillin
Bullous impetigo, systemically unwell, or high Penicillin allergy or
risk of complications: 250mg BD
flucloxacillin unsuitable:
Short-course oral antibiotic. Do not offer clarithromycin OR
combination treatment with a topical and oral
antibiotic to treat impetigo. *5 days is appropriate
250mg to 500mg
for most, can be increased to 7 days based on erythromycin (in pregnancy)
QDS
Last updated: clinical judgement.Referral to a consultant in
Feb 2020 Communicable Disease Control is required if
there is a significant local outbreak (for example, If MRSA suspected or confirmed – consult local
in a nursing home or school). For detailed microbiologist
information click on the visual summary.
Second line: topical Thinly OD3A+
Mild (open and closed comedones)1D or 6 to 8 weeks1D
retinoid1D,2D,3A+ OR
Acne moderate (inflammatory lesions):1D OTC benzoyl peroxide1A- 5% cream OD-BD3A+
,2D,3A+,4A- 6 to 8 weeks1D
First line: self-care1D (wash with mild soap; do
Not available.
not scrub; avoid make-up).1D Third-line: topical 1% cream, thinly
12 weeks1A-,2D Access
Public Health Second line: OTC benzoyl peroxide.2D or topical clindamycin3A+ BD3A+ supporting
England retinoid e.g. adapalene 0.1% gel/cream If treatment 408mg OD evidence and
failure/severe: At least 8 weeks
rationales on the
Third-line: add topical antibiotic,1D,3A+ or consider (BNF/cBNF)
oral lymecycline OR PHE website
addition of oral antibiotic.1D
Last updated: oral tetracycline1A-,3A+ OR 500mg BD3A+
Nov 2017 Severe (nodules and cysts):1D add oral antibiotic 6 to 12 weeks3A+
(for 3 months max)1D,3A+ and refer.1D,2D oral doxycycline3A+,4A- 100mg OD3A+ 6 to 12 weeks3A+
23 | P a g eDoses Visual
Infection Key points Medicine Length
Adult Child summary
Cold sores
Public Health Most resolve after 5 days without treatment.1A-,2A- Topical OTC antivirals applied prodromally can reduce duration by 12 to 18 hours.1A-,2A-,3A-
England If frequent, severe, and predictable triggers: consider oral prophylaxis:4D,5A+ aciclovir 400mg, twice daily, for 5 to 7 days.5A+,6A+
Last updated: Access supporting evidence and rationales on the PHE website
Nov 2017
Panton-Valentine leukocidin (PVL) is a toxin produced by 20.8 to 46% of S. aureus from boils/abscesses.1B+,2B+,3B- PVL strains are rare in healthy people,
but severe.2B+
Suppression therapy should only be started after primary infection has resolved, as ineffective if lesions are still leaking.4D
Risk factors for PVL: recurrent skin infections;2B+ invasive infections;2B+ MSM;3B- if there is more than one case in a home or close community 2B+,3B-
(school children;3B- military personnel;3B- nursing home residents;3B- household contacts).3B-
PVL-SA Consider taking a swab of pus from the contents of the lesion if the boil or carbuncle is:
• Not responding to treatment, persistent or recurrent, to exclude atypical mycobacteria or PVL-SA.
Public Health • There are multiple lesions.
England • The person: Is immunocompromised, is known to be colonized with MRSA, Has diabetes.
Last updated: • If PVL-SA is suspected, this should be mentioned specifically on the laboratory form
Nov 2017
If positive PVL MRSA or positive S. aureus contact the North East and North Central London Health Protection Team (NENCLHPT)
contact numbers:
• Daytime Tel: 020 3837 7084 (option 2)
• For Out of Hours Advice: Tel: 0151 909 1215 (between 5pm and 9am and during weekends and Bank Holidays)
• Email: necl.team@phe.gov.uk ; phe.nenclhpt@nhs.net
Access the supporting evidence and rationales on the PHE website.
First-choice:
flucloxacillin 500mg to 1g QDS - 7 days
Manage any underlying conditions to promote Penicillin allergy or if flucloxacillin unsuitable:
Leg ulcer ulcer healing.
Only offer an antibiotic when there are symptoms doxycycline OR 200mg on day 1,
or signs of infection (such as redness or swelling then 100mg OD (can
be increased to 200mg
spreading beyond the ulcer, localised warmth, daily)
increased pain or fever). Few leg ulcers are - 7 Days
clarithromycin OR 500mg BD
clinically infected but most are colonised by
bacteria. erythromycin (in 500mg QDS
When prescribing antibiotics, take account of pregnancy)
severity, risk of complications and previous Second choice:
antibiotic use. co-amoxiclav OR 500/125mg TDS
Last updated:
Feb 2020 For detailed information click on the visual - 7 Days
co-trimoxazole (in 960mg BD
summary.
penicillin allergy)
For antibiotic choices if severely unwell or MRSA suspected or confirmed,
click on the visual summary
24 | P a g eDoses Visual
Infection Key points Medicine Length
Adult Child summary
First choice:
flucloxacillin 500mg to 1g QDS 5 to 7 days*
Cellulitis and Penicillin allergy or if flucloxacillin unsuitable:
erysipelas Exclude other causes of skin redness clarithromycin (inc 500mg BD 5 to 7 days*
(inflammatory reactions or non-infectious causes). children with penicillin
Consider marking extent of infection with a single- allergy) OR
use surgical marker pen. erythromycin (in 500mg QDS
Offer an antibiotic. Take account of severity, site pregnancy) OR
of infection, risk of uncommon pathogens, any doxycycline (adults only) 200mg on day 1, -
microbiological results and MRSA status. OR then 100mg OD
Public Health Infection around eyes or nose is more concerning co-amoxiclav (children -
England because of serious intracranial complications. only: not in penicillin
allergy)
*A longer course (up to 14 days in total) may be
If infection near eyes or nose:
needed but skin takes time to return to normal,
co-amoxiclav 500/125mg TDS 7 days*
and full resolution at 5 to 7 days is not expected.
Do not routinely offer antibiotics to prevent If infection near eyes or nose (penicillin allergy):
recurrent cellulitis or erysipelas. clarithromycin AND 500mg BD 7 days*
Last updated: For detailed information click on the visual metronidazole (only add in 400mg TDS
Sept 2019 summary. children if anaerobes
suspected)
For alternative choice antibiotics for severe infection, suspected or
confirmed MRSA infection and IV antibiotics (specialist only) click on the
visual summary
Eczema
No visible signs of infection: antibiotic use (alone or with steroids)1A+ encourages resistance and does not improve healing.1A+
Public Health
With visible signs of infection: use oral flucloxacillin2D or clarithromycin,2D or topical treatment (as in impetigo).2D
England Access the supporting evidence and rationales on the PHE website
Last updated Nov17
Diabetic foot Mild infection: first choice
infection In diabetes, all foot wounds are likely to be flucloxacillin 500mg to 1g QDS - 7 days*
colonised with bacteria. Diabetic foot infection has Mild infection (penicillin allergy):
at least 2 of: local swelling or induration; clarithromycin OR 500mg BD
erythema; local tenderness or pain; local warmth; erythromycin (in
purulent discharge. 500mg QDS
pregnancy) OR
Severity is classified as: 200mg on day 1, - 7 days*
Mild: local infection with 0.5 to less than 2cm then 100mg OD (can
erythema doxycycline
be increased to
200mg daily)
25 | P a g eDoses Visual
Infection Key points Medicine Length
Adult Child summary
Moderate: local infection with more than 2cm
erythema or involving deeper structures (such as
abscess, osteomyelitis, septic arthritis or fasciitis)
Diabetic foot Severe: local infection with signs of a systemic
infection cont.. inflammatory response.
Start antibiotic treatment as soon as possible.
Take samples for microbiological testing before,
or as close as possible to, the start of treatment
When choosing an antibiotic, take account of
Last updated: For antibiotic choices for moderate or severe infection, infections where
severity, risk of complications, previous
Oct 2019 Pseudomonas aeruginosa or MRSA is suspected or confirmed, and IV
microbiological results and antibiotic use, and
antibiotics (specialist only) click on the visual summary
patient preference.
*A longer course (up to a further 7 days) may be
needed based on clinical assessment. However,
skin does take time to return to normal, and full
resolution at 7 days is not expected.
Do not offer antibiotics to prevent diabetic foot
infection.
For detailed information click on the visual
summary.
Scabies First choice OTC permethrin: Treat whole body OTC permethrin (>2yrs)
5% cream1D,2D Not available.
from ear/chin downwards,1D,2D and under 1D,2D,3A+
nails.1D,2D Access
Public Health 2 applications, 1- supporting
England If using permethrin and patient is under 2 years,
Permethrin allergy: 0.5% aqueous week apart1D evidence and
elderly or immunosuppressed, or if treating with rationales on the
malathion1D liquid1D
Last updated: malathion: also treat face and scalp.1D,2D PHE website
Oct 2018 Home/sexual contacts: treat within 24 hours.1D
Human: thorough irrigation is important.1A+,2D Prophylaxis/treatment all:
375mg to 625mg
Bites Antibiotic prophylaxis is advised.1A+,2D,3D Assess co-amoxiclav2D,3D 7 days3D
TDS3D
risk of tetanus, rabies,1A+ HIV, and hepatitis B and
C.3D Human bite + penicillin
Not available.
Cat: always give prophylaxis.1A+,3D allergy: Access
Public Health Dog: give prophylaxis if: puncture wound;1A+,3D metronidazole3D,4A+ AND 400mg TDS2D 7 days3D supporting
England bite to hand, foot, face, joint, tendon, or clarithromycin3D,4A+ 250mg to 500mg BD2D evidence and
ligament;1A+ immunocompromised; cirrhotic; rationales on the
asplenic; or presence of prosthetic Animal + penicillin PHE website
valve/joint.2D,4A+ allergy:
Last updated: metronidazole3D,4A+ AND 400mg TDS2D 7 days3D
July 2019 Penicillin allergy: Review all at 24 and
48 hours,3D as not all pathogens are covered.2D,3 doxycycline3D 100mg BD2D
26 | P a g eDoses Visual
Infection Key points Medicine Length
Adult Child summary
Insect bites An insect bite or sting often causes a small, red lump on the skin, which may be painful and itchy. Secondary bacterial infection is
and stings unlikely; it is unclear which causative organisms are most common. Do not offer an antibiotic if there are no symptoms or signs of
infection.
With rapid-onset skin reactions likely to be inflammatory or allergic reactions, most bites and stings will not need antibiotics.
The guideline notes people may wish to consider oral antihistamines (OTC) to help relieve itching (which may last up to 10 days), and
some antihistamines cause sedation, which might help at night.
Last updated:
Sept 2020
For bites and stings where there is a sign of an infection, antibiotic treatment recommendations in the NICE guideline on cellulitis and
erysipelas should be followed, or the guidance on Lyme disease if there is a known or suspected tick bite.
For lactating woman:
500mg QDS2D
flucloxacillin2D
If penicillin allergy: 250mg to 500mg
Mastitis S. aureus is the most common infecting erythromycin2D OR QDS2D Not available.
pathogen.1D Suspect if woman has: a painful clarithromycin2D 500mg BD2D Access
Public Health breast;2D fever and/or general malaise;2D a tender, supporting
For non-lactating woman
England red breast.2D (NICE CKS): 625mg TDS - 10 to 14 days2D evidence and
Breastfeeding: oral antibiotics are appropriate, co-amoxiclav rationales on the
Last updated: where indicated.2D,3A+ Women should continue If penicillin allergy (NICE PHE website
Nov 2017 feeding,1D,2D including from the affected breast.2D 500mg TDS
CKS): Metronidazole AND
Erythromycin OR 250mg to 500mg QDS
clarithromycin 500mg BD
Dermatophyte infection: skin topical terbinafine3A+,4D OR 1% OD to BD2A+ 1 to 4 weeks3A+
Including:
Tinea corporis (ringworm) topical clotrimazole 2A+,3A+ 1% OD to BD2A+ 4 to 6 weeks2A+,3A+
Dermatophyte Tinea pedis (athlete's foot), Tinea cruris (jock itch)
Tinea faciei (facial ringworm), Tinea capitis (scalp Alternative in athlete’s OD to BD2A+
infection: skin Not available.
ringworm) foot:
topical undecenoates2A+ Access
Most cases: use terbinafine as fungicidal, supporting
Public Health treatment time shorter and more effective than (such as Mycota®)2A+
evidence and
England with fungistatic imidazoles or undecenoates rationales on the
1D,2A+ If candida possible, use imidazole.4D
PHE website
Last updated: If intractable, or scalp: send skin scrapings,1D
Feb 2019 and if infection confirmed: use oral
terbinafine1D,3A+,4D or itraconazole.2A+,3A+,5D
Scalp: oral therapy,6D and discuss with
specialist.1D
27 | P a g eDoses Visual
Infection Key points Medicine Length
Adult Child summary
Take nail clippings;1D start therapy only if Fingers:
Dermatophyte infection is confirmed.1D Oral terbinafine is more 6 weeks1D,6D to 3
infection: nail effective than oral azole.1D,2A+,3A+,4D Liver reactions First line: months (NICE CKS)
250mg OD1D,2A+,6D
0.1 to 1% with oral antifungals.3A+ If candida or terbinafine1D,2A+,3A+,4D,6D Toes: Not available.
non-dermatophyte infection is confirmed, use oral 12 weeks1D,6D to 6 Access
Public Health itraconazole.1D,3A+,4D Topical nail lacquer is not as months (NICE CKS) supporting
effective.1D,5A+,6D 1 week repeated evidence and
England
To prevent recurrence: apply weekly 1% topical after 21 days rationales on the
Second line: PHE website
antifungal cream to entire toe area.6D 200mg BD 1D,4D Fingers:
itraconazole1D,3A+,4D,6D
Last updated: Children: seek specialist advice.4D 2 courses1D
Oct 2018 Toes: 3 courses1D
Stop treatment when continual, new, healthy, proximal nail growth.6D
Pregnant/immunocompromised/ First line for chicken pox
Varicella neonate/Breastfeeding: seek urgent specialist and shingles: 800mg 5 times
zoster/ advice.1D aciclovir3A+,7A+,10A+,13B+,14A- daily16A-
chickenpox Chickenpox: consider aciclovir2A+,3A+,4D if: onset
,15A+
Not available.
of rash 14 years of age;4D severe pain;4D dense/oral if poor compliance: 250mg to 500mg 7 days14A-,16A- supporting
rash;4D,5B+ taking steroids;4D smoker.4D,5B+ TDS15A+ OR evidence and
Herpes zoster/ not for children: -
rationales on the
shingles Give paracetamol for pain relief.6C famciclovir8D,14A-, 16A- 750mg BD15A+ PHE website
Shingles: treat if >50 years7A+,8D (PHN rare if (specialist only) ORYou can also read